
Characteristics and Short-Term Surgical Outcomes of Patients with Recurrent Lumbar Disc Herniation after Percutaneous Laser Disc Decompression

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Approval
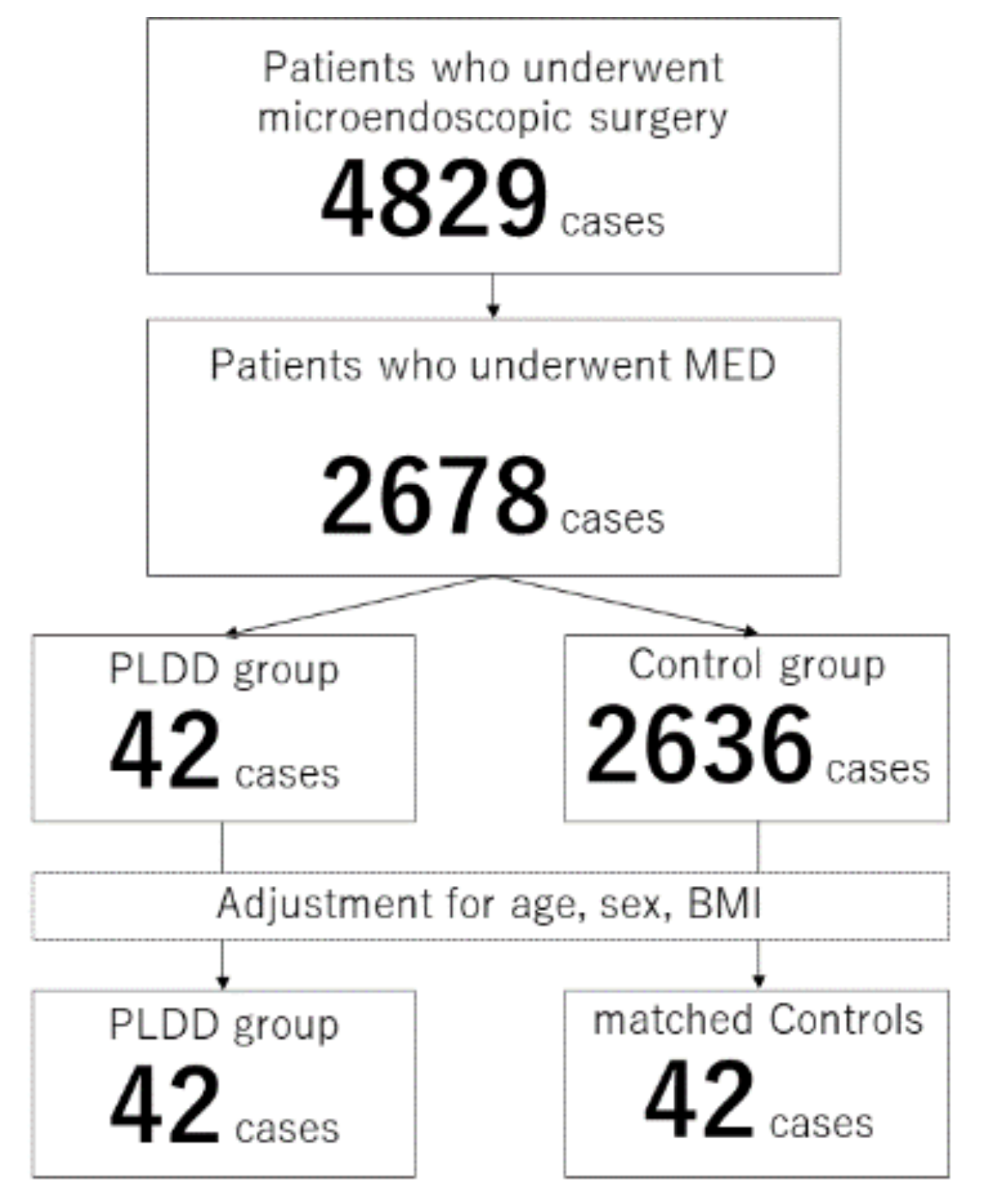
2.2. Study Population
2.3. Surgical Criteria and Preoperative Care
2.4. Collective Data
2.4.1. Preoperative Data
2.4.2. Radiologic Data
2.4.3. Surgical Data
2.4.4. Clinical Scores
2.5. Statistical Analysis
3. Results
3.1. Overall Comparisons
3.2. Comparisons between the PLDD Group and the Matched Control Group
3.3. Preoperative Data
3.4. Radiographic Findings
3.5. Surgical Data
3.6. Postoperative Clinical Score
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Benzakour, T.; Igoumenou, V.; Mavrogenis, A.F.; Benzakour, A. Current concepts for lumbar disc herniation. Int. Orthop. 2019, 43, 841–851. [Google Scholar] [CrossRef]
- Postacchini, F. Management of herniation of the lumbar disc. J. Bone Jt. Surg. Br. Vol. 1999, 81, 567–576. [Google Scholar] [CrossRef]
- Luo, X.; Pietrobon, R.; Sun, S.X.; Liu, G.G.; Hey, L. Estimates and Patterns of Direct Health Care Expenditures among Individuals with Back Pain in the United States. Spine 2004, 29, 79–86. [Google Scholar] [CrossRef]
- Kreiner, D.S.; Hwang, S.W.; Easa, J.E.; Resnick, D.K.; Baisden, J.L.; Bess, S.; Cho, C.H.; DePalma, M.J.; Dougherty, P.; Fernand, R.; et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014, 14, 180–191. [Google Scholar] [CrossRef]
- Barrios, C.; Ahmed, M.; Arrótegui, J.; Björnsson, A.; Gillström, P. Microsurgery Versus Standard Removal of the Herniated Lumbar Disc: A 3-year Comparison in 150 Cases. Acta Orthop. Scand. 1990, 61, 399–403. [Google Scholar] [CrossRef]
- Virk, S.S.; Diwan, A.; Phillips, F.M.; Sandhu, H.; Khan, S.N. What is the Rate of Revision Discectomies after Primary Discectomy on a National Scale? Clin. Orthop. Relat. Res. 2017, 475, 2752–2762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brouwer, P.A.; Brand, R.; van den Akker-van Marle, M.E.; Jacobs, W.C.; Schenk, B.; van den Berg-Huijsmans, A.A.; Koes, B.; van Buchem, M.A.; Arts, M.P.; Peul, W.C. Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: A randomized controlled trial. Spine J. 2015, 15, 857–865. [Google Scholar] [CrossRef] [PubMed]
- McCormick, Z.L.; Slipman, C.; Kotcharian, A.; Chhatre, A.; Bender, F.J.; Salam, A.; Menkin, S.; Kennedy, D.J.; Plastaras, C. Percutaneous Lumbar Disc Decompression Using the Dekompressor: A Prospective Long-Term Outcome Study. Pain Med. 2016, 17, 1023–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choy, D.S.; Hellinger, J.; Hellinger, S.; Tassi, G.P.; Lee, S.-H. 23rd Anniversary of Percutaneous Laser Disc Decompression (PLDD). Photomed. Laser Surg. 2009, 27, 535–538. [Google Scholar] [CrossRef]
- Ebeling, U.; Kalbarcyk, H.; Reulen, H.J. Microsurgical reoperation following lumbar disc surgery. J. Neurosurg. 1989, 70, 397–404. [Google Scholar] [CrossRef]
- Alvi, M.A.; Kerezoudis, P.; Wahood, W.; Goyal, A.; Bydon, M. Operative Approaches for Lumbar Disc Herniation: A Systematic Review and Multiple Treatment Meta-Analysis of Conventional and Minimally Invasive Surgeries. World Neurosurg. 2018, 114, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Minamide, A.; Yoshida, M.; Simpson, A.K.; Nakagawa, Y.; Iwasaki, H.; Tsutsui, S.; Takami, M.; Hashizume, H.; Yukawa, Y.; Yamada, H. Minimally invasive spinal decompression for degenerative lumbar spondylolisthesis and stenosis maintains stability and may avoid the need for fusion. Bone Jt. J. 2018, 100, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Pfirrmann, C.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic Resonance Classification of Lumbar Intervertebral Disc Degeneration. Spine 2001, 26, 1873–1878. [Google Scholar] [CrossRef] [PubMed]
- Emch, T.M.; Modic, M.T. Imaging of lumbar degenerative disk disease: History and current state. Skelet. Radiol. 2011, 40, 1175–1189. [Google Scholar] [CrossRef]
- Fujiwara, A.; Kobayashi, N.; Saiki, K.; Kitagawa, T.; Tamai, K.; Saotome, K. Association of the Japanese Orthopaedic Associ-ation score with the Oswestry Disability Index, Roland-Morris Disability Questionnaire, and Short-Form 36. Spine 2003, 28, 1601–1607. [Google Scholar] [CrossRef]
- Fairbank, J.C.T.; Couper, J.; Davies, J.B.; O’Brien, J.P. Oswestry Low Back Pain Disability Questionnaire. Physiotherapy 1980, 66, 271–273. [Google Scholar] [CrossRef]
- Haberman, S.J. The Analysis of Residuals in Cross-Classified Tables. Biometrics 1973, 29, 205. [Google Scholar] [CrossRef]
- Rubin, D.B. The designversus the analysis of observational studies for causal effects: Parallels with the design of randomized trials. Stat. Med. 2006, 26, 20–36. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.C.; Kabo, J.M.; Tsou, P.M.; Halevi, L.; Shamie, A.N. The effect of uniform heating on the biomechanical properties of the intervertebral disc in a porcine model. Spine J. 2005, 5, 64–70. [Google Scholar] [CrossRef]
- Burton, C.V.; Kirkaldy-Willis, W.H.; Yong-Hing, K.; Heithoff, K.B. Causes of Failure of Surgery on the Lumbar Spine. Clin. Orthop. Relat. Res. 1981, 157, 191–199. [Google Scholar] [CrossRef]
- Ross, J.S.; Robertson, J.T.; Frederickson, R.C.; Petrie, J.L.; Obuchowski, N.; Modic, M.T.; de Tribolet, N. Association between perid-ural scar and recurrent radicular pain after lumbar discectomy: Magnetic resonance evaluation. ADCON-L European Study Group. Neurosurgery 1996, 38, 855–861. [Google Scholar] [CrossRef] [Green Version]
- Akhgar, J.; Terai, H.; Rahmani, M.S.; Tamai, K.; Suzuki, A.; Toyoda, H.; Hoshino, M.; Ikebuchi, M.; Ahmadi, S.A.; Hayashi, K.; et al. Anatomical analysis of the relation between human ligamentum flavum and posterior spinal bony prominence. J. Orthop. Sci. 2017, 22, 260–265. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall Patients | PLDD Group | Control Group | p Value | |
|---|---|---|---|---|
| Number | 2578 | 42 (1.6%) | 2636 (98.4%) | |
| Age (years) | 48.2 ± 16.9 | 45.4 ± 14.9 | 48.3 ± 16.9 | 0.203 # |
| Sex (Female/Male) | 913/1765 | 6/36 | 907/1729 | 0.005 † |
| Body weight (kg) | 66.1 ± 13.2 | 70.9 ± 11.8 | 66.0 ± 13.3 | 0.007 # |
| Body height (cm) | 166.3 ± 9.3 | 169.5 ± 8.6 | 166.3 ± 9.3 | 0.024 # |
| BMI (kg/m2) | 23.8 ± 3.7 | 24.6 ± 2.9 | 23.8 ± 3.8 | 0.050 # |
| Preop JOA score | 12.6 ± 5.3 | 13.3 ± 4.6 | 12.6 ± 5.4 | 0.353 # |
| Preop ODI score | 47.9 ± 20.5 | 42.4 ± 20.1 | 48.0 ± 20.6 | 0.123 # |
| PLDD Group | Matched Controls | p Value | |
|---|---|---|---|
| Number | 42 | 42 | |
| Age (years old) | 45.4 ± 14.9 | 46.9 ± 17.1 | 0.664 # |
| Sex (Female/Male) | 6/36 | 4/38 | 0.738 † |
| Body height (cm) | 169.4 ± 8.6 | 168.4 ± 7.4 | 0.534 # |
| Body weight (kg) | 70.9 ± 11.8 | 66.7 ± 9.9 | 0.098 # |
| BMI (kg/m2) | 24.7 ± 3.0 | 23.6 ± 3.3 | 0.144 # |
| Comorbidity | |||
| Diabetes mellitus | 1 (2.4%) | 2 (4.8%) | 1.000 † |
| Hypertension | 4 (9.5%) | 5 (11.9%) | 1.000 † |
| Cardiac disease | 2 (4.8%) | 4 (9.5%) | 1.000 † |
| Respiratory disease | 1 (2.4%) | 3 (7.1%) | 0.616 † |
| Cerebrovascular disorders | 0 | 0 | 1.000 † |
| Preoperative symptoms | |||
| Motor weakness (MMT ≤ 4) | 7 (16.7%) | 9 (21.4%) | 0.782 † |
| Bowel bladder disfunction | 0 | 9 (21.4%) | 1.000 † |
| JOA score | 13.3 ± 4.6 | 11.6 ± 4.6 | 0.110 # |
| ODI score | 42.4 ± 20.1 | 47.2 ± 19.7 | 0.290 # |
| PLDD Group | Matched Controls | p Value | |
|---|---|---|---|
| Pfirrmann classification | 0.157 † | ||
| No/mild degeneration (Grade 1, 2, or 3) | 8 (19.0%) | 13 (31.0%) | |
| Severe degeneration (Grade 4 or 5) | 34 (81.0%) | 29 (69.0%) | |
| Modic change | 0.028 † | ||
| Negative | 14 (33.3%) | 25 (59.5%) | |
| Positive (Type 1, 2, or 3) | 28 (66.7%) | 17 (40.5%) | |
| Herniation pattern | 0.016 † | ||
| Subligamentous extrusion | 17 (40.5%) | 7 (16.7%) | >0.05 * |
| Transligamentous extrusion | 21 (50.0%) | 23 (54.8%) | |
| Sequestration | 4 (9.5%) | 12 (28.6%) | >0.05 * |
| PLDD Group | Matched Controls | p Value | |
|---|---|---|---|
| Total surgical time (min) | 69.2 ± 31.4 | 67.3 ± 39.1 | 0.866 # |
| Findings during surgery | |||
| Nerve root adhesion | 7 (16.7%) | 3 (7.1%) | 0.156 † |
| Dural injury | 2 (4.8%) | 1 (2.4%) | 1.000 † |
| Hard disc herniation | 6 (14.3%) | 0 | 0.026 † |
| Neurological deterioration | 0 | 0 | 1.000 † |
| In hospital period (days) | 6.2 ± 1.8 | 6.1 ± 1.2 | 0.897 # |
| Additional pain killer use | 1.0 ± 0.9 | 0.9 ± 1.0 | 0.649 # |
| Hematoma on postoperative MRI | 2 (4.8%) | 3 (7.1%) | 1.000 † |
| Recurrence of same level LDH | 1 (2.4%) | 2 (4.8%) | 1.000 † |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terai, H.; Tamai, K.; Iwamae, M.; Kaneda, K.; Katsuda, H.; Shimada, N.; Nakamura, H. Characteristics and Short-Term Surgical Outcomes of Patients with Recurrent Lumbar Disc Herniation after Percutaneous Laser Disc Decompression. Medicina 2021, 57, 1225. https://doi.org/10.3390/medicina57111225
Terai H, Tamai K, Iwamae M, Kaneda K, Katsuda H, Shimada N, Nakamura H. Characteristics and Short-Term Surgical Outcomes of Patients with Recurrent Lumbar Disc Herniation after Percutaneous Laser Disc Decompression. Medicina. 2021; 57(11):1225. https://doi.org/10.3390/medicina57111225
Chicago/Turabian StyleTerai, Hidetomi, Koji Tamai, Masayoshi Iwamae, Kunikazu Kaneda, Hiroshi Katsuda, Nagakazu Shimada, and Hiroaki Nakamura. 2021. "Characteristics and Short-Term Surgical Outcomes of Patients with Recurrent Lumbar Disc Herniation after Percutaneous Laser Disc Decompression" Medicina 57, no. 11: 1225. https://doi.org/10.3390/medicina57111225
APA StyleTerai, H., Tamai, K., Iwamae, M., Kaneda, K., Katsuda, H., Shimada, N., & Nakamura, H. (2021). Characteristics and Short-Term Surgical Outcomes of Patients with Recurrent Lumbar Disc Herniation after Percutaneous Laser Disc Decompression. Medicina, 57(11), 1225. https://doi.org/10.3390/medicina57111225