
Ultrasound-Guided Moving Shot Radiofrequency Ablation of Benign Soft Tissue Neoplasm


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population and Evaluation
2.2. RFA Technique
2.3. Follow-Up and Outcome Measurement
2.4. Statistical Analysis
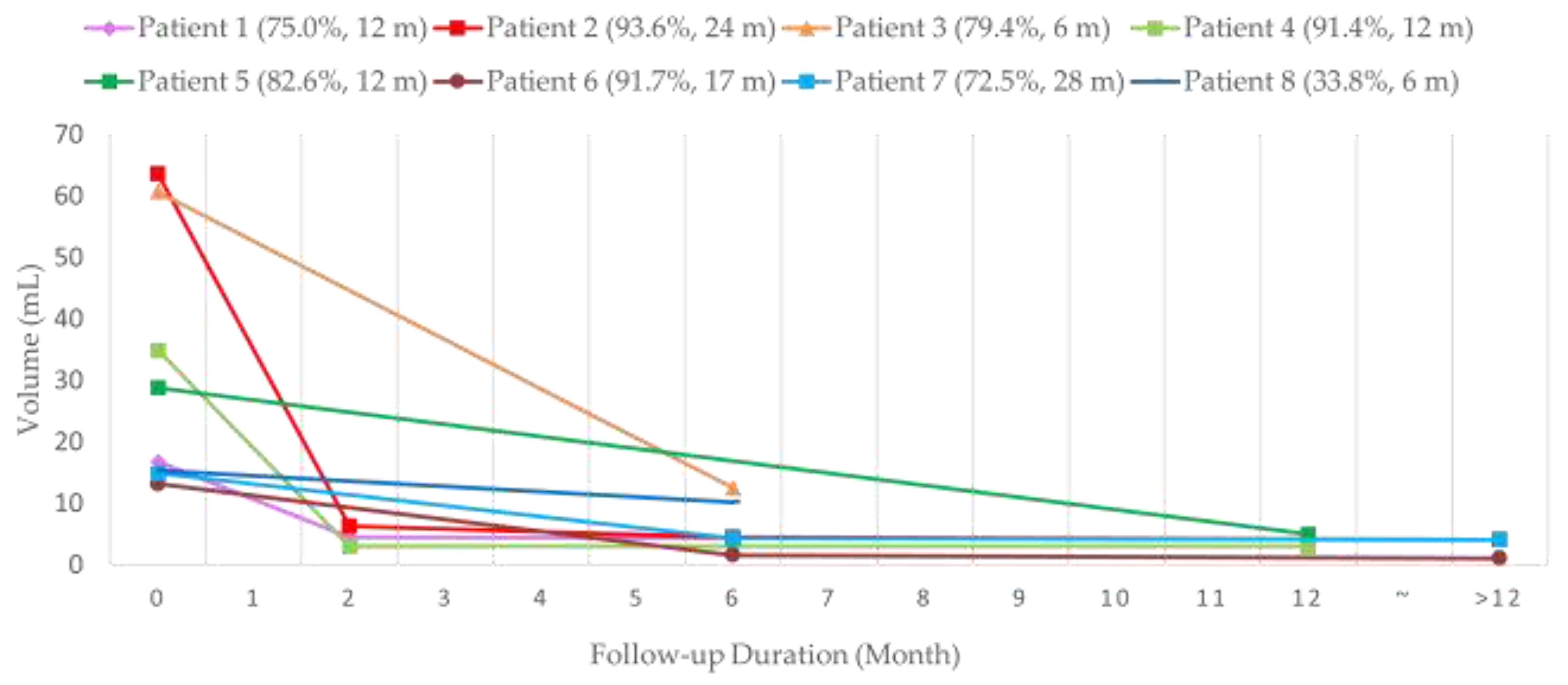
3. Results
4. Discussion
4.1. Summary
4.2. Cosmetic Concerns
4.3. Vascular Malformation
4.4. Neurofibroma
4.5. Local Anesthesia vs. General Anesthesia
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Steiner, F.; FitzJohn, T.; Tan, S.T. Surgical treatment for venous malformation. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 1741–1749. [Google Scholar] [CrossRef]
- Desai, K.I. The Surgical Management of Symptomatic Benign Peripheral Nerve Sheath Tumors of the Neck and Extremities: An Experience of 442 Cases. Neurosurgery 2017, 81, 568–580. [Google Scholar] [CrossRef]
- Guha, D.; Davidson, B.; Nadi, M.; Alotaibi, N.M.; Fehlings, M.G.; Gentili, F.; Valiante, T.A.; Tator, C.H.; Tymianski, M.; Guha, A.; et al. Management of peripheral nerve sheath tumors: 17 years of experience at Toronto Western Hospital. J. Neurosurg. 2018, 128, 1226–1234. [Google Scholar] [CrossRef]
- Thiesen, G.; Gribel, B.F.; Freitas, M.P. Facial asymmetry: A current review. Dent. Press J. Orthod. 2015, 20, 110–125. [Google Scholar] [CrossRef]
- Kobus, K.; Kobus-Zaleśna, K. The treatment of facial asymmetry: Review. Adv. Clin. Exp. Med. Off. Organ. Wroc. Med. Univ. 2017, 26, 1301–1311. [Google Scholar] [CrossRef] [Green Version]
- Fowell, C.; Verea Linares, C.; Jones, R.; Nishikawa, H.; Monaghan, A. Venous malformations of the head and neck: Current concepts in management. Br. J. Oral. Maxillofac. Surg. 2017, 55, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Behravesh, S.; Yakes, W.; Gupta, N.; Naidu, S.; Chong, B.W.; Khademhosseini, A.; Oklu, R. Venous malformations: Clinical diagnosis and treatment. Cardiovasc. Diagn. 2016, 6, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E.; Huson, S.M.; Thomas, N.; Moss, C.; Willshaw, H.; Evans, D.G.; Upadhyaya, M.; Towers, R.; Gleeson, M.; Steiger, C.; et al. Guidelines for the diagnosis and management of individuals with neurofibromatosis 1. J. Med. Genet. 2007, 44, 81–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, J.Y.; Eo, P.S.; Lee, J.S.; Lee, J.W.; Lee, S.J.; Lee, J.M.; Lee, S.Y.; Huh, S.; Kim, J.Y.; Chung, H.Y. Surgical approach for venous malformation in the head and neck. Arch. Craniofac. Surg. 2019, 20, 304–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, H.J.; Lee, J.H.; Kim, G.Y.; Choi, Y.J.; Baek, J.H.; Choi, S.H.; Nam, S.Y.; Kim, S.Y.; Suh, D.C. Ethanol and/or radiofrequency ablation to treat venolymphatic malformations that manifest as a bulging mass in the head and neck. Clin. Radiol. 2016, 71, 1070.e1–1070.e7. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Z.; Peng, C.Z.; Liu, J.B.; Li, Y.W.; He, H.F.; Hu, Q.H.; Lin, B.; Shen, X.G. Efficacy of Ultrasound-guided Radiofrequency Ablation of Parathyroid Hyperplasia: Single Session vs. Two-Session for Effect on Hypocalcemia. Sci. Rep. 2020, 10, 6206. [Google Scholar] [CrossRef] [Green Version]
- Lin, W.-C.; Kan, N.-N.; Chen, H.-L.; Luo, S.-D.; Tung, Y.-C.; Chen, W.-C.; Chou, C.-K.; Chi, S.-Y.; Chen, M.-H.; Su, Y.-Y.; et al. Efficacy and safety of single-session radiofrequency ablation for benign thyroid nodules of different sizes: A retrospective study. Int. J. Hyperth. 2020, 37, 1082–1089. [Google Scholar] [CrossRef] [PubMed]
- Tung, Y.C.; Luo, S.D.; Su, Y.Y.; Chen, W.C.; Chen, H.L.; Cheng, K.L.; Lin, W.C. Evaluation of Outcomes following Radiofrequency Ablation for Treatment of Parotid Tail Warthin Tumors. J. Vasc. Interv. Radiol. 2019, 30, 1574–1580. [Google Scholar] [CrossRef]
- Lim, H.K.; Cho, S.J.; Baek, J.H.; Lee, K.D.; Son, C.W.; Son, J.M.; Baek, S.M. US-Guided Radiofrequency Ablation for Low-Risk Papillary Thyroid Microcarcinoma: Efficacy and Safety in a Large Population. Korean J. Radiol. 2019, 20, 1653–1661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korkusuz, H.; Wolf, T.; Grunwald, F. Feasibility of bipolar radiofrequency ablation in patients with parathyroid adenoma: A first evaluation. Int. J. Hyperth. 2018, 34, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Chung, H.W.; Baek, J.H.; Lee, J.S.; Lee, S.H.; Lee, M.H.; Shin, M.J. Ultrasonography-guided radiofrequency ablation of malignant musculoskeletal soft-tissue tumors using the “moving-shot” technique at a single-institution experience. Ultrasound Q. 2014, 30, 295–300. [Google Scholar] [CrossRef]
- Ha, E.J.; Baek, J.H.; Lee, J.H. Moving-shot versus fixed electrode techniques for radiofrequency ablation: Comparison in an ex-vivo bovine liver tissue model. Korean J. Radiol. 2014, 15, 836–843. [Google Scholar] [CrossRef] [Green Version]
- Jung, S.L.; Baek, J.H.; Lee, J.H.; Shong, Y.K.; Sung, J.Y.; Kim, K.S.; Lee, D.; Kim, J.H.; Baek, S.M.; Sim, J.S.; et al. Efficacy and Safety of Radiofrequency Ablation for Benign Thyroid Nodules: A Prospective Multicenter Study. Korean J. Radiol. 2018, 19, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, J.H.; Kim, Y.S.; Lee, D.; Huh, J.Y.; Lee, J.H. Benign predominantly solid thyroid nodules: Prospective study of efficacy of sonographically guided radiofrequency ablation versus control condition. AJR Am. J. Roentgenol. 2010, 194, 1137–1142. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.H.; Lee, J.H.; Sung, J.Y.; Bae, J.I.; Kim, K.T.; Sim, J.; Baek, S.M.; Kim, Y.S.; Shin, J.H.; Park, J.S.; et al. Complications encountered in the treatment of benign thyroid nodules with US-guided radiofrequency ablation: A multicenter study. Radiology 2012, 262, 335–342. [Google Scholar] [CrossRef]
- Ko, H.K.; Kim, A.H.; Kim, H.B.; Suh, D.C.; Baek, J.H.; Lee, J.H.; Kim, P.N. Experience at 1 year with the moving tip technique of radiofrequency ablation for the treatment of symptomatic venous malformations in the head and neck. J. Vasc. Surg. Venous. Lymphat. Disord. 2013, 1, 263–269. [Google Scholar] [CrossRef]
- Bernardi, S.; Lanzilotti, V.; Papa, G.; Panizzo, N.; Dobrinja, C.; Fabris, B.; Stacul, F. Full-Thickness Skin Burn Caused by Radiofrequency Ablation of a Benign Thyroid Nodule. Thyroid 2016, 26, 183–184. [Google Scholar] [CrossRef] [Green Version]
- Khalilzadeh, O.; Baerlocher, M.O.; Shyn, P.B.; Connolly, B.L.; Devane, A.M.; Morris, C.S.; Cohen, A.M.; Midia, M.; Thornton, R.H.; Gross, K.; et al. Proposal of a New Adverse Event Classification by the Society of Interventional Radiology Standards of Practice Committee. J. Vasc. Interv. Radiol. 2017, 28, 1432–1437.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, Y.; Chen, H.; Lin, X.; Hu, X.; Jin, Y.; Ma, G. Outcomes and complications of sclerotherapy for venous malformations. Vasc. Endovasc. Surg. 2013, 47, 454–461. [Google Scholar] [CrossRef] [PubMed]
- Castren, E.; Aronniemi, J.; Klockars, T.; Pekkola, J.; Lappalainen, K.; Vuola, P.; Salminen, P.; Pitkaranta, A. Complications of sclerotherapy for 75 head and neck venous malformations. Eur. Arch. Otorhinolaryngol. 2016, 273, 1027–1036. [Google Scholar] [CrossRef] [Green Version]
- Greene, A.K.; Alomari, A.I. Management of venous malformations. Clin. Plast. Surg. 2011, 38, 83–93. [Google Scholar] [CrossRef]
- Sachin, K.; Rashmi, S.; Manish, S.; Siddhartha, W.; Uday, L. Haemangiomas and venous malformations of the head and neck: A retrospective analysis of endovascular management in 358 patients. Indian J. Plast. Surg. 2013, 46, 109–116. [Google Scholar] [CrossRef]
- Kim, A.H.; Ko, H.K.; Won, J.Y.; Lee, D.Y. Percutaneous radiofrequency ablation: A novel treatment of facial venous malformation. J. Vasc. Surg. 2009, 50, 424–427. [Google Scholar] [CrossRef] [Green Version]
- Wise, J.B.; Cryer, J.E.; Belasco, J.B.; Jacobs, I.; Elden, L. Management of head and neck plexiform neurofibromas in pediatric patients with neurofibromatosis type 1. Arch. Otolaryngol.-Head Neck Surg. 2005, 131, 712–718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baujat, B.; Krastinova-Lolov, D.; Blumen, M.; Baglin, A.C.; Coquille, F.; Chabolle, F. Radiofrequency in the treatment of craniofacial plexiform neurofibromatosis: A pilot study. Plast. Reconstr. Surg. 2006, 117, 1261–1268. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Li, X.; Wang, J.; Li, W.; Huang, Z. Retroperitoneal schwannoma treated with percutaneous computed tomography-guided radiofrequency ablation. J. Neurosurg. Spine. 2012, 17, 173–176. [Google Scholar] [CrossRef]
- Mrowczynski, O.; Mau, C.; Nguyen, D.T.; Sarwani, N.; Rizk, E.; Harbaugh, K. Percutaneous Radiofrequency Ablation for the Treatment of Peripheral Nerve Sheath Tumors: A Case Report and Review of the Literature. Cureus 2018, 10, e2534. [Google Scholar] [CrossRef] [Green Version]
- Piccioni, F.; Poli, A.; Templeton, L.C.; Templeton, T.W.; Rispoli, M.; Vetrugno, L.; Santonastaso, D.; Valenza, F. Anesthesia for Percutaneous Radiofrequency Tumor Ablation (PRFA): A Review of Current Practice and Techniques. Local Reg. Anesth. 2019, 12, 127–137. [Google Scholar] [CrossRef] [Green Version]
- Jeong, W.K.; Baek, J.H.; Rhim, H.; Kim, Y.S.; Kwak, M.S.; Jeong, H.J.; Lee, D. Radiofrequency ablation of benign thyroid nodules: Safety and imaging follow-up in 236 patients. Eur. Radiol. 2008, 18, 1244–1250. [Google Scholar] [CrossRef]
- Deandrea, M.; Trimboli, P.; Garino, F.; Mormile, A.; Magliona, G.; Ramunni, M.J.; Giovanella, L.; Limone, P.P. Long-Term Efficacy of a Single Session of RFA for Benign Thyroid Nodules: A Longitudinal 5-Year Observational Study. J. Clin. Endocrinol. Metab. 2019, 104, 3751–3756. [Google Scholar] [CrossRef]
- Vuong, N.L.; Dinh, L.Q.; Bang, H.T.; Thuy, T.T.M.; Bac, N.H.; Vy, T.T. Radiofrequency Ablation for Benign Thyroid Nodules: 1-Year Follow-Up in 184 Patients. World J. Surg. 2019, 43, 2447–2453. [Google Scholar] [CrossRef] [PubMed]
- Aysan, E.; Idiz, U.O.; Akbulut, H.; Elmas, L. Single-session radiofrequency ablation on benign thyroid nodules: A prospective single center study: Radiofrequency ablation on thyroid. Langenbecks Arch. Surg. 2016, 401, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Park, B.K.; Chung, I.S. Comparison of General Anesthesia and Conscious Sedation During Computed Tomography-Guided Radiofrequency Ablation of T1a Renal Cell Carcinoma. Can. Assoc. Radiol. J. 2018, 69, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Rhim, H.; Kim, Y.S.; Choi, D.; Lee, W.J.; Lim, H.K.; Shin, B. Percutaneous radiofrequency ablation of hepatocellular carcinomas: Factors related to intraprocedural and postprocedural pain. AJR Am. J. Roentgenol. 2009, 192, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.J.; Sung, J.Y.; Baek, J.H.; Je, M.S.; Choi, D.W.; Yoo, H.; Yang, S.J.; Nam, S.Y.; Yoo, E.Y. Safety and Efficacy of Radiofrequency Ablation for Nonfunctioning Benign Thyroid Nodules in Children and Adolescents in 14 Patients over a 10-Year Period. J. Vasc. Interv. Radiol. 2019, 30, 900–906. [Google Scholar] [CrossRef]
- Gomez, F.M.; Patel, P.A.; Stuart, S.; Roebuck, D.J. Systematic review of ablation techniques for the treatment of malignant or aggressive benign lesions in children. Pediatr. Radiol. 2014, 44, 1281–1289. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Number | Age (Year) | Sex | Diagnosis | Location | Image Modality | Volume (cm3) | Follow-Up (Month) | VRR a | CS b | Anesthesia Method | Discharge after RFA (Day) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | ||||||||||
| 1 | 27 | F | Venous Malformation | Right maxillary | US, CT | 16.8 | 4.2 | 12 | 75.0% | 4 | 1 | LA | - |
| 2 | 22 | M | Venous Malformation | Left masticator space | US, MR | 63.6 | 4.1 | 24 | 93.6% | 4 | 3 | GA | 1 |
| 3 | 30 | M | Venous Malformation | Right mandible | US, MR | 60.7 | 12 | 6 | 79.4% | 3 | 1 | LA | - |
| 4 | 59 | F | Venous Malformation | Left side mouth floor | US, MR | 34.9 | 3.0 | 12 | 91.4% | 4 | 1 | GA | 2 |
| 5 | 1 | F | Congenital Hemangioma | Left abdominal wall | US, MR | 28.8 | 5.0 | 12 | 82.6% | 4 | 3 | GA | 1 |
| 6 | 16 | F | Neurofibroma | Left temporal fossa | US, MR | 13.2 | 1.1 | 17 | 91.7% | 3 | 1 | GA | 4 |
| 7 | 5 | F | Neurofibroma | Right temporal fossa | US, MR | 14.9 | 4.1 | 28 | 72.5% | 3 | 1 | GA | 1 |
| 8 c | 7 | F | Congenital Hemangioma | Left buttock | US, MR | 15.4 | 10.2 | 6 | 33.8% | 4 | 4 | GA | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, W.-C.; Tai, Y.-F.; Chen, M.-H.; Luo, S.-D.; Huang, F.; Chen, W.-C.; Chiang, P.-L.; Chen, H.-L.; Chen, M.-H.; Baek, J.-H. Ultrasound-Guided Moving Shot Radiofrequency Ablation of Benign Soft Tissue Neoplasm. Medicina 2021, 57, 830. https://doi.org/10.3390/medicina57080830
Lin W-C, Tai Y-F, Chen M-H, Luo S-D, Huang F, Chen W-C, Chiang P-L, Chen H-L, Chen M-H, Baek J-H. Ultrasound-Guided Moving Shot Radiofrequency Ablation of Benign Soft Tissue Neoplasm. Medicina. 2021; 57(8):830. https://doi.org/10.3390/medicina57080830
Chicago/Turabian StyleLin, Wei-Che, Yi-Fan Tai, Meng-Hsiang Chen, Sheng-Dean Luo, Faye Huang, Wei-Chih Chen, Pi-Ling Chiang, Hsiu-Ling Chen, Mei-Hsiu Chen, and Jung-Hwan Baek. 2021. "Ultrasound-Guided Moving Shot Radiofrequency Ablation of Benign Soft Tissue Neoplasm" Medicina 57, no. 8: 830. https://doi.org/10.3390/medicina57080830
APA StyleLin, W. -C., Tai, Y. -F., Chen, M. -H., Luo, S. -D., Huang, F., Chen, W. -C., Chiang, P. -L., Chen, H. -L., Chen, M. -H., & Baek, J. -H. (2021). Ultrasound-Guided Moving Shot Radiofrequency Ablation of Benign Soft Tissue Neoplasm. Medicina, 57(8), 830. https://doi.org/10.3390/medicina57080830