Botulinum Toxin A Injection for the Treatment of Intractable Dry Eye Disease


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Nelson, J.D.; Craig, J.P.; Akpek, E.K.; Azar, D.T.; Belmonte, C.; Bron, A.J.; Clayton, J.A.; Dogru, M.; Dua, H.S.; Foulks, G.N.; et al. TFOS DEWS II Introduction. Ocul. Surf. 2017, 15, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Uchino, M.; Schaumberg, D.A. Dry eye disease: Impact on quality of life and vision. Curr. Ophthalmol. Rep. 2013, 1, 51–57. [Google Scholar] [CrossRef] [Green Version]
- Nigam, P.K.; Nigam, A. Botulinum toxin. Indian J. Dermatol. 2010, 55, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Petrillo, F.; Pignataro, D.; Lavano, M.A.; Santella, B.; Folliero, V.; Zannella, C.; Astarita, C.; Gagliano, C.; Franci, G.; Avitabile, T.; et al. Current Evidence on the Ocular Surface Microbiota and Related Diseases. Microorganisms 2020, 8, 1033. [Google Scholar] [CrossRef] [PubMed]
- Spiera, H.; Asbell, P.A.; Simpson, D.M. Botulinum toxin increases tearing in patients with Sjögren’s syndrome: A preliminary report. J. Rheumatol. 1997, 24, 1842–1843. [Google Scholar] [PubMed]
- Sahlin, S.; Chen, E.; Kaugesaar, T.; Almqvist, H.; Kjellberg, K.; Lennerstrand, G. Effect of eyelid botulinum toxin injection on lacrimal drainage. Am. J. Ophthalmol. 2000, 129, 481–486. [Google Scholar] [CrossRef]
- Chun, Y.S.; Kim, J.C. Treatment of superior limbic keratoconjunctivitis with a large-diameter contact lens and Botulium Toxin, A. Cornea 2009, 28, 752–758. [Google Scholar]
- Choi, M.G.; Yeo, J.H.; Kang, J.W.; Chun, Y.S.; Lee, J.K.; Kim, J.C. Effects of botulinum toxin type A on the treatment of dry eye disease and tear cytokines. Graefe’s Arch. Clin. Exp. Ophthalmol. 2019, 257, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Serna-Ojeda, J.C.; Nava-Castaneda, A. Paralysis of the orbicularis muscle of the eye using botulinum toxin type A in the treatment for dry eye. Acta Ophthalmol. 2017, 95, e132–e137. [Google Scholar] [CrossRef]
- Horwath-Winter, J.; Bergloeff, J.; Floegel, I.; Haller-Schober, E.M.; Schmut, O. Botulinum toxin A treatment in patients suffering from blepharospasm and dry eye. Br. J. Ophthalmol. 2003, 87, 54–56. [Google Scholar] [CrossRef]
- Schiffman, R.M.; Christianson, M.D.; Jacobsen, G.; Hirsch, J.D.; Reis, B.L. Reliability and validity of the Ocular Surface Disease Index. Arch. Ophthalmol. 2000, 118, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Jang, S.Y.; Lee, S.Y.; Yoon, J.S. Meibomian gland dysfunction in longstanding prosthetic eye wearers. Br. J. Ophthalmol. 2013, 97, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Bukhari, A.A. Botulinum neurotoxin type A versus punctal plug insertion in the management of dry eye disease. Oman J. Ophthalmol. 2014, 7, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Park, D.I.; Shin, H.M.; Lee, S.Y.; Lew, H. Tear production and drainage after botulinum toxin A injection in patients with essential blepharospasm. Acta Ophthalmol. 2013, 91, e108–e112. [Google Scholar] [CrossRef]
- Fouda, S.M.; Mattout, H.K. Comparison between botulinum toxin A injection and lacrimal punctal plugs for the control of post-LASIK dry eye manifestations: A prospective study. Ophthalmol. Ther. 2017, 6, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Isshiki, Y.; Ishikawa, H.; Mimura, O. Changes in ocular higher-order aberrations following botulinum toxin treatment in patients with blepharospasm: BTX improves dry eye in patients with BEB. Jpn. J. Ophthalmol. 2016, 60, 486–491. [Google Scholar] [CrossRef]
- Ho, M.C.; Hsu, W.C.; Hsieh, Y.T. Botulinum toxin type A injection for lateral canthal rhytids: Effect on tear film stability and tear production. JAMA Ophthalmol. 2014, 132, 332–337. [Google Scholar] [CrossRef] [Green Version]
- Wolffsohn, J.S.; Arita, R.; Chalmers, R.; Djalilian, A.; Dogru, M.; Dumbleton, K.; Gupta, P.K.; Karpecki, P.; Lazreg, S.; Pult, H.; et al. TFOS DEWS II diagnostic methodology report. Ocul. Surf. 2017, 15, 539–574. [Google Scholar] [CrossRef]
- Nichols, K.K.; Mitchell, G.L.; Zadnik, K. The repeatability of clinical measurements of dry eye. Cornea 2004, 23, 272–285. [Google Scholar] [CrossRef] [PubMed]
- Gumus, K.; Lee, S.; Yen, M.T.; Pflugfelder, S.C. Botulinum toxin injection for the management of refractory filamentary keratitis. Arch. Ophthalmol. 2012, 130, 446–450. [Google Scholar] [PubMed] [Green Version]
- Bourkiza, R.; Lee, V. A review of the complications of lacrimal occlusion with punctal and canalicular plugs. Orbit 2012, 31, 86–93. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Before | 1 Month after BTA Injection | p Value | |
|---|---|---|---|
| OSDI score | 62.22 ± 21.30 | 47.98 ± 17.23 | <0.001 |
| Tear osmolarity (mOsm/L) * | 320.82 ± 24.66 | 302.75 ± 22.33 | <0.001 |
| Schirmer test (mm) | 6.11 ± 2.51 | 7.18 ± 4.13 | 0.100 |
| TBUT (sec) | 3.07 ± 0.97 | 3.30 ± 1.06 | 0.229 |
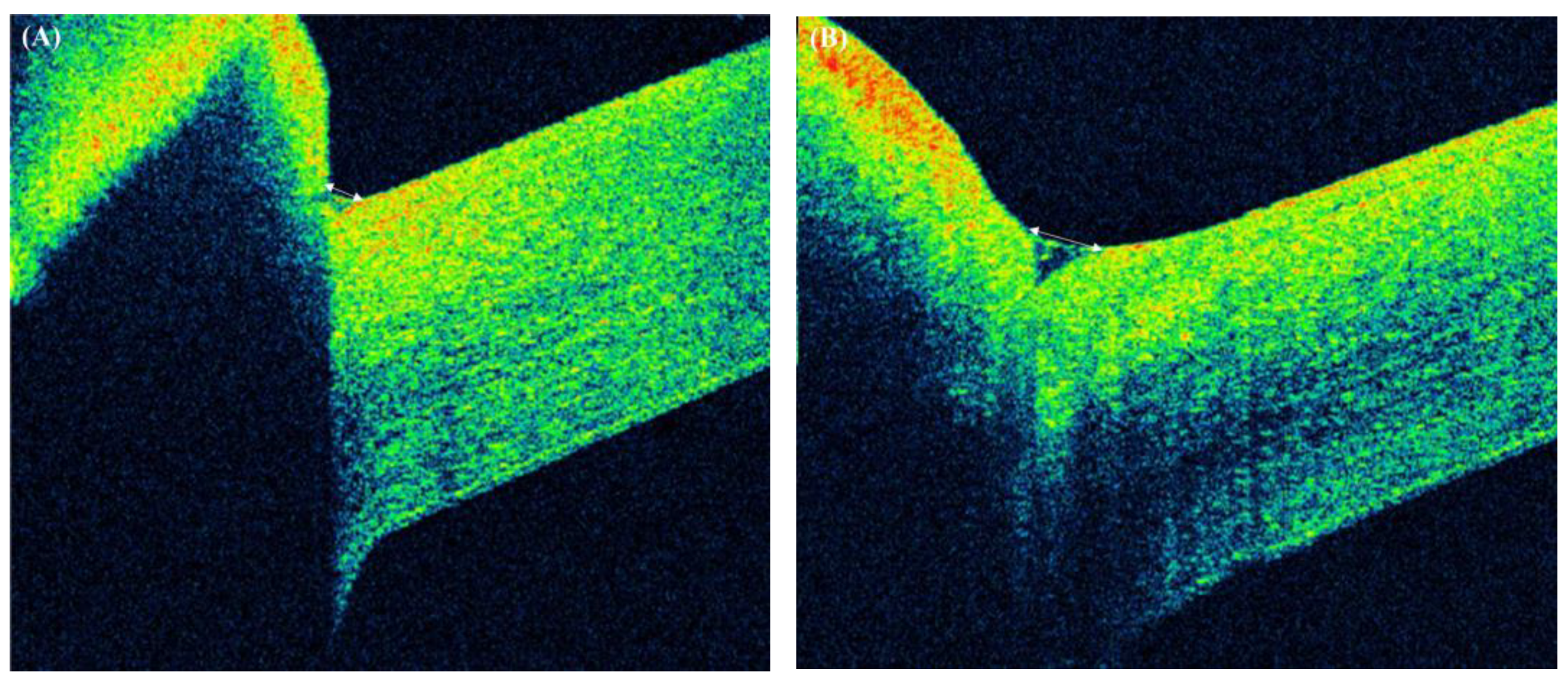
| TMH (mm) | 82.25 ± 40.50 | 138.02 ± 66.62 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, E.W.; Yeom, D.J.; Jang, S.Y. Botulinum Toxin A Injection for the Treatment of Intractable Dry Eye Disease. Medicina 2021, 57, 247. https://doi.org/10.3390/medicina57030247
Choi EW, Yeom DJ, Jang SY. Botulinum Toxin A Injection for the Treatment of Intractable Dry Eye Disease. Medicina. 2021; 57(3):247. https://doi.org/10.3390/medicina57030247
Chicago/Turabian StyleChoi, Eun Woo, Dong Ju Yeom, and Sun Young Jang. 2021. "Botulinum Toxin A Injection for the Treatment of Intractable Dry Eye Disease" Medicina 57, no. 3: 247. https://doi.org/10.3390/medicina57030247
APA StyleChoi, E. W., Yeom, D. J., & Jang, S. Y. (2021). Botulinum Toxin A Injection for the Treatment of Intractable Dry Eye Disease. Medicina, 57(3), 247. https://doi.org/10.3390/medicina57030247