
Strong Genetic Effects on Bone Mineral Density in Multiple Locations with Two Different Techniques: Results from a Cross-Sectional Twin Study

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Study Design
2.2. Bone Mineral Density Assessment
2.3. Statistical Analysis
3. Results
3.1. Study Population
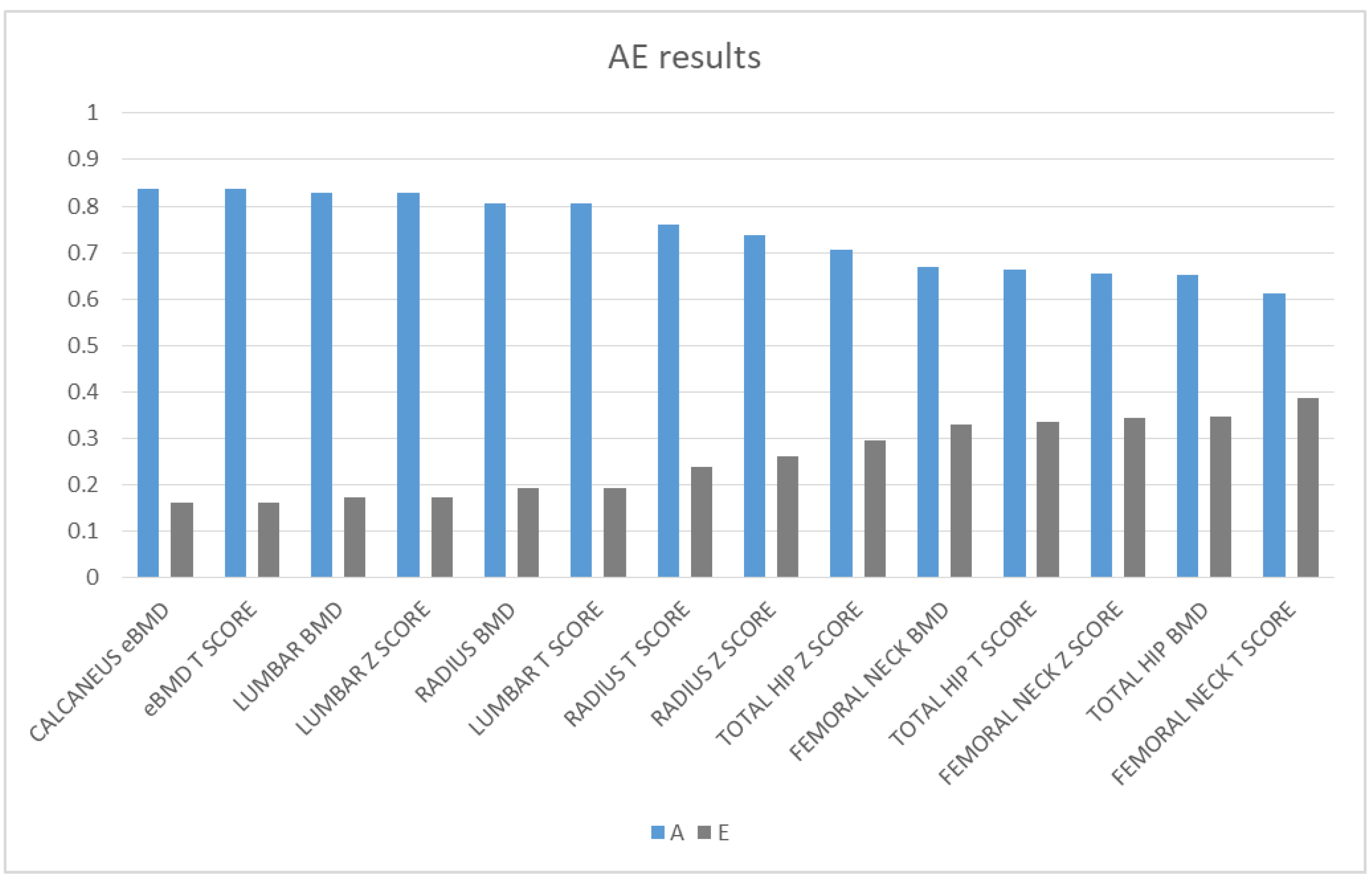
3.2. Heritability of Bone Mineral Density
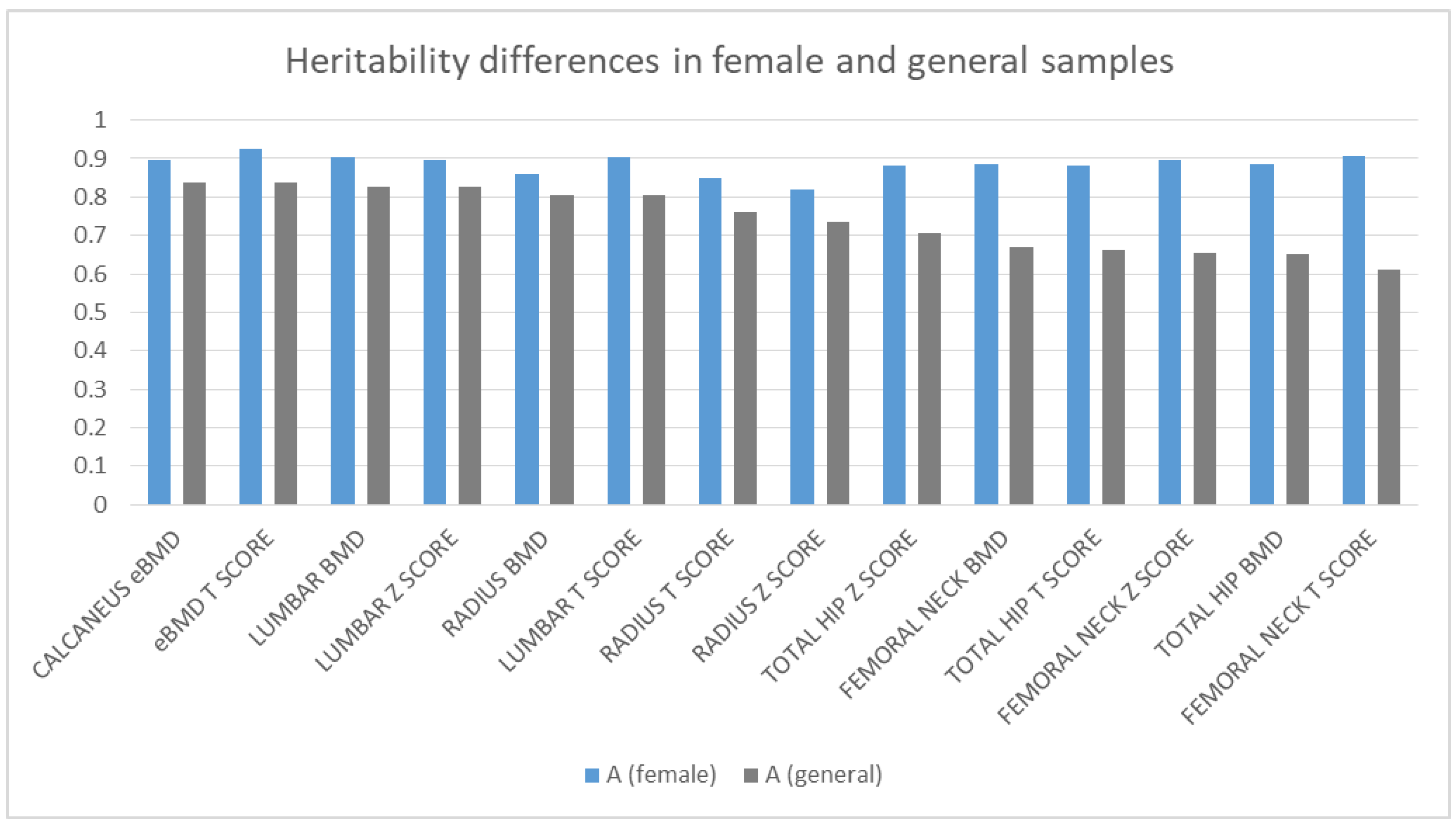
3.3. Differences between Genders
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boomsma, I.D.; Busjahn, A.; Peltonen, L. Classical twin studies and beyond. Nat. Rev. Genet. 2002, 3, 872–882. [Google Scholar] [CrossRef]
- Arden, N.; Baker, J.; Hogg, C.; Baan, K.; Spector, T. The heritability of bone mineral density, ultrasound of the calcaneus and hip axis length: A study of postmenopausal twins. J. Bone Miner. Res. 2009, 11, 530–534. [Google Scholar] [CrossRef]
- Koromani, F.; Trajanoska, K.; Rivadeneira, F.; Oei, L. Recent Advances in the Genetics of Fractures in Osteoporosis. Front. Endocrinol. 2019, 10, 337. [Google Scholar] [CrossRef] [Green Version]
- Zheng, H.; Forgetta, V.; Hsu, Y.; Estrada, K.; Rosello-Diez, A.; Leo, P.J.; Dahia, C.L.; Park-Min, K.H.; Tobias, J.H.; Kooperberg, C.; et al. Whole-genome sequencing identifies EN1 as a determinant of bone density and fracture. Nat. Cell Biol. 2015, 526, 112–117. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.B.; Rivadeneira, F.; Inouye, M.; Pastinen, T.M.; Soranzo, N.; Wilson, S.G.; Andrew, T.; Falchi, M.; Gwilliam, R.; Ahmadi, K.R.; et al. Bone mineral density, osteoporosis, and osteoporotic fractures: A genome-wide association study. Lancet 2008, 371, 1505–1512. [Google Scholar] [CrossRef] [Green Version]
- Styrkarsdottir, U.; Halldorsson, B.V.; Gretarsdottir, S.; Gudbjartsson, D.F.; Walters, G.B.; Ingvarsson, T.; Jonsdottir, T.; Saemundsdottir, J.; Center, J.R.; Nguyen, T.V.; et al. Multiple Genetic Loci for Bone Mineral Density and Fractures. New Engl. J. Med. 2008, 358, 2355–2365. [Google Scholar] [CrossRef] [Green Version]
- Genetic Factors Osteoporosis. The Genetic Factors for Osteoporosis (GEFOS) Consortium Twenty bone-mineral-density loci identified by large-scale meta-analysis of genome-wide association studies. Nat. Genet. 2009, 41, 1199–1206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estrada, K.; Styrkarsdottir, U.; Evangelou, E.; Hsu, Y.H.; Duncan, E.L.; Ntzani, E.E.; Oei, L.; Albagha, O.M.; Amin, N.; Kemp, J.P.; et al. Genome-wide meta-analysis identifies 56 bone mineral density loci and reveals 14 loci associated with risk of fracture. Nat. Genet. 2012, 44, 491–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Styrkarsdottir, U.; Halldorsson, B.V.; Gretarsdottir, S.; Gudbjartsson, D.F.; Walters, G.B.; Ingvarsson, T.; Jonsdottir, T.; Saemundsdottir, J.; Snorradóttir, S.; Center, J.R.; et al. New sequence variants associated with bone mineral density. Nat. Genet. 2008, 41, 15–17. [Google Scholar] [CrossRef]
- Littvay, L.; Métneki, J.; Tarnoki, A.D.; Tarnoki, D.L. The Hungarian Twin Registry. Twin Res. Hum. Genet. 2013, 16, 185–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heath, A.C.; Nyholt, D.R.; Neuman, R.; Madden, P.A.; Bucholz, K.K.; Todd, R.D.; Nelson, E.C.; Montgomery, G.W.; Martin, N.G. Zygosity diagnosis in the absence of genotypic data: An approach using latent class analysis. Twin Res. 2003, 6, 22–26. [Google Scholar] [CrossRef]
- Neale, M.C.; Hunter, M.D.; Pritikin, J.N.; Zahery, M.; Brick, T.R.; Kirkpatrick, R.M.; Estabrook, R.; Bates, T.C.; Maes, H.H.; Boker, S.M. OpenMx 2.0: Extended Structural Equation and Statistical Modeling. Psychometrika 2016, 81, 535–549. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing: Vienna, Australia, 2016. Available online: https://www.R-project.org (accessed on 1 July 2019).
- Neale, M.C.; Cardon, L.R. Methodology for Genetic Studies of Twins and Families; Springer Science and Business Media LLC: Berlin/Heidelberg, Germany; Kluwer Academic Publishers B.V: Dordrecht, The Netherlands, 2013; Volume 67. [Google Scholar]
- Pritikin, J.N.; Rappaport, L.M.; Neale, M.C. Likelihood-Based Confidence Intervals for a Parameter With an Upper or Lower Bound. Struct. Equ. Model. Multidiscip. J. 2017, 24, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Peacock, M.; Turner, C.H.; Econs, M.J.; Foroud, T. Genetics of osteoporosis. Endocr. Rev. 2002, 23, 303–326. [Google Scholar] [CrossRef]
- Yang, T.-L.; Shen, H.; Liu, A.; Dong, S.-S.; Zhang, L.; Deng, F.-Y.; Zhao, Q.; Deng, H.-W. A road map for understanding molecular and genetic determinants of osteoporosis. Nat. Rev. Endocrinol. 2019, 16, 91–103. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.W.; Mahaney, M.C.; Williams, J.T.; Li, J.; Conway, T.; Davies, K.M.; Li, J.L.; Deng, H.; Recker, R.R. Relevance of the genes for bone mass variation to susceptibility to osteoporotic fractures and its implica-tions to gene search for complex human diseases. Genet. Epidemiol. 2002, 22, 12–25. [Google Scholar] [CrossRef] [PubMed]
- Glüer, C.C.; Wu, C.Y.; Jergas, M.; Goldstein, S.A.; Genant, H.K. Three quantitative ultrasound parameters reflect bone structure. Calcif. Tissue Int. 1994, 55, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Pan, F.; Wu, F.; Squibb, K.; Thomson, R.; Winzenberg, T.; Jones, G. Familial resemblance in trabecular and cortical volumetric bone mineral density and bone microarchitecture as measured by HRpQCT. Bone 2018, 110, 76–83. [Google Scholar] [CrossRef]
- Rocha-Braz, M.G.M.; França, M.M.; Fernandes, A.M.; Lerario, A.M.; Zanardo, A.E.; De Santana, L.S.; Kulikowski, L.D.; Martin, R.M.; Mendonca, B.B.; Ferraz-De-Souza, B. Comprehensive Genetic Analysis of 128 Candidate Genes in a Cohort With Idiopathic, Severe, or Familial Osteoporosis. J. Endocr. Soc. 2020, 4, bvaa148. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; He, J.; Qi, L.; Wang, C.; Yue, H.; Gu, J.; Zhang, H.; Wang, Y.; Zhang, Z. Association of HIVEP3 Gene and Lnc RNA with Femoral Neck Bone Mineral Content and Hip Geometry by Genome-Wide Association Analysis in Chinese People. Int. J. Endocrinol. 2020, 2020, 1–8. [Google Scholar] [CrossRef]
- Zhang, H.; Liu, L.; Ni, J.-J.; Wei, X.-T.; Feng, G.-J.; Yang, X.-L.; Xu, Q.; Zhang, Z.-J.; Hai, R.; Tian, Q.; et al. Pleiotropic loci underlying bone mineral density and bone size identified by a bivariate genome-wide association analysis. Osteoporos. Int. 2020, 31, 1691–1701. [Google Scholar] [CrossRef] [PubMed]
- Kaprio, J. Twins and the mystery of missing heritability: The contribution of gene-environment interactions. J. Intern. Med. 2012, 272, 440–448. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.-C.; Greenbaum, J.; Shen, H.; Deng, H.-W. Association Between Gut Microbiota and Bone Health: Potential Mechanisms and Prospective. J. Clin. Endocrinol. Metab. 2017, 102, 3635–3646. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Gao, W.; Wang, B.; Zhao, H.; Zeng, Y.; Ji, Y.; Hao, D. Diversity analysis of gut microbiota in osteoporosis and osteopenia patients. PeerJ 2017, 5, e3450. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Total (n = 216) | MZ (n = 124) | DZ (n = 92) |
|---|---|---|---|
| Sex | 72:28 | 66:34 | 80:20 |
| Age | 54.2 ± 14.3 | 52.34 * ± 14.48 | 56.76 * ± 13.72 |
| BMI | 25.63 ± 4.72 | 25.2 ± 4.54 | 26.2 ± 4.92 |
| LUMBAR BMD | 1 ± 0.15 | 1 ± 0.15 | 0.99 ± 0.16 |
| LUMBAR Z SCORE | 0.35 ± 1.25 | 0.28 ± 1.23 | 0.44 ± 1.26 |
| LUMBAR T SCORE | −0.73 ± 1.38 | −0.68 ± 1.37 | −0.8 ± 1.41 |
| FEMORAL NECK BMD | 0.79 ± 0.15 | 0.8 ± 0.16 | 0.77 ± 0.13 |
| FEMORAL NECK Z SCORE | 0.23 ± 1 | 0.22 ± 1.06 | 0.25 ± 0.92 |
| FEMORAL NECK T SCORE | −0.94 ± 1.08 | −0.89 ± 1.16 | −1 ± 0.99 |
| TOTAL HIP BMD | 0.92 ± 0.15 | 0.94 ± 0.15 | 0.9 ± 0.14 |
| TOTAL HIP Z SCORE | 0.29 ± 1.02 | 0.31 ± 0.98 | 0.27 ± 1.07 |
| TOTAL HIP T SCORE | −0.44 ± 1.12 | −0.41 ± 1.12 | −0.49 ± 1.13 |
| RADIUS BMD | 0.65 ± 0.09 | 0.66 * ± 0.09 | 0.63 * ± 0.09 |
| RADIUS Z SCORE | −0.39 ± 1.01 | −0.4 ± 1.01 | −0.38 ± 1.02 |
| RADIUS T SCORE | −1.53 ± 1.18 | −1.41 ± 1.14 | −1.68 ± 1.22 |
| CALCANEUS eBMD | 0.52 ± 0.13 | 0.53 ± 0.13 | 0.51 ± 0.12 |
| CALCANEUS eBMD T SCORE | −0.6 ± 1.14 | −0.54 ± 1.17 | −0.68 ± 1.11 |
| Measure | rMZ | rDZ | A | C | E | Model Fit |
|---|---|---|---|---|---|---|
| LUMBAR BMD | 0.834 (0.73 0.9) | 0.304 (0.007 0.553) | 0.828 (0.726, 0.89) | 0 | 0.172 (0.11, 0.274) | 1 |
| LUMBAR Z SCORE | 0.828 (0.724 0.896) | 0.325 (0.036 0.564) | 0.828 (0.728, 0.889) | 0 | 0.172 (0.111, 0.272) | 1 |
| LUMBAR T SCORE | 0.824 (0.695 0.901) | 0.291 (−0.044 0.568) | 0.806 (0.676, 0.882) | 0 | 0.194 (0.118, 0.324) | 0.950 |
| FEMORAL NECK BMD | 0.679 (0.507 0.798) | 0.066 (−0.236 0.357) | 0.669 (0.511, 0.779) | 0 | 0.378 (0.253, 0.554) | 1 |
| FEMORAL NECK Z SCORE | 0.715 (0.557 0.822) | 0.162 (−0.139 0.437) | 0.656 (0.492, 0.77) | 0 | 0.331 (0.221, 0.489) | 1 |
| FEMORAL NECK T SCORE | 0.665 (0.466 0.8) | 0.054 (−0.284 0.38) | 0.613 (0.409, 0.754) | 0 | 0.387 (0.246, 0.591) | 1 |
| TOTAL HIP BMD | 0.659 (0.469 0.787) | 0.29 2 (−0.007 0.543) | 0.653 (0.477, 0.773) | 0 | 0.347 (0.227, 0.523) | 1 |
| TOTAL HIP Z SCORE | 0.696 (0.53 0.81) | 0.318 (0.026 0.56) | 0.705 (0.548, 0.809) | 0 | 0.295 (0.191, 0.452) | 1 |
| TOTAL HIP T SCORE | 0.654 (0.446 0.795) | 0.25 (−0.088 0.537) | 0.664 (0.462, 0.794) | 0 | 0.336 (0.206, 0.538) | 1 |
| RADIUS BMD | 0.795 (0.671 0.874) | 0.375 (0.086 0.606) | 0.806 (0.694, 0.875) | 0 | 0.194 (0.125, 0.306) | 1 |
| RADIUS Z SCORE | 0.73 (0.58 0.831) | 0.452 (0.183 0.658) | 0.737 (0.606, 0.825) | 0 | 0.263 (0.175, 0.394) | 0.557 |
| RADIUS T SCORE | 0.742 (0.575 0.85) | 0.391 (0.073 0.637) | 0.761 (0.611, 0.853) | 0 | 0.239 (0.147, 0.389) | 1 |
| CALCANEUS eBMD ⸸ | 0.834 (0.721 0.902) | 0.564 (0.319 0.739) | 0.838 (0.742, 0.896) | 0 | 0.162 (0.104, 0.258) | 0.259 |
| CALCANEUS eBMD T SCORE ⸸ | 0.853 (0.739 0.917) | 0.596 (0.335 0.771) | 0.838 (0.735, 0.899) | 0 | 0.162 (0.101, 0.265) | 0.182 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piroska, M.; Tarnoki, D.L.; Szabo, H.; Jokkel, Z.; Meszaros, S.; Horvath, C.; Tarnoki, A.D. Strong Genetic Effects on Bone Mineral Density in Multiple Locations with Two Different Techniques: Results from a Cross-Sectional Twin Study. Medicina 2021, 57, 248. https://doi.org/10.3390/medicina57030248
Piroska M, Tarnoki DL, Szabo H, Jokkel Z, Meszaros S, Horvath C, Tarnoki AD. Strong Genetic Effects on Bone Mineral Density in Multiple Locations with Two Different Techniques: Results from a Cross-Sectional Twin Study. Medicina. 2021; 57(3):248. https://doi.org/10.3390/medicina57030248
Chicago/Turabian StylePiroska, Marton, David Laszlo Tarnoki, Helga Szabo, Zsofia Jokkel, Szilvia Meszaros, Csaba Horvath, and Adam Domonkos Tarnoki. 2021. "Strong Genetic Effects on Bone Mineral Density in Multiple Locations with Two Different Techniques: Results from a Cross-Sectional Twin Study" Medicina 57, no. 3: 248. https://doi.org/10.3390/medicina57030248
APA StylePiroska, M., Tarnoki, D. L., Szabo, H., Jokkel, Z., Meszaros, S., Horvath, C., & Tarnoki, A. D. (2021). Strong Genetic Effects on Bone Mineral Density in Multiple Locations with Two Different Techniques: Results from a Cross-Sectional Twin Study. Medicina, 57(3), 248. https://doi.org/10.3390/medicina57030248