
The Relationship of 25(OH)D3 with Diabetes Mellitus and the Mediation Effect of Lipid Profile in Chinese Rural Population of Henan Province



Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Selection of Participants
2.3. Data Collection
2.4. Blood Samples
2.5. Laboratory Measurements
2.6. Definition
2.7. Statistical Analysis
3. Results
3.1. Demography Characteristics of Participants
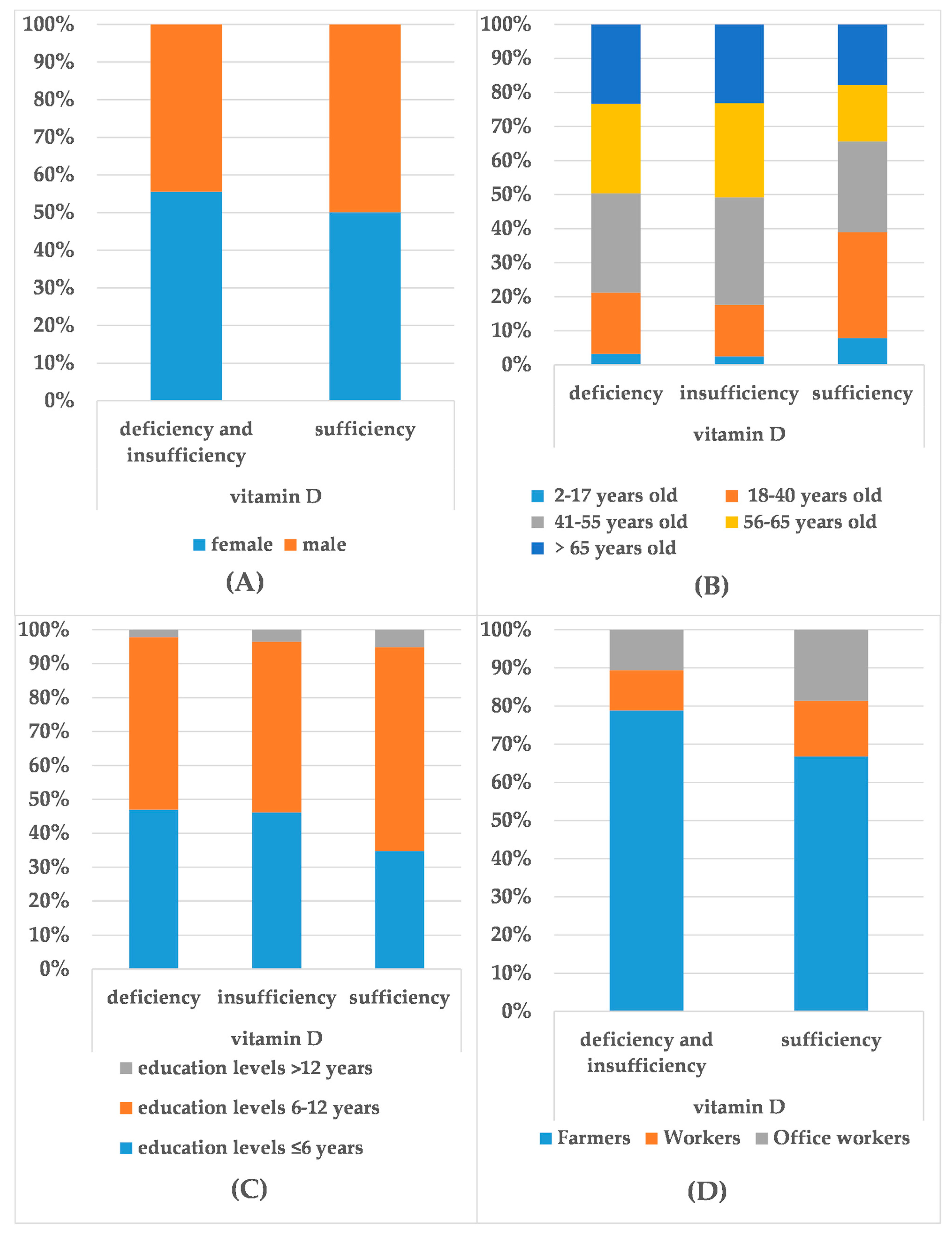
3.2. Distribution of 25(OH)D3 and the Demographic Characteristics
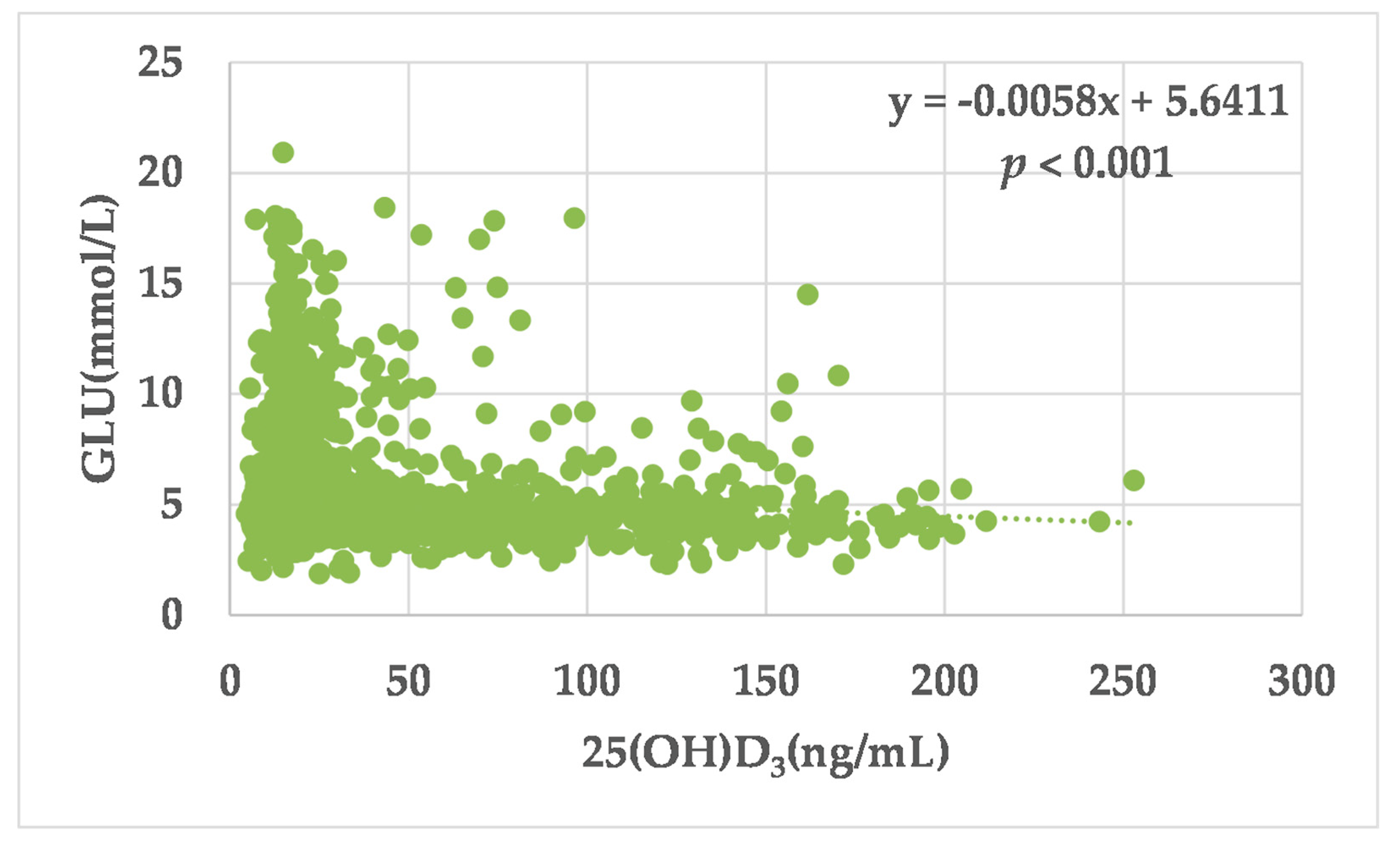
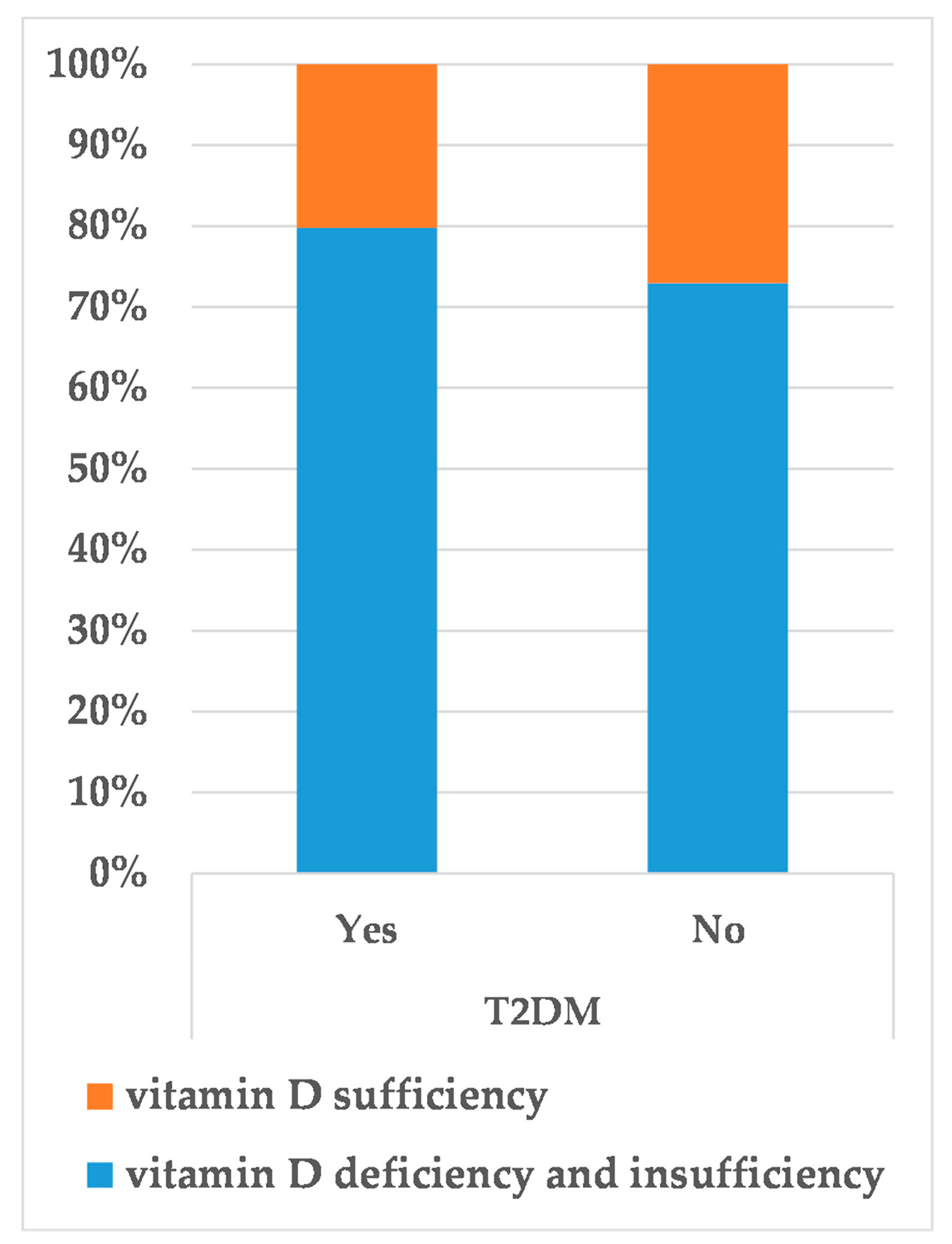
3.3. 25(OH)D3 Levels, Serum Glucose (GLU) and T2DM
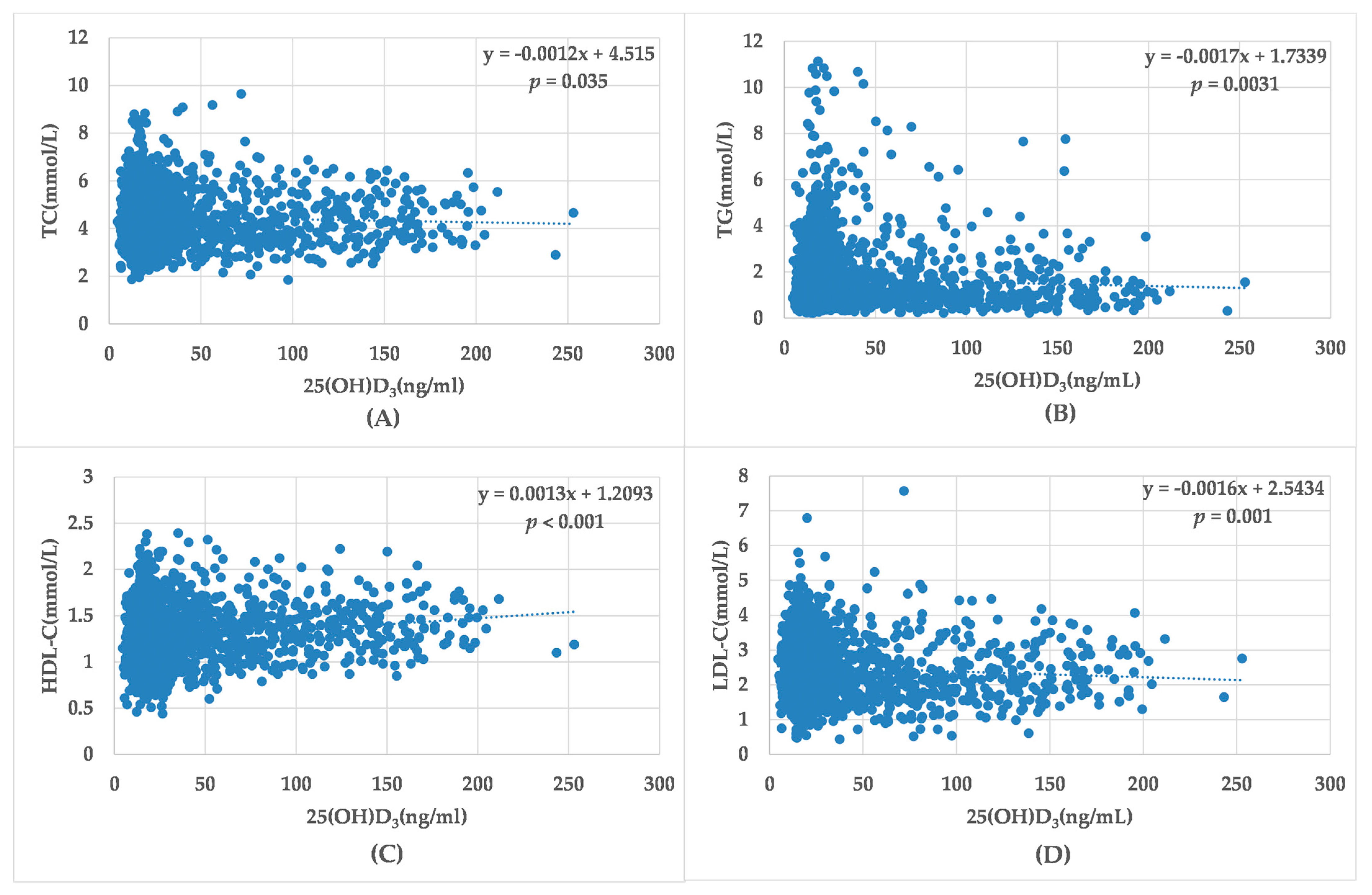
3.4. 25(OH)D3 Levels and the Incidence of Dyslipidemias, as Well as Lipid Profile
3.5. The Prevalence of T2DM in the Stratified Serum Lipid Profile
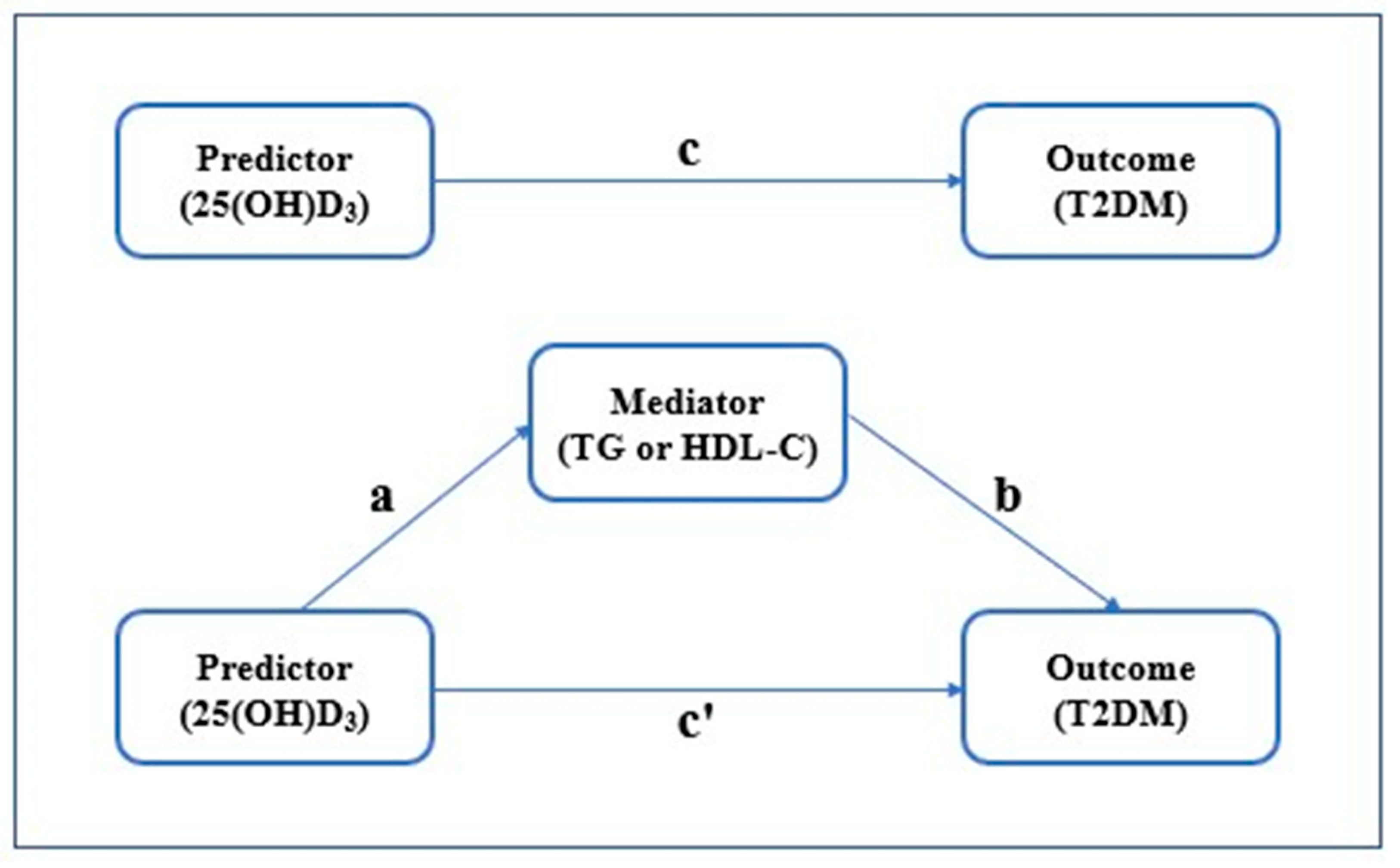
3.6. 25(OH)D3 Level, Serum Lipid Levels (TG or HDL-C) and T2DM
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, M.S.; Alslamah, T.; Alannaz, S.M.; Shaik, R.A.; Ahmad, R.K.; Yusuf, M.; Khan, M.; Ghimire, A. Prevalence of micro and macro vascular complications and their risk factors in type 2 diabetes in Saudi Arabian population: An analysis from SHIS. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 4308–4316. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.; Lundman, P. The emerging role of lipoproteins in atherogenesis: Beyond LDL cholesterol. Semin. Vasc. Med. 2004, 4, 187–195. [Google Scholar] [CrossRef]
- Kopin, L.; Lowenstein, C. Dyslipidemia. Ann. Intern. Med. 2017, 167, 81–96. [Google Scholar] [CrossRef]
- Sadeghi, E.; Hosseini, S.M.; Vossoughi, M.; Aminorroaya, A.; Amini, M. Association of Lipid Profile with Type 2 Diabetes in First-Degree Relatives: A 14-Year Follow-Up Study in Iran. Diabetes Metab. Syndr. Obes. 2020, 13, 2743–2750. [Google Scholar] [CrossRef]
- Palazhy, S.; Viswanathan, V. Lipid Abnormalities in Type 2 Diabetes Mellitus Patients with Overt Nephropathy. Diabetes Metab. J. 2017, 41, 128–134. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Hirose, H.; Zhou, Y.T.; Esser, V.; McGarry, J.D.; Unger, R.H. Increased lipogenic capacity of the islets of obese rats: A role in the pathogenesis of NIDDM. Diabetes 1997, 46, 408–413. [Google Scholar] [CrossRef]
- Milburn, J.L., Jr.; Hirose, H.; Lee, Y.H.; Nagasawa, Y.; Ogawa, A.; Ohneda, M.; BeltrandelRio, H.; Newgard, C.B.; Johnson, J.H.; Unger, R.H. Pancreatic beta-cells in obesity. Evidence for induction of functional, morphologic, and metabolic abnormalities by increased long chain fatty acids. J. Biol. Chem. 1995, 270, 1295–1299. [Google Scholar] [CrossRef] [Green Version]
- Lin, D.; Qi, Y.; Huang, C.; Wu, M.; Wang, C.; Li, F.; Yang, C.; Yan, L.; Ren, M.; Sun, K. Associations of lipid parameters with insulin resistance and diabetes: A population-based study. Clin. Nutr. 2018, 37, 1423–1429. [Google Scholar] [CrossRef]
- Sintov, A.C.; Yarmolinsky, L.; Dahan, A.; Ben-Shabat, S. Pharmacological effects of vitamin D and its analogs: Recent developments. Drug Discov. Today 2014, 19, 1769–1774. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D: Evolutionary, physiological and health perspectives. Curr. Drug Targets 2011, 12, 4–18. [Google Scholar] [CrossRef]
- Delvin, E.; Souberbielle, J.C.; Viard, J.P.; Salle, B. Role of vitamin D in acquired immune and autoimmune diseases. Crit. Rev. Clin. Lab. Sci. 2014, 51, 232–247. [Google Scholar] [CrossRef]
- Fayed, A.; El Nokeety, M.M.; Heikal, A.A.; Abdulazim, D.O.; Naguib, M.M.; Sharaf El Din, U.A.A.; Vascular Calcification, G. Fibroblast growth factor-23 is a strong predictor of insulin resistance among chronic kidney disease patients. Ren. Fail. 2018, 40, 226–230. [Google Scholar] [CrossRef]
- Jensen, M.E.; Ducharme, F.M.; Theoret, Y.; Belanger, A.S.; Delvin, E. Data in support for the measurement of serum 25-hydroxyvitamin D (25OHD) by tandem mass spectrometry. Data Brief 2016, 8, 925–929. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine, S. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj Fuleihan, G.; Josse, R.G.; Lips, P.; Morales-Torres, J.; et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [Green Version]
- Griz, L.H.; Bandeira, F.; Gabbay, M.A.; Dib, S.A.; Carvalho, E.F. Vitamin D and diabetes mellitus: An update 2013. Arq. Bras. De Endocrinol. E Metabol. 2014, 58, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ge, H.; Sun, H.; Wang, T.; Liu, X.; Li, X.; Yu, F.; Han, H.; Wang, J.; Li, W. The association between serum 25-hydroxyvitamin D3 concentration and serum lipids in the rural population of China. Lipids Health Dis. 2017, 16, 215. [Google Scholar] [CrossRef] [Green Version]
- Jorde, R.; Figenschau, Y.; Hutchinson, M.; Emaus, N.; Grimnes, G. High serum 25-hydroxyvitamin D concentrations are associated with a favorable serum lipid profile. Eur. J. Clin. Nutr. 2010, 64, 1457–1464. [Google Scholar] [CrossRef] [PubMed]
- Strobel, F.; Reusch, J.; Penna-Martinez, M.; Ramos-Lopez, E.; Klahold, E.; Klepzig, C.; Wehrle, J.; Kahles, H.; Badenhoop, K. Effect of a randomised controlled vitamin D trial on insulin resistance and glucose metabolism in patients with type 2 diabetes mellitus. Horm. Metab. Res. 2014, 46, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez-Molero, I.; Rojo-Martinez, G.; Morcillo, S.; Gutierrez-Repiso, C.; Rubio-Martin, E.; Almaraz, M.C.; Olveira, G.; Soriguer, F. Vitamin D and incidence of diabetes: A prospective cohort study. Clin. Nutr. 2012, 31, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, F.; Blasey, C.; Feldman, D.; Caulfield, M.P.; Hantash, F.M.; Reaven, G.M. Low circulating 25-hydroxyvitamin D concentrations are associated with defects in insulin action and insulin secretion in persons with prediabetes. J. Nutr. 2015, 145, 714–719. [Google Scholar] [CrossRef]
- Wimalawansa, S.J. Associations of vitamin D with insulin resistance, obesity, type 2 diabetes, and metabolic syndrome. J. Steroid Biochem. Mol. Biol. 2018, 175, 177–189. [Google Scholar] [CrossRef]
- Mitri, J.; Dawson-Hughes, B.; Hu, F.B.; Pittas, A.G. Effects of vitamin D and calcium supplementation on pancreatic beta cell function, insulin sensitivity, and glycemia in adults at high risk of diabetes: The Calcium and Vitamin D for Diabetes Mellitus (CaDDM) randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 486–494. [Google Scholar] [CrossRef] [Green Version]
- Alam, M.S.; Kamrul-Hasan, M.; Kalam, S.T.; Selim, S.; Akter, F.; Saifuddin, M. Vitamin D Status in Newly Diagnosed Type 2 Diabetes Patients Attending in a Tertiary Hospital of Bangladesh. Mymensingh Med. J. 2018, 27, 362–368. [Google Scholar]
- Wang, J.M.; Ye, S.D.; Li, S.M.; Hu, W. Correlations of 25 (OH)D level with blood lipid, inflammatory factors and vascular endothelial function in diabetic patients. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 731–735. [Google Scholar] [CrossRef]
- Rodrigues, K.F.; Pietrani, N.T.; Bosco, A.A.; de Sousa, M.C.R.; Silva, I.F.O.; Silveira, J.N.; Gomes, K.B. Lower Vitamin D Levels, but Not VDR Polymorphisms, Influence Type 2 Diabetes Mellitus in Brazilian Population Independently of Obesity. Medicina 2019, 55, 188. [Google Scholar] [CrossRef] [Green Version]
- Nam, H.; Kim, H.Y.; Choi, J.S.; Kweon, S.S.; Lee, Y.H.; Nam, H.S.; Park, K.S.; Ryu, S.Y.; Choi, S.W.; Oh, S.H.; et al. Association between Serum 25-hydroxyvitamin D Levels and Type 2 Diabetes in Korean Adults. Chonnam Med. J. 2017, 53, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Sergi, G.; De Rui, M.; Bolzetta, F.; Toffanello, E.D.; Zambon, S.; Corti, M.C.; Sartori, L.; Musacchio, E.; Baggio, G.; et al. Serum 25-hydroxyvitamin D and incidence of diabetes in elderly people: The PRO.V.A. study. J. Clin. Endocrinol. Metab. 2014, 99, 2351–2358. [Google Scholar] [CrossRef]
- Pittas, A.G.; Dawson-Hughes, B.; Sheehan, P.; Ware, J.H.; Knowler, W.C.; Aroda, V.R.; Brodsky, I.; Ceglia, L.; Chadha, C.; Chatterjee, R.; et al. Vitamin D Supplementation and Prevention of Type 2 Diabetes. N. Engl. J. Med. 2019, 381, 520–530. [Google Scholar] [CrossRef] [Green Version]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for health: A global perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef] [Green Version]
- Craig, M.E.; Jefferies, C.; Dabelea, D.; Balde, N.; Seth, A.; Donaghue, K.C. The International Society for Pediatric and Ado-lescent Diabetes. ISPAD Clinical Practice Consensus Guidelines 2014. Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatric Diabetes 2014, 15 (Suppl. 20), 4–17. [Google Scholar] [CrossRef]
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents. Expert panel on integrated guidelines for cardiovascular health and risk reduction in children and adolescents: Summary report. Pediatrics 2011, 128 (Suppl. 5), S213–S256. [Google Scholar] [CrossRef] [Green Version]
- Stewart, J.; McCallin, T.; Martinez, J.; Chacko, S.; Yusuf, S. Hyperlipidemia. Pediatr. Rev. 2020, 41, 393–402. [Google Scholar] [CrossRef]
- National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation; Treatment of High Blood Choles-terol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation 2002, 106, 3143–3421. [Google Scholar] [CrossRef]
- Wang, L.; Liu, X.; Hou, J.; Wei, D.; Liu, P.; Fan, K.; Zhang, L.; Nie, L.; Li, X.; Huo, W.; et al. Serum Vitamin D Affected Type 2 Diabetes though Altering Lipid Profile and Modified the Effects of Testosterone on Diabetes Status. Nutrients 2020, 13, 90. [Google Scholar] [CrossRef]
- Gagnon, C.; Lu, Z.X.; Magliano, D.J.; Dunstan, D.W.; Shaw, J.E.; Zimmet, P.Z.; Sikaris, K.; Grantham, N.; Ebeling, P.R.; Daly, R.M. Serum 25-hydroxyvitamin D, calcium intake, and risk of type 2 diabetes after 5 years: Results from a national, population-based prospective study (the Australian Diabetes, Obesity and Lifestyle study). Diabetes Care 2011, 34, 1133–1138. [Google Scholar] [CrossRef] [Green Version]
- Barbarawi, M.; Zayed, Y.; Barbarawi, O.; Bala, A.; Alabdouh, A.; Gakhal, I.; Rizk, F.; Alkasasbeh, M.; Bachuwa, G.; Manson, J.E. Effect of Vitamin D Supplementation on the Incidence of Diabetes Mellitus. J. Clin. Endocrinol. Metab. 2020, 105, 2857–2868. [Google Scholar] [CrossRef]
- Liu, E.; Meigs, J.B.; Pittas, A.G.; Economos, C.D.; McKeown, N.M.; Booth, S.L.; Jacques, P.F. Predicted 25-hydroxyvitamin D score and incident type 2 diabetes in the Framingham Offspring Study. Am. J. Clin. Nutr. 2010, 91, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Santos-Gallego, C.G.; Rosenson, R.S. Role of HDL in those with diabetes. Curr. Cardiol. Rep. 2014, 16, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Mooradian, A.D. Dyslipidemia in type 2 diabetes mellitus. Nat. Clin. Practice. Endocrinol. Metab. 2009, 5, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Bhowmik, B.; Siddiquee, T.; Mujumder, A.; Afsana, F.; Ahmed, T.; Mdala, I.A.; do, V.M.N.C.; Khan, A.K.A.; Hussain, A.; Holmboe-Ottesen, G.; et al. Serum Lipid Profile and Its Association with Diabetes and Prediabetes in a Rural Bangladeshi Population. Int. J. Environ. Res. Public Health 2018, 15, 1944. [Google Scholar] [CrossRef] [Green Version]
- Young, K.A.; Rasouli, N. Serum lipid profile as a tool to predict incident diabetes: Is it a wishful thinking? J. Diabetes Complicat. 2020, 34, 107755. [Google Scholar] [CrossRef]
- Cui, R.; Qi, Z.; Zhou, L.; Li, Z.; Li, Q.; Zhang, J. Evaluation of serum lipid profile, body mass index, and waistline in Chinese patients with type 2 diabetes mellitus. Clin. Interv. Aging 2016, 11, 445–452. [Google Scholar] [CrossRef] [Green Version]
- Xiao, P.; Zhao, X.Y.; Hong, W.; Hou, D.Q.; Yu, Z.C.; Wang, L.G.; Wang, H.J.; Gao, A.Y.; Cheng, H.; Mi, J. A prospective cohort study on the associations between vitamin D nutritional status and cardiometabolic abnormities in children. Zhonghua Liuxingbingxue Zazhi 2020, 41, 2059–2065. [Google Scholar] [CrossRef]
- Wang, Y.; Si, S.; Liu, J.; Wang, Z.; Jia, H.; Feng, K.; Sun, L.; Song, S.J. The Associations of Serum Lipids with Vitamin D Status. PLoS ONE 2016, 11, e0165157. [Google Scholar] [CrossRef]
- Szymczak-Pajor, I.; Drzewoski, J.; Sliwinska, A. The Molecular Mechanisms by Which Vitamin D Prevents Insulin Resistance and Associated Disorders. Int. J. Mol. Sci. 2020, 21, 6644. [Google Scholar] [CrossRef]
- Jungert, A.; Roth, H.J.; Neuhauser-Berthold, M. Associations of serum 25-hydroxycholecalciferol and parathyroid hormone with serum lipids differ by sex and vitamin D status. Public Health Nutr. 2015, 18, 1684–1691. [Google Scholar] [CrossRef] [Green Version]
- Jorde, R.; Sneve, M.; Torjesen, P.; Figenschau, Y. No improvement in cardiovascular risk factors in overweight and obese subjects after supplementation with vitamin D3 for 1 year. J. Intern. Med. 2010, 267, 462–472. [Google Scholar] [CrossRef]
- Maki, K.C.; Rubin, M.R.; Wong, L.G.; McManus, J.F.; Jensen, C.D.; Lawless, A. Effects of vitamin D supplementation on 25-hydroxyvitamin D, high-density lipoprotein cholesterol, and other cardiovascular disease risk markers in subjects with elevated waist circumference. Int. J. Food Sci. Nutr. 2011, 62, 318–327. [Google Scholar] [CrossRef]
- Kazlauskaite, R.; Powell, L.H.; Mandapakala, C.; Cursio, J.F.; Avery, E.F.; Calvin, J. Vitamin D is associated with atheroprotective high-density lipoprotein profile in postmenopausal women. J. Clin. Lipidol. 2010, 4, 113–119. [Google Scholar] [CrossRef] [Green Version]
- Randle, P.J.; Garland, P.B.; Hales, C.N.; Newsholme, E.A. The glucose fatty-acid cycle. Its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet 1963, 1, 785–789. [Google Scholar] [CrossRef]
- Randle, P.J.; Garland, P.B.; Newsholme, E.A.; Hales, C.N. The glucose fatty acid cycle in obesity and maturity onset diabetes mellitus. Ann. N. Y. Acad. Sci. 1965, 131, 324–333. [Google Scholar] [CrossRef]
- Yahya, R.; Jainandunsing, S.; Rashid, M.; van der Zee, L.; Touw, A.; de Rooij, F.W.M.; Sijbrands, E.J.G.; Verhoeven, A.J.M.; Mulder, M.T. HDL associates with insulin resistance and beta-cell dysfunction in South Asian families at risk of type 2 diabetes. J. Diabetes Complicat. 2021, 35, 107993. [Google Scholar] [CrossRef]
- Obesity: Preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ. Tech. Rep. Ser. 2000, 894, 1–253.
- Walsh, J.S.; Bowles, S.; Evans, A.L. Vitamin D in obesity. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 389–394. [Google Scholar] [CrossRef]
- Walsh, J.S.; Evans, A.L.; Bowles, S.; Naylor, K.E.; Jones, K.S.; Schoenmakers, I.; Jacques, R.M.; Eastell, R. Free 25-hydroxyvitamin D is low in obesity, but there are no adverse associations with bone health. Am. J. Clin. Nutr. 2016, 103, 1465–1471. [Google Scholar] [CrossRef] [Green Version]
- Samuel, L.; Borrell, L.N. The effect of body mass index on optimal vitamin D status in U.S. adults: The National Health and Nutrition Examination Survey 2001-2006. Ann. Epidemiol. 2013, 23, 409–414. [Google Scholar] [CrossRef]
- Vimaleswaran, K.S.; Berry, D.J.; Lu, C.; Tikkanen, E.; Pilz, S.; Hiraki, L.T.; Cooper, J.D.; Dastani, Z.; Li, R.; Houston, D.K.; et al. Causal relationship between obesity and vitamin D status: Bi-directional Mendelian randomization analysis of multiple cohorts. PLoS Med. 2013, 10, e1001383. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Event (T2DM) (n = 395) | No Event (n = 1931) | p |
|---|---|---|---|
| Gender | 0.004 * | ||
| male | 155 (39.24%) | 911 (47.18%) | |
| female | 240 (60.76%) | 1020 (52.82%) | |
| Age | <0.001 * | ||
| <18 | 1 (0.25%) | 97 (5.02%) | |
| ≥18 | 394 (99.75%) | 1834 (94.98%) | |
| Education (years) | <0.001 * | ||
| ≤6 | 218 (55.10%) | 797 (41.30%) | |
| 6~12 | 173 (43.88%) | 1061 (54.94%) | |
| >12 | 4 (1.02%) | 73 (3.76%) | |
| Occupation | <0.001 * | ||
| Farmer | 338 (85.53%) | 1424 (73.73%) | |
| Worker | 33 (8.38%) | 236 (12.22%) | |
| Office worker | 24 (6.09%) | 271 (14.05%) | |
| GLU (mmol/L) | 9.08 ± 3.32 | 4.71 ± 0.81 | <0.001 * |
| TC (mmol/L) | 4.74 ± 1.05 | 4.42 ± 1.01 | <0.001 * |
| TG (mmol/L) | 2.29 ± 1.76 | 1.55 ± 1.21 | <0.001 * |
| HDL-C (mmol/L) | 1.21 ± 0.27 | 1.26 ± 0.31 | 0.003 * |
| LDL-C (mmol/L) | 2.56 ± 0.80 | 2.48 ± 0.78 | 0.066 |
| 25(OH)D3 (ng/mL) | 29.07 ± 28.76 | 34.75 ± 37.04 | 0.001 * |
| Parameter | Unadjusted | Adjusted | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |
| TC | ||||||
| Low TC | 1.00 (ref.) | 1.00 (ref.) | ||||
| High TC | 1.58 | 1.02–2.46 | 0.040 * | 1.34 | 0.84–2.13 | 0.220 |
| TG | ||||||
| Low TG | 1.00 (ref.) | 1.00 (ref.) | ||||
| High TG | 2.40 | 1.89–3.05 | <0.001 * | 2.48 | 1.94–3.18 | <0.001 * |
| HDL-C | ||||||
| High HDL-C | 1.00 (ref.) | 1.00 (ref.) | ||||
| Low HDL-C | 1.44 | 1.14–1.82 | 0.003 * | 1.37 | 1.07–1.75 | 0.011 * |
| LDL-C | ||||||
| Low LDL-C | 1.00 (ref.) | 1.00 (ref.) | ||||
| High LDL-C | 0.65 | 0.29–1.45 | 0.295 | 0.51 | 0.23–1.15 | 0.106 |
| Effects | Parameter Estimate (95%CI) | OR (95%CI) | Relative Effect Value | p |
|---|---|---|---|---|
| Path a | −0.15 (−0.28, −0.02) | 0.86 (0.76, 0.98) | — | 0.025 * |
| Path b | 0.32 (0.25, 0.39) | 1.38 (1.28, 1.48) | — | <0.001 * |
| Indirect effect-path a, b | −0.04 (−0.09, −0.01) | 0.96 (0.91, 0.99) | 10.26% | — |
| Direct effect-path c’ | −0.35 (−0.62, −0.08) | 0.70 (0.54, 0.92) | 89.74% | 0.012 * |
| Total effect-path c | −0.39 (−0.68, −0.14) | 0.68 (0.51, 0.87) | 100% | 0.004 * |
| Effects | Parameter Estimate (95%CI) | OR (95%CI) | Relative Effect Value | p |
|---|---|---|---|---|
| Path a | 0.14 (0.11, 0.16) | 1.15 (1.12,1.17) | — | <0.001 * |
| Path b | −0.47 (−0.84, −0.10) | 0.63 (0.43,0.90) | — | 0.013 * |
| Indirect effect-path a, b | −0.06 (−0.12, −0.01) | 0.94 (0.89,0.99) | 15.38% | — |
| Direct effect-path c’ | −0.33 (−0.60, −0.06) | 0.72 (0.55,0.94) | 84.62% | 0.017 * |
| Total effect-path c | −0.39 (−0.68, −0.14) | 0.68 (0.51,0.87) | 100% | 0.004 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, M.; Yu, F.; Xue, Y.; Song, L.; Du, M.; Li, X.; Li, W. The Relationship of 25(OH)D3 with Diabetes Mellitus and the Mediation Effect of Lipid Profile in Chinese Rural Population of Henan Province. Medicina 2022, 58, 85. https://doi.org/10.3390/medicina58010085
Zhang M, Yu F, Xue Y, Song L, Du M, Li X, Li W. The Relationship of 25(OH)D3 with Diabetes Mellitus and the Mediation Effect of Lipid Profile in Chinese Rural Population of Henan Province. Medicina. 2022; 58(1):85. https://doi.org/10.3390/medicina58010085
Chicago/Turabian StyleZhang, Mimi, Fei Yu, Yuan Xue, Lulu Song, Mengsi Du, Xing Li, and Wenjie Li. 2022. "The Relationship of 25(OH)D3 with Diabetes Mellitus and the Mediation Effect of Lipid Profile in Chinese Rural Population of Henan Province" Medicina 58, no. 1: 85. https://doi.org/10.3390/medicina58010085
APA StyleZhang, M., Yu, F., Xue, Y., Song, L., Du, M., Li, X., & Li, W. (2022). The Relationship of 25(OH)D3 with Diabetes Mellitus and the Mediation Effect of Lipid Profile in Chinese Rural Population of Henan Province. Medicina, 58(1), 85. https://doi.org/10.3390/medicina58010085