

Impact of a Moderate CYP3A4 Inducer (Bosentan) on Lurbinectedin Pharmacokinetics and Safety in Patients with Advanced Solid Tumors: An Open-Label, Two-Way, Crossover, Phase Ib Drug–Drug Interaction Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
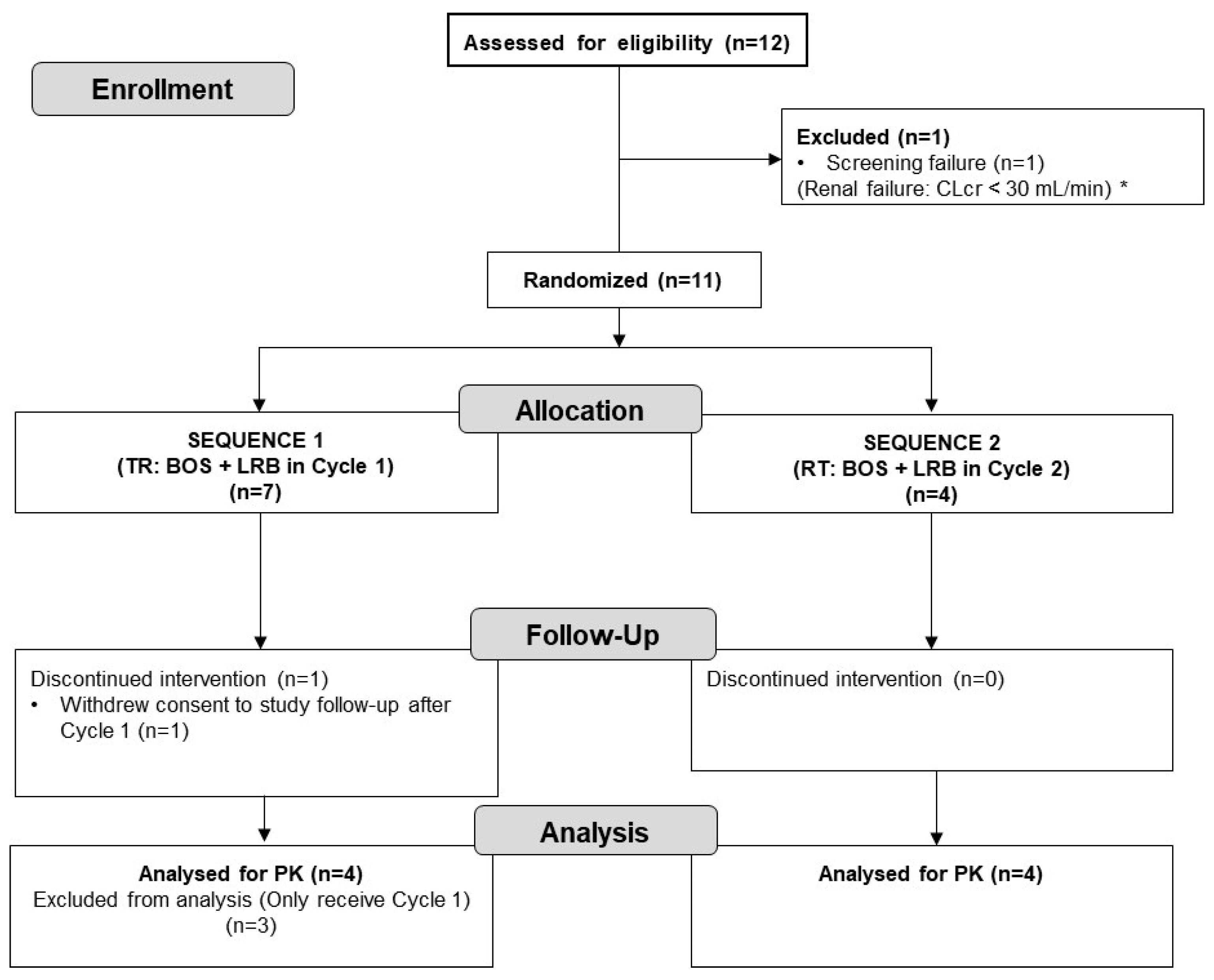
2.1. Patient Disposition and Baseline Characteristics
2.2. Pharmacokinetics
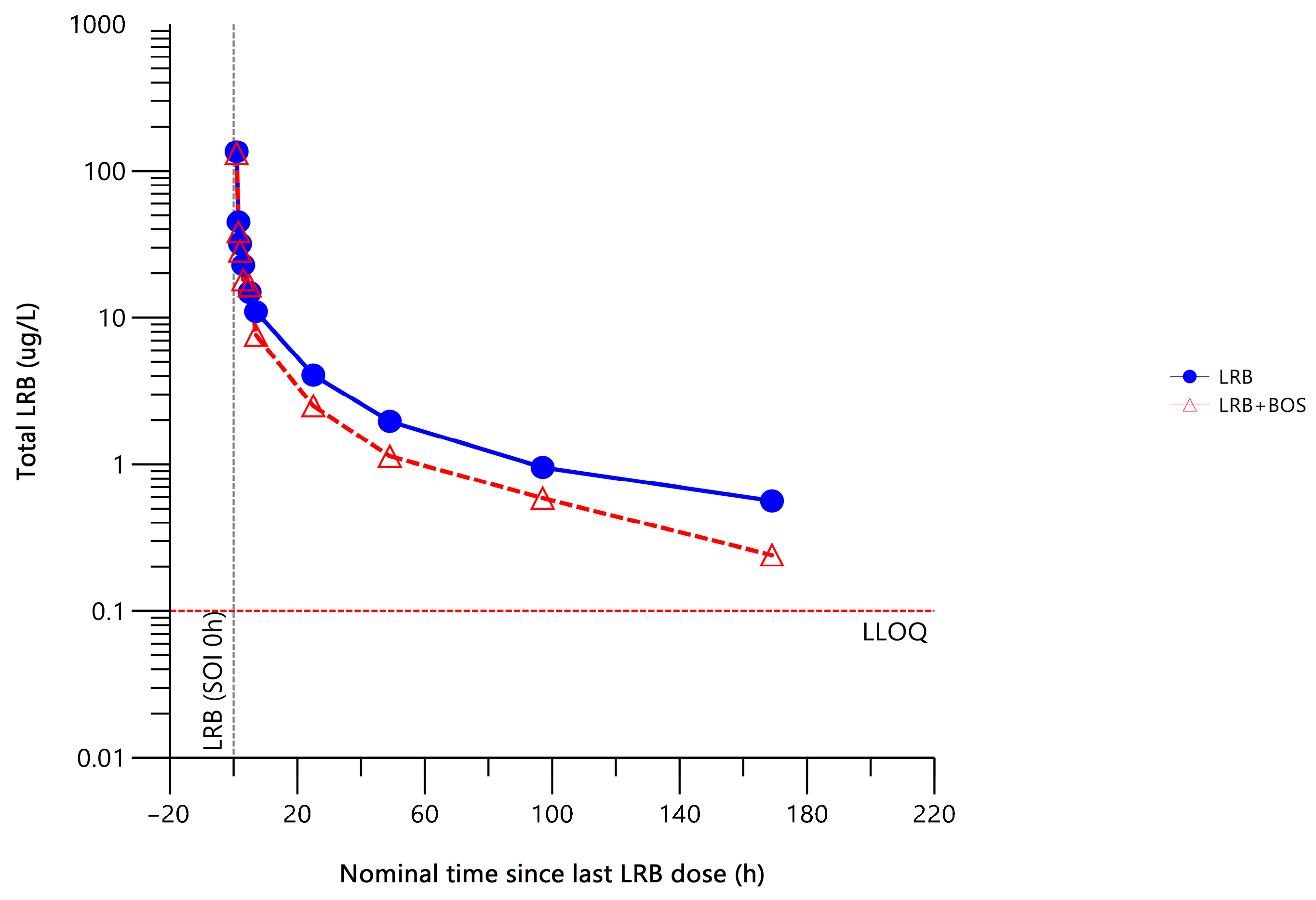
2.2.1. Total Plasma Lurbinectedin Pharmacokinetics
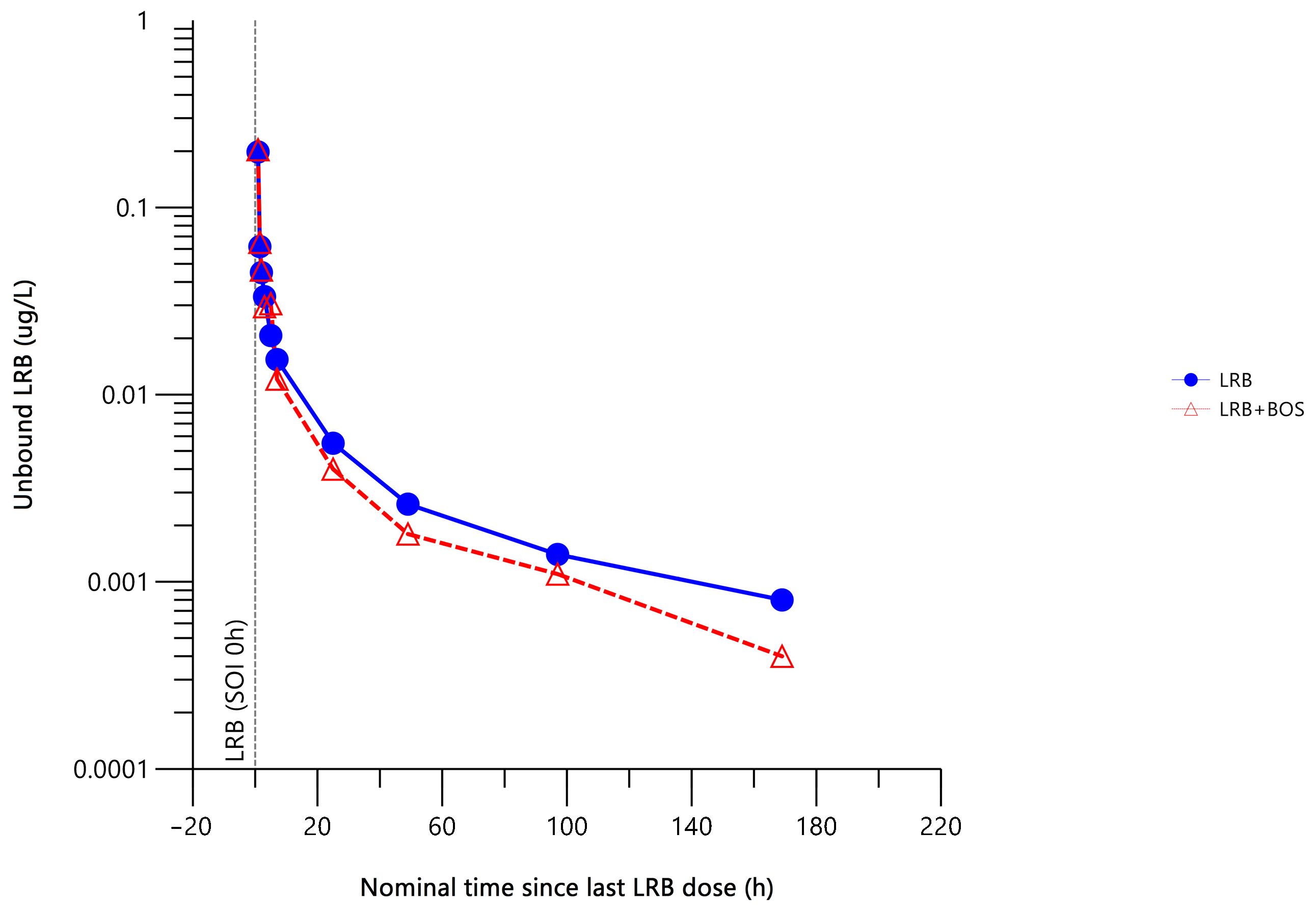
2.2.2. Unbound Plasma Lurbinectedin Pharmacokinetics
2.2.3. Lurbinectedin Metabolites (M1 and M4) Plasma Pharmacokinetics
2.3. Safety
3. Discussion
4. Materials and Methods
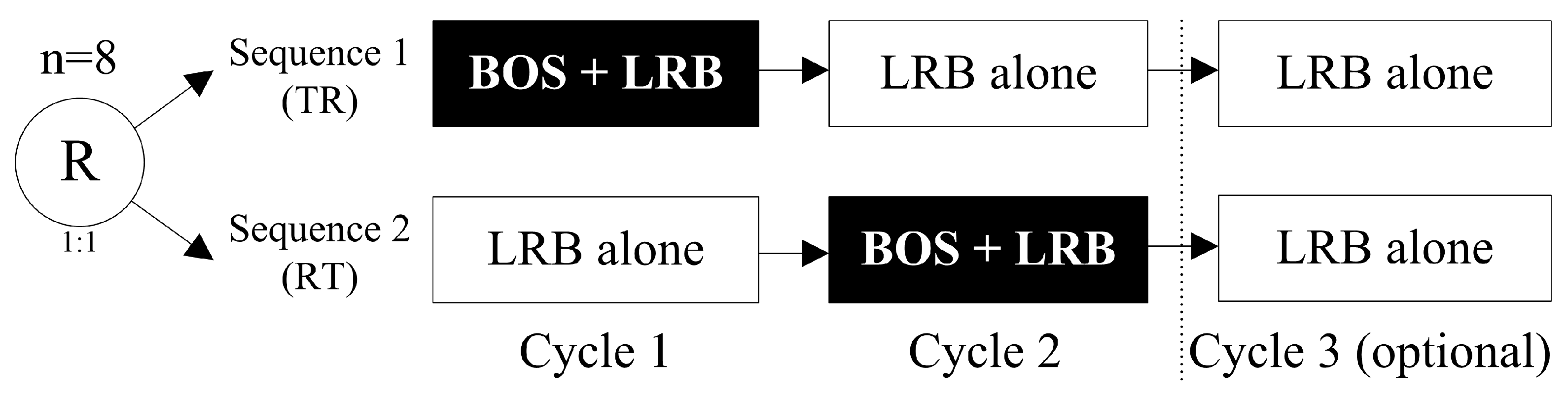
4.1. Study Design and Settings
4.2. Study Population
4.3. Randomization
4.4. Pharmacokinetic Evaluations
4.4.1. Sample Collection
4.4.2. Pharmacokinetic Parameters
4.4.3. Bioanalytical Procedures
4.5. Safety Evaluations
4.6. Statistical Methods
4.6.1. Sample Size
4.6.2. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bueren-Calabuig, J.A.; Giraudon, C.; Galmarini, C.M.; Egly, J.M.; Gago, F. Temperature-induced melting of double-stranded DNA in the absence and presence of covalently bonded antitumour drugs: Insight from molecular dynamics simulations. Nucleic Acids Res. 2011, 39, 8248–8257. [Google Scholar] [CrossRef]
- Harlow, M.L.; Maloney, N.; Roland, J.; Navarro, M.J.G.; Easton, M.K.; Kitchen-Goosen, S.M.; Boguslawski, E.A.; Madaj, Z.B.; Johnson, B.K.; Bowman, M.J.; et al. Lurbinectedin Inactivates the Ewing Sarcoma Oncoprotein Ews-Fli1 by Redistributing It within the Nucleus. Cancer Res. 2016, 76, 6657–6668. [Google Scholar] [CrossRef]
- Jimeno, A.; Sharma, M.R.; Szyldergemajn, S.; Gore, L.; Geary, D.; Diamond, J.R.; Teruel, C.F.; Matos-Pita, A.S.; Iglesias, J.L.; Cullell-Young, M.; et al. Phase I study of lurbinectedin, a synthetic tetrahydroisoquinoline that inhibits activated transcription, induces DNA single- and double-strand breaks, on a weekly × 2 every-3-week schedule. Investig. New Drugs 2017, 35, 471–477. [Google Scholar] [CrossRef]
- Santamaria Nunez, G.; Robles, C.M.; Giraudon, C.; Martinez-Leal, J.F.; Compe, E.; Coin, F.; Aviles, P.; Galmarini, C.M.; Egly, J.M. Lurbinectedin Specifically Triggers the Degradation of Phosphorylated Rna Polymerase Ii and the Formation of DNA Breaks in Cancer Cells. Mol. Cancer Ther. 2016, 15, 2399–2412. [Google Scholar] [CrossRef]
- Leal, J.F.; Martinez-Diez, M.; Garcia-Hernandez, V.; Moneo, V.; Domingo, A.; Bueren-Calabuig, J.A.; Negri, A.; Gago, F.; Guillen-Navarro, M.J.; Aviles, P.; et al. Pm01183, a New DNA Minor Groove Covalent Binder with Potent in Vitro and in Vivo Anti-Tumour Activity. Br. J. Pharmacol. 2010, 161, 1099–1110. [Google Scholar] [CrossRef] [PubMed]
- Markham, A. Lurbinectedin: First Approval. Drugs 2020, 80, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Jaigirdar, A.A.; Mulkey, F.; Cheng, J.; Hamed, S.S.; Li, Y.; Liu, J.; Zhao, H.; Goheer, A.; Helms, W.S.; et al. Fda Approval Summary: Lurbinectedin for the Treatment of Metastatic Small Cell Lung Cancer. Clin. Cancer Res. 2021, 27, 2378–2382. [Google Scholar] [CrossRef] [PubMed]
- Trigo, J.; Subbiah, V.; Besse, B.; Moreno, V.; Lopez, R.; Sala, M.A.; Peters, S.; Ponce, S.; Fernandez, C.; Alfaro, V.; et al. Lurbinectedin as Second-Line Treatment for Patients with Small-Cell Lung Cancer: A Single-Arm, Open-Label, Phase 2 Basket Trial. Lancet Oncol. 2020, 21, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Nccn Clinical Practice Guidelines in Oncology. Small Cell Lung Cancer. Version 1.2024. Available online: https://www.nccn.org/guidelines/recently-published-guidelines (accessed on 5 September 2023).
- Dingemans, A.M.; Früh, M.; Ardizzoni, A.; Besse, B.; Faivre-Finn, C.; Hendriks, L.E.; Lantuejoul, S.; Peters, S.; Reguart, N.; Rudin, C.M.; et al. Small-Cell Lung Cancer: Esmo Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2021, 32, 839–853. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Braña, I.; Longhi, A.; Boni, V.; Delord, J.-P.; Awada, A.; Boudou-Rouquette, P.; Sarantopoulos, J.; Shapiro, G.I.; Elias, A.; et al. Antitumor Activity of Lurbinectedin, a Selective Inhibitor of Oncogene Transcription, in Patients with Relapsed Ewing Sarcoma: Results of a Basket Phase II Study. Clin. Cancer Res. 2022, 28, 2762–2770. [Google Scholar] [CrossRef]
- Kristeleit, R.; Leary, A.; Delord, J.P.; Moreno, V.; Oaknin, A.; Castellano, D.; Shappiro, G.I.; Fernández, C.; Kahatt, C.; Alfaro, V.; et al. Lurbinectedin in patients with pretreated endometrial cancer: Results from a phase 2 basket clinical trial and exploratory translational study. Investig. New Drugs 2023, 41, 677–687. [Google Scholar] [CrossRef]
- Longo-Muñoz, F.; Castellano, D.; Alexandre, J.; Chawla, S.P.; Fernández, C.; Kahatt, C.; Alfaro, V.; Siguero, M.; Zeaiter, A.; Moreno, V.; et al. Lurbinectedin in patients with pretreated neuroendocrine tumours: Results from a phase II basket study. Eur. J. Cancer 2022, 172, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Boni, V.; Pistilli, B.; Brana, I.; Shapiro, G.I.; Trigo, J.; Moreno, V.; Castellano, D.; Fernandez, C.; Kahatt, C.; Alfaro, V.; et al. Lurbinectedin, a Selective Inhibitor of Oncogenic Transcription, in Patients with Pretreated Germline Brca1/2 Metastatic Breast Cancer: Results from a Phase Ii Basket Study. ESMO Open 2022, 7, 100571. [Google Scholar] [CrossRef] [PubMed]
- Besse, B.; Paz-Ares, L.G.; Peters, S.; Cappuzzo, F.; Reck, M.; Calles, A.; Califano, R.; Lopez-Vilariño, J.A.; Veramendi, S.; Kahatt, C.M.; et al. A Phase Iii Study of Lurbinectedin Alone or in Combination with Irinotecan Vs Investigator’s Choice (Topotecan or Irinotecan) in Patients with Relapsed Small Cell Lung Cancer (Sclc; Lagoon Trial). J. Clin. Oncol. 2023, 41, TPS8613. [Google Scholar] [CrossRef]
- Machiels, J.-P.; Staddon, A.; Herremans, C.; Keung, C.; Bernard, A.; Phelps, C.; Khokhar, N.Z.; Knoblauch, R.; Parekh, T.V.; Dirix, L.; et al. Impact of cytochrome P450 3A4 inducer and inhibitor on the pharmacokinetics of trabectedin in patients with advanced malignancies: Open-label, multicenter studies. Cancer Chemother. Pharmacol. 2014, 74, 729–737. [Google Scholar] [CrossRef]
- Iversen, D.B.; Andersen, N.E.; Dunvald, A.D.; Pottegård, A.; Stage, T.B. Drug metabolism and drug transport of the 100 most prescribed oral drugs. Basic Clin. Pharmacol. Toxicol. 2022, 131, 311–324. [Google Scholar] [CrossRef] [PubMed]
- Clozel, M.; Breu, V.; A Gray, G.; Kalina, B.; Löffler, B.M.; Burri, K.; Cassal, J.M.; Hirth, G.; Müller, M.; Neidhart, W. Pharmacological Characterization of Bosentan, a New Potent Orally Active Nonpeptide Endothelin Receptor Antagonist. J. Pharmacol. Exp. Ther. 1994, 270, 228–235. [Google Scholar]
- Weber, C.; Gasser, R.; Hopfgartner, G. Absorption, Excretion, and Metabolism of the Endothelin Receptor Antagonist Bosentan in Healthy Male Subjects. Drug Metab. Dispos. 1999, 27, 810–815. [Google Scholar]
- Aviles, P.; Altares, R.; van Andel, L.; Lubomirov, R.; Fudio, S.; Rosing, H.; del Pino, F.M.M.; Tibben, M.M.; Benedit, G.; Nan-Offeringa, L.; et al. Metabolic Disposition of Lurbinectedin, a Potent Selective Inhibitor of Active Transcription of Protein-Coding Genes, in Nonclinical Species and Patients. Drug Metab. Dispos. 2022, 50, 327–340. [Google Scholar] [CrossRef]
- Leary, A.; Oaknin, A.; Trigo, J.M.; Moreno, V.; Delord, J.-P.; Boni, V.; Braña, I.; Fernández, C.; Kahatt, C.; Nieto, A.; et al. Pooled Safety Analysis of Single-Agent Lurbinectedin in Patients With Advanced Solid Tumours. Eur. J. Cancer 2023, 192, 113259. [Google Scholar] [CrossRef]
- Elez, M.E.; Tabernero, J.; Geary, D.; Macarulla, T.; Kang, S.P.; Kahatt, C.; Pita, A.S.-M.; Teruel, C.F.; Siguero, M.; Cullell-Young, M.; et al. First-In-Human Phase I Study of Lurbinectedin (PM01183) in Patients with Advanced Solid Tumors. Clin. Cancer Res. 2014, 20, 2205–2214. [Google Scholar] [CrossRef] [PubMed]
- Gaillard, S.; Oaknin, A.; Ray-Coquard, I.; Vergote, I.; Scambia, G.; Colombo, N.; Fernandez, C.; Alfaro, V.; Kahatt, C.; Nieto, A.; et al. Lurbinectedin Versus Pegylated Liposomal Doxorubicin or Topotecan in Patients with Platinum-Resistant Ovarian Cancer: A Multicenter, Randomized, Controlled, Open-Label Phase 3 Study (Corail). Gynecol. Oncol. 2021, 163, 237–245. [Google Scholar] [CrossRef] [PubMed]
- King, N.; Garcia-Martinez, S.; Alcaraz, E.; Grisalena, A.; Lubomirov, R.; Altares, R.; Fernandez-Teruel, C.; Francesch, A.M.; Aviles, P.M.; Fudio, S. Quantitative Determination of Lurbinectedin, Its Unbound Fraction and Its Metabolites in Human Plasma Utilizing Ultra-Performance Lc-Ms/Ms. PLoS ONE 2023, 18, e0283783. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequences | Total | |||
|---|---|---|---|---|
| Seq. 1 (TR: BOS + LRB Cycle 1) | Seq. 2 (RT: BOS + LRB Cycle 2) | |||
| (n = 7) | (n = 4) a | (n = 4) | (N = 11) | |
| Gender | ||||
| Male | 3 (43%) | 2 (50%) | 2 (50%) | 5 (45%) |
| Female | 4 (57%) | 2 (50%) | 2 (50%) | 6 (55%) |
| Median age, years (range) | 67 (58–74) | 66 (61–69) | 60 (35–65) | 63 (35–74) |
| ECOG performance status | ||||
| 0 | 4 (57%) | 3 (75%) | 2 (50%) | 6 (55%) |
| 1 | 3 (43%) | 1 (25%) | 2 (50%) | 5 (45%) |
| Median BSA, m2 (range) | 1.7 (1.5–2.0) | 1.9 (1.5–2.0) | 1.9 (1.7–2.2) | 1.7 (1.5–2.2) |
| Stage at diagnosis | ||||
| Early | 4 (57%) | 2 (50%) | 1 (25%) | 5 (45%) |
| Locally advanced | 2 (29%) | 2 (50%) | 1 (25%) | 3 (27%) |
| Metastatic | 1 (14%) | – | 2 (50%) | 3 (27%) |
| Primary tumors | ||||
| Lung | 1 (14%) | 1 (25%) | 2 (50%) | 3 (27%) b |
| Ovarian | 1 (14%) | – | 1 (25%) | 2 (18%) |
| Breast | 1 (14%) | 1 (25%) | – | 1 (9%) |
| Cervical | 1 (14%) | 1 (25%) | – | 1 (9%) |
| Colon | 1 (14%) | 1 (25%) | – | 1 (9%) |
| Gall bladder | 1 (14%) | – | – | 1 (9%) |
| Mesothelioma | 1 (14%) | – | – | 1 (9%) |
| Neuroendocrine tumor | – | – | 1 (25%) | 1 (9%) |
| Number of sites of disease involvement | ||||
| Median (range) | 3 (2–4) | 2 (2–4) | 6 (2–7) | 3 (2–7) |
| Sites of disease | ||||
| Lymph node | 4 (57%) | 2 (50%) | 4 (100%) | 8 (73%) |
| Liver | 4 (57%) | 3 (75%) | 3 (75%) | 7 (64%) |
| Lung | 4 (57%) | 2 (50%) | 3 (75%) | 7 (64%) |
| Peritoneum | 4 (57%) | 2 (50%) | 1 (25%) | 5 (45%) |
| Bone | 1 (14%) | 1 (25%) | 3 (75%) | 4 (36%) |
| CNS | – | – | 3 (75%) | 3 (27%) |
| Adrenal | – | – | 2 (50%) | 2 (18%) |
| Pleura | 1 (14%) | – | 1 (25%) | 2 (18%) |
| Soft tissue | 1 (14%) | – | – | 1 (9%) |
| Pancreas | – | – | 1 (25%) | 1 (9%) |
| Time from diagnosis to first infusion (months) | ||||
| Median (range) | 47.7 (30.5–91.6) | 41.9 (30.5–91.6) | 13.7 (6.8–59.4) | 47.3 (6.8–91.6) |
| Prior treatment for advanced disease (prior chemotherapy lines) | ||||
| Median (range) | 3 (3–5) | 3 (3–4) | 2.5 (1–3) | 3 (1–5) |
| PK Parameter (Units) | Treatment b | Geometric Mean (CV%) | Ratio (%) c | 90% CI (%) d | Intra-Subject CV (%) |
|---|---|---|---|---|---|
| Cmax (µg/L/mg) a | BOS + LRB (T) | 20.71 (54.81) | 96.83 | (81.09–115.62) * | 18.41 |
| LRB (R) | 21.39 (49.56) | ||||
| AUC0–t (µg·h/L/mg) a | BOS + LRB (T) | 56.33 (76.47) | 79.20 | (64.12–97.82) * | 21.99 |
| LRB (R) | 71.13 (84.97) | ||||
| AUC0-∞ (µg·h/L/mg) a | BOS + LRB (T) | 58.83 (75.83) | 79.81 | (64.78–98.32) * | 21.72 |
| LRB (R) | 73.71 (86.93) | ||||
| CL (L/h) | BOS + LRB (T) | 17.00 (75.83) | 125.30 | (101.71–154.36) * | 21.72 |
| LRB (R) | 13.57 (86.93) | ||||
| t1/2 (h) | BOS + LRB (T) | 35.51 (61.54) | 104.93 | (69.49 –158.44) | 44.40 |
| LRB (R) | 33.84 (35.26) | ||||
| Vss (L) | BOS + LRB (T) | 412.94 (78.11) | 106.79 | (74.63–152.8) | 38.17 |
| LRB (R) | 386.69 (65.5) |
| PK Parameter (Units) | Treatment b | Geometric Mean (CV%) | Ratio (%) c | 90% CI (%) d | Intra-Subject CV (%) |
|---|---|---|---|---|---|
| Cmax (µg/L/mg) a | BOS + LRB (T) | 0.0324 (51.77) | 88.44 | (65.62–119.19) | 23.16 |
| LRB (R) | 0.0332 (19.18) | ||||
| AUC0–t (µg·h/L/mg) a | BOS + LRB (T) | 0.0907 (72.73) | 80.26 | (54.26–118.72) | 30.68 |
| LRB (R) | 0.1099 (58.24) | ||||
| AUC0–∞ (µg·h/L/mg) a | BOS + LRB (T) | 0.095 (73.04) | 81.08 | (54.8–119.96) | 30.70 |
| LRB (R) | 0.114 (61.09) | ||||
| CL (L/h) | BOS + LRB (T) | 10,530.93 (73.04) | 123.34 | (83.36–182.49) | 30.70 |
| LRB (R) | 8773.36 (61.09) | ||||
| t1/2 (h) | BOS + LRB (T) | 37.41 (73.98) | 120.50 | (64.79–224.13) | 50.36 |
| LRB (R) | 32.33 (39.36) | ||||
| Vss (L) | BOS + LRB (T) | 266,905.87 (73.09) | 121.90 | (68.59–216.62) | 46.27 |
| LRB (R) | 241,282.16 (23.18) |
| Lurbinectedin Metabolites | MPR of PK Parameter (Units) a | Treatment (n) | Geometric Mean (CV%) | Ratio (%) c | 90% CI (%) d | Intra-Subject CV (%) |
|---|---|---|---|---|---|---|
| M1 (1′,3′-dihydroxy-lurbinectedin) | Cmax (µg/L/mg) | BOS + LRB (T) (n = 8) | 0.3849 (92.13) | 188.13 | (132.93–266.26) | 33.84 |
| LRB (R) (n = 7) b | 0.268 (78.43) | |||||
| AUC0–t (µg·h/L/mg) | BOS + LRB (T) (n = 8) | 0.728 (236.22) | 245.46 | (133.40–451.65) | 63.43 | |
| LRB (R) (n = 7) b | 0.6916 (114.55) | |||||
| M4 (PM030047, N-desmethyl-lurbinectedin) | Cmax (µg/L/mg) | BOS + LRB (T) (n = 8) | 0.5617 (103.28) | 104.94 | (94.07–117.05) | 11.28 |
| LRB (R) (n = 8) | 0.5528 (101.15) | |||||
| AUC0–t (µg·h/L/mg) | BOS + LRB (T) (n = 8) | 0.9962 (267.9) | 91.02 | (71.39–116.04) | 25.39 | |
| LRB (R) (n = 8) | 1.382 (390.96) |
| BOS + LRB (n = 11) | LRB Alone (n = 8) | |||||
|---|---|---|---|---|---|---|
| NCI-CTCAE Grade | All | 3 | 4 | All | 3 | 4 |
| Infections and infestations | ||||||
| Bacteremia | – | – | – | 1 (12.5) | – | – |
| Pneumonia | 1 (9.1) | – | – | – | – | – |
| Upper respiratory tract infection | 1 (9.1) | – | – | – | – | – |
| Nervous system disorders | ||||||
| Monoparesis | 1 (9.1) | 1 (9.1) | – | – | – | – |
| Paresthesia | 1 (9.1) | – | – | – | – | – |
| Vascular disorders | ||||||
| Venous thrombosis | – | – | – | 1 (12.5) | – | – |
| Hot flush | 1 (9.1) | – | – | – | – | – |
| Respiratory, thoracic and mediastinal disorders | ||||||
| Cough | 1 (9.1) | – | – | – | – | – |
| Dyspnea | 2 (18.2) | – | – | – | – | – |
| Gastrointestinal disorders | ||||||
| Diarrhea | 1 (9.1) | – | – | 1 (12.5) | – | – |
| Nausea | 2 (18.2) | 1 (9.1) | – | 1 (12.5) | – | – |
| Constipation | 1 (9.1) | – | – | – | – | – |
| Dyspepsia | 1 (9.1) | – | – | – | – | – |
| Gastritis | 1 (9.1) | – | – | – | – | – |
| Esophagitis | 1 (9.1) | 1 (9.1) | – | – | – | – |
| Vomiting | 2 (18.2) | 1 (9.1) | – | – | – | – |
| Musculoskeletal and connective tissue disorders | ||||||
| Back pain | 1 (9.1) | – | – | – | – | – |
| Bone pain | 1 (9.1) | – | – | – | – | – |
| General disorders and administration site conditions | ||||||
| Fatigue | 5 (45.5) | 1 (9.1) | – | 1 (12.5) | – | – |
| Pain | – | – | – | 1 (12.5) | – | – |
| Edema peripheral | 1 (9.1) | – | – | – | – | – |
| Investigations | ||||||
| Weight decreased | 1 (9.1) | – | – | – | – | – |
| Product issues | ||||||
| Thrombosis in device | 1 (9.1) | 1 (9.1) | – | – | – | – |
| BOS + LRB (n = 11) | LRB Alone (n = 8) | |||||
|---|---|---|---|---|---|---|
| NCI-CTCAE Grade | All | 3 | 4 | All | 3 | 4 |
| Treatment-related AEs | ||||||
| Nausea | 1 (9.1) | – | – | 1 (12.5) | – | – |
| Hematological laboratory abnormalities (regardless of relationship) | ||||||
| Anemia | 10 (90.9) | 1 (9.1) | – | 8 (100.0) | 1 (12.5) | – |
| Leukopenia | 5 (45.5) | – | – | 6 (75.0) | 4 (50.0) | – |
| Lymphopenia | 11 (100.0) | 3 (27.3) | – | 8 (100.0) | 3 (37.5) | – |
| Neutropenia | 3 (27.3) | – | – | 5 (62.5) | 2 (25.0) | 1 (12.5) |
| Thrombocytopenia | 4 (36.4) | 1 (9.1) | 4 (50.0) | – | – | |
| Biochemical laboratory abnormalities (regardless of relationship) | ||||||
| ALT increased | 4 (36.4) | – | – | 2 (25.0) | – | – |
| AP increased | 3 (27.3) | – | – | 2 (25.0) | – | – |
| AST increased | 3 (27.3) | – | – | 1 (12.5) | – | – |
| Creatinine increased | 3 (27.3) | – | – | 3 (37.5) | – | – |
| GGT increased | 2 (18.2) | 1 (9.1) | – | 3 (37.5) | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moreno, I.; Hernández, T.; Calvo, E.; Fudio, S.; Kahatt, C.; Fernández, C.; Iglesias, J.L.; Corral, G.; Pérez-Ramos, L.; Montilla, L.; et al. Impact of a Moderate CYP3A4 Inducer (Bosentan) on Lurbinectedin Pharmacokinetics and Safety in Patients with Advanced Solid Tumors: An Open-Label, Two-Way, Crossover, Phase Ib Drug–Drug Interaction Study. Pharmaceuticals 2024, 17, 182. https://doi.org/10.3390/ph17020182
Moreno I, Hernández T, Calvo E, Fudio S, Kahatt C, Fernández C, Iglesias JL, Corral G, Pérez-Ramos L, Montilla L, et al. Impact of a Moderate CYP3A4 Inducer (Bosentan) on Lurbinectedin Pharmacokinetics and Safety in Patients with Advanced Solid Tumors: An Open-Label, Two-Way, Crossover, Phase Ib Drug–Drug Interaction Study. Pharmaceuticals. 2024; 17(2):182. https://doi.org/10.3390/ph17020182
Chicago/Turabian StyleMoreno, Irene, Tatiana Hernández, Emiliano Calvo, Salvador Fudio, Carmen Kahatt, Cristian Fernández, Jorge Luis Iglesias, Gema Corral, Laura Pérez-Ramos, Lola Montilla, and et al. 2024. "Impact of a Moderate CYP3A4 Inducer (Bosentan) on Lurbinectedin Pharmacokinetics and Safety in Patients with Advanced Solid Tumors: An Open-Label, Two-Way, Crossover, Phase Ib Drug–Drug Interaction Study" Pharmaceuticals 17, no. 2: 182. https://doi.org/10.3390/ph17020182
APA StyleMoreno, I., Hernández, T., Calvo, E., Fudio, S., Kahatt, C., Fernández, C., Iglesias, J. L., Corral, G., Pérez-Ramos, L., Montilla, L., Zeaiter, A., & Lubomirov, R. (2024). Impact of a Moderate CYP3A4 Inducer (Bosentan) on Lurbinectedin Pharmacokinetics and Safety in Patients with Advanced Solid Tumors: An Open-Label, Two-Way, Crossover, Phase Ib Drug–Drug Interaction Study. Pharmaceuticals, 17(2), 182. https://doi.org/10.3390/ph17020182