

Effect of 9% Hydrofluoric Acid Gel Hot-Etching Surface Treatment on Shear Bond Strength of Resin Cements to Zirconia Ceramics



Abstract
:1. Introduction
2. Material and Methods
- Control (CT): No surface treatment
- Sandblasting (SB): Specimens were sandblasted with 110-μm Al2O3 at an air pressure of 1 bar for 10 s.
- Hot-etching with 9% HF gel (HE): Specimens were etched using the Zirconia Etchant Cloud System in a safety shell according to the manufacturer’s recommended procedure for 10 min. The manufacturer’s recommended procedure is illustrated in Figure 1.
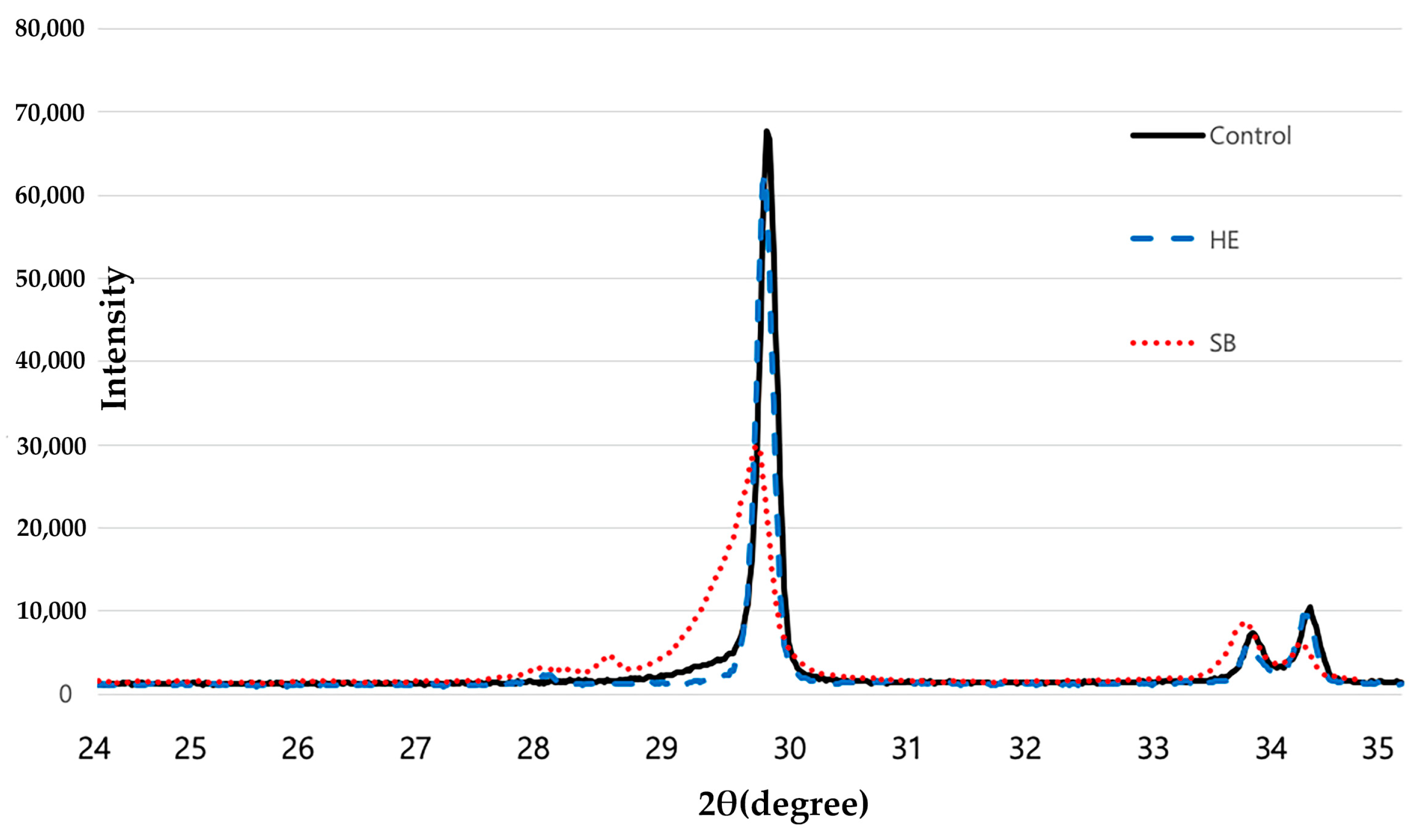
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Miyazaki, T.; Hotta, Y.; Kunii, J.; Kuriyama, S.; Tamaki, Y. A review of dental CAD/CAM: Current status and future perspectives from 20 years of experience. Dent. Mater. J. 2009, 28, 44–56. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.Y.; Stoner, B.R.; Piascik, J.R.; Smith, R. Adhesion/cementation to zirconia and other non-silicate ceramics: Where are we now? Dent. Mater. 2011, 27, 71–82. [Google Scholar] [CrossRef] [Green Version]
- Ardlin, B.I. Transformation-toughened zirconia for dental inlays, crowns and bridges: Chemical stability and effect of low-temperature aging on flexural strength and surface structure. Dent. Mater. 2002, 18, 590–595. [Google Scholar] [CrossRef]
- Blatz, M.B.; Sadan, A.; Kern, M. Resin-ceramic bonding: A review of the literature. J. Prosthet. Dent. 2003, 89, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Burke, F.J.; Fleming, G.J.; Nathanson, D.; Marquis, P.M. Are adhesive technologies needed to support ceramics? An assessment of the current evidence. J. Adhes. Dent. 2002, 4, 7–22. [Google Scholar]
- Stefani, A.; Brito, R.B., Jr.; Kina, S.; Andrade, O.S.; Ambrosano, G.M.; Carvalho, A.A.; Giannini, M. Bond Strength of Resin Cements to Zirconia Ceramic Using Adhesive Primers. J. Prosthodont. 2016, 25, 380–385. [Google Scholar] [CrossRef]
- Aboushelib, M.N.; Kleverlaan, C.J.; Feilzer, A.J. Selective infiltration-etching technique for a strong and durable bond of resin cements to zirconia-based materials. J. Prosthet. Dent. 2007, 98, 379–388. [Google Scholar] [CrossRef]
- Casucci, A.; Monticelli, F.; Goracci, C.; Mazzitelli, C.; Cantoro, A.; Papacchini, F.; Ferrari, M. Effect of surface pre-treatments on the zirconia ceramic-resin cement microtensile bond strength. Dent. Mater. 2011, 27, 1024–1030. [Google Scholar] [CrossRef]
- Kitayama, S.; Nikaido, T.; Takahashi, R.; Zhu, L.; Ikeda, M.; Foxton, R.M.; Sadr, A.; Tagami, J. Effect of primer treatment on bonding of resin cements to zirconia ceramic. Dent. Mater. 2010, 26, 426–432. [Google Scholar] [CrossRef]
- Lindgren, J.; Smeds, J.; Sjögren, G. Effect of surface treatments and aging in water on bond strength to zirconia. Oper. Dent. 2008, 33, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Piascik, J.R.; Wolter, S.D.; Stoner, B.R. Development of a novel surface modification for improved bonding to zirconia. Dent. Mater. 2011, 27, e99–e105. [Google Scholar] [CrossRef] [PubMed]
- Comino-Garayoa, R.; Peláez, J.; Tobar, C.; Rodríguez, V.; Suárez, M.J. Adhesion to Zirconia: A Systematic Review of Surface Pretreatments and Resin Cements. Materials 2021, 14, 2751. [Google Scholar] [CrossRef] [PubMed]
- Karakoca, S.; Yilmaz, H. Influence of surface treatments on surface roughness, phase transformation, and biaxial flexural strength of Y-TZP ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91, 930–937. [Google Scholar] [CrossRef]
- Sato, H.; Yamada, K.; Pezzotti, G.; Nawa, M.; Ban, S. Mechanical properties of dental zirconia ceramics changed with sandblasting and heat treatment. Dent. Mater. J. 2008, 27, 408–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blatz, M.B.; Chiche, G.; Holst, S.; Sadan, A. Influence of surface treatment and simulated aging on bond strengths of luting agents to zirconia. Quintessence Int. 2007, 38, 745–753. [Google Scholar] [PubMed]
- Atsu, S.S.; Kilicarslan, M.A.; Kucukesmen, H.C.; Aka, P.S. Effect of zirconium-oxide ceramic surface treatments on the bond strength to adhesive resin. J. Prosthet. Dent. 2006, 95, 430–436. [Google Scholar] [CrossRef]
- Blatz, M.B.; Sadan, A.; Martin, J.; Lang, B. In vitro evaluation of shear bond strengths of resin to densely-sintered high-purity zirconium-oxide ceramic after long-term storage and thermal cycling. J. Prosthet. Dent. 2004, 91, 356–362. [Google Scholar] [CrossRef]
- Kern, M.; Wegner, S.M. Bonding to zirconia ceramic: Adhesion methods and their durability. Dent. Mater. 1998, 14, 64–71. [Google Scholar] [CrossRef]
- Lüthy, H.; Loeffel, O.; Hammerle, C.H. Effect of thermocycling on bond strength of luting cements to zirconia ceramic. Dent. Mater. 2006, 22, 195–200. [Google Scholar] [CrossRef]
- Wolfart, M.; Lehmann, F.; Wolfart, S.; Kern, M. Durability of the resin bond strength to zirconia ceramic after using different surface conditioning methods. Dent. Mater. 2007, 23, 45–50. [Google Scholar] [CrossRef]
- Casucci, A.; Osorio, E.; Osorio, R.; Monticelli, F.; Toledano, M.; Mazzitelli, C.; Ferrari, M. Influence of different surface treatments on surface zirconia frameworks. J. Dent. 2009, 37, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Tada, K.; Sato, T.; Yoshinari, M. Influence of surface treatment on bond strength of veneering ceramics fused to zirconia. Dent. Mater. J. 2012, 31, 287–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamaguchi, H.; Ino, S.; Hamano, N.; Okada, S.; Teranaka, T. Examination of bond strength and mechanical properties of Y-TZP zirconia ceramics with different surface modifications. Dent. Mater. J. 2012, 31, 472–480. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.; Kim, R.H.; Lee, S.C.; Lee, T.K.; Hayashi, M.; Yu, B.; Jo, D.W. Evaluation of Tensile Bond Strength between Self-Adhesive Resin Cement and Surface-Pretreated Zirconia. Materials 2022, 15, 3089. [Google Scholar] [CrossRef] [PubMed]
- Alghazzawi, T.F.; Janowski, G.M. Evaluation of zirconia-porcelain interface using X-ray diffraction. Int. J. Oral. Sci. 2015, 7, 187–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sriamporn, T.; Thamrongananskul, N.; Busabok, C.; Poolthong, S.; Uo, M.; Tagami, J. Dental zirconia can be etched by hydrofluoric acid. Dent. Mater. J. 2014, 33, 79–85. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.H.; Kim, S.J.; Shim, J.S.; Lee, K.W. Effect of zirconia surface treatment using nitric acid-hydrofluoric acid on the shear bond strengths of resin cements. J. Adv. Prosthodont. 2017, 9, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Smielak, B.; Klimek, L. Effect of hydrofluoric acid concentration and etching duration on select surface roughness parameters for zirconia. J. Prosthet. Dent. 2015, 113, 596–602. [Google Scholar] [CrossRef]
- Canay, S.; Hersek, N.; Ertan, A. Effect of different acid treatments on a porcelain surface. J. Oral. Rehabil. 2001, 28, 95–101. [Google Scholar] [CrossRef]
- Elsaka, S.E. Influence of surface treatments on the surface properties of different zirconia cores and adhesion of zirconia-veneering ceramic systems. Dent. Mater. 2013, 29, e239–e251. [Google Scholar] [CrossRef]
- Kosmac, T.; Oblak, C.; Jevnikar, P.; Funduk, N.; Marion, L. The effect of surface grinding and sandblasting on flexural strength and reliability of Y-TZP zirconia ceramic. Dent. Mater. 1999, 15, 426–433. [Google Scholar] [CrossRef]
- Kang, Y.J.; Shin, Y.; Kim, J.H. Effect of Low-Concentration Hydrofluoric Acid Etching on Shear Bond Strength and Biaxial Flexural Strength after Thermocycling. Materials 2020, 13, 1409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wegner, S.M.; Kern, M. Long-term resin bond strength to zirconia ceramic. J. Adhes. Dent. 2000, 2, 139–147. [Google Scholar]
- Llerena-Icochea, A.E.; Costa, R.M.; Borges, A.; Bombonatti, J.; Furuse, A.Y. Bonding Polycrystalline Zirconia with 10-MDP-containing Adhesives. Oper. Dent. 2017, 42, 335–341. [Google Scholar] [CrossRef]
- Dias de Souza, G.M.; Thompson, V.P.; Braga, R.R. Effect of metal primers on microtensile bond strength between zirconia and resin cements. J. Prosthet. Dent. 2011, 105, 296–303. [Google Scholar] [CrossRef]
- Della Bona, A.; Kelly, J.R. The clinical success of all-ceramic restorations. J. Am. Dent. Assoc. 2008, 139, S8–S13. [Google Scholar] [CrossRef] [Green Version]
- Awliya, W.; Odén, A.; Yaman, P.; Dennison, J.B.; Razzoog, M.E. Shear bond strength of a resin cement to densely sintered high-purity alumina with various surface conditions. Acta Odontol. Scand. 1998, 56, 9–13. [Google Scholar] [CrossRef]
- Wang, H.; Aboushelib, M.N.; Feilzer, A.J. Strength influencing variables on CAD/CAM zirconia frameworks. Dent. Mater. 2008, 24, 633–638. [Google Scholar] [CrossRef]
- Zhang, Y.; Lawn, B.R.; Rekow, E.D.; Thompson, V.P. Effect of sandblasting on the long-term performance of dental ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2004, 71, 381–386. [Google Scholar] [CrossRef]
- Kim, H.K.; Yoo, K.W.; Kim, S.J.; Jung, C.H. Phase Transformations and Subsurface Changes in Three Dental Zirconia Grades after Sandblasting with Various Al2O3 Particle Sizes. Materials 2021, 14, 5321. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, C.H. Effect of the Surface Treatment Method Using Airborne-Particle Abrasion and Hydrofluoric Acid on the Shear Bond Strength of Resin Cement to Zirconia. Dent. J. 2017, 5, 23. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.H.; Son, J.S.; Kim, K.H.; Kwon, T.Y. Improved resin-zirconia bonding by room temperature hydrofluoric acid etching. Materials 2015, 8, 850–866. [Google Scholar] [CrossRef] [PubMed]
- Iijima, T.; Homma, S.; Sekine, H.; Sasaki, H.; Yajima, Y.; Yoshinari, M. Influence of surface treatment of yttria-stabilized tetragonal zirconia polycrystal with hot isostatic pressing on cyclic fatigue strength. Dent. Mater. J. 2013, 32, 274–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seo, S.H.; Kim, J.E.; Nam, N.E.; Moon, H.S. Effect of air abrasion, acid etching, and aging on the shear bond strength with resin cement to 3Y-TZP zirconia. J. Mech. Behav. Biomed. Mater. 2022, 134, 105348. [Google Scholar] [CrossRef]
- Akar, T.; Dündar, A.; Kırmalı, Ö.; Üstün, Ö.; Kapdan, A.; Er, H.; Kuştarcı, A.; Er, K.; Yılmaz, B. Evaluation of the shear bond strength of zirconia to a self-adhesive resin cement after different surface treatment. Dent. Med. Probl. 2021, 58, 463–472. [Google Scholar] [CrossRef]
- el Saadi, M.S.; Hall, A.H.; Hall, P.K.; Riggs, B.S.; Augenstein, W.L.; Rumack, B.H. Hydrofluoric acid dermal exposure. Vet. Hum. Toxicol. 1989, 31, 243–247. [Google Scholar]
- Wu, M.L.; Yang, C.C.; Ger, J.; Tsai, W.J.; Deng, J.F. Acute hydrofluoric acid exposure reported to Taiwan Poison Control Center, 1991–2010. Hum. Exp. Toxicol. 2014, 33, 449–454. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Manufacturer | Composition |
|---|---|---|
| Maxcem Elite | Kerr Corporation Brea, CA, USA | GPDM, Monomers, Nonhazardous inert mineral fillers, Ytterbium fluoride, Activators, Stabilizers, and Colorants |
| MAZIC Cem | Vericom Co., Ltd. Chuncheon, Korea | Barium silicate, Fluorinated barium silicate, Fumed silica, MDP, Bis-GMA, Dimethacrylate, Catalyst, Stabilizer, Pigments |
| RelyX U200 | 3M ESPE, Maplewood, MN, USA | Methacrylate monomers containing phosphoric acid group, Methacrylate monomers, Silanated fillers, Alkaline (basic) fillers, Initiator components, Stabilizers, Rheological additives, Pigments |
| Surface Treatment | Surface Roughness Values, Ra (μm) | Peak to Valley Roughness, Rt (μm) |
|---|---|---|
| Control (CT) | 0.190 ± 0.01 | 2.40 ± 0.28 |
| Sandblast (SB) | 0.320 ± 0.01 | 4.21 ± 0.42 |
| HF etching (HE) | 0.230 ± 0.01 | 3.03 ± 0.69 |
| Surface Treatment | N | Maxcem Elite | MAZIC Cem | RelayX U200 | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| Control (CT) | 15 | 0.76 | 0.35 | 4.93 | 1.42 | 3.33 | 1.27 |
| Al2O3 Sandblast (SB) | 15 | 3.38 | 2.09 | 6.80 | 2.11 | 6.00 | 0.78 |
| HF Etching (HE) | 15 | 6.98 | 1.81 | 9.53 | 1.50 | 7.27 | 1.32 |
| Resin Cement | Comparing Surface Treatment | 95% Confidence Interval | |||
|---|---|---|---|---|---|
| Mean Difference | Lower Bound | Upper Bound | p-Value | ||
| Maxcem Elite | Control–SB | −2.61358 | −4.0424 | −1.1848 | 0.000 |
| Control–HE | −6.21811 | −7.6469 | −4.7893 | 0.000 | |
| SB–HE | −3.60453 | −5.0333 | −2.1757 | 0.000 | |
| MAZIC Cem | Control–SB | −1.87301 | −3.3842 | −0.3618 | 0.012 |
| Control–HE | −4.59795 | −6.1092 | −3.0867 | 0.000 | |
| SB–HE | −2.72494 | −4.2362 | −1.2137 | 0.000 | |
| RelayX U200 | Control–SB | −2.67207 | −3.6954 | −1.6487 | 0.000 |
| Control–HE | −4.24693 | −5.2703 | −3.2236 | 0.000 | |
| SB–HE | −1.57485 | −2.5982 | −0.5515 | 0.002 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.-H.; Cho, S.-C.; Lee, M.-H.; Kim, H.-J.; Oh, N.-S. Effect of 9% Hydrofluoric Acid Gel Hot-Etching Surface Treatment on Shear Bond Strength of Resin Cements to Zirconia Ceramics. Medicina 2022, 58, 1469. https://doi.org/10.3390/medicina58101469
Kim S-H, Cho S-C, Lee M-H, Kim H-J, Oh N-S. Effect of 9% Hydrofluoric Acid Gel Hot-Etching Surface Treatment on Shear Bond Strength of Resin Cements to Zirconia Ceramics. Medicina. 2022; 58(10):1469. https://doi.org/10.3390/medicina58101469
Chicago/Turabian StyleKim, So-Hyun, Sung-Chan Cho, Myung-Hyun Lee, Hyo-Jung Kim, and Nam-Sik Oh. 2022. "Effect of 9% Hydrofluoric Acid Gel Hot-Etching Surface Treatment on Shear Bond Strength of Resin Cements to Zirconia Ceramics" Medicina 58, no. 10: 1469. https://doi.org/10.3390/medicina58101469
APA StyleKim, S. -H., Cho, S. -C., Lee, M. -H., Kim, H. -J., & Oh, N. -S. (2022). Effect of 9% Hydrofluoric Acid Gel Hot-Etching Surface Treatment on Shear Bond Strength of Resin Cements to Zirconia Ceramics. Medicina, 58(10), 1469. https://doi.org/10.3390/medicina58101469