Why and How the Old Neuroleptic Thioridazine Cures the XDR-TB Patient


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
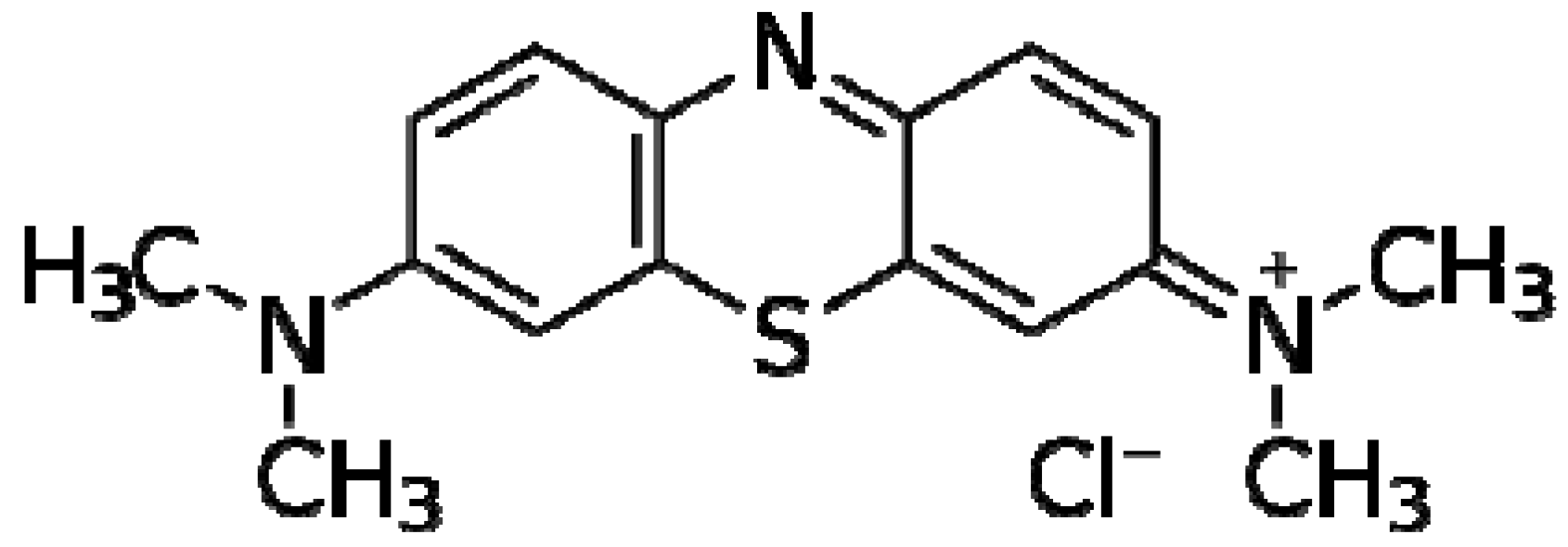
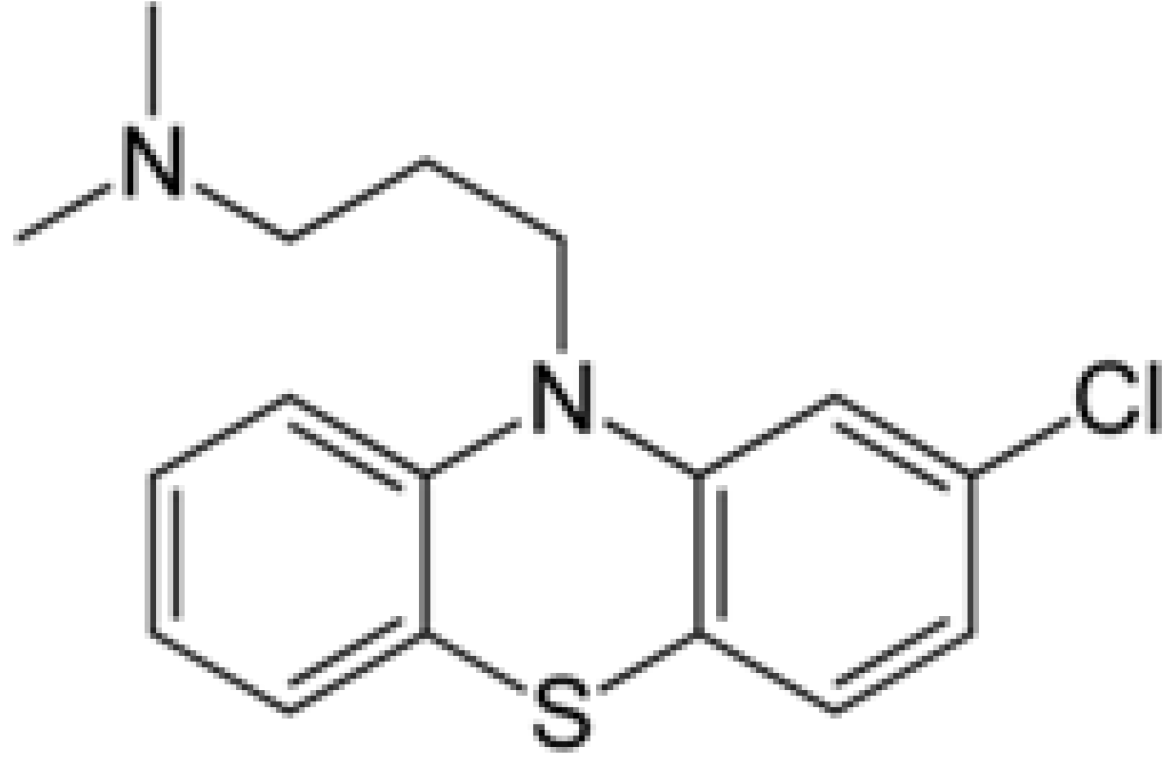
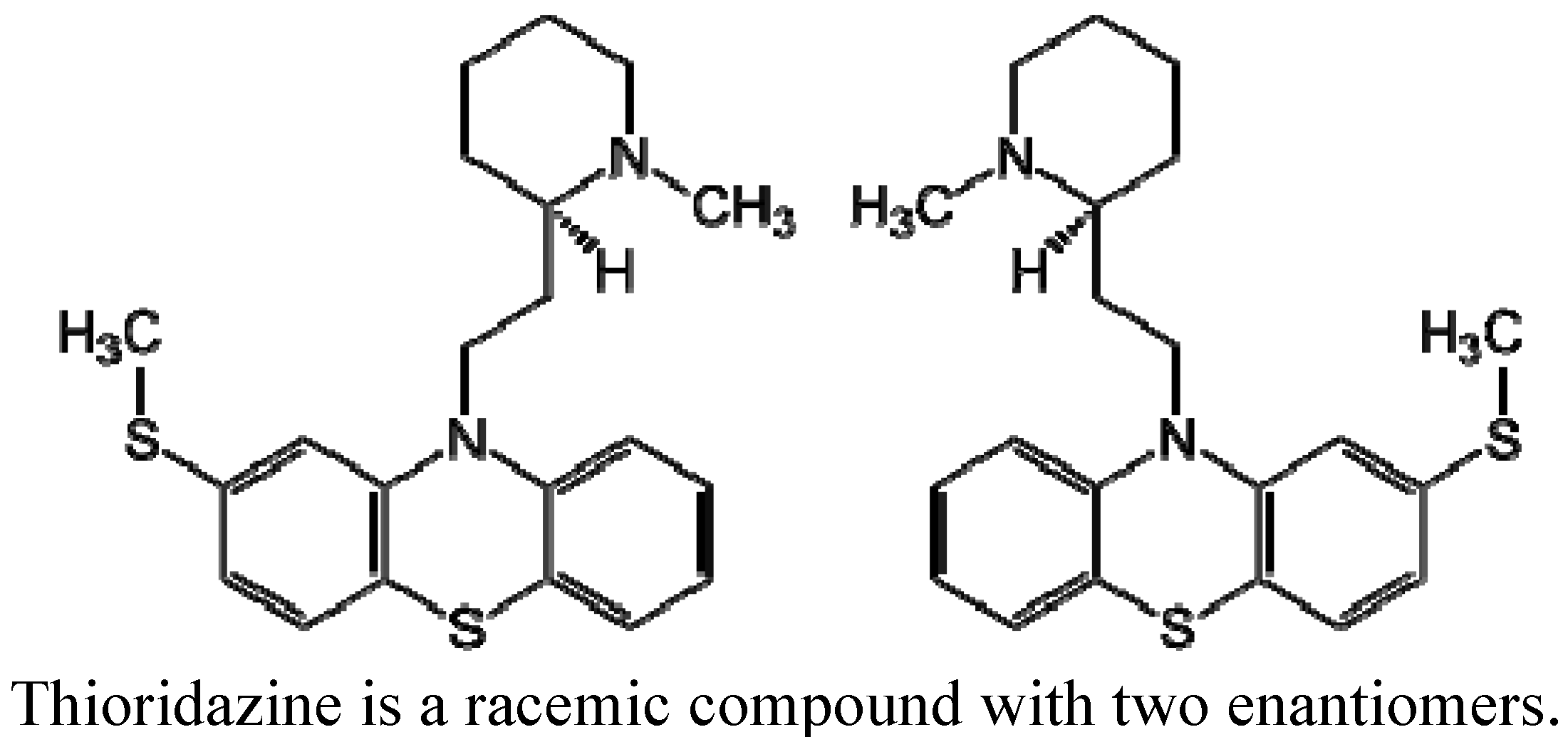
2. Phenothiazines


3. Anti-Tubercular Activity of CPZ and Other Phenothiazines

4. How Does TZ Cure Drug Resistant Pulmonary Infections Such As XDR-TB and Probably TDR-TB?
4.1. The Role of TZ as an Inhibitor of Mtb Efflux Pumps
4.2. The Mechanism by Which TZ Enhances the Killing of Intracellular Mtb
5. Conclusions
Acknowledgement
References
- World Health Organization 2010/2011 Tuberculosis Global Facts. Available online: http://www.who.int/tb/publications/2010/factsheet_tb_2010.pdf (accessed on 14 September 2012).
- Udwadia, Z.F.; Amale, R.A.; Ajbani, K.K.; Rodrigues, C. Totally drug-resistant tuberculosis in India. Clin. Infect. Dis. 2012, 54, 579–581. [Google Scholar] [CrossRef]
- Wang, W.; Hu, Y.; Mathema, B.; Jiang, W.; Kreiswirth, B.; Xu, B. Recent transmission of W-Beijing family Mycobacterium tuberculosis in rural eastern China. Int. J. Tuberc. Lung. Dis. 2012, 16, 306–311. [Google Scholar] [CrossRef]
- Costa, J.C.; Silva, R.; Ferreira, J.; Nienhaus, A. Active tuberculosis among health care workers in Portugal. J. Bras. Pneumol. 2011, 37, 636–645. [Google Scholar]
- Zignol, M.; van Gemert, W.; Falzon, D.; Sismanidis, C.; Glaziou, P.; Floyd, K.; Raviglione, M. Surveillance of anti-tuberculosis drug resistance in the world: An updated analysis, 2007-2010. Bull. World Health Organ. 2012, 90, 111D–119D. [Google Scholar] [CrossRef]
- Oren, E.; Koepsell, T.; Leroux, B.G.; Mayer, J. Area-based socio-economic disadvantage and tuberculosis incidence. Int. J. Tuberc. Lung. Dis. 2012, 16, 880–885. [Google Scholar] [CrossRef]
- Geldmacher, C.; Zumla, A.; Hoelscher, M. Interaction between HIV and Mycobacterium tuberculosis: HIV-1-induced CD4 T-cell depletion and the development of active tuberculosis. Curr. Opin. HIV AIDS 2012, 7, 268–275. [Google Scholar]
- Gupta, V.; Singla, N. Avian influenza: Current scenario. J. Commun. Dis. 2008, 40, 233–241. [Google Scholar]
- Oxlade, O.; Falzon, D.; Menzies, D. The impact and cost-effectiveness of strategies to detect drug-resistant tuberculosis. Eur. Respir. J. 2012, 39, 626–634. [Google Scholar] [CrossRef]
- Udwadia, Z.F. Totally drug-resistant tuberculosis in India: Who let the djinn out? Respirology 2012, 17, 741–742. [Google Scholar] [CrossRef]
- Veziris, N.; Aubry, A.; Truffot-Pernot, C. Trends in tuberculosis treatment duration. Presse Med. 2006, 35, 1758–1764. [Google Scholar] [CrossRef]
- Ajbani, K.; Shetty, A.; Mehta, A.; Rodrigues, C. Rapid diagnosis of extensively drug-resistant tuberculosis by use of a reverse line blot hybridization assay. J. Clin. Microbiol. 2011, 49, 2546–2551. [Google Scholar] [CrossRef]
- Machado, D.; Couto, I.; Perdigão, J.; Rodrigues, L.; Portugal, I.; Baptista, P.; Veigas, B.; Amaral, L.; Viveiros, M. Contribution of efflux to the emergence of isoniazid and multidrug resistance in Mycobacterium tuberculosis. PLoS One 2012, 7, e34538. [Google Scholar]
- Rodrigues, L.; Ramos, J.; Couto, I.; Amaral, L.; Viveiros, M. Ethidium bromide transport across Mycobacterium smegmatis cell-wall: Correlation with antibiotic resistance. BMC Microbiol. 2011, 11, 35. [Google Scholar] [CrossRef]
- Yew, W.W. Management of multidrug-resistant tuberculosis and extensively drug-resistant tuberculosis: current status and future prospects. Kekkaku 2011, 86, 9–16. [Google Scholar]
- Chhabria, M.; Jani, M.; Patel, S. New frontiers in the therapy of tuberculosis: Fighting with the global menace. Mini Rev. Med. Chem. 2009, 9, 401–430. [Google Scholar] [CrossRef]
- von Groote-Bidlingmaier, F.; Diacon, A.H. Medical treatment of tuberculosis update 2011. Ther. Umsch. 2011, 68, 395–401. [Google Scholar]
- Amaral, L.; Viveiros, M. Why thioridazine in combination with antibiotics cures extensively drug-resistant Mycobacterium tuberculosis infections. Int. J. Antimicrob. Agents 2012, 39, 376–380. [Google Scholar] [CrossRef]
- Amaral, L.; Molnar, J. Potential therapy of multidrug-resistant and extremely drug-resistant tuberculosis with thioridazine. In Vivo 2012, 26, 231–236. [Google Scholar]
- Ehrlich, P. The Collected Papers of Paul Erhlich; Himmelweit, F., Marquart, M., Dale, H., Eds.; Pergamon Press: London, UK, 1956; pp. 500–508. [Google Scholar]
- Bodoni, M. La bleu de methylene comme calmant chez les alienes (in French). Sem. Med. 1899, 7, 56. [Google Scholar]
- Charpentier, P.; Gaillot, P.; Jacob, R.; Gaudechon, J.; Buisson, P. Recherches sur les dimethylaminopropyl N-phenothiazines. C. R. Aux Acad. Sci. 1952, 235, 59–60. [Google Scholar]
- Wainwright, M.; Amaral, L.; Kristiansen, J.E. The Evolution of antimycobacterial agents from non-antibiotics. Open J. Pharmacol. 2012, 2, 1. [Google Scholar]
- el-On, J.; Rubinstein, N.; Kernbaum, S.; Schnur, L.F. In vitro and in vivo anti-leishmanial activity of chlorpromazine alone and combined with N-meglumine antimonate. Ann. Trop. Med. Parasitol. 1986, 80, 509–517. [Google Scholar]
- Leandro, C.; Campino, L. Leishmaniasis: Efflux pumps and chemoresistance. Int. J. Antimicrob. Agents 2003, 22, 352–357. [Google Scholar] [CrossRef]
- Yakubu, M.A.; Majumder, S.; Kierszenbaum, F. Changes in Trypanosoma cruzi infectivity by treatments that affect calcium ion levels. Mol. Biochem. Parasitol. 1994, 66, 119–125. [Google Scholar] [CrossRef]
- Barr, R.; Branstetter, B.A.; Rajnicek, A.; Crane, F.L.; Löw, H. Chloroquine-sensitive transplasmalemma electron transport in Tetrahymena pyriformis: A hypothesis for control of parasite protozoa through transmembrane redox. Biochim. Biophys. Acta 1991, 1058, 261–268. [Google Scholar]
- Schuster, F.L.; Visvesvara, G.S. Efficacy of novel antimicrobials against clinical isolates of opportunistic amebas. J. Eukaryot. Microbiol. 1998, 45, 612–618. [Google Scholar]
- Ockert, G. Protozoacidal effect of chlorpromazine. Angew. Parasitol. 1984, 25, 163–167. [Google Scholar]
- Schuster, F.L.; Mandel, N. Phenothiazine compounds inhibit in vitro growth of pathogenic free-living amoebae. Antimicrob. Agents Chemother. 1984, 25, 109–112. [Google Scholar] [CrossRef]
- Kim, J.H.; Jung, S.Y.; Lee, Y.J.; Song, K.J.; Kwon, D.; Kim, K.; Park, S; Im, K.I.; Shin, H.J. Effect of therapeutic chemical agents in vitro and on experimental meningoencephalitis due to Naegleria fowleri. Antimicrob. Agents Chemother. 2008, 52, 4010–4016. [Google Scholar]
- Amaral, L.; Spengler, G.; Martins, A.; Armada, A.; Handzlik, J.; Kiec-Kononowicz, K.; Molnar, J. Inhibitors of bacterial efflux pumps that also inhibit efflux pumps of cancer cells. Anticancer Res. 2012, 32, 2947–2957. [Google Scholar]
- Amaral, L.; Engi, H.; Viveiros, M.; Molnar, J. Comparison of multidrug resistant efflux pumps of cancer and bacterial cells with respect to the same inhibitory agents. In Vivo 2007, 21, 237–244. [Google Scholar]
- Gil-Ad, I.; Shtaif, B.; Levkovitz, Y.; Nordenberg, J.; Taler, M.; Korov, I.; Weizman, A. Phenothiazines induce apoptosis in a B16 mouse melanoma cell line and attenuate in vivo melanoma tumor growth. Oncol. Rep. 2006, 15, 107–112. [Google Scholar]
- Zhelev, Z.; Ohba, H.; Bakalova, R.; Hadjimitova, V.; Ishikawa, M.; Shinohara, Y.; Baba, Y. Phenothiazines suppress proliferation and induce apoptosis in cultured leukemic cells without any influence on the viability of normal lymphocytes. Cancer Chemother. Pharmacol. 2004, 53, 267–275. [Google Scholar] [CrossRef]
- Kristiansen, J.E.; Thomsen, V.F.; Martins, A.; Viveiros, M.; Amaral, L. Non-antibiotics reverse resistance of bacteria to antibiotics. In Vivo 2010, 24, 751–754. [Google Scholar]
- Molnár, J.; Hevér, A.; Fakla, I.; Fischer, J.; Ocsovski, I.; Aszalós, A. Inhibition of the transport function of membrane proteins by some substituted phenothiazines in E. coli and multidrug resistant tumor cells. Anticancer Res. 1997, 17, 481–486. [Google Scholar]
- Costa, S.S.; Falcão, C.; Viveiros, M.; Machado, D.; Martins, M.; Melo-Cristino, J.; Amaral, L.; Couto, I. Exploring the contribution of efflux on the resistance to fluoroquinolones in clinical isolates of Staphylococcus aureus. BMC Microbiol. 2011. [Google Scholar]
- Molnár, J. Antiplasmid activity of tricyclic compounds. Methods Find. Exp. Clin. Pharmacol. 1988, 10, 467–474. [Google Scholar]
- Molnár, J.; Schneider, B.; Mándi, Y.; Farkas, S.; Holland, I.B. New mechanism of plasmid curing by psychotropic drugs. Acta Microbiol. Acad. Sci. Hung. 1980, 27, 309–315. [Google Scholar]
- Spina, E.; Perucca, E. Clinical significance of pharmacokinetic interactions between antiepileptic and psychotropic drugs. Epilepsia 2002, 43, 37–44. [Google Scholar] [CrossRef]
- Wainwright, M.; Amaral, L. The phenothiazinium chromophore and the evolution of antimalarial drugs. Trop. Med. Int. Health 2005, 10, 501–511. [Google Scholar] [CrossRef]
- Aguet, F.; Bossy, A.; Ducommun, P.; Favez, G. Non-specific therapeutic stimulation in evolutive pulmonary tuberculosis. I. Properties of chlorpromazine and phenylsemicarbazide. Schweiz. Med. Wochenschr. 1956, 86, 1239–1245. [Google Scholar]
- Marchand, H.; Reuter, C. Phenothiazine derivatives in treatment of pulmonary tuberculosis. Tuberkulosearzt 1957, 11, 19–27. [Google Scholar]
- Shubin, H.; Heikien, C.A.; Glaskin, A.; Pennes, E.; Arsenian, J. Chlorpromazine as an adjunct in managing tuberculous patients. Int. Rec. Med. Gen. Pract. Clin. 1957, 170, 369–373. [Google Scholar]
- Hollister, L.E.; Eikenberry, D.T.; Raffels, S. Chlorpromazine in nonpsychotic patients with pulmonary tuberculosis. Am. Rev. Respir. Dis. 1960, 81, 562–566. [Google Scholar]
- Filippov, M.I. Aminazin therapy of active forms of tuberculosis in mental patients. (Preliminary communication). Zh. Nevropatol. Psikhiatr. Im. S S Korsakova 1960, 60, 1024–1026. [Google Scholar]
- Santopadre, I.; Silanos, G. Neuroplegics as a therapeutic aid in treatment of tuberculous meningitis. Clin. Pediatr. (Bologna) 1959, 41, 925–936. [Google Scholar]
- Reuter, C. Complications in tuberculosis treatment with phenothiazine derivatives. Dtsch. Gesundheitsw. 1958, 13, 332–334. [Google Scholar]
- Amaral, L.; Kristiansen, J.E.; Viveiros, M.; Atouguia, J. Activity of phenothiazines against antibiotic-resistant Mycobacterium tuberculosis: A review supporting further studies that may elucidate the potential use of thioridazine as anti-tuberculosis therapy. J. Antimicrob. Chemother. 2001, 47, 505–511. [Google Scholar] [CrossRef]
- Raffel, S.; Kochan, I.; Poland, N.; Hollister, L.E. The action of chlorpromazine upon Mycobacterium tuberculosis. Am. Rev. Respir. Dis. 1960, 81, 555–561. [Google Scholar]
- Libenson, V.S.; Braude, V.I. The antitubercular effect of aminazin. Biull. Eksp. Biol. Med. 1967, 63, 61–63. [Google Scholar]
- Molnár, J.; Béládi, I.; Földes, I. Studies on antituberculotic action of some phenothiazine derivatives in vitro. Zentralbl. Bakteriol. Orig. A 1977, 239, 521–526. [Google Scholar]
- Crowle, A.J.; Douvas, G.S.; May, M.H. Chlorpromazine: A drug potentially useful for treating mycobacterial infections. Chemotherapy 1992, 38, 410–419. [Google Scholar] [CrossRef]
- Moss, A.R.; Alland, D.; Telzak, E.; Hewlett, D. Jr; Sharp, V.; Chiliade, P.; LaBombardi, V.; Kabus, D.; Hanna, B.; Palumbo, L.; et al. A city-wide outbreak of a multiple-drug-resistant strain of Mycobacterium tuberculosis in New York. Int. J. Tuberc. Lung Dis. 1997, 1, 115–121. [Google Scholar]
- Amaral, L.; Kristiansen, J.E.; Abebe, L.S.; Millet, W. Inhibition of the respiration of multi-drug resistant clinical isolates of Mycobacterium tuberculosis by Thioridazine: Potential use for the initial therapy of freshly diagnosed tuberculosis. J. Antimicrob. Chemother. 1996, 38, 1049–1053. [Google Scholar] [CrossRef]
- Ordway, D.; Viveiros, M.; Leandro, C.; Amaral, L. Clinical concentrations of Thioridazine kill intracellular Multi-drug resistant Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 2003, 47, 917–922. [Google Scholar]
- Martins, M.; Viveiros, M.; Amaral, L. The curative activity of thioridazine on mice infected With Mycobacterium tuberculosis. In Vivo 2007, 21, 771–776. [Google Scholar]
- van Soolingen, D.; Pando, R.H.; Orozco, H.; Aguilar, D.; Magis, C.; van Ingen, J.; Amaral, L.; Boeree, M. Thioridazine shows promising activity in a murine model of multi-drug resistant tuberculosis. PLoS One 2010, 5, e12640. [Google Scholar]
- Viveiros, M.; Amaral, L. Enhancement of antibiotic activity against poly-drug resistant Mycobacterium tuberculosis by phenothiazines. Int. J. Antimicrob. Agents 2001, 17, 225–228. [Google Scholar] [CrossRef]
- Abbate, E.; Vescovo, M.; Natiello, M.; Cufré, M.; García, A.; Montaner, P.G.; Ambroggi, M.; Ritacco, V.; van Soolingen, D. Successful alternative treatment of extensively drug-resistant tuberculosis in Argentina with a combination of linezolid, moxifloxacin and thioridazine. J. Antimicrob. Chemother. 2012, 67, 473–477. [Google Scholar] [CrossRef]
- Udwadia, Z.F.; Sen, T.; Pinto, L.M. Safety and efficacy of thioridazine as salvagetherapy in Indian patients with XDR-TB. Recent Pat. Antiinfect. Drug Discov. 2011, 6, 88–91. [Google Scholar] [CrossRef]
- Rodrigues, L.; Machado, D.; Couto, I.; Amaral, L.; Viveiros, M. Contribution of efflux activity to isoniazid resistance in the Mycobacterium tuberculosis complex. Infect. Genet. Evol. 2012, 12, 695–700. [Google Scholar] [CrossRef]
- Viveiros, M.; Portugal, I.; Bettencourt, R.; Victor, T.C.; Jordaan, A.M.; Leandro, C.; Ordway, D.; Amaral, L. Isoniazid-induced transient high-level resistance in Mycobacterium tuberculosis. Antimicrob. Agents Chemother. 2002, 46, 2804–2810. [Google Scholar] [CrossRef]
- Dutta, N.K.; Mazumdar, K.; Dastidar, S.G.; Karakousis, P.C.; Amaral, L. New patentable use of an old neuroleptic compound thioridazine to combat tuberculosis: A gene regulation perspective. Recent Pat. Antiinfect. Drug Discov. 2011, 6, 128–138. [Google Scholar] [CrossRef]
- Dutta, N.K.; Mehra, S.; Kaushal, D. A Mycobacterium tuberculosis sigma factor network responds to cell-envelope damage by the promising anti-mycobacterial thioridazine. PLoS One 2010, 5, e10069. [Google Scholar] [CrossRef]
- Sohaskey, C. Latent tuberculosis: Is there a role for thioridazine? Recent Pat. Antiinfect. Drug Discov. 2011, 6, 139–146. [Google Scholar] [CrossRef]
- Sohaskey, C.D. Nitrate enhances the survival of Mycobacterium tuberculosis during inhibition of respiration. J. Bacteriol. 2008, 190, 2981–2986. [Google Scholar] [CrossRef]
- Amaral, L.; Martins, A.; Molnar, J.; Kristiansen, J.E.; Martins, M.; Viveiros, M.; Rodrigues, L.; Spengler, G.; Couto, I.; Ramos, J.; et al. Phenothiazines, bacterial efflux pumps and targeting the macrophage for enhanced killing of intracellular XDRTB. In Vivo 2010, 24, 409–424. [Google Scholar]
- Martins, M.; Bleiss, W.; Marko, A.; Ordway, D.; Viveiros, M.; Leandro, C.; Pacheco, T.; Molnar, J.; Kristiansen, J.E.; Amaral, L. Clinical concentrations of thioridazine enhance the killing of intracellular methicillin-resistant Staphylococcus aureus: An in vivo, ex vivo and electron microscopy study. In Vivo 2004, 18, 787–794. [Google Scholar]
- Ordway, D.; Viveiros, M.; Leandro, C.; Arroz, M.J.; Molnar, J.; Kristiansen, J.E.; Amaral, L. Chlorpromazine has intracellular killing activity against phagocytosed Staphylococcus aureus at clinical concentrations. J. Infect. Chemother. 2002, 8, 227–231. [Google Scholar] [CrossRef]
- Martins, M.; Viveiros, M.; Couto, I.; Amaral, L. Targeting human macrophages for enhanced killing of intracellular XDR-TB and MDR-TB. Int. J. Tuberc. Lung Dis. 2009, 13, 569–573. [Google Scholar]
- Martins, M.; Viveiros, M.; Amaral, L. Inhibitors of Ca2+ and K+ transport enhance intracellular killing of M. tuberculosis by non-killing macrophages. In Vivo 2008, 22, 69–75. [Google Scholar]
- Martins, M.; Viveiros, M.; Amaral, L. The TB laboratory of the future:macrophage-based selection of XDR-TB therapeutics. Future Microbiol. 2008, 3, 135–144. [Google Scholar]
- Martins, M.; Schelz, Z.; Martins, A.; Molnar, J.; Hajös, G.; Riedl, Z.; Viveiros, M.; Yalcin, I.; Aki-Sener, E.; Amaral, L. In vitro and ex vivo activity of thioridazine derivatives against Mycobacterium tuberculosis. Int. J. Antimicrob. Agents 2007, 29, 338–340. [Google Scholar]
- Amaral, L.; Martins, M.; Viveiros, M. Enhanced killing of intracellular multidrug-resistant Mycobacterium tuberculosis by compounds that affect the activity of efflux pumps. J. Antimicrob. Chemother. 2007, 59, 1237–1246. [Google Scholar] [CrossRef]
- Martins, M.; Viveiros, M.; Amaral, L. Sila Compound 421, an Inhibitor of efflux pumps of cancer cells, enhances the killing of intracellular XDRTB. Int. J. Antimicrobial. Agents 2008, 33, 479–482. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Amaral, L.; Molnar, J. Why and How the Old Neuroleptic Thioridazine Cures the XDR-TB Patient. Pharmaceuticals 2012, 5, 1021-1031. https://doi.org/10.3390/ph5091021
Amaral L, Molnar J. Why and How the Old Neuroleptic Thioridazine Cures the XDR-TB Patient. Pharmaceuticals. 2012; 5(9):1021-1031. https://doi.org/10.3390/ph5091021
Chicago/Turabian StyleAmaral, Leonard, and Joseph Molnar. 2012. "Why and How the Old Neuroleptic Thioridazine Cures the XDR-TB Patient" Pharmaceuticals 5, no. 9: 1021-1031. https://doi.org/10.3390/ph5091021
APA StyleAmaral, L., & Molnar, J. (2012). Why and How the Old Neuroleptic Thioridazine Cures the XDR-TB Patient. Pharmaceuticals, 5(9), 1021-1031. https://doi.org/10.3390/ph5091021