
Medication and ECG Patterns That May Hinder SPECT Myocardial Perfusion Scans

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. ECG Alterations
2.1. Left Bundle Branch Block (LBBB)
2.2. Atrioventricular Block (AVB)
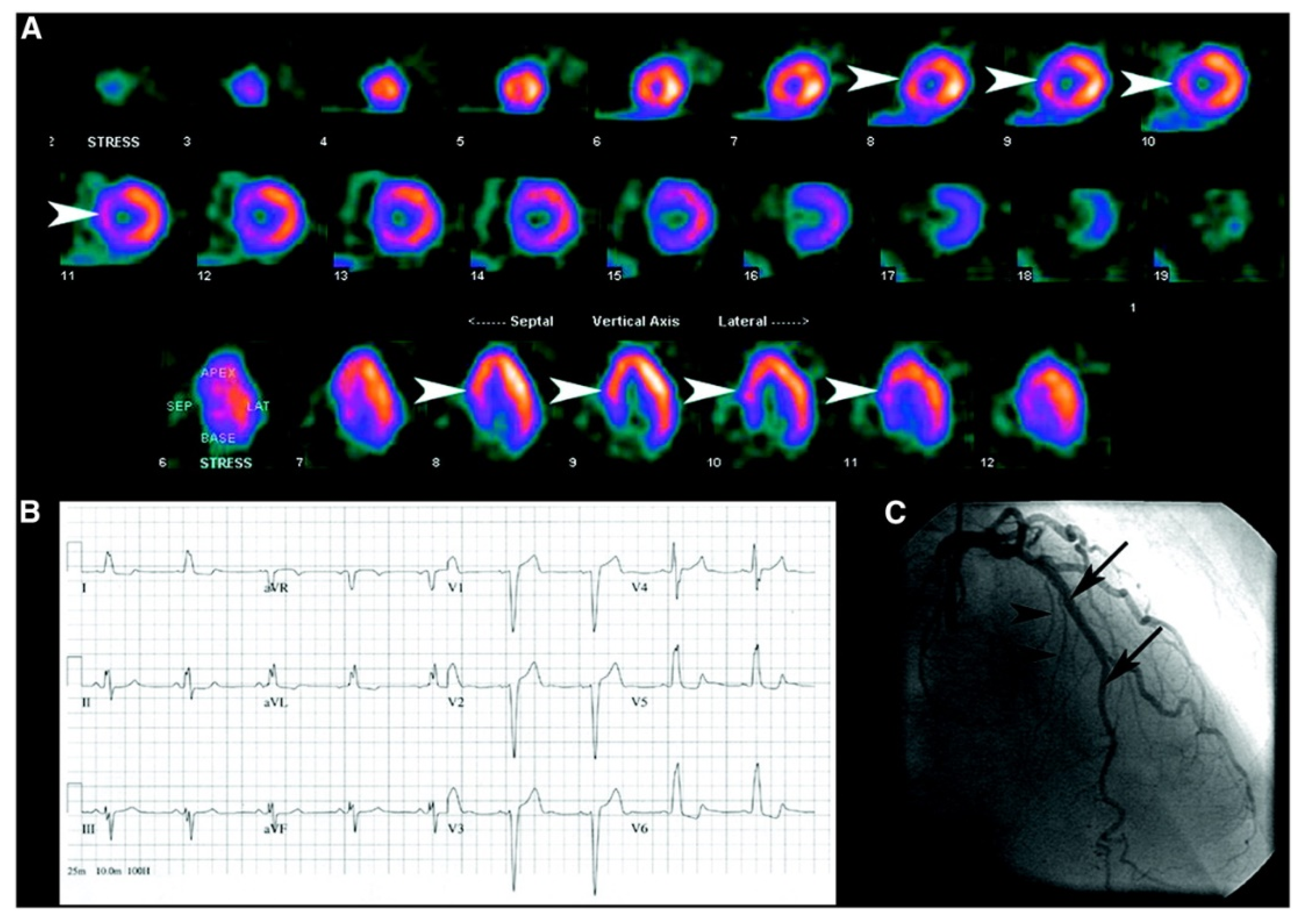
2.3. Balanced Ischemia
3. Medication
3.1. Calcium Channel Blockers (CCB)
3.2. Beta-Blockers (BB)
3.3. Adenosine
3.4. Dobutamine
3.5. Nitroglicerine
4. Other SPECT Affecting Conditions
4.1. Hypertrophic Cardiomiopathy
4.2. Dextrocardia
4.3. Attenuation Correction
5. Future Perspectives
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kochanek, K.D.; Xu, J.; Arias, E. Mortality in the United States, 2019; NCHS data brief, no 395; National Center for Health Statistics: Hyattsville, MD, USA, 2020.
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart disease and stroke statistics-2021 update: A report from the american heart association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Odden, M.C.; Coxson, P.G.; Moran, A.; Lightwood, J.M.; Goldman, L.; Bibbins-Domingo, K. The impact of the aging population on coronary heart disease in the United States. Am. J. Med. 2011, 124, 827–833.e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, H.; Much, A.A.; Maor, E.; Asher, E.; Younis, A.; Xu, Y.; Lu, Y.; Liu, X.; Shu, J.; Bragazzi, N.L. Global, regional, and national burden of ischemic heart disease and its attributable risk factors, 1990–2017: Results from the global Burden of Disease Study 2017. Eur. Heart J. Qual. Care Clin. Outcomes 2022, 8, 50–60. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Aminorroaya, A.; Yoosefi, M.; Rezaei, N.; Shabani, M.; Mohammadi, E.; Fattahi, N.; Azadnajafabad, S.; Nasserinejad, M.; Rezaei, N.; Naderimagham, S.; et al. Global, regional, and national quality of care of ischaemic heart disease from 1990 to 2017: A systematic analysis for the global burden of disease study 2017. Eur. J. Prev. Cardiol. 2021, 29, 371–379. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino RBSr Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart Study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American college of cardiology/american heart association task force on practice guidelines. J. Am. Coll. Cardiol. 2014, 63, 2935–2959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar]
- Rosendorff, C.; Black, H.R.; Cannon, C.P.; Gersh, B.J.; Gore, J.; Izzo, J.L., Jr.; Kaplan, N.M.; O’Connor, C.M.; O’Gara, P.T.; Oparil, S.; et al. Treatment of hypertension in the prevention and management of ischemic heart disease: A scientific statement from the american heart association council for high blood pressure research and the councils on clinical cardiology and epidemiology and prevention. Circulation 2007, 115, 2761–2788. [Google Scholar] [PubMed] [Green Version]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: A report of the american college of cardiology/american heart association task force on clinical practice guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef]
- Bedetti, G.; Pasanisi, E.M.; Pizzi, C.; Turchetti, G.; Loré, C. Economic analysis including long-term risks and costs of alternative diagnostic strategies to evaluate patients with chest pain. Cardiovasc. Ultrasound 2008, 6, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, J.J.; Alzahrani, T. Myocardial Perfusion Scan. [Updated 8 August 2022]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Gaudio, C.; Mirabelli, F.; Pelliccia, F.; Francone, M.; Tanzilli, G.; Di Michele, S.; Leonetti, S.; De Vincentis, G.; Carbone, I.; Mangieri, E.; et al. Early detection of coronary artery disease by 64-slice multidetector computed tomography in asymptomatic hypertensive high-risk patients. Int. J. Cardiol. 2009, 135, 280–286. [Google Scholar] [CrossRef]
- Soman, P.; Parsons, A.; Lahiri, N.; Lahiri, A. The prognostic value of a normal Tc-99m sestamibi SPECT study in suspected coronary artery disease. J. Nucl. Cardiol. 1999, 6, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Iskander, S.; Iskandrian, A.E. Risk assessment using single-photon emission computed tomographic technetium-99m sestamibi imaging. J. Am. Coll. Cardiol. 1998, 32, 57–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallaj, S.; Mirza-Aghazadeh-Attari, M.; Arasteh, A.; Ghorbani, A.; Lee, D.; Jadidi-Niaragh, F. Adenosine: The common target between cancer immunotherapy and glaucoma in the eye. Life Sci. 2021, 282, 119796. [Google Scholar] [CrossRef] [PubMed]
- Leppo, J.A. Comparison of pharmacologic stress agents. J. Nucl. Cardiol. 1996, 3, S22–S26. [Google Scholar] [CrossRef] [PubMed]
- Verberne, H.J.; Acampa, W.; Anagnostopoulos, C.; Ballinger, J.; Bengel, F.; De Bondt, P.; Buechel, R.R.; Cuocolo, A.; van Eck-Smit, B.L.F.; Flotats, A.; et al. EANM procedural guidelines for radionuclide myocardial perfusion imaging with SPECT and SPECT/CT: 2015 revision. Eur. J. Nucl. Med. 2015, 42, 1929–1940. [Google Scholar] [CrossRef] [Green Version]
- Francia, P.; Balla, C.; Paneni, F.; Volpe, M. Left bundle-branch block--pathophysiology, prognosis, and clinical management. Clin. Cardiol. 2007, 30, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Surawicz, B.; Childers, R.; Deal, B.J.; Gettes, L.S.; Bailey, J.J.; Gorgels, A.; Hancock, E.W.; Josephson, M.; Kligfield, P.; Kors, J.A.; et al. AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part III: Intraventricular conduction distur-bances: A scientific statement from the american heart association electrocardiography and arrhythmias committee, council on clinical cardiology; the american college of cardiology foundation; and the heart rhythm society. endorsed by the international society for computerized electrocardiology. J. Am. Coll. Cardiol. 2009, 53, 976–981. [Google Scholar]
- Tandogan, I.; Yetkin, E.; Ileri, M.; Ortapamuk, H.; Yanik, A.; Cehreli, S.; Duru, E. Diagnosis of coronary artery disease with Tl-201 SPECT in patients with left bundle branch block: Importance of alternative interpretation approaches for left anterior descending coronary lesions. Angiology 2001, 52, 103–108. [Google Scholar] [CrossRef]
- Hirzel, H.O.; Senn, M.; Nuesch, K.; Buettner, C.; Pfeiffer, A.; Hess, O.M.; Krayenbuehl, H.P. Thallium-201 scintigraphy in complete left bundle branch block. Am. J. Cardiol. 1984, 53, 764–769. [Google Scholar] [CrossRef]
- Larcos, G.; Gibbons, R.J.; Brown, M.L. Diagnostic accuracy of exercise thallium-201 single-photon emission computed tomography in patients with left bundle branch block. Am. J. Cardiol. 1991, 68, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Vaduganathan, P.; He, Z.X.; Raghavan, C.; Mahmarian, J.J.; Verani, M.S. Detection of left anterior descending coronary artery stenosis in patients with left bundle branch block: Exercise, adenosine or dobutamine imaging? J. Am. Coll. Cardiol. 1996, 28, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Burrell, S.; MacDonald, A. Artifacts and Pitfalls in Myocardial Perfusion Imaging. J. Nucl. Med. Technol. 2006, 34, 193–211. [Google Scholar] [PubMed]
- Kashou, A.H.; Goyal, A.; Nguyen, T.; Chhabra, L. Atrioventricular Block. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Li, X.; Xue, Y.; Wu, H. A Case of Atrioventricular Block Potentially Associated with Right Coronary Artery Lesion and Ticagrelor Therapy Mediated by the Increasing Adenosine Plasma Concentration. Case Rep. Vasc. Med. 2018, 2018, 9385017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Batra, A.S.; Balaji, S. Fetal arrhythmias: Diagnosis and management. Indian Pacing Electrophysiol. J. 2019, 19, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Saadi, M.; Tagliari, A.P.; Danzmann, L.C.; Bartholomay, E.; Kochi, A.N.; Saadi, E.K. Update in Heart Rhythm Abnormalities and Indications for Pacemaker After Transcatheter Aortic Valve Implantation. Braz. J. Cardiovasc. Surg. 2018, 33, 286–290. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Furlanello, F.; Lupo, P.; Foresti, S.; De Ambroggi, G.; Epicoco, G.; Semprini, L.; Fundaliotis, A.; Cappato, R. Clinical and electrocardiographic features of complete heart block after blunt cardiac injury: A systematic review of the literature. Heart Rhythm. 2017, 14, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- Mangi, M.A.; Jones, W.M.; Mansour, M.K.; Napier, L. Atrioventricular Block Second-Degree. [Updated 22 August 2022]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kashou, A.H.; Goyal, A.; Nguyen, T.; Ahmed, I.; Chhabra, L. Atrioventricular Block. 24 February 2023. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Andrikopoulou, E.; Morgan, C.J.; Brice, L.; Bajaj, N.S.; Doppalapudi, H.; Iskandrian, A.E.; Hage, F.G. Incidence of atrioventricular block with vasodilator stress SPECT: A meta-analysis. J. Nucl. Cardiol. 2019, 26, 616–628. [Google Scholar] [CrossRef]
- Alkoutami, G.S.; Reeves, W.C.; Movahed, A. The safety of adenosine pharmacologic stress testing in patients with first-degree atrioventricular block in the presence and absence of atrioventricular blocking medications. J. Nucl. Cardiol. 1999, 6, 495–497. [Google Scholar] [CrossRef] [PubMed]
- Aziz, E.F.; Javed, F.; Alviar, C.L.; Herzog, E. Triple vessel coronary artery disease presenting as a markedly positive stress electrocardiographic test and a negative SPECT-TL scintigram: A case of balanced ischemia. Heart Int. 2011, 6, e22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lesser, J.R.; Bae, R.; Flygenring, B.; Sharkey, S.S.; Lindberg, J.; Schwartz, R.S. Balanced myocardial ischaemia: A case of “normal” stress Tc99 sestamibi scan and diagnosis. Heart 2005, 91, e53. [Google Scholar] [CrossRef] [Green Version]
- Robertson, R.M.; Robertson, D. Drugs used for the treatment of myocardial ischemia. In Goodman and Gilman’s The Parmacological Basis of Therapeutics, 9th ed.; Hardman, J.G., Goodman Gilman, A., Limbird, L.E., Eds.; McGraw-Hill: New York, NY, USA, 1996; pp. 759–769. [Google Scholar]
- Opie, L.H. Clinical Use of Calcium Channel Antagonist Drugs; Kluver Academic Publishers: Boston, MA, USA, 1990; Volume 1. [Google Scholar]
- Grossman, E.; Messerli, F.H. Calcium antagonists. Prog. Cardiovasc. Dis. 2004, 47, 34. [Google Scholar] [CrossRef] [PubMed]
- Tillmanns, H.; Neumann, F.J.; Parekh, N.; Waas, W.; Möller, P.; Zimmermann, R.; Steinhausen, M.; Köbler, W. Calcium antagonists and myocardial microperfusion. Drugs 1991, 42 (Suppl. S1), 1–6. [Google Scholar] [CrossRef]
- Park, S.W.; Tang, X.L.; Qiu, Y.; Sun, J.Z.; Bolli, R. Nisoldipine attenuates myocardial stunning induced by multiple coronary occlusions in conscious pigs and this effect is independent of changes in hemodynamics or coronary blood flow. J. Mol. Cell. Cardiol. 1996, 28, 655–666. [Google Scholar] [CrossRef]
- Bugiardini, R.; Manfrini, O.; Pizzi, C.; Fontana, F.; Morgagni, G. Endothelial Function Predicts Future Development of Coronary Artery Disease: A Study of Women with Chest Pain and Normal Coronary Angiograms. Circ. J. Am. Heart Assoc. 2004, 109, 2518–2523. [Google Scholar] [CrossRef] [Green Version]
- Lanza, G.A.; Morrone, D.; Pizzi, C.; Tritto, I.; Bergamaschi, L.; De Vita, A.; Villano, A.; Crea, F. Diagnostic approach for coronary microvascular dysfunction in patients with chest pain and no obstructive coronary artery disease. Trends Cardiovasc. Med. 2021, 32, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Stegaru, B.; Loose, R.; Keller, H.; Buss, J.; Wetzel, E. Effects of long-term treatment with 120 mg of sustained-release isosorbide dinitrate and 60 mg of sustained-release nifedipine on myocardial perfusion. Am. J. Cardiol. 1988, 61, 74E–77E. [Google Scholar] [CrossRef]
- Eldridge, J.E.; Burdick, D.C.; Jones, R.H.; Hossack, K.F. Comparison of nitroglycerin patches and nifedipine. J. Cardiovasc. Pharmacol. 1987, 10, 315–319. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, J.; Ohsawa, H.; Uchi, T.; Iida, M.; Nakano, H.; Hosoi, H.; Morishita, T.; Yabe, Y.; Koyama, N.; Komatsu, H. Study of the efficacy of nicorandil in patients with ischaemic heart disease using ExerciseT1-201 myocardial tomography. Eur. J. Clin. Pharmacol. 1993, 44, 211–217. [Google Scholar] [CrossRef]
- Guth, B.D.; Heusch, G.; Seitelberger, R.; Ross, J., Jr. Mechanism of beneficial effect of beta-adrenergic blockade on exercise-induced myocardial ischemia in conscious dogs. Circ. Res. 1987, 60, 738–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koepfli, P.; Wyss, C.A.; Namdar, M.; Klainguti, M.; von Schulthess, G.K.; Lüscher, T.F.; Kaufmann, P.A. Beta-adrenergic blockade and myocardial perfusion in coronary artery disease: Differential effects in stenotic versus remote myocardial segments. J. Nucl. Med. 2004, 45, 1626–1631. [Google Scholar] [PubMed]
- Gorre, F.; Vandekerckhove, H. Beta-blockers: Focus on mechanism of action. Which beta-blocker, when and why? Acta Cardiol. 2010, 65, 565–570. [Google Scholar] [CrossRef]
- Rehsia, N.S.; Dhalla, N.S. Mechanisms of the beneficial effects of beta-adrenoceptor antagonists in congestive heart failure. Exp. Clin. Cardiol. 2010, 15, e86–e95. [Google Scholar]
- Machackova, J.; Sanganalmath, S.K.; Elimban, V.; Dhalla, N.S. β-adrenergic blockade attenuates cardiac dysfunction and myofibrillar remodelling in congestive heart failure. J. Cell. Mol. Med. 2011, 15, 545–554. [Google Scholar] [CrossRef] [Green Version]
- Hockings, B.; Saltissi, S.; Croft, D.N.; Webb-Peploe, M.M. Effect of beta adrenergic blockade on thallium-201 myocardial perfusion imaging. Br. Heart J. 1983, 49, 83–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, G.J.; Henkin, R.E.; Scanlon, P.J. Beta blockers and the sensitivity of the thallium treadmill test. Chest 1987, 92, 486–487. [Google Scholar] [CrossRef] [Green Version]
- Bridges, A.B.; Kennedy, N.; McNeill, G.P.; Cook, B.; Pringle, T.H. The effect of atenolol on dipyridamole 201Tl myocardial perfusion tomography in patients with coronary artery disease. Nucl. Med. Commun. 1992, 13, 41–46. [Google Scholar] [CrossRef]
- Taillefer, R.; Ahlberg, A.W.; Masood, Y.; White, C.; Lamargese, I.; Mather, J.F.; McGill, C.C.; Heller, G.V. Acute beta-blockade reduces the extent and severity of myocardial perfusion defects with dipyridamole Tc-99m sestamibi SPECT imaging. J. Am. Coll. Cardiol. 2003, 42, 1475–1483. [Google Scholar] [CrossRef] [Green Version]
- Samsel, M.; Dzierzbicka, K.; Trzonkowski, P. Adenosine, its analogues and conjugates. Postepy Hig. Med. Dosw. 2013, 67, 1189–1203. [Google Scholar] [CrossRef]
- Mosqueda-Garcia, R. Adenosine as a therapeutic agent. Clin. Investig. Med. 1992, 15, 445–455. [Google Scholar]
- Rankin, A.C.; Brooks, R.; Ruskin, J.N.; McGovern, B.A. Adenosine and the treatment of supraventricular tachycardia. Am. J. Med. 1992, 92, 655–664. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, G.J.; Dorfman, T.A.; Iskandrian, A.E. The effects of medications on myocardial perfusion. J. Am. Coll. Cardiol. 2008, 52, 401–416. [Google Scholar] [CrossRef] [Green Version]
- Bokhari, S.; Ficaro, E.P.; McCallister, B.D., Jr. Adenosine stress protocols for myocardial perfusion imaging. J. Nucl. Cardiol. 2007, 14, 415–416. [Google Scholar] [CrossRef]
- Pennell, D.J.; Mavrogeni, S.I.; Forbat, S.M.; Karwatowski, S.P.; Underwood, S.R. Adenosine combined with dynamic exercise for myocardial perfusion imaging. J. Am. Coll. Cardiol. 1995, 25, 1300–1309. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, A.; Palmer, E.L.; Scott, J.A.; Abraham, S.A.; Fischman, A.J.; Force, T.L.; Newell, J.B.; Rabito, C.A.; Zervos, G.D.; Yasuda, T. Complications of exercise and pharmacologic stress tests: Differences in younger and elderly patients. J. Nucl. Cardiol. 1999, 6, 612–619. [Google Scholar] [CrossRef]
- McNeill, A.J.; Fioretti, P.M.; el-Said, S.M.; Salustri, A.; Forster, T.; Roelandt, J.R. Enhanced sensitivity for detection of coronary artery disease by addition of atropine to dobutamine stress echocardiography. Am. J. Cardiol. 1992, 70, 41–46. [Google Scholar] [CrossRef]
- Elhendy, A.; Valkema, R.; Van Domburg, R.T.; Bax, J.J.; Nierop, P.R.; Cornel, J.; Geleijnse, M.L.; Reijs, A.E.; Krenning, E.P.; Roelandt, J.R. Safety of dobutamine-atropine stress myocardial perfusion scintigraphy. J. Nucl. Med. 1998, 39, 1662–1666. [Google Scholar]
- Alhayek, S.; Preuss, C.V. Beta 1 Receptors. 8 August 2022. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kislitsina, O.N.; Rich, J.D.; Wilcox, J.E.; Pham, D.T.; Churyla, A.; Vorovich, E.B.; Ghafourian, K.; Yancy, C.W. Shock—Classification and Pathophysiological Principles of Therapeutics. Curr. Cardiol. Rev. 2019, 15, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Katzung, B.; Chatterjee, K. Basic and Clinical Pharmacology, 7th ed.; Appleton and Lange: Stamford, CT, USA, 1998. [Google Scholar]
- Habazettl, H.; Vollmar, B.; Christ, M.; Baier, H.; Conzen, P.F.; Peter, K. Heterogeneous microvascular coronary vasodilation by adenosine and nitroglycerin in dogs. J. Appl. Physiol. 1994, 76, 1951–1960. [Google Scholar] [CrossRef]
- Feldman, R.L.; Marx, J.D.; Pepine, C.J.; Conti, C.R. Analysis of coronary responses to various doses of intracoronary nitroglycerin. Circulation 1982, 66, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Kanatsuka, H.; Eastham, C.L.; Marcus, M.L.; Lamping, K.G. Effects of nitroglycerin on the coronary microcirculation in normal and ischemic myocardium. J. Cardiovasc. Pharmacol. 1992, 19, 755–763. [Google Scholar] [PubMed]
- Aoki, M.; Sakai, K.; Koyanagi, S.; Takeshita, A.; Nakamura, M. Effect of nitroglycerin on coronary collateral function during exercise evaluated by quantitative analysis of thallium-201 single photon emission computed tomography. Am. Heart J. 1991, 121, 1361–1366. [Google Scholar] [CrossRef]
- Göller, V.; Clausen, M.; Henze, E.; Giesler, M.; Schmidt, A.; Kochs, M.; Hombach, V. Reduction of exercise-induced myocardial perfusion defects by isosorbide-5-nitrate: Assessment using quantitative Tc-99m-MIBI-SPECT. Coron. Artery Dis. 1995, 6, 245–249. [Google Scholar]
- Lewin, H.C.; Hachamovitch, R.; Harris, A.G.; Williams, C.; Schmidt, J.; Harris, M.; Van Train, K.; Siligan, G.; Berman, D.S. Sustained reduction of exercise perfusion defect extent and severity with isosorbide mononitrate (Imdur) as demonstrated by means of technetium 99m sestamibi. J. Nucl. Cardiol. 2000, 7, 342–353. [Google Scholar] [CrossRef] [PubMed]
- Mahmarian, J.J.; Fenimore, N.L.; Marks, G.F.; Francis, M.J.; Morales-Ballejo, H.; Verani, M.S.; Pratt, C.M. Transdermal nitroglycerin patch therapy reduces the extent of exercise-induced myocardial ischemia: Results of a double-blind, placebo-controlled trial using quantitative thallium-201 tomography. J. Am. Coll. Cardiol. 1994, 24, 25–32. [Google Scholar] [CrossRef] [Green Version]
- Marian, A.J.; Braunwald, E. Hypertrophic Cardiomyopathy: Genetics, Pathogenesis, Clinical Manifestations, Diagnosis, and Therapy. Circ Res. 2017, 121, 749–770. [Google Scholar] [CrossRef]
- Evans, W.N.; Acherman, R.J.; Collazos, J.C.; Castillo, W.J.; Rollins, R.C.; Kip, K.T.; Restrepo, H. Dextrocardia: Practical clinical points and comments on terminology. Pediatr. Cardiol. 2010, 31, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Tanawuttiwat, T.; Vasaiwala, S.; Dia, M. Mirror mirror (ECG image of the month). Am. J. Med. 2010, 123, 34–36. [Google Scholar] [CrossRef]
- Mozayan, C.; Levis, J.T. ECG Diagnosis: Dextrocardia. Perm J. 2019, 23, 18–244. [Google Scholar] [CrossRef] [Green Version]
- Pawar, S.U.; Shetye, S.S.; Ghorpade, M.K.; Azeez Seena, R. Assessment of Myocardial Viability Using Nuclear Medicine Imaging in Dextrocardia. J. Nucl. Med. Technol. 2020, 48, 372–377. [Google Scholar] [CrossRef]
- Stathaki, M.; Koukouraki, S.; Papadaki, E.; Tsaroucha, A.; Karkavitsas, N. The Benefits of Prone SPECT Myocardial Perfusion Imaging in Reducing Both Artifact Defects and Patient Radiation Exposure. Arq. Bras. Cardiol. 2015, 105, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, A.; Koshida, K.; Matsubara, K. Effects of pacemaker, implantable cardioverter-defibrillator, and left ventricular leads on CT-based attenuation correction. J. Nucl. Med. Technol. 2014, 42, 37–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boschi, A.; Uccelli, L.; Marvelli, L.; Cittanti, C.; Giganti, M.; Martini, P. Technetium-99m Radiopharmaceuticals for Ideal Myocardial Perfusion Imaging: Lost and Found Opportunities. Molecules 2022, 27, 1188. [Google Scholar] [CrossRef]
- Gould, K.L.; Taegtmeyer, H. Myocardial ischemia, fluorodeoxyglucose, and severity of coronary artery stenosis: The complexities of Curr Cardiol Rep (2010) 12:170–178 177 metabolic remodeling in hibernating myocardium. Circulation 2004, 109, e167–e170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, D.; Ghanbarinia, A.; He, Z.X. Developing a new PET myocardial perfusion tracer. J. Nucl. Cardiol. 2009, 16, 689–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curley, D.; Lavin Plaza, B.; Shah, A.M.; Botnar, R.M. Molecular imaging of cardiac remodelling after myocardial infarction. Basic Res. Cardiol. 2018, 113, 10. [Google Scholar] [CrossRef] [Green Version]
- Maron, D.J.; Hochman, J.S.; Reynolds, H.R.; Bangalore, S.; O’Brien, S.M.; Boden, W.E.; Chaitman, B.R.; Senior, R.; López-Sendón, J.; Alexander, K.P.; et al. Initial Invasive or Conservative Strategy for Stable Coronary Disease. N. Engl. J. Med. 2020, 382, 1395–1407. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| ECG patterns | Left bundle branch block | LBBB, a common abnormality on electrocardiograms (ECGs), can complicate the interpretation of SPECT images due to its diverse effects on the structure, function, and blood supply to the heart muscle. This can result in the presence of anteroseptal and septal perfusion defects even in the absence of coronary artery disease (CAD). |
| Atrio-ventricular block | SPECT-MPI and AV block: A meta-analysis showed that the incidence of de novo AV block during pharmacologic stress single-photon emission computed tomography myocardial perfusion imaging (SPECT-MPI) with vasodilators including adenosine or regadenoson was around 4%, with a high-grade AV block incidence rate of approximately 2%. Adenosine was associated with a significantly higher incidence of AV block compared to regadenoson. Age and diabetes history were not associated with the rates of de novo AV block. | |
| Balanced ischemia | Balanced ischemia refers to a condition where there is an equal reduction in blood flow across all regions of the myocardium during stress. It is typically caused by factors including coronary artery disease, resulting in narrowed or blocked coronary arteries. SPECT imaging revealed a uniform decrease in radiotracer uptake throughout the myocardium, indicating impaired perfusion to the entire heart. | |
| Medication | Calcium channel blockers | CCBs exhibit vasodilatory effects on larger arterioles, reducing myocardial oxygen demand indirectly through decreased heart rate and contractility. They also directly decrease myocardial energy requirements and promote the utilization of free fatty acids in the ischemic myocardium, resulting in a reduced defect extent, severity, and ST-segment depression. |
| Beta-blockers | By exerting negative effects on heart rate, contractility, and renin release, beta-blockers improve angina symptoms and exhibit antiarrhythmic effects. Different types and doses of beta-blockers have been studied in exercise or dobutamine myocardial perfusion imaging (MPI), showing improvements in tracer activity and reductions in perfusion defect size and severity. Acute administration of beta-blockers before MPI has also been shown to decrease defect size and severity, while the chronic use of beta-blockers may not always result in significant differences in perfusion defect size and severity compared to the placebo. | |
| Adenosine | Adenosine causes vasodilation in the coronary system through A2a receptors, leading to increased perfusion. However, this effect is observed primarily in the non-stenotic vessel segments. Adenosine also induces a reflex increase in the heart rate and a slight decrease in the blood pressure. Importantly, adenosine stress testing rarely induces ischemia, except in cases of the coronary steal phenomenon. The duration of action of adenosine is short, and its side effects are reversible within minutes. Adenosine infusion should be administered slowly to prevent side effects such as transient AV block and bradycardias. | |
| Dobutamine | Dobutamine is a sympathomimetic agent that stimulates beta-1 adrenergic receptors, resulting in an increased heart rate, blood pressure, and contractility. It is commonly used in myocardial stress testing to evaluate myocardial viability and detect coronary artery disease (CAD). Dobutamine has a relatively short half-life, and its effects can be reversed with beta blockers if necessary. In addition to its diagnostic application, dobutamine is also used therapeutically in decompensated congestive heart failure to improve cardiac contractility and overall heart function | |
| Nitroglycerin | Nitroglycerin also reduces coronary vascular resistance and increases the diameter of large conduit vessels. The anti-ischemic effects of nitroglycerin may also be attributed to the dilation of the collateral vessels, redistributing the coronary flow from the normal to ischemic myocardium. Both the acute and chronic administration of nitrates have been shown to decrease the severity or size of ischemic perfusion in the culprit zone compared to the placebo or baseline without nitrates. | |
| Other conditions | Hypertrophic cardiomyopathy | Hypertrophic cardiomyopathy is an inherited condition characterized by the unexplained thickening of the left ventricle, particularly in the basal interventricular septum. Around one-third of patients experience obstruction of the left ventricular outflow tract at rest or under induced conditions. In SEPCT imaging, HCM can disrupt normal wall uptake, resulting in reduced perfusion in most areas of the left ventricle except for the septum. |
| Dextrocardia | Patients with dextrocardia show unique electrocardiogram (ECG) patterns, including right-axis deviation, inverted waves, and reversed QRS complexes. Reorienting precordial leads to a right-sided approach that allows for observing characteristic septal depolarization. Various imaging methods, such as changing rotation arc and prone positioning, have been suggested for SPECT acquisition to maintain heart visibility and reduce tissue attenuation. | |
| Implantable devices | The presence of pacemaker and LV leads in SPECT imaging may cause slight overestimation when using CT attenuation correction (CTAC). However, a study revealed minimal impact on SPECT findings, with only a 4% overestimation for the ICD leads. Lead diameter and material composition influence the level of overestimation. Overall, CTAC remained useful, and leads did not significantly affect the SPECT results, as clarified by the study. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sidrak, M.M.A.; De Feo, M.S.; Gorica, J.; Corica, F.; Conte, M.; Filippi, L.; De Vincentis, G.; Frantellizzi, V. Medication and ECG Patterns That May Hinder SPECT Myocardial Perfusion Scans. Pharmaceuticals 2023, 16, 854. https://doi.org/10.3390/ph16060854
Sidrak MMA, De Feo MS, Gorica J, Corica F, Conte M, Filippi L, De Vincentis G, Frantellizzi V. Medication and ECG Patterns That May Hinder SPECT Myocardial Perfusion Scans. Pharmaceuticals. 2023; 16(6):854. https://doi.org/10.3390/ph16060854
Chicago/Turabian StyleSidrak, Marko Magdi Abdou, Maria Silvia De Feo, Joana Gorica, Ferdinando Corica, Miriam Conte, Luca Filippi, Giuseppe De Vincentis, and Viviana Frantellizzi. 2023. "Medication and ECG Patterns That May Hinder SPECT Myocardial Perfusion Scans" Pharmaceuticals 16, no. 6: 854. https://doi.org/10.3390/ph16060854
APA StyleSidrak, M. M. A., De Feo, M. S., Gorica, J., Corica, F., Conte, M., Filippi, L., De Vincentis, G., & Frantellizzi, V. (2023). Medication and ECG Patterns That May Hinder SPECT Myocardial Perfusion Scans. Pharmaceuticals, 16(6), 854. https://doi.org/10.3390/ph16060854