
Ablation Zone Involution of Liver Tumors Is Faster in Patients Treated with Irreversible Electroporation Than Microwave Ablation


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Population
2.3. Ablation Techniques
2.4. Imaging and Analysis
2.5. Liver Function Values
2.6. Statistical Analysis
3. Results
3.1. Population and Ablation Characteristics
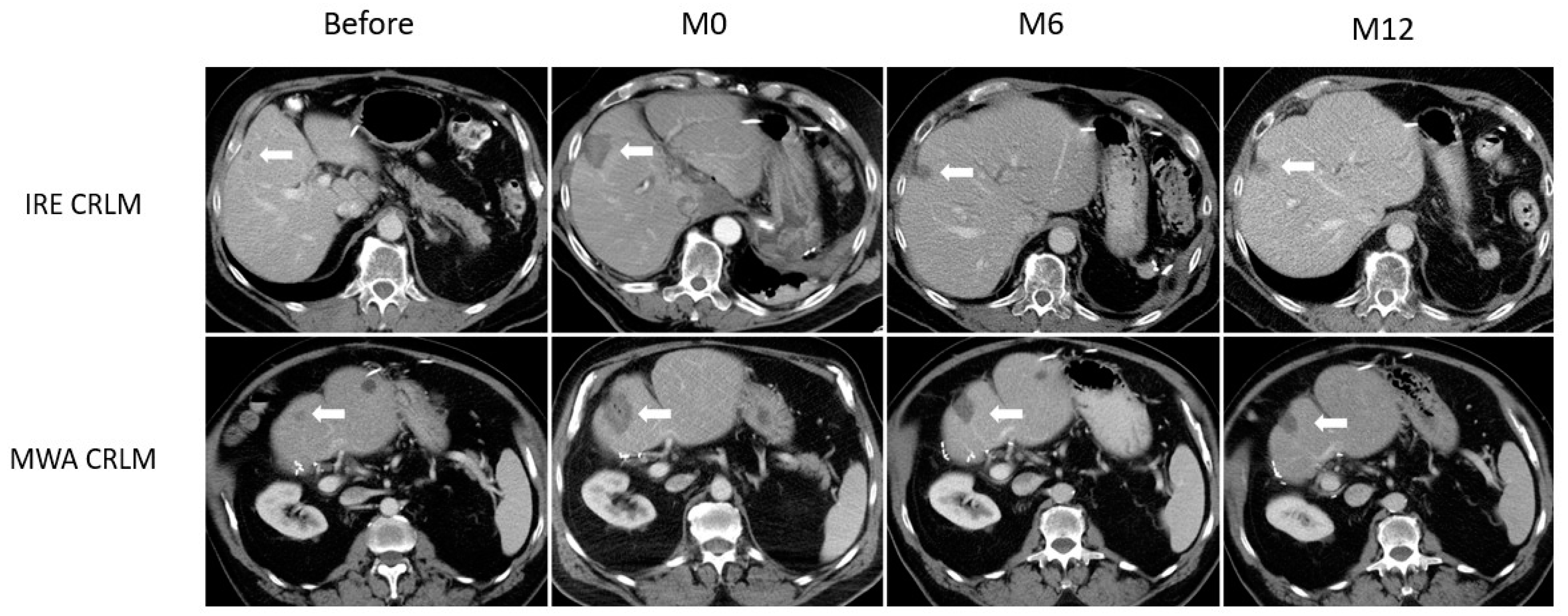
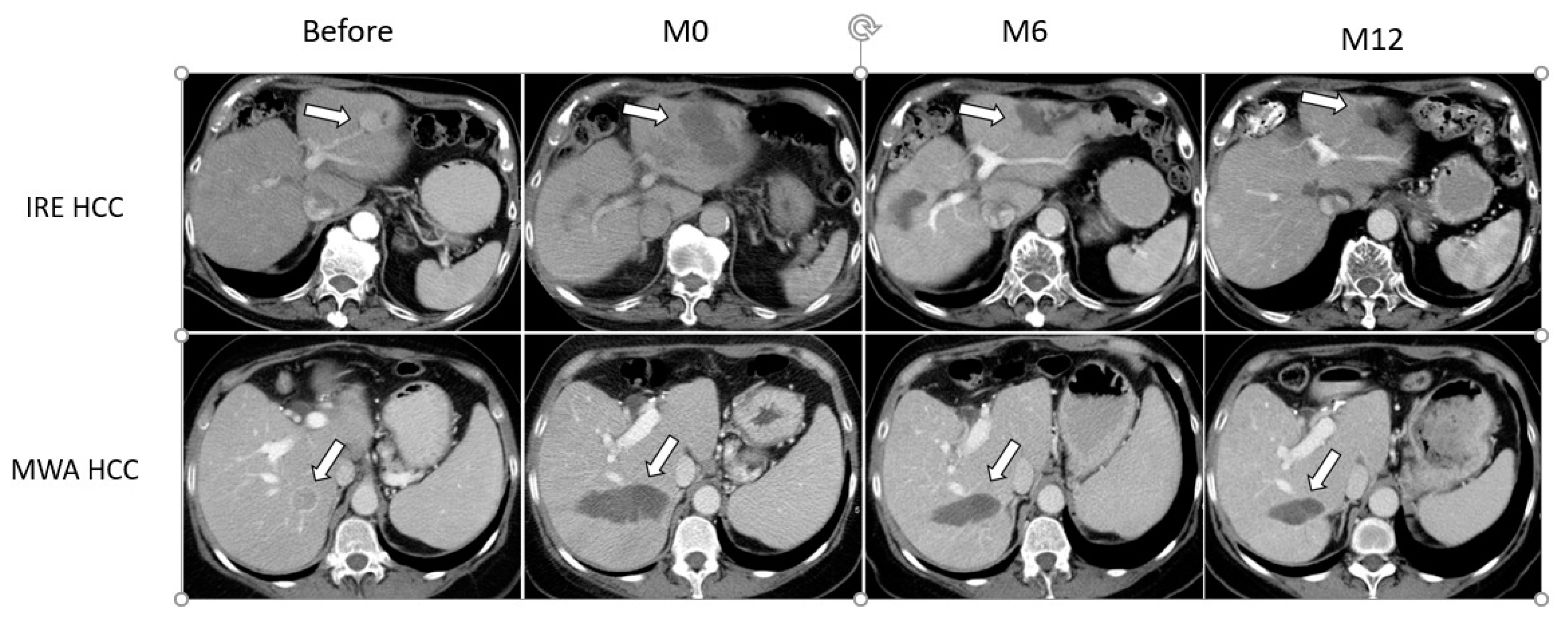
3.2. Ablation Zone Involution
3.3. Ablation Zone by Disease Type
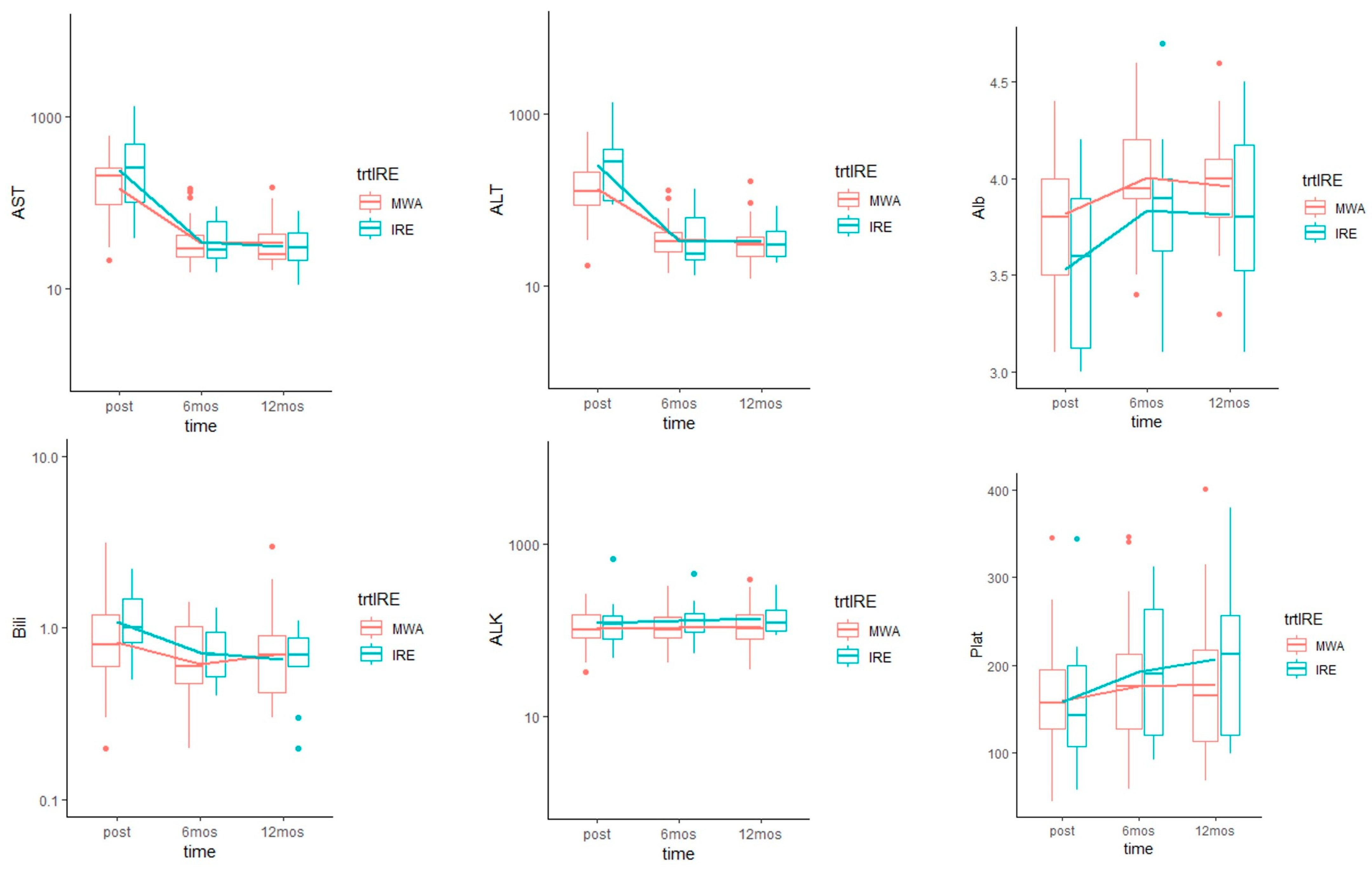
3.4. Liver Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Kim, Y.; Lim, H.K.; Rhim, H.; Lee, M.W.; Choi, D.; Lee, W.J.; Paik, S.W.; Koh, K.C.; Lee, J.H.; Choi, M.S.; et al. Ten-year outcomes of percutaneous radiofrequency ablation as first-line therapy of early hepatocellular carcinoma: Analysis of prognostic factors. J. Hepatol. 2013, 58, 89–97. [Google Scholar] [CrossRef]
- Waki, K.; Aikata, H.; Katamura, Y.; Kawaoka, T.; Takaki, S.; Hiramatsu, A.; Takahashi, S.; Toyota, N.; Ito, K.; Chayama, K. Percutaneous radiofrequency ablation as first-line treatment for small hepatocellular carcinoma: Results and prognostic factors on long-term follow up. J. Gastroenterol. Hepatol. 2010, 25, 597–604. [Google Scholar] [CrossRef]
- Ahmed, M.; Solbiati, L.; Brace, C.L.; Breen, D.J.; Callstrom, M.R.; Charboneau, J.W.; Chen, M.H.; Choi, B.I.; de Baère, T.; Dodd, G.D., 3rd; et al. Image-guided tumor ablation: Standardization of terminology and reporting criteria—A 10-year update. Radiology 2014, 273, 241–260. [Google Scholar] [CrossRef]
- Gillams, A.; Goldberg, N.; Ahmed, M.; Bale, R.; Breen, D.; Callstrom, M.; Chen, M.H.; Choi, B.I.; de Baere, T.; Dupuy, D.; et al. Thermal ablation of colorectal liver metastases: A position paper by an international panel of ablation experts, The Interventional Oncology Sans Frontières meeting 2013. Eur. Radiol. 2015, 25, 3438–3454. [Google Scholar] [CrossRef] [PubMed]
- Groeschl, R.T.; Pilgrim, C.H.C.; Hanna, E.M.; Simo, K.A.; Swan, R.Z.; Sindram, D.; Martinie, J.B.; Iannitti, D.A.; Bloomston, M.; Schmidt, C.; et al. Microwave ablation for hepatic malignancies: A multiinstitutional analysis. Ann. Surg. 2014, 259, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.; Badger, S.A.; Ellis, G. The role of microwave ablation in the management of hepatic colorectal metastases. Surgeon 2011, 9, 33–37. [Google Scholar] [CrossRef]
- Kim, K.H.; Yoon, Y.S.; Yu, C.S.; Kim, T.W.; Kim, H.J.; Kim, P.N.; Ha, H.K.; Kim, J.C. Comparative analysis of radiofrequency ablation and surgical resection for colorectal liver metastases. J. Korean Surg. Soc. 2011, 81, 25–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hur, H.; Ko, Y.T.; Min, B.S.; Kim, K.S.; Choi, J.S.; Sohn, S.K.; Cho, C.H.; Ko, H.K.; Lee, J.T.; Kim, N.K. Comparative study of resection and radiofrequency ablation in the treatment of solitary colorectal liver metastases. Am. J. Surg. 2009, 197, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Oshowo, A.; Gillams, A.; Harrison, E.; Lees, W.R.; Taylor, I. Comparison of resection and radiofrequency ablation for treatment of solitary colorectal liver metastases. Br. J. Surg. 2003, 90, 1240–1243. [Google Scholar] [CrossRef] [PubMed]
- Lin, S.-M.; Lin, C.-J.; Lin, C.-C.; Hsu, C.-W.; Chen, Y.-C. Randomised controlled trial comparing percutaneous radiofrequency thermal ablation, percutaneous ethanol injection, and percutaneous acetic acid injection to treat hepatocellular carcinoma of 3 cm or less. Gut 2005, 54, 1151–1156. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology 2005, 42, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Frassoni, S.; Rampoldi, A.; Tuscano, B.; Bagnardi, V.; Vanzulli, A.; De Carlis, L. Surgical Resection vs. Percutaneous Ablation for Single Hepatocellular Carcinoma: Exploring the Impact of Li-RADS Classification on Oncological Outcomes. Cancers 2021, 13, 1671. [Google Scholar] [CrossRef] [PubMed]
- Lu, D.S.; Raman, S.S.; Limanond, P.; Aziz, D.; Economou, J.; Busuttil, R.; Sayre, J. Influence of large peritumoral vessels on outcome of radiofrequency ablation of liver tumors. J. Vasc. Interv. Radiol. 2003, 14, 1267–1274. [Google Scholar] [CrossRef]
- Rhim, H.; Yoon, K.-H.; Lee, J.M.; Cho, Y.; Cho, J.-S.; Kim, S.H.; Lee, W.J.; Lim, H.K.; Nam, G.J.; Han, S.S.; et al. Major complications after radio-frequency thermal ablation of hepatic tumors: Spectrum of imaging findings. Radiographics 2003, 23, 123–134; discussion 134–136. [Google Scholar] [CrossRef]
- van Tilborg, A.A.J.M.; Scheffer, H.J.; de Jong, M.C.; Vroomen, L.G.P.H.; Nielsen, K.; van Kuijk, C.; van den Tol, P.M.; Meijerink, M.R. MWA Versus RFA for Perivascular and Peribiliary CRLM: A Retrospective Patient- and Lesion-Based Analysis of Two Historical Cohorts. Cardiovasc. Interv. Radiol. 2016, 39, 1438–1446. [Google Scholar] [CrossRef] [Green Version]
- Lee, E.W.; Chen, C.; Prieto, V.E.; Dry, S.M.; Loh, C.T.; Kee, S.T. Advanced hepatic ablation technique for creating complete cell death: Irreversible electroporation. Radiology 2010, 255, 426–433. [Google Scholar] [CrossRef]
- Sutter, O.; Calvo, J.; N’Kontchou, G.; Nault, J.-C.; Ourabia, R.; Nahon, P.; Ganne-Carrié, N.; Bourcier, V.; Zentar, N.; Bouhafs, F.; et al. Safety and Efficacy of Irreversible Electroporation for the Treatment of Hepatocellular Carcinoma Not Amenable to Thermal Ablation Techniques: A Retrospective Single-Center Case Series. Radiology 2017, 284, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Zupanic, A.; Kos, B.; Miklavcic, D. Treatment planning of electroporation-based medical interventions: Electrochemotherapy, gene electrotransfer and irreversible electroporation. Phys. Med. Biol. 2012, 57, 5425–5440. [Google Scholar] [CrossRef] [Green Version]
- Kingham, T.P.; Karkar, A.M.; D’Angelica, M.I.; Allen, P.J.; Dematteo, R.P.; Getrajdman, G.I.; Sofocleous, C.T.; Solomon, S.B.; Jarnagin, W.R.; Fong, Y. Ablation of perivascular hepatic malignant tumors with irreversible electroporation. J. Am. Coll Surg. 2012, 215, 379–387. [Google Scholar] [CrossRef]
- Langan, R.C.; Goldman, D.A.; D’Angelica, M.I.; DeMatteo, R.P.; Allen, P.J.; Balachandran, V.P.; Jarnagin, W.R.; Kingham, T.P. Recurrence patterns following irreversible electroporation for hepatic malignancies. J. Surg. Oncol. 2017, 115, 704–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davalos, R.V.; Mir, I.L.M.; Rubinsky, B. Tissue ablation with irreversible electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef]
- Miller, L.; Leor, J.; Rubinsky, B. Cancer Cells Ablation with Irreversible Electroporation: Technology in Cancer Research & Treatment; SAGE Publications: Los Angeles, CA, USA, 2016; Available online: https://journals.sagepub.com/doi/10.1177/153303460500400615 (accessed on 12 November 2020).
- Srimathveeravalli, G.; Silk, M.; Wimmer, T.; Monette, S.; Kimm, S.; Maybody, M.; Solomon, S.B.; Coleman, J.; Durack, J.C. Feasibility of catheter-directed intraluminal irreversible electroporation of porcine ureter and acute outcomes in response to increasing energy delivery. J. Vasc. Interv. Radiol. 2015, 26, 1059–1066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bulvik, B.E.; Rozenblum, N.; Gourevich, S.; Ahmed, M.; Andriyanov, A.V.; Galun, E.; Goldberg, S.N. Irreversible Electroporation versus Radiofrequency Ablation: A Comparison of Local and Systemic Effects in a Small-Animal Model. Radiology 2016, 280, 413–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Golberg, A.; Bruinsma, B.G.; Jaramillo, M.; Yarmush, M.L.; Uygun, B.E. Rat liver regeneration following ablation with irreversible electroporation. PeerJ 2016, 4, e1571. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Zeng, Q.; Zhong, R.; Mao, S.; Shen, L.; Wu, P. Liver regeneration after radiofrequency ablation versus irreversible electroporation. Zhonghua Yi Xue Za Zhi 2015, 95, 66–68. [Google Scholar] [PubMed]
- Sugimoto, K.; Kakimi, K.; Takeuchi, H.; Fujieda, N.; Saito, K.; Sato, E.; Sakamaki, K.; Moriyasu, F.; Itoi, T. Irreversible Electroporation versus Radiofrequency Ablation: Comparison of Systemic Immune Responses in Patients with Hepatocellular Carcinoma. J. Vasc. Interv. Radiol. 2019, 30, 845–853.e6. [Google Scholar] [CrossRef]
- Cheng, R.G.; Bhattacharya, R.; Yeh, M.M.; Padia, S.A. Irreversible Electroporation Can Effectively Ablate Hepatocellular Carcinoma to Complete Pathologic Necrosis. J. Vasc. Interv. Radiol. 2015, 26, 1184–1188. [Google Scholar] [CrossRef]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Sainani, N.I.; Gervais, D.A.; Mueller, P.R.; Arellano, R.S. Imaging after percutaneous radiofrequency ablation of hepatic tumors: Part 1, Normal findings. AJR Am. J. Roentgenol. 2013, 200, 184–193. [Google Scholar] [CrossRef]
- Kei, S.K.; Rhim, H.; Choi, D.; Lee, W.J.; Lim, H.K.; Kim, Y. Local tumor progression after radiofrequency ablation of liver tumors: Analysis of morphologic pattern and site of recurrence. AJR Am. J. Roentgenol. 2008, 190, 1544–1551. [Google Scholar] [CrossRef]
- Vroomen, L.G.P.H.; Petre, E.N.; Cornelis, F.H.; Solomon, S.B.; Srimathveeravalli, G. Irreversible electroporation and thermal ablation of tumors in the liver, lung, kidney and bone: What are the differences? Diagn. Interv. Imaging 2017, 98, 609–617. [Google Scholar] [CrossRef]
- Petre, E.N.; Sofocleous, C. Thermal Ablation in the Management of Colorectal Cancer Patients with Oligometastatic Liver Disease. Visc. Med. 2017, 33, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Scheck, J.; Bruners, P.; Schindler, D.; Kuhl, C.; Isfort, P. Comparison of Chronologic Change in the Size and Contrast-Enhancement of Ablation Zones on CT Images after Irreversible Electroporation and Radiofrequency Ablation. Korean J. Radiol. 2018, 19, 560–567. [Google Scholar] [CrossRef]
- Rubinsky, B.; Onik, G.; Mikus, P. Irreversible electroporation: A new ablation modality—Clinical implications. Technol. Cancer Res. Treat. 2007, 6, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Lu, D.S.K.; Osuagwu, F.; Lassman, C. Irreversible electroporation in porcine liver: Acute computed tomography appearance of ablation zone with histopathologic correlation. J. Comput. Assist. Tomogr. 2013, 37, 154–158. [Google Scholar] [CrossRef]
- Ma, H.; Wang, J.; Thomas, D.P.; Tong, C.; Leng, L.; Wang, W.; Merk, M.; Zierow, S.; Bernhagen, J.; Ren, J.; et al. Impaired macrophage migration inhibitory factor-AMP-activated protein kinase activation and ischemic recovery in the senescent heart. Circulation 2010, 122, 282–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heinrichs, D.; Knauel, M.; Offermanns, C.; Berres, M.-L.; Nellen, A.; Leng, L.; Schmitz, P.; Bucala, R.; Trautwein, C.; Weber, C.; et al. Macrophage migration inhibitory factor (MIF) exerts antifibrotic effects in experimental liver fibrosis via CD74. Proc. Natl. Acad. Sci. USA 2011, 108, 17444–17449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujimori, M.; Kimura, Y.; Ueshima, E.; Dupuy, D.E.; Adusumilli, P.S.; Solomon, S.B.; Srimathveeravalli, G. Lung Ablation with Irreversible Electroporation Promotes Immune Cell Infiltration by Sparing Extracellular Matrix Proteins and Vasculature: Implications for Immunotherapy. Bioelectricity 2021. Available online: https://www.liebertpub.com/doi/abs/10.1089/bioe.2021.0014 (accessed on 10 July 2021).
- Froud, T.; Venkat, S.R.; Barbery, K.J.; Gunjan, A.; Narayanan, G. Liver Function Tests Following Irreversible Electroporation of Liver Tumors: Experience in 174 Procedures. Tech. Vasc. Interv. Radiol. 2015, 18, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Nakazawa, T.; Kokubu, S.; Shibuya, A.; Ono, K.; Watanabe, M.; Hidaka, H.; Tsuchihashi, T.; Saigenji, K. Radiofrequency ablation of hepatocellular carcinoma: Correlation between local tumor progression after ablation and ablative margin. AJR Am. J. Roentgenol. 2007, 188, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.T.; Silverman, S.G.; Tuncali, K.; Obuchowski, N.A.; vanSonnenberg, E.; Shankar, S. Biochemical and hematologic alterations following percutaneous cryoablation of liver tumors: Experience in 48 procedures. Radiology 2008, 248, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Silk, M.T.; Wimmer, T.; Lee, K.S.; Srimathveeravalli, G.; Brown, K.T.; Kingham, P.T.; Fong, Y.; Durack, J.C.; Sofocleous, C.T.; Solomon, S.B. Percutaneous ablation of peribiliary tumors with irreversible electroporation. J. Vasc. Interv. Radiol. 2014, 25, 112–118. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | IRE | MWA | p |
|---|---|---|---|
| No = 14 | No = 30 | ||
| Age at ablation, years | 61 ± 13 (44–82) | 67 ± 10 (43–81) | 0.13 |
| Sex | >0.9 | ||
| Female | 5 (5/14, 36%) | 12 (12/30, 40%) | |
| Male | 9 (9/14, 64%) | 18 (18/30, 60%) | |
| BMI, kg/m2 | 26 ± 5 (17–33) | 29 ± 7 (17–42) | 0.21 |
| Prior systemic chemotherapy | 11 (11/14, 79%) | 16 (16/30, 53%) | 0.18 |
| Subcapsular location | 10 (10/14, 71%) | 16 (16/30, 53%) | 0.33 |
| Proximity to > 3 mm vessel | 12 (12/14, 86%) | 18 (18/30, 60%) | 0.16 |
| Liver segment | 0.041 | ||
| Segment 1 | 4 (4/14, 29%) | 0 (0/30, 0%) | |
| Segment 2 | 1 (1/14, 7.1%) | 4 (4/30, 13%) | |
| Segment 3 | 0 (0/14, 0%) | 1 (1/30, 3.3%) | |
| Segment 4 | 4 (4/14, 29%) | 5 (5/30, 17%) | |
| Segment 5 | 2 (2/14, 14%) | 4 (4/30, 13%) | |
| Segment 6 | 0 (0/14, 0%) | 7 (7/30, 23%) | |
| Segment 7 | 1 (1/14, 7.1%) | 2 (2/30, 6.7%) | |
| Segment 8 | 2 (2/14, 14%) | 7 (7/30, 23%) | |
| Tumor size, mm | 17 ± 7 (6–29) | 21 ± 10 (9–50) | 0.29 |
| Disease type | 0.10 | ||
| CRLM | 9 (6/14, 64%) | 10 (10/30, 33%) | |
| HCC | 5 (5/14, 36%) | 20 (20/30, 67%) | |
| Pre-treatment Bilirubin, mg/dL | 0.74 ± 0.22 (0.40–1.20) | 0.64 ± 0.33 (0.20–1.50) | 0.10 |
| Pre-treatment AST, U/L | 35 ± 17 (18–73) | 38 ± 25 (15–125) | 0.76 |
| Pre-treatment ALT, U/L | 38 ± 22 (16–92) | 39 ± 25 (14–111) | 0.71 |
| Pre-treatment ALK, U/L | 118 ± 94 (55–430) | 105 ± 47 (36–211) | >0.9 |
| Pre-treatment Albumin, g/dL | 4.02 ± 0.35 (3.30–4.50) | 4.11 ± 0.34 (3.40–5.00) | 0.52 |
| Pre-treatment Platelet, K/mcL | 201 ± 62 (104–297) | 181 ± 68 (81–368) | 0.27 |
| Ablation Type | Time (Months) | Mean (mm²) | Ratio of IRE vs. MWA | 95% CI | p Interaction |
|---|---|---|---|---|---|
| IRE | 0 | 923.61 | 0.813 | 0.523–1.265 | <0.01 |
| MWA | 0 | 1136.03 | |||
| IRE | 6 | 241.04 | 0.313 | 0.165–0.592 | |
| MWA | 6 | 771.08 | |||
| IRE | 12 | 60.47 | 0.103 | 0.029–0.365 | |
| MWA | 12 | 589.43 |
| Disease | Ablation Type | Time (months) | Mean (mm²) | Ratio of IRE vs. MWA | 95% CI | p Interaction |
|---|---|---|---|---|---|---|
| HCC | IRE | 0 | 1499.33 | 1.326 | 0.549–3.206 | 0.17 |
| MWA | 0 | 1130.49 | ||||
| IRE | 6 | 562.29 | 0.714 | 0.316–1.612 | ||
| MWA | 6 | 787.63 | ||||
| IRE | 12 | 327.91 | 0.525 | 0.178–1.547 | ||
| MWA | 12 | 624.47 | ||||
| CRLM | IRE | 0 | 705.65 | 0.615 | 0.42–0.9 | <0.01 |
| MWA | 0 | 1147.19 | ||||
| IRE | 6 | 150.57 | 0.204 | 0.1–0.415 | ||
| MWA | 6 | 739.00 | ||||
| IRE | 12 | 23.64 | 0.045 | 0.009–0.219 | ||
| MWA | 12 | 525.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ridouani, F.; Ghosn, M.; Cornelis, F.; Petre, E.N.; Hsu, M.; Moskowitz, C.S.; Kingham, P.T.; Solomon, S.B.; Srimathveeravalli, G. Ablation Zone Involution of Liver Tumors Is Faster in Patients Treated with Irreversible Electroporation Than Microwave Ablation. Medicina 2021, 57, 877. https://doi.org/10.3390/medicina57090877
Ridouani F, Ghosn M, Cornelis F, Petre EN, Hsu M, Moskowitz CS, Kingham PT, Solomon SB, Srimathveeravalli G. Ablation Zone Involution of Liver Tumors Is Faster in Patients Treated with Irreversible Electroporation Than Microwave Ablation. Medicina. 2021; 57(9):877. https://doi.org/10.3390/medicina57090877
Chicago/Turabian StyleRidouani, Fourat, Mario Ghosn, Francois Cornelis, Elena N Petre, Meier Hsu, Chaya S Moskowitz, Peter T Kingham, Stephen B Solomon, and Govindarajan Srimathveeravalli. 2021. "Ablation Zone Involution of Liver Tumors Is Faster in Patients Treated with Irreversible Electroporation Than Microwave Ablation" Medicina 57, no. 9: 877. https://doi.org/10.3390/medicina57090877
APA StyleRidouani, F., Ghosn, M., Cornelis, F., Petre, E. N., Hsu, M., Moskowitz, C. S., Kingham, P. T., Solomon, S. B., & Srimathveeravalli, G. (2021). Ablation Zone Involution of Liver Tumors Is Faster in Patients Treated with Irreversible Electroporation Than Microwave Ablation. Medicina, 57(9), 877. https://doi.org/10.3390/medicina57090877