
Stable Low-Grade Degenerative Spondylolisthesis Does Not Compromise Clinical Outcome of Minimally Invasive Tubular Decompression in Patients with Spinal Stenosis

Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
4.1. Participants
4.2. Outcome Data and Main Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Number of Patients | N | S | p-Value | ||
|---|---|---|---|---|---|
| Length of stay(days) | Age < 65y | 26 | 1.6 ± 0.5 | 1.8 ± 1.0 | 0.027 |
| Age 65–75y | 41 | 4.0 ± 5.9 | 2.3 ± 1.6 | 0.022 | |
| Age > 75y | 29 | 3.1 ± 3.1 | 2.4 ± 1.3 | 0.038 |
References
- Watters, W.C.; Bono, C.M.; Gilbert, T.J.; Kreiner, D.S.; Mazanec, D.J.; Shaffer, W.O.; Baisden, J.; Easa, J.E.; Fernand, R.; Ghiselli, G.; et al. An evidence-based clinical guideline for the diagnosis and treatment of degenerative lumbar spondylolisthesis. Spine J. 2009, 9, 609–614. [Google Scholar] [CrossRef]
- Deyo, R.A.; Mirza, S.K.; Martin, B.I.; Kreuter, W.; Goodman, D.C.; Jarvik, J.G. Trends, major medical complications, and charges associated with surgery for lumbar spinal stenosis in older adults. JAMA 2010, 303, 1259–1265. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, J.N.; Lurie, J.D.; Tosteson, T.D.; Zhao, W.; Blood, E.A.; Tosteson, A.N.; O Birkmeyer, N.J.; Herkowitz, H.N.; Longley, M.C.; Lenke, L.G.; et al. Surgical compared with nonoperative treatment for lumbar degenerative spondylolisthesis. Four-year results in the Spine Patient Outcomes Research Trial (SPORT) randomized and observational cohorts. J. Bone Jt. Surg. Am. 2009, 91, 1295–1304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.N.; Blood, E.; Hanscom, B.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.D.; et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N. Engl. J. Med. 2008, 358, 794–810. [Google Scholar] [CrossRef] [Green Version]
- Malmivaara, A.; Slätis, P.; Heliövaara, M.; Sainio, P.; Kinnunen, H.; Kankare, J.; Dalin-Hirvonen, N.; Seitsalo, S.; Herno, A.; Kortekangas, P.; et al. Surgical or nonoperative treatment for lumbar spinal stenosis? A randomized controlled trial. Spine 2007, 32, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Guha, D.; Heary, R.F.; Shamji, M.F. Iatrogenic spondylolisthesis following laminectomy for degenerative lumbar stenosis: Systematic review and current concepts. Neurosurg. Focus 2015, 39, E9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.K.; Bisson, E.F.; Bydon, M.; Glassman, S.D.; Foley, K.T.; Potts, E.A.; Shaffrey, C.I.; Shaffrey, M.E.; Coric, D.; Knightly, J.J.; et al. Laminectomy alone versus fusion for grade 1 lumbar spondylolisthesis in 426 patients from the prospective Quality Outcomes Database. J. Neurosurg. Spine 2018, 30, 234–241. [Google Scholar] [CrossRef]
- Bridwell, K.H.; Sedgewick, T.A.; O’Brien, M.F.; Lenke, L.G.; Baldus, C. The role of fusion and instrumentation in the treatment of degenerative spondylolisthesis with spinal stenosis. J. Spinal Disord. 1993, 6, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Herkowitz, H.N.; Kurz, L.T. Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J. Bone Jt. Surg. Am. 1991, 73, 802–808. [Google Scholar] [CrossRef]
- Ghogawala, Z.; Dziura, J.; Butler, W.E.; Dai, F.; Terrin, N.; Magge, S.N.; Coumans, J.-V.C.; Harrington, J.F.; Amin-Hanjani, S.; Schwartz, J.S.; et al. Laminectomy plus Fusion versus Laminectomy Alone for Lumbar Spondylolisthesis. N. Engl. J. Med. 2016, 374, 1424–1434. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.; Yuwen, P.; Zhu, Y.; Wei, N.; Feng, C.; Zhang, Y.; Chen, W. Effectiveness of decompression alone versus decompression plus fusion for lumbar spinal stenosis: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2017, 137, 637–650. [Google Scholar] [CrossRef]
- Försth, P.; Ólafsson, G.; Carlsson, T.; Frost, A.; Borgström, F.; Fritzell, P.; Öhagen, P.; Michaëlsson, K.; Sandén, B. A Randomized, Controlled Trial of Fusion Surgery for Lumbar Spinal Stenosis. N. Engl. J. Med. 2016, 374, 1413–1423. [Google Scholar] [CrossRef]
- Schöller, K.; Alimi, M.; Cong, G.-T.; Christos, P.; Härtl, R. Lumbar Spinal Stenosis Associated With Degenerative Lumbar Spondylolisthesis: A Systematic Review and Meta-analysis of Secondary Fusion Rates Following Open vs. Minimally Invasive Decompression. Neurosurgery 2017, 80, 355–367. [Google Scholar] [CrossRef]
- Stevens, K.J.; Spenciner, D.B.; Griffiths, K.L.; Kim, K.D.; Zwienenberg-Lee, M.; Alamin, T.; Bammer, R.; Stevens, K.J.; Spenciner, D.B.; Griffiths, K.L.; et al. Comparison of minimally invasive and conventional open posterolateral lumbar fusion using magnetic resonance imaging and retraction pressure studies. J. Spinal Disord. Tech. 2006, 19, 77–86. [Google Scholar] [CrossRef]
- Kim, D.-Y.; Lee, S.-H.; Chung, S.K.; Lee, H.-Y. Comparison of multifidus muscle atrophy and trunk extension muscle strength: Percutaneous versus open pedicle screw fixation. Spine 2005, 30, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Fan, S.; Hu, Z.; Zhao, F.; Zhao, X.; Huang, Y.; Fang, X. Multifidus muscle changes and clinical effects of one-level posterior lumbar interbody fusion: Minimally invasive procedure versus conventional open approach. Eur. Spine J. 2010, 19, 316–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mobbs, R.J.; Li, J.; Sivabalan, P.; Raley, D.; Rao, P.J. Outcomes after decompressive laminectomy for lumbar spinal stenosis: Comparison between minimally invasive unilateral laminectomy for bilateral decompression and open laminectomy: Clinical article. J. Neurosurg. Spine 2014, 21, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Phan, K.; Mobbs, R.J. Minimally Invasive Versus Open Laminectomy for Lumbar Stenosis: A Systematic Review and Meta-Analysis. Spine 2016, 41, E91–E100. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.S.; Tribus, C.B.; Diab, M.; Ghanayem, A.J. Spondylolisthesis and spondylolysis. J. Bone Jt. Surg. Am. 2008, 90, 656–671. [Google Scholar]
- Boden, S.D.; Wiesel, S.W. Lumbosacral segmental motion in normal individuals. Have we been measuring instability properly? Spine 1991, 16, 855. [Google Scholar] [CrossRef]
- Clark, A.J.; Safaee, M.M.; Khan, N.R.; Brown, M.T.; Foley, K.T. Tubular microdiscectomy: Techniques, complication avoidance, and review of the literature. Neurosurg. Focus. 2017, 43, E7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoo, L.T.; Fessler, R.G. Microendoscopic decompressive laminotomy for the treatment of lumbar stenosis. Neurosurgery 2002, 51, S146–S154. [Google Scholar] [CrossRef]
- Carreon, L.Y.; Bratcher, K.R.; Canan, C.E.; Burke, L.O.; Djurasovic, M.; Glassman, S.D. Differentiating minimum clinically important difference for primary and revision lumbar fusion surgeries. J. Neurosurg. Spine 2013, 18, 102–106. [Google Scholar] [CrossRef]
- Khashan, M.; Lidar, Z.; Salame, K.; Mangel, L.; Lador, R.; Drexler, M.; Sapirstein, E.; Regev, G.J. Minimally Invasive Spinal Decompression in Patients Older Than 75 Years of Age: Perioperative Risks, Complications, and Clinical Outcomes Compared with Patients Younger Than 45 Years of Age. World Neurosurg. 2016, 89, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Ishikura, H.; Ogihara, S.; Oka, H.; Maruyama, T.; Inanami, H.; Miyoshi, K.; Matsudaira, K.; Chikuda, H.; Azuma, S.; Kawamura, N.; et al. Risk factors for incidental durotomy during posterior open spine surgery for degenerative diseases in adults: A multicenter observational study. PLoS ONE 2017, 12, e0188038. [Google Scholar] [CrossRef] [PubMed]
- Herren, C.; Sobottke, R.; Mannion, A.F.; Zweig, T.; Munting, E.; Otten, P.; Pigott, T.; Siewe, J.; Aghayev, E. Incidental durotomy in decompression for lumbar spinal stenosis: Incidence, risk factors and effect on outcomes in the Spine Tango registry. Eur. Spine J. 2017, 26, 2483–2495. [Google Scholar] [CrossRef]
- Weiss, H.; Garcia, R.M.; Hopkins, B.; Shlobin, N.; Dahdaleh, N.S. A Systematic Review of Complications Following Minimally Invasive Spine Surgery Including Transforaminal Lumbar Interbody Fusion. Curr. Rev. Musculoskelet. Med. 2019, 12, 328–339. [Google Scholar] [CrossRef]
- Alimi, M.; Hofstetter, C.P.; Pyo, S.Y.; Paulo, D.; Härtl, R. Minimally invasive laminectomy for lumbar spinal stenosis in patients with and without preoperative spondylolisthesis: Clinical outcome and reoperation rates. J. Neurosurg. Spine 2015, 22, 339–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ee, W.W.G.; Lau, W.L.J.; Yeo, W.; Von Bing, Y.; Yue, W.M. Does minimally invasive surgery have a lower risk of surgical site infections compared with open spinal surgery? Clin. Orthop. Relat. Res. 2014, 472, 1718–1724. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.; Wang, R.; Huo, X.; Xiong, W.; Kang, L.; Xue, Y. Incidence of Surgical Site Infection after Spine Surgery: A Systematic Review and Meta-Analysis. Spine 2020, 45, 208–216. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, J.E.; Eichholz, K.M.; Fessler, R.G. Surgical site infection rates after minimally invasive spinal surgery. J. Neurosurg. Spine 2009, 11, 471–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shousha, M.; Cirovic, D.; Boehm, H. Infection rate after minimally invasive noninstrumented spinal surgery based on 4350 procedures. Spine 2015, 40, 201–205. [Google Scholar] [CrossRef]
- Blumenthal, C.; Curran, J.; Benzel, E.C.; Potter, R.; Magge, S.N.; Harrington, J.F.; Coumans, J.-V.; Ghogawala, Z. Radiographic predictors of delayed instability following decompression without fusion for degenerative grade I lumbar spondylolisthesis. J. Neurosurg. Spine 2013, 18, 340–346. [Google Scholar] [CrossRef]
- Ahmad, S.; Hamad, A.; Bhalla, A.; Turner, S.; Balain, B.; Jaffray, D. The outcome of decompression alone for lumbar spinal stenosis with degenerative spondylolisthesis. Eur. Spine J. 2017, 26, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Koenig, S.; Jauregui, J.J.; Shasti, M.; Jazini, E.; Koh, E.Y.; Banagan, K.E.; Gelb, D.E.; Ludwig, S.C. Decompression Versus Fusion for Grade I Degenerative Spondylolisthesis: A Meta-Analysis. Glob. Spine J. 2019, 9, 155–161. [Google Scholar] [CrossRef] [Green Version]
- Sihvonen, T.; Herno, A.; Paljärvi, L.; Airaksinen, O.; Partanen, J.; Tapaninaho, A. Local denervation atrophy of paraspinal muscles in postoperative failed back syndrome. Spine 1993, 18, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Suwa, H.; Hanakita, J.; Ohshita, N.; Gotoh, K.; Matsuoka, N.; Morizane, A. Postoperative changes in paraspinal muscle thickness after various lumbar back surgery procedures. Neurol. Med. Chir. 2000, 40, 151–154; discussion 154–155. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.J.; Bransford, R.J.; Bellabarba, C.; Chapman, J.R.; Cohen, A.M.; Harrington, R.M.; Ching, R.P. The effect of bilateral laminotomy versus laminectomy on the motion and stiffness of the human lumbar spine: A biomechanical comparison. Spine 2010, 35, 1789–1793. [Google Scholar] [CrossRef]
- Hamasaki, T.; Tanaka, N.; Kim, J.; Okada, M.; Ochi, M.; Hutton, W.C. Biomechanical assessment of minimally invasive decompression for lumbar spinal canal stenosis: A cadaver study. J. Spinal Disord. Tech. 2009, 22, 486–491. [Google Scholar] [CrossRef]
- Bresnahan, L.; Ogden, A.T.; Natarajan, R.N.; Fessler, R.G. A biomechanical evaluation of graded posterior element removal for treatment of lumbar stenosis: Comparison of a minimally invasive approach with two standard laminectomy techniques. Spine 2009, 34, 17–23. [Google Scholar] [CrossRef]
- Ravinsky, R.A.; Crawford, E.J.; Reda, L.A.; Rampersaud, Y.R. Slip progression in degenerative lumbar spondylolisthesis following minimally invasive decompression surgery is not associated with increased functional disability. Eur. Spine J. 2020, 29, 896–903. [Google Scholar] [CrossRef]
- Park, P.; Garton, H.J.; Gala, V.C.; Hoff, J.T.; McGillicuddy, J.E. Adjacent segment disease after lumbar or lumbosacral fusion: Review of the literature. Spine 2004, 29, 1938–1944. [Google Scholar] [CrossRef]
- Chow, D.H.; Luk, K.D.; Evans, J.H.; Leong, J.C. Effects of short anterior lumbar interbody fusion on biomechanics of neighboring unfused segments. Spine 1996, 21, 549–555. [Google Scholar] [CrossRef]



| N | S | p-Value | |
|---|---|---|---|
| Total | 43 | 53 | |
| Male | 27 (63%) | 26 (49%) | 0.22 |
| Age | 65.8 ± 13.2 | 71.5 ± 8.7 | 0.02 |
| BMI | 27.4 ± 6.3 | 28.6 ± 4.5 | 0.47 |
| BMI > 30 | 10 (23%) | 18 (34%) | 0.27 |
| Smoking | 11 (26%) | 12 (23%) | 0.46 |
| ASA score | |||
| I | 5 (12%) | 3 (6%) | 0.49 |
| II | 23 (53%) | 32 (60%) | |
| III | 13 (30%) | 15 (28%) | |
| IV | 2 (5%) | 4 (8%) | |
| Comorbidities | |||
| Cerebrovascular | 4 (9%) | 4 (8%) | 0.52 |
| Renal | 4 (9%) | 1 (2%) | 0.17 |
| Oncological | 3 (7%) | 3 (6%) | 0.56 |
| HTN | 23 (53%) | 37 (70%) | 0.08 |
| DM | 13 (30%) | 17 (32%) | 0.51 |
| Cardiovascular | 27 (63%) | 31 (58%) | 0.68 |
| Other endocrine | 9 (21%) | 12 (23%) | 0.52 |
| N | S | p-Value | |
|---|---|---|---|
| Total | 43 | 53 | |
| LOS | 2.0 ± 1.6 | 3.1 ± 4.2 | 0.01 |
| Complications | 9 (21%) | 5 (9%) | 0.10 |
| Immediate complication | 5 (12%) | 3 (6%) | 0.46 |
| After discharge | 3 (7%) | 3 (6%) | 0.56 |
| Durotomy | 4 (9%) | 3 (6%) | 0.70 |
| Neurological | 1 (42%) | 0 (0%) | 0.45 |
| SSI | 0 (0%) | 2 (4%) | 0.50 |
| Pneumonia | 1 (2%) | 0 (0%) | 0.45 |
| UTI | 0 (0%) | 0 (0%) | - |
| PE/DVT | 0 (0%) | 0 (0%) | - |
| Residual stenosis | 2 (5%) | 1 (2%) | 0.58 |
| Other complications | 0 (0%) | 1 (2%) | 0.55 |
| Revision | 3 (7%) | 3 (6%) | 0.56 |
| Baseline | 1 Year | p-Value 1y-BL | 1 Year | p-Value 1y-BL | ||
|---|---|---|---|---|---|---|
| ODI | All patients | 49.1 ± 21.2 | 21.4 ± 26.1 | <0.01 | 23.4 ± 25.8 | <0.01 |
| N group | 52.8 ± 20.2 | 18.2 ± 24.7 | <0.01 | 25.8 ± 26.9 | <0.01 | |
| S group | 46.2 ± 21.6 | 23.9 ± 27.2 | <0.01 | 21.5 ± 24.9 | <0.01 | |
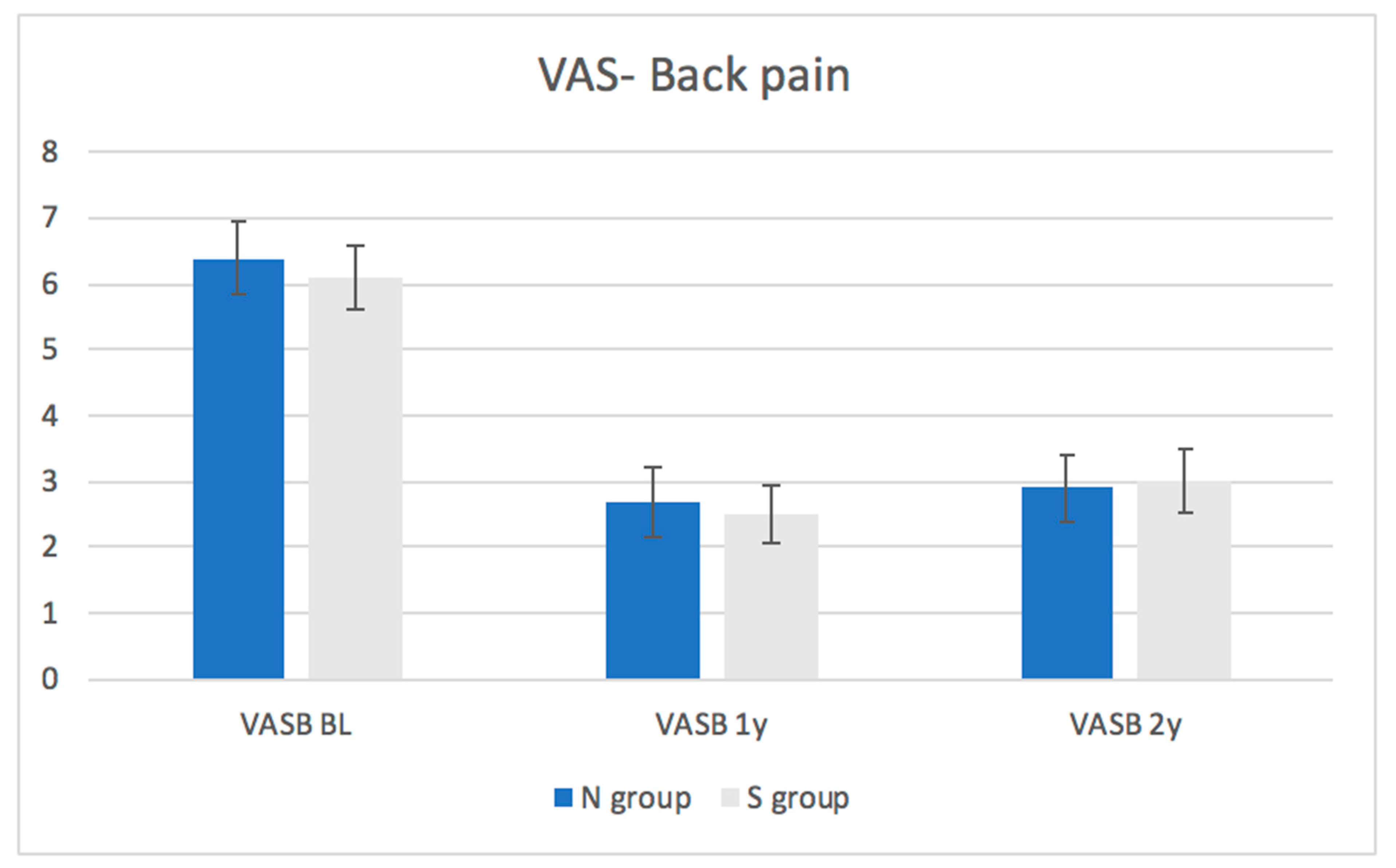
| VAS- Back pain | All patients | 6.2 ± 3.5 | 2.6 ± 3.2 | <0.01 | 2.9 ± 3.5 | <0.01 |
| N group | 6.4 ± 6.4 | 2.7 ± 2.7 | <0.01 | 2.9 ± 2.9 | <0.01 | |
| S group | 6.1 ± 3.4 | 2.6 ± 3.1 | <0.01 | 3.0 ± 3.5 | <0.01 | |
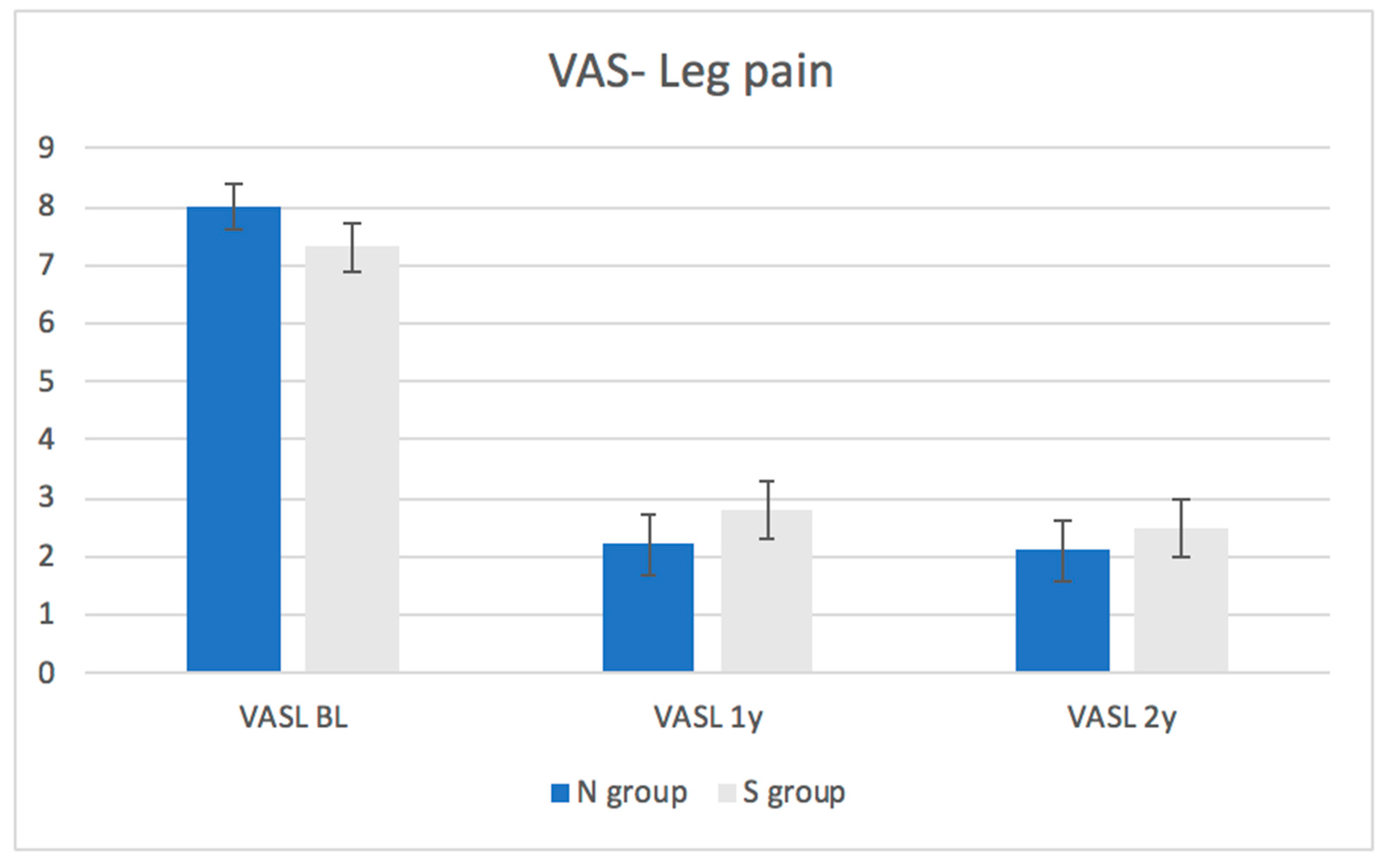
| VAS- Leg pain | All patients | 7.6 ± 2.9 | 2.5 ± 3.5 | <0.01 | 2.3 ± 3.5 | <0.01 |
| N group | 8.0 ± 8.0 | 2.2 ± 2.2 | <0.01 | 2.1 ± 2.1 | <0.01 | |
| S group | 7.3 ± 7.3 | 2.8 ± 2.8 | <0.01 | 2.4 ± 2.4 | <0.01 |
| Total | N | S | p-Value | ||
|---|---|---|---|---|---|
| ODI 1 year | Patients with available scores | 82 | 35 | 47 | |
| Improvement above the MCID | 53 (65%) | 27 (77%) | 27 (57%) | 0.16 | |
| ODI 2 year | Patients with available scores | 68 | 30 | 38 | |
| Improvement above the MCID | 45 (66%) | 23 (77%) | 22 (58%) | 0.12 | |
| VASB 1 year | Patients with available scores | 80 | 33 | 47 | |
| Improvement above the MCID | 44 (55%) | 16 (48%) | 28 (60%) | 0.16 | |
| VASB 2 year | Patients with available scores | 67 | 28 | 39 | |
| Improvement above the MCID | 39 (58%) | 14 (50%) | 25 (64%) | 0.31 | |
| VASL 1 year | Patients with available scores | 79 | 33 | 46 | |
| Improvement above the MCID | 55 (70%) | 24 (73%) | 31 (67%) | 0.8 | |
| VASL 2 year | Patients with available scores | 64 | 28 | 36 | |
| Improvement above the MCID | 41 (64%) | 17 (61%) | 24 (67%) | 0.79 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khashan, M.; Salame, K.; Ofir, D.; Lidar, Z.; Regev, G.J. Stable Low-Grade Degenerative Spondylolisthesis Does Not Compromise Clinical Outcome of Minimally Invasive Tubular Decompression in Patients with Spinal Stenosis. Medicina 2021, 57, 1270. https://doi.org/10.3390/medicina57111270
Khashan M, Salame K, Ofir D, Lidar Z, Regev GJ. Stable Low-Grade Degenerative Spondylolisthesis Does Not Compromise Clinical Outcome of Minimally Invasive Tubular Decompression in Patients with Spinal Stenosis. Medicina. 2021; 57(11):1270. https://doi.org/10.3390/medicina57111270
Chicago/Turabian StyleKhashan, Morsi, Khalil Salame, Dror Ofir, Zvi Lidar, and Gilad J. Regev. 2021. "Stable Low-Grade Degenerative Spondylolisthesis Does Not Compromise Clinical Outcome of Minimally Invasive Tubular Decompression in Patients with Spinal Stenosis" Medicina 57, no. 11: 1270. https://doi.org/10.3390/medicina57111270
APA StyleKhashan, M., Salame, K., Ofir, D., Lidar, Z., & Regev, G. J. (2021). Stable Low-Grade Degenerative Spondylolisthesis Does Not Compromise Clinical Outcome of Minimally Invasive Tubular Decompression in Patients with Spinal Stenosis. Medicina, 57(11), 1270. https://doi.org/10.3390/medicina57111270