Positive Anti-SSA/Ro Antibody in a Woman with SARS-CoV-2 Infection Using Immunophenotyping: A Case Report

 and
and
Abstract
:1. Introduction
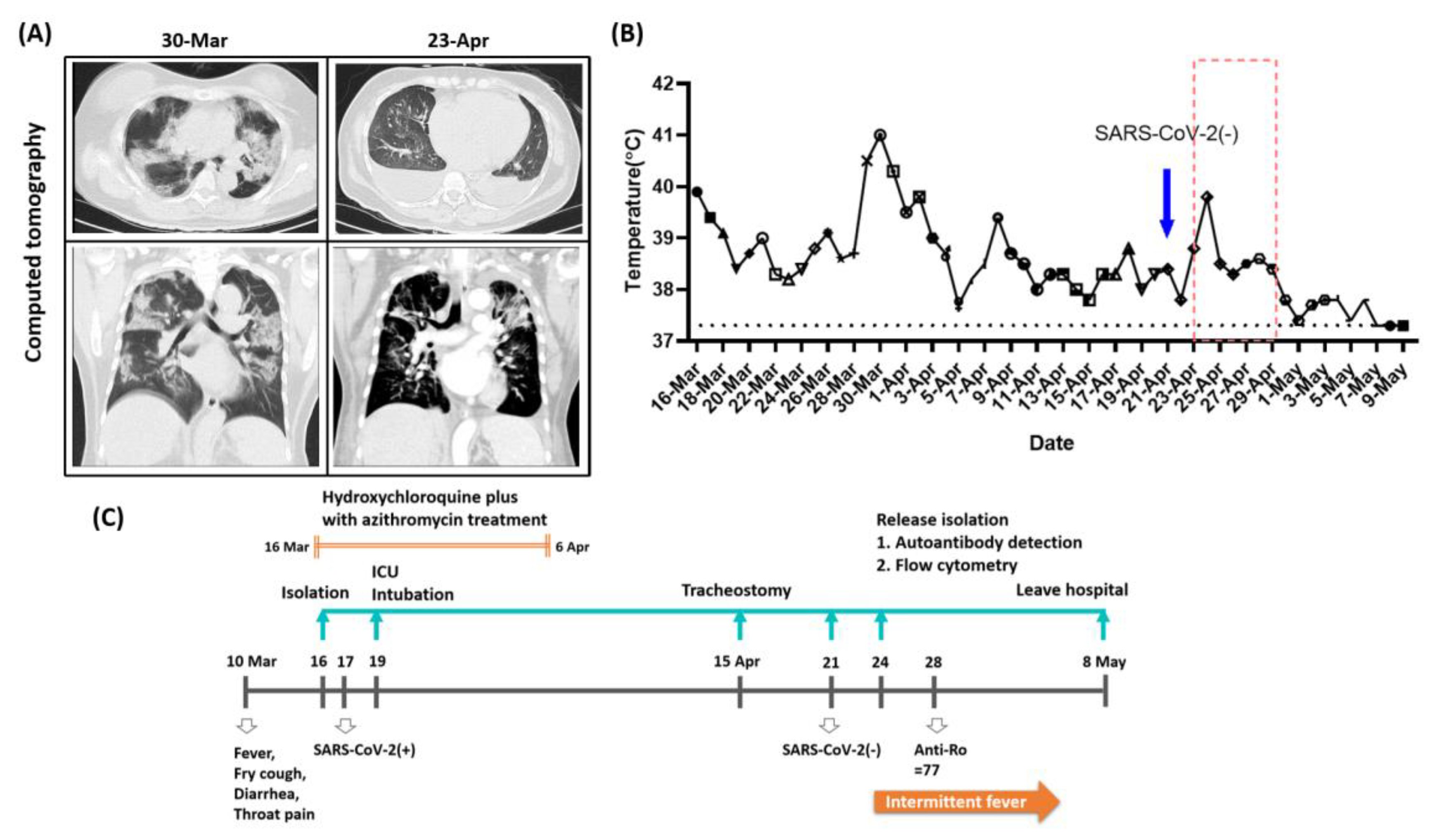
2. Case Report
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Sene, D.; Piette, J.C.; Cacoub, P. Antiphospholipid antibodies, antiphospholipid syndrome and infections. Autoimmun. Rev. 2008, 7, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Yoshimi, R.; Ueda, A.; Ozato, K.; Ishigatsubo, Y. Clinical and pathological roles of Ro/SSA autoantibody system. Clin. Dev. Immunol. 2012, 2012, 606195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Han, T.; Chen, J.; Hou, C.; Hua, L.; He, S.; Guo, Y.; Zhang, S.; Wang, Y.; Yuan, J.; et al. Clinical and Autoimmune Characteristics of Severe and Critical Cases of COVID-19. Clin. Transl. Sci. 2020. [Google Scholar] [CrossRef] [PubMed]
- Gao, Z.W.; Wang, X.; Lin, F.; Dong, K. The correlation between SARS-CoV-2 infection and rheumatic disease. Autoimmun. Rev. 2020, 19, 102557. [Google Scholar] [CrossRef] [PubMed]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94, e00127-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.; Wei, Q.; Alvarez, X.; Wang, H.; Du, Y.; Zhu, H.; Jiang, H.; Zhou, J.; Lam, P.; Zhang, L.; et al. Epithelial cells lining salivary gland ducts are early target cells of severe acute respiratory syndrome coronavirus infection in the upper respiratory tracts of rhesus macaques. J. Virol. 2011, 85, 4025–4030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lyons-Weiler, J. Pathogenic priming likely contributes to serious and critical illness and mortality in COVID-19 via autoimmunity. J. Transl. Autoimmun. 2020, 3, 100051. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J. Infect. 2020, 81, e6–e12. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Hou, S.; Fang, Q.; Liu, X.; Liu, X.; Qi, H. PD-1 Controls Follicular T Helper Cell Positioning and Function. Immunity 2018, 49, 264–274.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Henson, S.M.; Akbar, A.N. KLRG1--more than a marker for T cell senescence. Age 2009, 31, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avery, L.; Filderman, J.; Szymczak-Workman, A.L.; Kane, L.P. Tim-3 co-stimulation promotes short-lived effector T cells, restricts memory precursors, and is dispensable for T cell exhaustion. Proc. Natl. Acad. Sci. USA 2018, 115, 2455–2460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.; Guan, Z.; Zhao, L.; Song, Y.; Wang, H. Elevated level of circulating CD4(+)Helios(+)FoxP3(+) cells in primary Sjogren’s syndrome patients. Mod. Rheumatol. 2017, 27, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Saadoun, D.; Terrier, B.; Bannock, J.; Vazquez, T.; Massad, C.; Kang, I.; Joly, F.; Rosenzwajg, M.; Sene, D.; Benech, P.; et al. Expansion of autoreactive unresponsive CD21-/low B cells in Sjogren’s syndrome-associated lymphoproliferation. Arthritis Rheum. 2013, 65, 1085–1096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bende, R.J.; van Noesel, C.J.M. Rheumatoid Factor Reactivity of Expanded CD21(-/low) B Cells in Patients With Sjogren’s Syndrome: Comment on the Article by Glauzy et al. Arthritis Rheumatol. 2019, 71, 169–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| The Case | Mean ± 3SD | ||||
|---|---|---|---|---|---|
| Groups | Recovered COVID-19 (n = 4) | Sjögren’s Syndrome (n = 4) | Healthy Control (n = 4) | ||
| Clinical Characteristics | |||||
| Age (years) | 60 | 45.25 ± 70.54 | 56.75 ± 20.11 | 46.75 ± 16.68 | |
| Duration | 43 days | 41.75 ± 49.56 days | 3.00 ± 8.49 years | - | |
| Severity | Severe | Mild | - | - | |
| ESSDAI | - | - | 2.00 ± 4.24 | - | |
| Autoantibody | Anti-Ro (U/mL) | 77 | <0.3 | 76.00 ± 106.24 | - |
| Anti-La (U/mL) | 3.7 | <0.3 | 5.70 ± 5.94 | - | |
| Anti-Histone (U/mL) | 1.2 | - | - | - | |
| Connective Tissue (Ratio) | 1.4 | - | 3.98 ± 7.90 | - | |
| Hematology Test | WBC (*103/mm3) | 8.43 | 6.64 ± 6.54 | 7.52 ± 8.76 | - |
| RBC (*106/mm3) | 3.5 | 4.55 ± 1.31 | 4.32 ± 2.12 | - | |
| Hb (g/dL) | 10.7 | 13.35 ± 2.74 | 12.20 ± 4.00 | - | |
| PLT (*103/mm3) | 367 | 220.25 ± 25.14 (↓) | 284.00 ± 263.49 | - | |
| Neutrophil (%) | 81.7 | 54.53 ± 12.80 (↓) | 66.53 ± 31.74 | - | |
| Lymphocyte (%) | 13.6 | 33.38 ± 19.32 (↑) | 26.68 ± 25.12 | - | |
| Neutrophil/Lymphocyte (Ratio) | 6.01 | 1.69 ± 1.26 (↓) | 2.77 ± 3.54 | - | |
| Basophil (%) | 0.2 | 0.90 ± 0.65 (↑) | 0.53 ± 0.62 | - | |
| Biochemistry Test | BUN (mg/dL) | 16 | 11.25 ± 3.77 (↓) | 17.25 ± 33.26 | - |
| ALT (IU/L) | 34 | 11.50 ± 16.34 (↓) | 11.75 ± 5.12 (↓) | - | |
| CRP (mg/dL) | 1.57 | <0.1 (↓) | 0.07 ± 0.41 (↓) | - | |
| T Cell Panel | |||||
| Lymphocytes/Leukocytes | 34.15 | 40.26 ± 38.92 | 35.17 ± 7.28 | 43.88 ± 60.99 | |
| T cells (CD3 +) | 74.26 | 70.92 ± 18.94 | 70.06 ± 21.43 | 65.50 ± 13.07 | |
| T helper cells (CD3 + CD4 +) | 65.26 | 51.27 ± 33.59 | 66.16 ± 33.16 | 62.24 ± 37.59 | |
| KLRG1 | 15.59 | 26.05 ± 26.17 # | 27.44 ± 21.86 # | 70.80 ± 97.94 | |
| PD-1 | 47.35 | 34.44 ± 5.50 (↓) | 34.61 ± 37.35 | 32.99 ± 27.36 | |
| Tim-3 | 0.86 | 0.59 ± 0.79 | 1.33 ± 2.14 | 14.42 ± 59.75 | |
| Naïve T helper cells (CD3 + CD4 + CCR7 + CD45RA +) | 27.25 | 27.00 ± 44.66 | 31.84 ± 43.62 | 39.64 ± 36.43 | |
| KLRG1 | 2.45 | 15.73 ± 27.05 | 20.91 ± 29.42 | 58.22 ± 144.22 | |
| PD-1 | 3.02 | 3.29 ± 3.29 | 2.88 ± 3.51 | 2.84 ± 6.03 | |
| Tim-3 | 0.32 | 0.16 ± 0.30 | 0.33 ± 0.61 | 4.86 ± 27.00 | |
| Central memory T helper cells (CD3 + CD4 + CCR7 + CD45RA -) | 55.18 | 54.39 ± 41.55 | 54.45 ± 49.40 | 48.07 ± 30.10 | |
| KLRG1 | 16.22 | 26.16 ± 33.05 # | 30.88 ± 31.80 # | 74.65 ± 85.37 | |
| PD-1 | 59.23 | 41.93 ± 27.52 | 43.68 ± 43.09 | 47.70 ± 19.18 | |
| Tim-3 | 1.06 | 0.65 ± 1.04 | 1.47 ± 2.38 | 18.17 ± 65.66 | |
| Effector T helper cells (CD3 + CD4 + CCR7 - CD45RA +) | 1.1 | 0.36 ± 1.52 | 0.13 ± 0.26 (↓) | 0.32 ± 1.03 | |
| KLRG1 | 75.68 | 52.82 ± 16.16 (↓) # | 40.79 ± 34.61 (↓) # | 91.98 ± 9.14 (↑) | |
| PD-1 | 80.89 | 72.71 ± 18.79 | 57.81 ± 49.83 | 65.86 ± 58.13 | |
| Tim-3 | 1.49 | 0.62 ± 2.33 | 5.34 ± 10.04 | 13.52 ± 65.06 | |
| Effector memory T helper cells (CD3 + CD4 + CCR7 - CD45RA -) | 16.47 | 18.26 ± 8.26 # | 13.59 ± 31.79 | 11.98 ± 14.40 | |
| KLRG1 | 31.2 | 40.95 ± 28.12 # | 38.46 ± 43.25 # | 92.02 ± 31.60 (↑) | |
| PD-1 | 78.66 | 62.92 ± 31.40 | 68.31 ± 37.08 | 72.38 ± 49.70 | |
| Tim-3 | 1.05 | 1.32 ± 2.62 | 2.89 ± 5.37 | 22.61 ± 77.90 | |
| Cytotoxic T cells (CD3 + CD8 +) | 25.46 | 38.80 ± 29.16 | 23.86 ± 40.24 | 27.77 ± 22.00 | |
| KLRG1 | 39.13 | 49.27 ± 30.53 # | 45.92 ± 51.78 # | 89.38 ± 41.50 (↑) | |
| PD-1 | 57.34 | 37.36 ± 33.09 | 31.71 ± 36.92 | 34.84 ± 40.54 | |
| Tim-3 | 1.95 | 1.18 ± 1.38 | 1.79 ± 1.24 | 2.21 ± 4.65 | |
| Naïve cytotoxic T cells (CD3 + CD8 + CCR7 + CD45RA +) | 27.72 | 21.43 ± 64.43 | 32.17 ± 49.83 | 35.40 ± 56.95 | |
| KLRG1 | 4.12 | 21.13 ± 20.39 # | 23.05 ± 60.99 | 66.49 ± 116.17 | |
| PD-1 | 5.03 | 9.03 ± 22.21 | 6.04 ± 8.28 | 7.70 ± 15.61 | |
| Tim-3 | 1.24 | 0.99 ± 3.87 | 0.88 ± 0.57 # | 0.57 ± 0.51 (↓) | |
| Central memory cytotoxic T cells (CD3 + CD8 + CCR7 + CD45RA -) | 10.89 | 12.76 ± 7.08 | 21.22 ± 37.55 | 14.82 ± 14.01 | |
| KLRG1 | 22.52 | 40.44 ± 18.67 # | 32.02 ± 32.84 # | 84.74 ± 64.38 | |
| PD-1 | 73.23 | 59.52 ± 29.93 | 45.59 ± 43.46 | 57.54 ± 36.95 | |
| Tim-3 | 2.38 | 1.04 ± 1.26 (↓) | 2.21 ± 2.40 | 2.45 ± 4.24 | |
| Effector cytotoxic T cells (CD3 + CD8 + CCR7 - CD45RA +) | 17.89 | 19.33 ± 66.97 | 14.46 ± 29.48 | 23.74 ± 50.89 | |
| KLRG1 | 63.89 | 53.79 ± 46.75 # | 68.41 ± 52.49 # | 98.67 ± 5.57 (↑) | |
| PD-1 | 53.98 | 31.93 ± 65.59 | 22.37 ± 25.24 (↓) | 37.15 ± 60.29 | |
| Tim-3 | 2.23 | 1.43 ± 1.61 | 1.95 ± 2.32 | 2.63 ± 4.22 | |
| Effector memory cytotoxic T cells (CD3 + CD8 + CCR7-CD45RA-) | 43.5 | 46.49 ± 58.75 | 32.15 ± 54.01 | 26.05 ± 16.01 (↓) | |
| KLRG1 | 55.4 | 66.67 ± 58.52 # | 67.55 ± 20.33 # | 95.66 ± 21.43 (↑) | |
| PD-1 | 88.08 | 57.66 ± 83.82 | 53.18 ± 43.46 | 62.24 ± 57.13 | |
| Tim-3 | 2.19 | 1.76 ± 4.29 | 2.59 ± 2.95 | 3.46 ± 6.71 | |
| Treg Cell Panel | |||||
| T helper cells | |||||
| Treg (CD3 + CD4 + CD25high) | 6.69 | 5.43 ± 6.08 | 4.93 ± 5.78 | 6.65 ± 4.84 | |
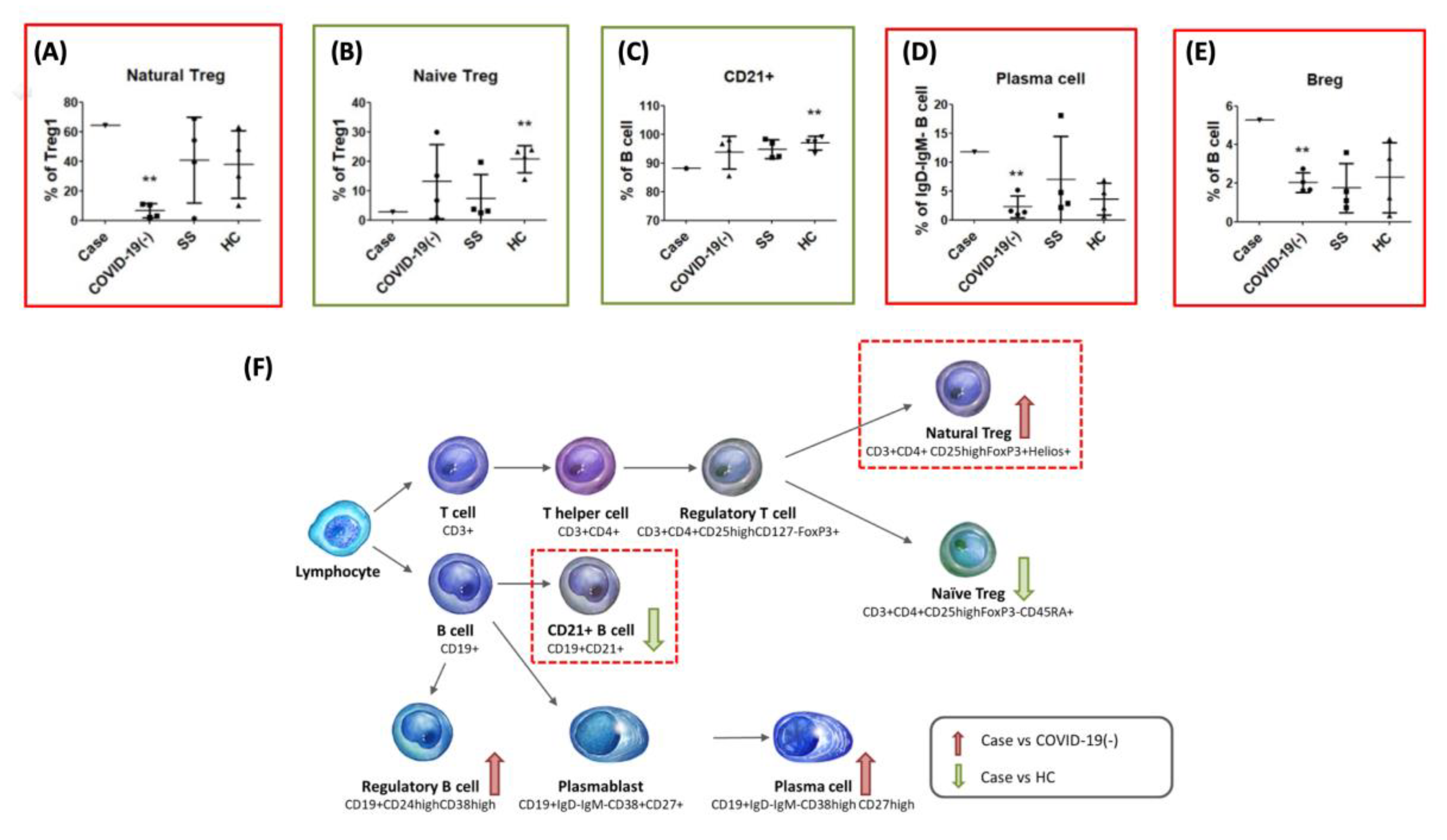
| Natural Treg (CD3 + CD4 + CD25highFoxP3 + Helios +) | 64.38 | 6.75 ± 14.31 (↓) | 40.85 ± 86.61 | 37.90 ± 68.42 | |
| Naïve Treg (CD3 + CD4 + CD25highFoxP3 - CD45RA+) | 2.77 | 13.18 ± 37.88 | 7.27 ± 25.09 # | 20.66 ± 13.77 (↑) | |
| B Cell Panel | |||||
| Lymphocytes | |||||
| B cells (CD19 +) | 12.56 | 21.82 ± 64.71 | 6.48 ± 11.12 | 10.03 ± 8.87 | |
| CD21+ | 88.17 | 93.72 ± 17.09 | 94.83 ± 9.76 | 96.87 ± 7.29 (↑) | |
| HLADR+ | 97.12 | 96.93 ± 3.18 | 97.02 ± 4.80 | 96.33 ± 12.09 | |
| PD-1+ | 11.75 | 47.43 ± 40.69 | 28.48 ± 43.97 | 30.01 ± 64.67 | |
| Marginal zone B cells (CD19 + CD27 + IgD +) | 5.77 | 12.35 ± 16.70 | 5.80 ± 2.65 # | 15.23 ± 25.45 | |
| CD21+ | 89.36 | 96.93 ± 3.55 (↑) | 92.79 ± 16.86 | 97.36 ± 5.42 (↑) | |
| HLADR+ | 95.48 | 94.08 ± 13.34 | 97.64 ± 3.25 | 94.72 ± 15.88 | |
| PD-1+ | 16.75 | 57.88 ± 28.40 (↑) | 34.02 ± 44.40 | 33.39 ± 65.69 | |
| Naïve B cells (CD19 + CD27 – IgD +) | 69.94 | 52.70 ± 44.17 | 65.57 ± 9.63 | 55.80 ± 30.40 | |
| CD21+ | 96.81 | 96.74 ± 7.26 | 98.79 ± 2.41 | 98.58 ± 4.10 | |
| HLADR+ | 98.85 | 98.07 ± 3.25 | 97.91 ± 4.68 | 96.45 ± 12.25 | |
| PD-1+ | 11.18 | 52.19 ± 43.81 | 31.92 ± 47.65 | 32.11 ± 69.86 | |
| Switch memory B cells (CD19 + CD27 + IgD-) | 18.23 | 24.55 ± 27.77 | 23.34 ± 7.77 | 21.95 ± 14.87 | |
| CD21 + | 63.18 | 94.21 ± 14.69 (↑) | 87.66 ± 20.81 (↑) | 94.50 ± 13.18 (↑) | |
| HLADR + | 91.04 | 96.36 ± 5.02 (↑) | 94.55 ± 7.09 | 96.68 ± 9.24 | |
| PD-1 + | 11.63 | 38.79 ± 42.40 | 18.87 ± 34.43 | 24.27 ± 56.87 | |
| Double negative B cells (CD19 + CD27 – IgD -) | 6.06 | 10.39 ± 23.53 | 5.30 ± 3.70 | 7.02 ± 8.30 | |
| CD21 + | 62.59 | 77.54 ± 34.60 | 83.43 ± 33.56 | 88.69 ± 32.39 | |
| HLADR + | 96.97 | 97.55 ± 4.52 | 96.47 ± 7.02 | 96.49 ± 17.37 | |
| PD-1 + | 13.94 | 41.26 ± 35.18 | 22.78 ± 42.48 | 27.25 ± 75.70 | |
| Breg (CD19 + CD24highCD38high) | 5.28 | 2.03 ± 1.55 (↓) | 1.76 ± 3.83 | 2.29 ± 5.47 | |
| Plasmablasts (CD19 + IgD - IgM - CD38 + CD27 + /CD19 + CD27 + CD38 + B cells) | 54.92 | 59.52 ± 23.35 | 68.25 ± 55.27 | 58.29 ± 57.36 | |
| Plasma cells (CD19 + IgD – IgM - CD38high CD27high/CD19 + IgD – IgM - B cells) | 11.77 | 2.27 ± 5.76 (↓) | 6.97 ± 22.53 | 3.58 ± 8.25 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, P.-I.; Lin, T.-C.; Liu, F.-C.; Ho, Y.-J.; Lu, J.-W.; Lin, T.-Y. Positive Anti-SSA/Ro Antibody in a Woman with SARS-CoV-2 Infection Using Immunophenotyping: A Case Report. Medicina 2020, 56, 521. https://doi.org/10.3390/medicina56100521
Huang P-I, Lin T-C, Liu F-C, Ho Y-J, Lu J-W, Lin T-Y. Positive Anti-SSA/Ro Antibody in a Woman with SARS-CoV-2 Infection Using Immunophenotyping: A Case Report. Medicina. 2020; 56(10):521. https://doi.org/10.3390/medicina56100521
Chicago/Turabian StyleHuang, Po-I, Ting-Chun Lin, Feng-Cheng Liu, Yi-Jung Ho, Jeng-Wei Lu, and Te-Yu Lin. 2020. "Positive Anti-SSA/Ro Antibody in a Woman with SARS-CoV-2 Infection Using Immunophenotyping: A Case Report" Medicina 56, no. 10: 521. https://doi.org/10.3390/medicina56100521
APA StyleHuang, P. -I., Lin, T. -C., Liu, F. -C., Ho, Y. -J., Lu, J. -W., & Lin, T. -Y. (2020). Positive Anti-SSA/Ro Antibody in a Woman with SARS-CoV-2 Infection Using Immunophenotyping: A Case Report. Medicina, 56(10), 521. https://doi.org/10.3390/medicina56100521