

Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
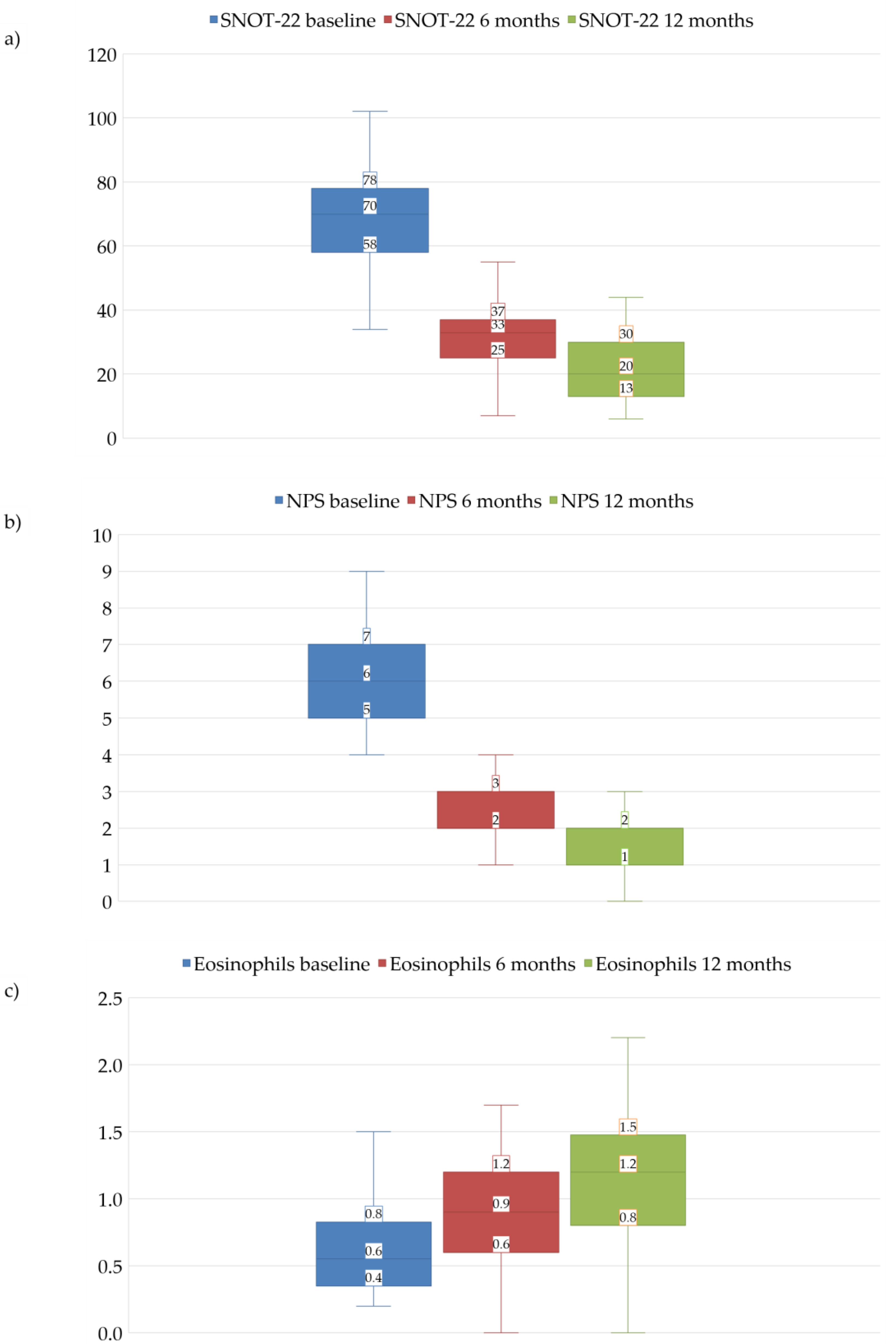
2. Results
Safety Profile
3. Discussion
Strengths and Limitations
4. Materials and Methods
4.1. Study Population
4.2. Clinical Evaluation
4.3. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoy, S.M. Dupilumab: A Review in Chronic Rhinosinusitis with Nasal Polyps. Drugs 2020, 80, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Ottaviano, G.; Saccardo, T.; Roccuzzo, G.; Bernardi, R.; Di Chicco, A.; Pendolino, A.L.; Scarpa, B.; Mairani, E.; Nicolai, P. Effectiveness of Dupilumab in the Treatment of Patients with Uncontrolled Severe CRSwNP: A “Real-Life” Observational Study in Naïve and Post-Surgical Patients. J. Pers. Med. 2022, 12, 1526. [Google Scholar] [CrossRef]
- De Corso, E.; Montuori, C.; Settimi, S.; Mele, D.A.; Cantiani, A.; Corbò, M.; Cantone, E.; Paludetti, G.; Galli, J. Efficacy of Biologics on Refractory Eosinophilic Otitis Media Associated with Bronchial Asthma or Severe Uncontrolled CRSwNP. J. Clin. Med. 2022, 11, 926. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Naclerio, R. Therapeutic Potential of Dupilumab in the Treatment of Chronic Rhinosinusitis with Nasal Polyps: Evidence to Date. Ther. Clin. Risk Manag. 2020, 16, 31–37. [Google Scholar] [CrossRef] [PubMed]
- Agache, I.; Song, Y.; Alonso-Coello, P.; Vogel, Y.; Rocha, C.; Solà, I.; Santero, M.; Akdis, C.A.; Akdis, M.; Canonica, G.W.; et al. Efficacy and safety of treatment with biologicals for severe chronic rhinosinusitis with nasal polyps: A systematic review for the EAACI guidelines. Allergy 2021, 76, 2337–2353. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinol. J. 2020, 58, 1–464. [Google Scholar] [CrossRef]
- Raciborski, F.; Arcimowicz, M.; Samolinski, B.; Pinkas, W.; Samel-Kowalik, P.; Śliwczyński, A. Recorded prevalence of nasal polyps increases with age. Adv. Dermatol. Allergol. 2021, 38, 682–688. [Google Scholar] [CrossRef]
- Lildholdt, T. Surgical versus medical treatment of nasal polyps. Rhinology 1989, 105, 140–143. [Google Scholar] [CrossRef]
- Hopkins, C.; Browne, J.P.; Slack, R.; Lund, V.; Brown, P. The Lund-Mackay staging system for chronic rhinosinusitis: How is it used and what does it predict? Otolaryngol. Neck Surg. 2007, 137, 555–561. [Google Scholar] [CrossRef]
- Lund, V.J.; Kennedy, D.W. Staging for Rhinosinusitis. Otolaryngol. Neck Surg. 1997, 117, S35–S40. [Google Scholar] [CrossRef]
- Helliwell, T. Inflammatory diseases of the nasal cavities and paranasal sinuses. Diagn. Histopathol. 2010, 16, 255–264. [Google Scholar] [CrossRef]
- Ikeda, K.; Shiozawa, A.; Ono, N.; Kusunoki, T.; Hirotsu, M.; Homma, H.; Saitoh, T.; Murata, J. Subclassification of chronic rhinosinusitis with nasal polyp based on eosinophil and neutrophil. Laryngoscope 2013, 123, E1–E9. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Akdis, C.A. Phenotypes and Emerging Endotypes of Chronic Rhinosinusitis. J. Allergy Clin. Immunol. Pract. 2016, 4, 621–628. [Google Scholar] [CrossRef] [PubMed]
- Bachert, C.; Han, J.K.; Desrosiers, M.; Hellings, P.W.; Amin, N.; Lee, S.E.; Mullol, J.; Greos, L.S.; Bosso, J.V.; Laidlaw, T.M.; et al. Efficacy and safety of dupilumab in patients with severe chronic rhinosinusitis with nasal polyps (LIBERTY NP SINUS-24 and LIBERTY NP SINUS-52): Results from two multicentre, randomised, double-blind, placebo-controlled, parallel-group phase 3 trials. Lancet 2019, 394, 1638–1650. [Google Scholar] [CrossRef]
- Huang, Z.-Q.; Liu, J.; Ong, H.H.; Yuan, T.; Zhou, X.-M.; Wang, J.; Sen Tan, K.; Chow, V.T.; Yang, Q.-T.; Shi, L.; et al. Interleukin-13 Alters Tight Junction Proteins Expression Thereby Compromising Barrier Function and Dampens Rhinovirus Induced Immune Responses in Nasal Epithelium. Front. Cell Dev. Biol. 2020, 8, 572749. [Google Scholar] [CrossRef] [PubMed]
- Kato, A.; Peters, A.T.; Stevens, W.W.; Schleimer, R.P.; Tan, B.K.; Kern, R.C. Endotypes of chronic rhinosinusitis: Relationships to disease phenotypes, pathogenesis, clinical findings, and treatment approaches. Allergy 2022, 77, 812–826. [Google Scholar] [CrossRef]
- Yip, J.; Monteiro, E.; Chan, Y. Endotypes of chronic rhinosinusitis. Curr. Opin. Otolaryngol. Head Neck Surg. 2019, 27, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Kariyawasam, H.H.; James, L.K.; Gane, S.B. Dupilumab: Clinical Efficacy of Blocking IL-4/IL-13 Signalling in Chronic Rhinosinusitis with Nasal Polyps. Drug Des. Dev. Ther. 2020, 14, 1757–1769. [Google Scholar] [CrossRef]
- Morse, J.C.; Miller, C.; Senior, B. Management of Chronic Rhinosinusitis with Nasal Polyposis in the Era of Biologics. J. Asthma Allergy 2021, 14, 873–882. [Google Scholar] [CrossRef]
- Rabe, K.F.; Nair, P.; Brusselle, G.; Maspero, J.F.; Castro, M.; Sher, L.; Zhu, H.; Hamilton, J.D.; Swanson, B.N.; Khan, A.; et al. Efficacy and Safety of Dupilumab in Glucocorticoid-Dependent Severe Asthma. N. Engl. J. Med. 2018, 378, 2475–2485. [Google Scholar] [CrossRef]
- Laidlaw, T.M.; Bachert, C.; Amin, N.; Desrosiers, M.; Hellings, P.W.; Mullol, J.; Maspero, J.F.; Gevaert, P.; Zhang, M.; Mao, X.; et al. Dupilumab improves upper and lower airway disease control in chronic rhinosinusitis with nasal polyps and asthma. Ann. Allergy Asthma Immunol. 2021, 126, 584–592. [Google Scholar] [CrossRef]
- Junttila, I.S. Tuning the Cytokine Responses: An Update on Interleukin (IL)-4 and IL-13 Receptor Complexes. Front. Immunol. 2018, 9, 888. [Google Scholar] [CrossRef] [PubMed]
- Napolitano, M.; Maffei, M.; Patruno, C.; Leone, C.A.; Di Guida, A.; Potestio, L.; Scalvenzi, M.; Fabbrocini, G. Dupilumab effectiveness for the treatment of patients with concomitant atopic dermatitis and chronic rhinosinusitis with nasal polyposis. Dermatol. Ther. 2021, 34, e15120. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency Dupixent®, Summary of Product Characteristics. Available online: https://ec.europa.eu/health/documents/communityregister/2019/20190506144541/anx_144541_en.pdf (accessed on 1 March 2023).
- Bachert, C.; Han, J.K.; Wagenmann, M.; Hosemann, W.; Lee, S.E.; Backer, V.; Mullol, J.; Gevaert, P.; Klimek, L.; Prokopakis, E.; et al. EUFOREA expert board meeting on uncontrolled severe chronic rhinosinusitis with nasal polyps (CRSwNP) and biologics: Definitions and management. J. Allergy Clin. Immunol. 2021, 147, 29–36. [Google Scholar] [CrossRef]
- Bachert, C.; Bhattacharyya, N.; Desrosiers, M.; Khan, A.H. Burden of Disease in Chronic Rhinosinusitis with Nasal Polyps. J. Asthma Allergy 2021, 14, 127–134. [Google Scholar] [CrossRef]
- Pendolino, A.L.; Scarpa, B.; Ottaviano, G. Relationship Between Nasal Cycle, Nasal Symptoms and Nasal Cytology. Am. J. Rhinol. Allergy 2019, 33, 644–649. [Google Scholar] [CrossRef] [PubMed]
- Kilty, S.J.; Lasso, A. Canadian real-world study of access and clinical results using dupilumab for chronic rhinosinusitis with polyps. J. Otolaryngol.—Head Neck Surg. 2022, 51, 17. [Google Scholar] [CrossRef]
- Grose, E.; Li, A.Y.; Lee, J.M. Clinical outcomes of dupilumab therapy in chronic rhinosinusitis with nasal polyps in a Canadian tertiary care rhinology practice. Allergy Asthma Clin. Immunol. 2023, 19, 26. [Google Scholar] [CrossRef]
- Bassiouni, A.; Naidoo, Y.; Wormald, P.-J. When FESS fails: The inflammatory load hypothesis in refractory chronic rhinosinusitis. Laryngoscope 2012, 122, 460–466. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.; Bachert, C.; Mullol, J.; Bjermer, L.; Bousquet, J.; Canonica, G.W.; Deneyer, L.; Desrosiers, M.; Diamant, Z.; et al. EUFOREA consensus on biologics for CRSwNP with or without asthma. Allergy Eur. J. Allergy Clin. Immunol. 2019, 74, 2312–2319. [Google Scholar] [CrossRef]
- Schleimer, R.P. Immunopathogenesis of Chronic Rhinosinusitis and Nasal Polyposis. Annu. Rev. Pathol. Mech. Dis. 2017, 12, 331–357. [Google Scholar] [CrossRef] [PubMed]
- Jansen, F.; Becker, B.; Eden, J.K.; Breda, P.C.; Hot, A.; Oqueka, T.; Betz, C.S.; Hoffmann, A.S. Dupilumab (Dupixent®) tends to be an effective therapy for uncontrolled severe chronic rhinosinusitis with nasal polyps: Real data of a single-centered, retrospective single-arm longitudinal study from a university hospital in Germany. Eur. Arch. Oto-Rhino-Laryngol. 2023, 280, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Wechsler, M.E.; Klion, A.D.; Paggiaro, P.; Nair, P.; Staumont-Salle, D.; Radwan, A.; Johnson, R.R.; Kapoor, U.; Khokhar, F.A.; Daizadeh, N.; et al. Effect of Dupilumab on Blood Eosinophil Counts in Patients with Asthma, Chronic Rhinosinusitis with Nasal Polyps, Atopic Dermatitis, or Eosinophilic Esophagitis. J. Allergy Clin. Immunol. Pract. 2022, 10, 2695–2709. [Google Scholar] [CrossRef]
- Aldajani, A.; Alroqi, A.; Alromaih, S.; Aloulah, M.O.; Alsaleh, S. Adverse events of biological therapy in chronic rhinosinusitis with nasal polyps: A systematic review. Am. J. Otolaryngol. 2022, 43, 103615. [Google Scholar] [CrossRef] [PubMed]
- Chrétien, B.; Dolladille, C.; Alexandre, J.; Fedrizzi, S.; Lelong-Boulouard, V.; Lambert, J.C.; Ezine, E. Dupilumab-associated arthralgia: An observational retrospective study in VigiBase®. Br. J. Dermatol. 2021, 185, 464–465. [Google Scholar] [CrossRef]
- Akinlade, B.; Guttman-Yassky, E.; Bruin-Weller, M.; Simpson, E.L.; Blauvelt, A.; Cork, M.J.; Prens, E.; Asbell, P.; Akpek, E.; Corren, J.; et al. Conjunctivitis in dupilumab clinical trials. Br. J. Dermatol. 2019, 181, 459–473. [Google Scholar] [CrossRef]
- Nitro, L.; Bulfamante, A.M.; Rosso, C.; Saibene, A.M.; Arnone, F.; Felisati, G.; Pipolo, C. Adverse effects of dupilumab in chronic rhinosinusitis with nasal polyps. Case report and narrative review. Acta Otorhinolaryngol. Ital. 2022, 42, 199–204. [Google Scholar] [CrossRef]
- Chromy, D.; Bartosik, T.; Brkic, F.F.; Quint, T.; Tu, A.; Eckl-Dorna, J.; Schneider, S.; Bangert, C. Dupilumab-induced skin-associated side effects in patients with chronic rhinosinusitis with nasal polyposis. J. Dermatol. 2023, 50, 89–93. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Cicala, G.; Cutroneo, P.M.; Gerratana, E.; Palleria, C.; De Sarro, C.; Vero, A.; Iannone, L.; Manti, A.; Russo, E.; et al. Safety profile of biologics used in rheumatology: An italian prospective pharmacovigilance study. J. Clin. Med. 2020, 9, 1227. [Google Scholar] [CrossRef]
- Barbieri, M.A.; Viola, A.; Cicala, G.; Spina, E.; Fries, W. Effectiveness and Safety Profiles of Biological Therapies in Inflammatory Bowel Disease: Real Life Data from an Active Pharmacovigilance Project. Biomedicines 2022, 10, 3280. [Google Scholar] [CrossRef]
- Roberti, R.; Iannone, L.F.; Palleria, C.; De Sarro, C.; Spagnuolo, R.; Barbieri, M.A.; Vero, A.; Manti, A.; Pisana, V.; Fries, W.; et al. Safety profiles of biologic agents for inflammatory bowel diseases: A prospective pharmacovigilance study in Southern Italy. Curr. Med. Res. Opin. 2020, 36, 1457–1463. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Post-Surgical (n = 46) | Naïve (n = 23) | p Value | All (n = 63) | |
|---|---|---|---|---|
| Sex, male n (%) | 34 (73.9) | 9 (39.1) | 0.112 | 43 (68.3) |
| Age, years median (Q1–Q3) | 63 (49–69) | 53.5 (45.3–58.3) | 0.074 | 54 (46–64) |
| Smokers, n (%) | 5 (10.9) | 10 (43.5) | 0.005 | 15 (23.8) |
| Allergic conditions, n (%) | 27 (58.7) | 15 (65.2) | 0.794 | 42 (66.7) |
| Concomitant asthma, n (%) | 22 (47.8) | 12 (52.2) | 0.932 | 34 (54.0) |
| SNOT-22, median (Q1–Q3) | 74.5 (57.8–78.3) | 63 (56.5–74.5) | 0.224 | 70 (58–78) |
| NPS, median (Q1–Q3) | 6 (5–7) | 5 (5–6) | 0.361 | 6 (5–7) |
| Blood eosinophil count, median (Q1–Q3) | 0.5 (0.4–0.8) | 0.8 (0.5–0.9) | 0.077 | 0.6 (0.4–0.8) |
| Previous corticosteroid treatment, n (%) | 46 (100) | 23 (100) | - | 63 (100) |
| Duration of therapy, median (Q1–Q3) | 12 (12–18) | 12 (12–15) | 0.811 | 12 (6–18) |
| 6th Month vs. Baseline | p Value | 12th Month vs. Baseline | p Value | |
|---|---|---|---|---|
| SNOT-22, median (Q1–Q3) | −37 | <0.001 | −50 | <0.001 |
| NPS, median (Q1–Q3) | −3 | <0.001 | −4 | <0.001 |
| Blood eosinophil count, median (Q1–Q3) | +0.1 | <0.001 | +0.4 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galletti, C.; Barbieri, M.A.; Ciodaro, F.; Freni, F.; Galletti, F.; Spina, E.; Galletti, B. Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care. Pharmaceuticals 2023, 16, 630. https://doi.org/10.3390/ph16040630
Galletti C, Barbieri MA, Ciodaro F, Freni F, Galletti F, Spina E, Galletti B. Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care. Pharmaceuticals. 2023; 16(4):630. https://doi.org/10.3390/ph16040630
Chicago/Turabian StyleGalletti, Cosimo, Maria Antonietta Barbieri, Francesco Ciodaro, Francesco Freni, Francesco Galletti, Edoardo Spina, and Bruno Galletti. 2023. "Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care" Pharmaceuticals 16, no. 4: 630. https://doi.org/10.3390/ph16040630
APA StyleGalletti, C., Barbieri, M. A., Ciodaro, F., Freni, F., Galletti, F., Spina, E., & Galletti, B. (2023). Effectiveness and Safety Profile of Dupilumab in Chronic Rhinosinusitis with Nasal Polyps: Real-Life Data in Tertiary Care. Pharmaceuticals, 16(4), 630. https://doi.org/10.3390/ph16040630