
Does the Severity of Obstructive Sleep Apnea Have an Independent Impact on Systemic Inflammation?

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stradling, J.R.; Chadwick, G.A.; Frew, A.J. Changes in ventilation and its components in normal subjects during sleep. Thorax 1985, 40, 364–370. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.; Zhang, D.; Chen, B. Endothelial mechanisms of endothelial dysfunction in patients with obstructive sleep apnea. Sleep Breath. 2011, 16, 283–294. [Google Scholar] [CrossRef]
- Ryan, S.; Taylor, C.; McNicholas, W.T. Selective activation of inflammatory pathways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation 2005, 112, 2660–2667. [Google Scholar] [CrossRef] [Green Version]
- Kokturk, O.; Ciftci, T.U.; Mollarecep, E.; Ciftci, B. Elevated C-reactive protein levels and increased cardiovascular risk in pa-tients with obstructive sleep apnea syndrome. Int. Heart J. 2005, 46, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ursavaş, A.; Karadağ, M.; Rodoplu, E.; Yilmaztepe, A.; Oral, H.B.; Gözü, R.O. Circulating ICAM-1 and VCAM-1 levels in pa-tients with obstructive sleep apnea syndrome. Respiration 2007, 74, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Von Känel, R.; Loredo, J.; Ancoli-Israel, S.; Mills, P.; Natarajan, L.; Dimsdale, J. Association between polysomnographic measures of disrupted sleep and prothrombotic factors. Chest 2007, 131, 733–739. [Google Scholar] [CrossRef]
- Punjabi, N.M.; Beamer, B.A. C-reactive protein is associated with sleep disordered breathing independent of adiposity. Sleep 2007, 30, 29–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Pena Bravo, M.; Serpero, L.D.; Barcelo, A. Inflammatory proteins in patients with obstructive sleep apnea with and without daytime sleepiness. Sleep Breath. 2007, 11, 177–185. [Google Scholar] [CrossRef] [PubMed]
- Minoguchi, K.; Tazaki, T.; Yokoe, T. Elevated production of tumor necrosis factor-α by monocytes in patients with obstructive sleep apnea syndrome. Chest 2004, 126, 1473–1479. [Google Scholar] [CrossRef] [PubMed]
- Roytblat, L.; Rachinsky, M.; Fisher, A.; Greemberg, L.; Shapira, Y.; Douvdevani, A. Raised interleukin-6 levels in obese patients. Obes. Res. 2000, 8, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Borrud, L.G.; Everhart, J.E.; Flegal, K.M.; Harris, T.; Looker, A.C.; Shepherd, J.A. Body compostion data for individuals eight years of age and older: US population, 1999–2004. National center for health statistics. Vital Health Stat. 2010, 11, 1–87. [Google Scholar]
- Nadeem, R.; Molnar, J.; Madbouly, E.; Nida, M.; Aggarwal, S.; Sajid, H.; Naseem, J.; Loomba, R. Serum inflammatory markers in obstructive sleep apnea: A meta-analysis. J. Clin. Sleep Med. 2013, 9, 1003–1012. [Google Scholar] [CrossRef]
- Guven, S.F.; Turkkani, M.H.; Ciftci, B.; Ciftci, T.U.; Erdogan, Y. The relationship between high-sensitivity C-reactive protein levels and the severity of obstructive sleep apnea. Sleep Breath. 2012, 16, 217–221. [Google Scholar] [CrossRef]
- Lee, L.-A.; Chen, N.-H.; Huang, C.-G.; Lin, S.-W.; Fang, T.-J.; Li, H.-Y. Patients with severe obstructive sleep apnea syndrome and elevated high-sensitivity C-reactive protein need priority treatment. Otolaryngol. Neck Surg. 2010, 143, 72–77. [Google Scholar] [CrossRef]
- Barceló, A.; Miralles, C.; Barbe, F.; Vila, M.; Pons, S.; Agustı, A.G.N. Abnormal lipid peroxidation in patients with sleep apnoea. Eur. Respir. J. 2000, 16, 644–647. [Google Scholar] [CrossRef] [Green Version]
- Sharma, S.; Mishra, H.K.; Sharma, H.; Goel, A.; Sreenivas, V.; Gulati, V.; Tahir, M. Obesity, and not obstructive sleep apnea, is responsible for increased serum hs-CRP levels in patients with sleep-disordered breathing in Delhi. Sleep Med. 2008, 9, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C.; Kirisoglu, C.; Ohayon, M.M. C-Reactive Protein and Sleep-Disordered Breathing. Sleep 2004, 27, 1507–1517. [Google Scholar] [CrossRef] [PubMed]
- Ryan, S.; Nolan, G.M.; Hannigan, E.; Cunningham, S.; Taylor, C.; McNicholas, W.T. Cardiovascular risk markers in obstructive sleep apnoea syndrome and correlation with obesity. Thorax 2007, 62, 509–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imagawa, S.; Yamaguchi, Y.; Ogawa, K.; Obara, N.; Suzuki, N.; Yamamoto, M.; Nagasawa, T. Interleukin-6 and Tumor Necrosis Factor-α in Patients with Obstructive Sleep Apnea-Hypopnea Syndrome. Respiration 2004, 71, 24–29. [Google Scholar] [CrossRef]
- Alberti, A.; Sarchielli, P.; Gallinella, E.; Floridi, A.; Floridi, A.; Mazzotta, G.; Gallai, V. Plasma cytokine levels in patients with obstructive sleep apnea syndrome: A preliminary study. J. Sleep Res. 2003, 12, 305–311. [Google Scholar] [CrossRef] [Green Version]
- Fornadi, K.; Lindner, A.; Czira, M.E.; Szentkiralyi, A.; Lazar, A.S.; Zoller, R.; Turanyi, C.Z.; Veber, O.; Novak, M.; Mucsi, I.; et al. Lack of association between objectively assessed sleep disorders and inflammatory markers among kidney transplant recipients. Int. Urol. Nephrol. 2011, 44, 607–617. [Google Scholar] [CrossRef] [PubMed]
- Sahlman, J.; Miettinen, K.; Peuhkurinen, K.; Seppä, J.; Peltonen, M.; Herder, C.; Punnonen, K.; Vanninen, E.; Gylling, H.; Partinen, M.; et al. The activation of the inflammatory cytokines in overweight patients with mild obstructive sleep apnoea. J. Sleep Res. 2009, 19, 341–348. [Google Scholar] [CrossRef]
- Vgontzas, A.N.; Papanicolaou, D.A.; Bixler, E.O.; Kales, A.; Tyson, K.; Chrousos, G.P. Elevation of Plasma Cytokines in Disorders of Excessive Daytime Sleepiness: Role of Sleep Disturbance and Obesity. J. Clin. Endocrinol. Metab. 1997, 82, 1313–1316. [Google Scholar] [CrossRef] [PubMed]
- Mehra, R.; Storfer-Isser, A.; Kirchner, H.L.; Johnson, N.; Jenny, N.; Tracy, R.P.; Redline, S. Soluble Interleukin 6 Receptor. Arch. Intern. Med. 2006, 166, 1725–1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosacka, M.; Piesiak, P.; Jankowska, R. Differences Between Overlap Syndrome and Severe Sleep Apnea Syndrome In BIA/ BIvA, Adiponectin Serum Levels and in Pro-Atherogenic Indices. Paripex Indian J. Res. 2012, 3, 175–179. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Examined Parameters X ±SD (min-max) | AHI < 15 | AHI ≥ 15 | p |
|---|---|---|---|
| Age (years) | 42.57 ± 13.63 | 52.44 ± 11.38 | 0.033 |
| AHI n (min-max) | 10.2 (5.1–14.8) | 24.3 (15.1–82) | <0.001 |
| ODI | 4.63 ± 7.06 (0–23.5) | 21.56 ± 14.45 | <0.001 |
| Mean SatO2 (%) (min/max) | 93.54 ± 2.90 (88–97) | 85.63 ± 12.52 (43–96) | 0.035 |
| Min SatO2 (%) (min/max) | 86.08 ± 4.80 (80–94) | 67.75 ± 13.26 (39–85) | <0.001 |
| SatO2 < 90% (%) (min/max) | 4.90 ± 10.04 (0–32.6) | 41.86 ± 38.43 (1–99) | 0.001 |
| BMI (kg/m2) | 32.29 ± 5.58 (23.5–42.2) | 36.55 ± 6.74 (26.8–52.6) | 0.156 |
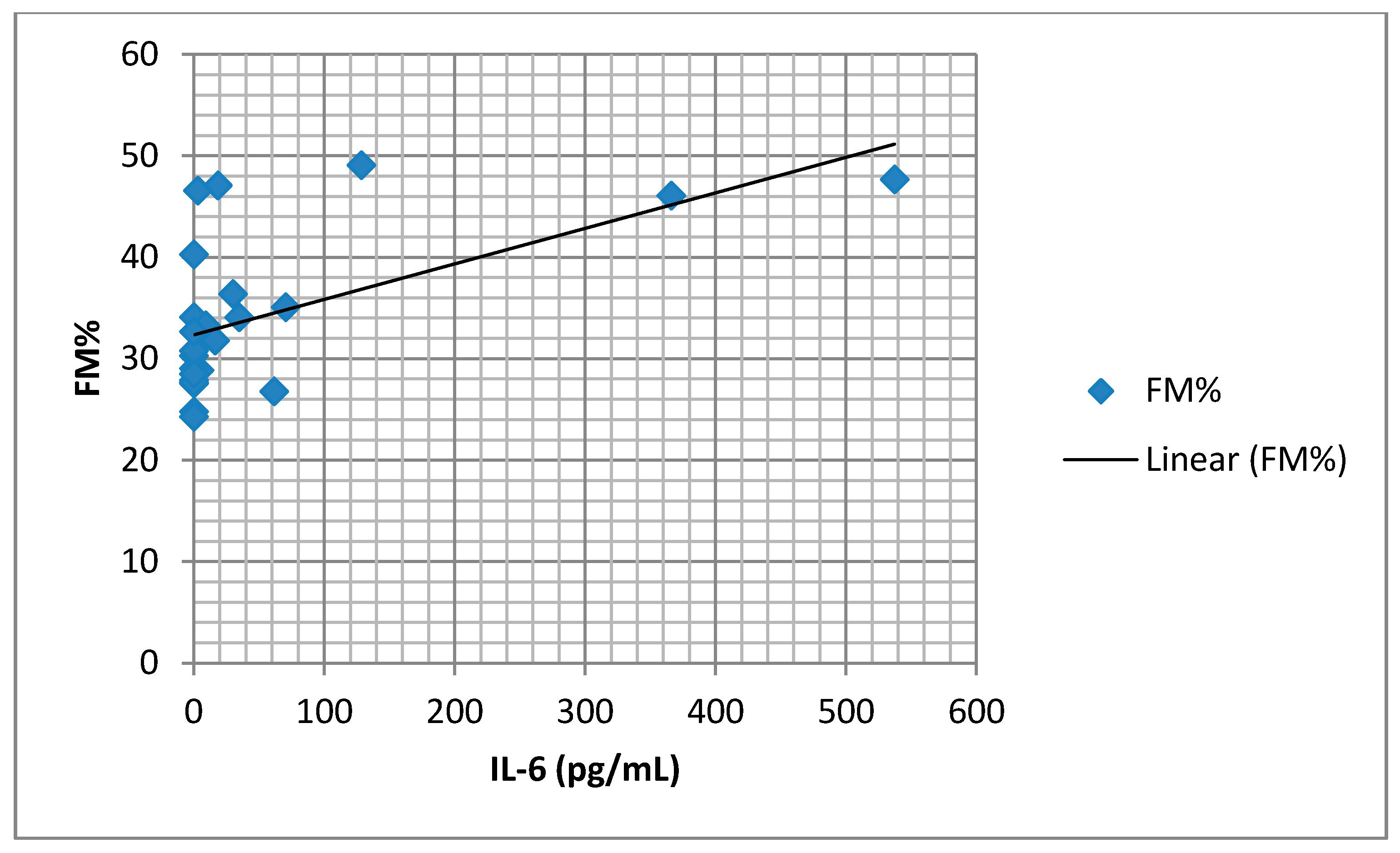
| FM% | 31.97 ± 4.13 (26.8–40.3) | 34.25 ± 9.36 (24.3–49.1) | 0.234 |
| FMI (kg) | 31.68 ± 7.78 | 34.89 ± 9.64 | 0. 483 |
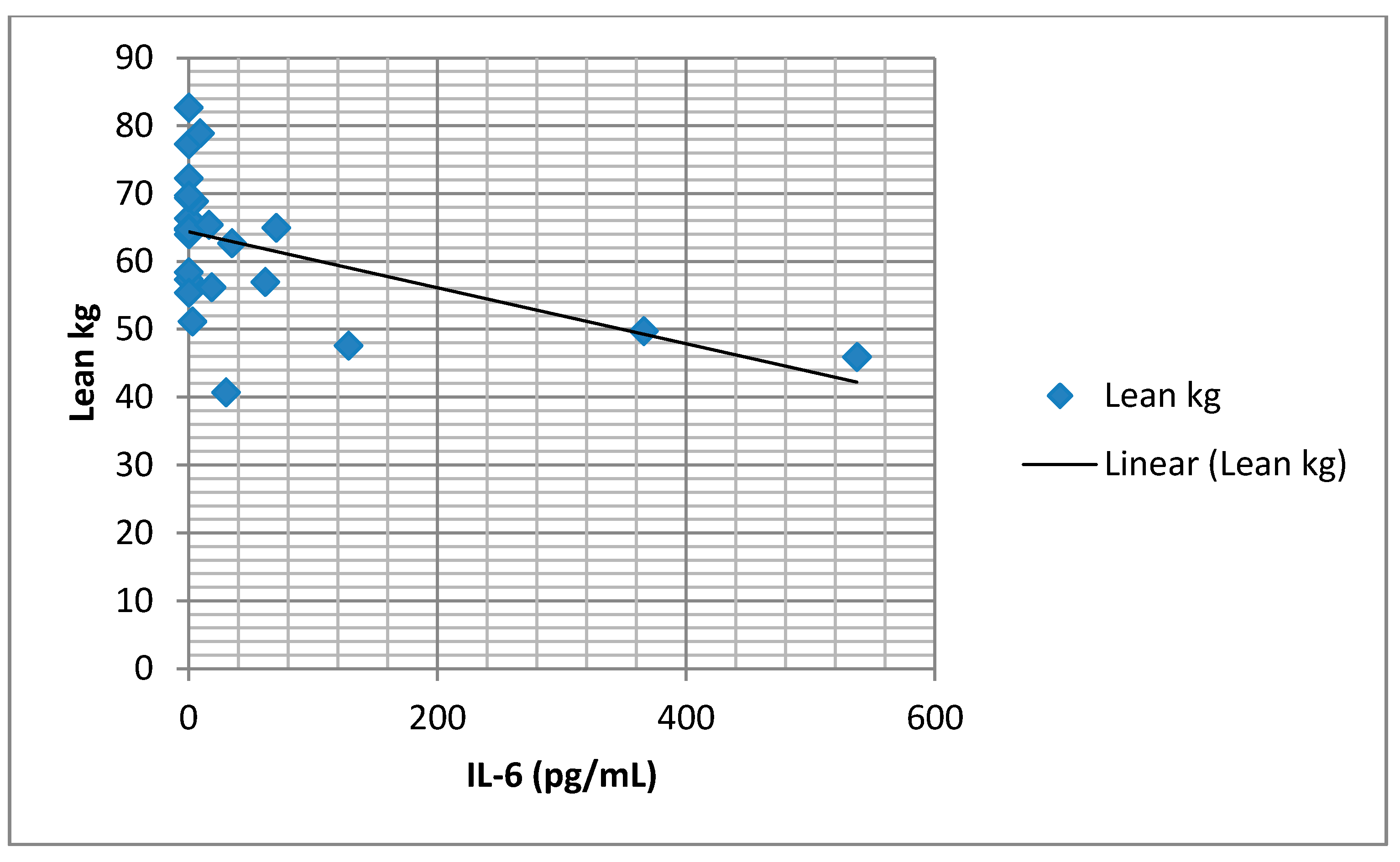
| FFM (kg) | 64.01 ± 12.14 | 59.0 ± 10.16 | 0.929 |
| FFMI | 20.80 ± 3.46 | 20.8 ± 4.12 | 0.172 |
| CentrFM (kg) | 16.84 ± 3.98 (11.28–23.11) | 17.87 ± 3.84 (12.52–26.50) | 0.51 |
| TNF-α(pg/mL) | 4.26 ± 3.92 (4–6–9.9) | 10.32 ± 2.32 | 0.929 |
| IL-6 (pg/mL) | 38.41 ± 12.5 (0–333) | 65.17 ± 21.90 (0–537) | 0.964 |
| CRP (mg/L) | 4.52 ± 3.40(0.5–10.7) | 6.2 ± 4.43 (0.5–18.1) | 0.261 |
| Risk Factors Examined | Univariate | |
|---|---|---|
| # B (95%CI) | p | |
| Age | 0.089 (−0.021–0.199) | 0.109 |
| Gender | 2.646 (−0.536–5.828) | 0.100 |
| AHI | 0.021 (−0.031–0.072) | 0.419 |
| ODI | 0.047 (−0.008–0.101) | 0.09 |
| Mean SatO2 | −0.076 (−0.239–0.086) | 0.342 |
| MinSatO2 | −0.157 (−0.262–−0.053) | 0.005 * |
| SatO2 < 90% | 0.033 (−0.019–0.084) | 0.202 |
| BMI | 0.396 (0.212–0.579) | 0.015 * |
| FM% | 0.194 (0.028–0.36) | 0.051 |
| FMkg | 0.131 (−0.021–0.284) | 0.154 |
| CentrFM | 0.137 (−0.231–0.504) | 0.939 |
| FFM | −0.096 (−0.218–0.27) | 0.078 |
| FFMI | 0.141 (−0.415–0.697) | 0.083 |
| Risk Factors Examined | Multivariate R2 | |
|---|---|---|
| B (95%CI) | p | |
| minSatO2 | −0.017 (−0.215–0.182) | 0.808 |
| BMI | 0.534 (−1.836–2.903) | 0.525 |
| FM% | 1.306 (1.935–4.547) | 0.290 |
| FMI | −3.015 (−11.3–5.27) | 0.331 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suša, R.; Ćupurdija, V.; Novković, L.; Ratinac, M.; Janković, S.; Đoković, D.; Jovanović, J.; Pantić, K.; Simović, S.; Bazić-Sretenović, D.; et al. Does the Severity of Obstructive Sleep Apnea Have an Independent Impact on Systemic Inflammation? Medicina 2021, 57, 292. https://doi.org/10.3390/medicina57030292
Suša R, Ćupurdija V, Novković L, Ratinac M, Janković S, Đoković D, Jovanović J, Pantić K, Simović S, Bazić-Sretenović D, et al. Does the Severity of Obstructive Sleep Apnea Have an Independent Impact on Systemic Inflammation? Medicina. 2021; 57(3):292. https://doi.org/10.3390/medicina57030292
Chicago/Turabian StyleSuša, Romana, Vojislav Ćupurdija, Ljiljana Novković, Miloš Ratinac, Slobodan Janković, Danijela Đoković, Jovan Jovanović, Katarina Pantić, Stefan Simović, Danijela Bazić-Sretenović, and et al. 2021. "Does the Severity of Obstructive Sleep Apnea Have an Independent Impact on Systemic Inflammation?" Medicina 57, no. 3: 292. https://doi.org/10.3390/medicina57030292
APA StyleSuša, R., Ćupurdija, V., Novković, L., Ratinac, M., Janković, S., Đoković, D., Jovanović, J., Pantić, K., Simović, S., Bazić-Sretenović, D., & Čekerevac, I. (2021). Does the Severity of Obstructive Sleep Apnea Have an Independent Impact on Systemic Inflammation? Medicina, 57(3), 292. https://doi.org/10.3390/medicina57030292