
To Angulate or Not to Angulate the Ulna during the Progressive Distraction Period Performed with a Monolateral External Fixator in Paediatric Patients with a Chronic Monteggia Fracture?

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
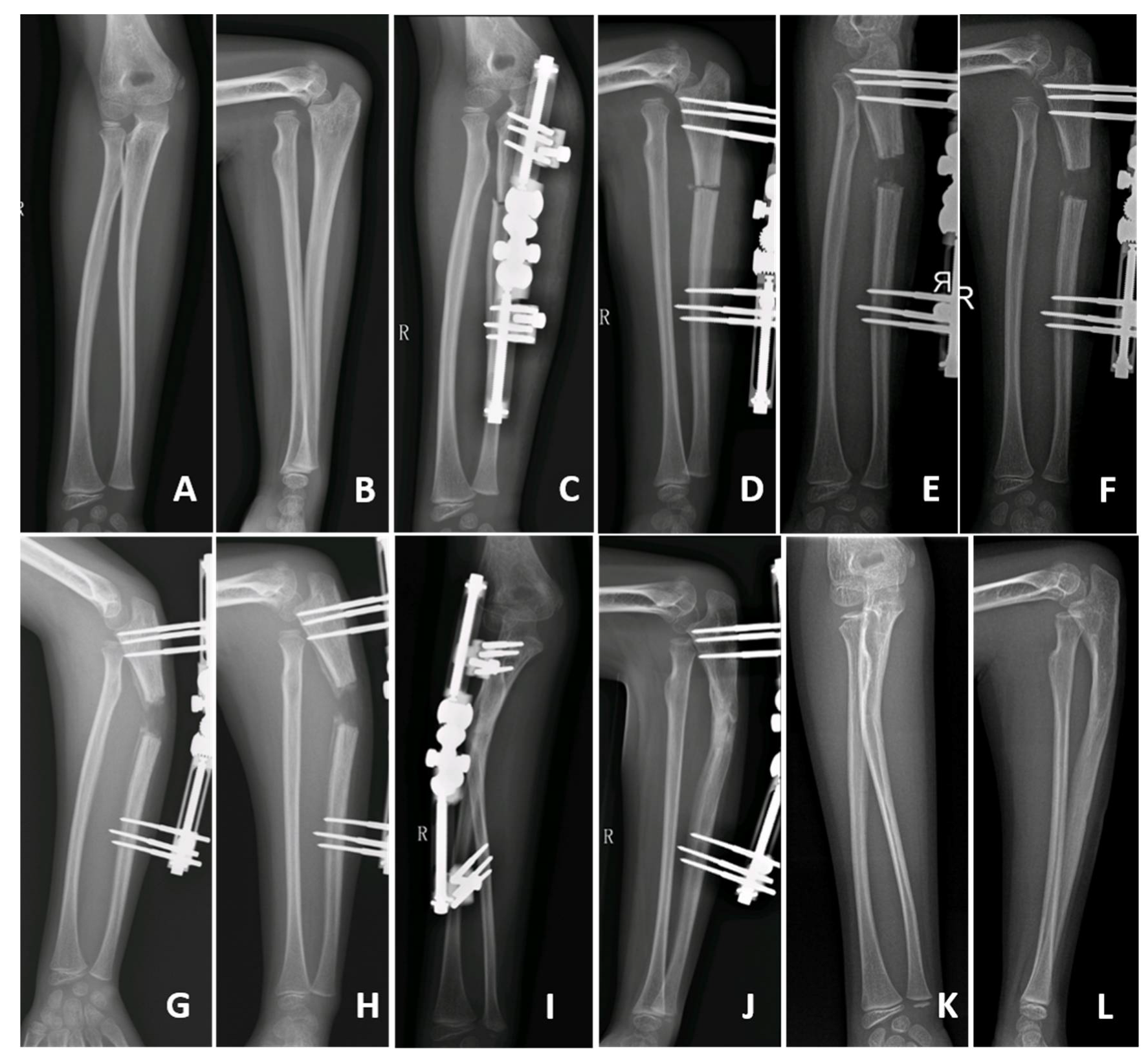
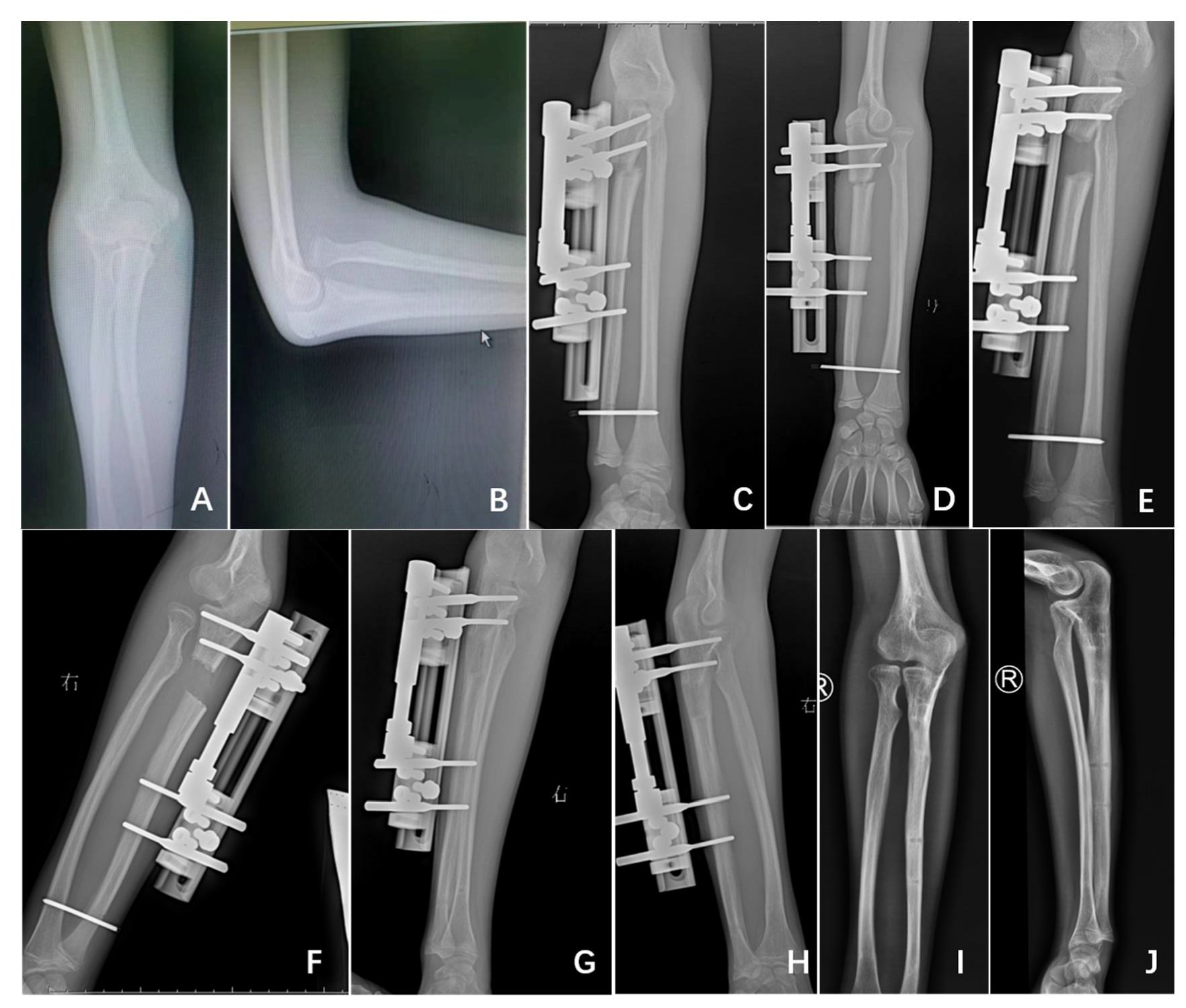
2.1. Surgical Technique
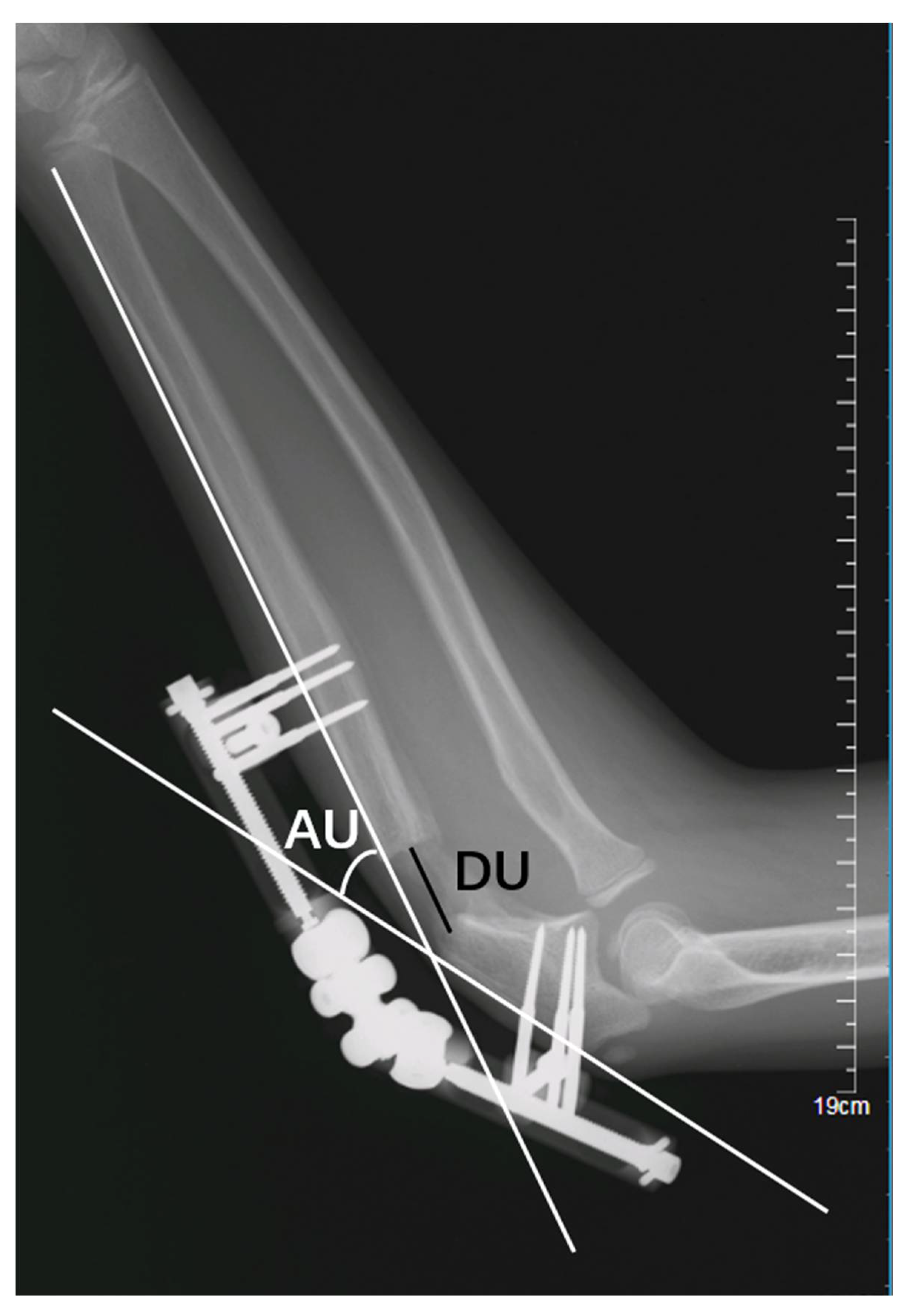
2.2. Radiological Evaluation
- (1)
- Lengthening distance of the ulna (DU): the distance, in millimetres (mm), between the proximal and distal fragments of the fractured ulna (Figure 3); and
- (2)
- Angulation of the ulna (AU): the angle, in degrees, between the line passing at the level of posterior cortex of the proximal and the distal fragment of the fractured ulna (Figure 3);
2.3. Clinical Outcomes
2.4. Statistical Analysis
3. Results
3.1. Radiological Evaluation
3.2. Clinical Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethical approval
References
- Rehim, S.A.; Maynard, M.A.; Sebastin, S.J.; Chung, K.C. Monteggia fracture dislocations: A historical review. J. Hand Surg. 2014, 39, 1384–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soni, J.F.; Valenza, W.R.; Pavelec, A.C. Chronic Monteggia. Curr. Opin. Pediatr. 2019, 31, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Soni, J.F.; Valenza, W.R.; Matsunaga, C.U.; Costa, A.C.P.; Faria, F.F. Chronic monteggia fracture-dislocation in children surgical strategy and results. Acta Ortop. Bras. 2019, 27, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Baydar, M.; Öztürk, K.; Orman, O.; Akbulut, D.; Keskinbıçkı, M.V.; Şencan, A. Use of Corrective Ulnar Osteotomy and Radial Head Relocation Into Preserved Annular Ligament in the Treatment of Radiocapitellar Instability Secondary to Pediatric Chronic Monteggia Fracture-Dislocation. J. Hand Surg. Am. 2021, 47, 481.e1–481.e9. [Google Scholar] [CrossRef] [PubMed]
- Stoll, T.M.; Willis, R.B.; Paterson, D.C. Treatment of the missed Monteggia fracture in the child. J. Bone Jt. Surg. Br. 1992, 74, 436–440. [Google Scholar] [CrossRef] [Green Version]
- Eamsobhana, P.; Chalayon, O.; Kaewpornsawan, K.; Ariyawatkul, T. Missed Monteggia fracture dislocations treated by open reduction of the radial head. Bone Jt. J. 2018, 100, 1117–1124. [Google Scholar] [CrossRef]
- Nakamura, K.; Hirachi, K.; Uchiyama, S.; Takahara, M.; Minami, A.; Imaeda, T.; Kato, H. Long-term clinical and radiographic outcomes after open reduction for missed Monteggia fracture-dislocations in children. J. Bone Jt. Surg. Am. 2009, 91, 1394–1404. [Google Scholar] [CrossRef]
- Wang, Q.; Du, M.M.; Pei, X.J.; Luo, J.Z.; Li, Y.Z.; Liu, Y.C.; Wang, X.; Cao, J.C.; Han, J.H. External Fixator-assisted Ulnar Osteotomy: A Novel Technique to Treat Missed Monteggia Fracture in Children. Orthop. Surg. 2019, 11, 102–108. [Google Scholar] [CrossRef] [Green Version]
- Liao, S.; Pan, J.; Lin, H.; Xu, Y.; Lu, R.; Wu, J.; Zhao, M.; Chen, H.; Cai, M.; Ding, X.; et al. A new approach for surgical treatment of chronic Monteggia fracture in children. Injury 2019, 50, 1237–1241. [Google Scholar] [CrossRef]
- Chen, H.Y.; Wu, K.W.; Dong, Z.R.; Huang, S.C.; Kuo, K.N.; Wang, T.M. The treatment of chronic radial head dislocation in Monteggia fracture without annular ligament reconstruction. Int. Orthop. 2018, 42, 2165–2172. [Google Scholar] [CrossRef]
- Song, K.S.; Ramnani, K.; Bae, K.C.; Cho, C.H.; Lee, K.J.; Son, E.S. Indirect reduction of the radial head in children with chronic Monteggia lesions. J. Orthop. Trauma 2012, 26, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Z.; Xu, H.W.; Liu, Y.Z.; Li, Y.Q.; Li, J.C.; Canavese, F. The use of external fixation for the management of acute and chronic Monteggia fractures in children. J. Child. Orthop. 2019, 13, 551–559. [Google Scholar] [CrossRef] [PubMed]
- Llusà Perez, M.; Lamas, C.; Martínez, I.; Pidemunt, G.; Mir, X. Monteggia fractures in adults. Review of 54 cases. Chir. Main 2002, 21, 293–297. [Google Scholar] [CrossRef]
- Delpont, M.; Louahem, D.; Cottalorda, J. Monteggia injuries. Orthop. Traumatol. Surg. Res. 2018, 104, S113–S120. [Google Scholar] [CrossRef]
- Goyal, T.; Arora, S.S.; Banerjee, S.; Kandwal, P. Neglected Monteggia fracture dislocations in children: A systematic review. J. Pediatr. Orthop. B 2015, 24, 191–199. [Google Scholar] [CrossRef]
- Miller, T.C.; Fishman, F.G. Management of Monteggia Injuries in the Pediatric Patient. Hand Clin. 2020, 36, 469–478. [Google Scholar] [CrossRef]
- Exner, G.U. Missed chronic anterior Monteggia lesion. Closed reduction by gradual lengthening and angulation of the ulna. J. Bone Jt. Surg. Br. 2001, 83, 547–550. [Google Scholar] [CrossRef]
- Kim, H.T.; Conjares, J.N.; Suh, J.T.; Yoo, C.I. Chronic radial head dislocation in children, Part 1: Pathologic changes preventing stable reduction and surgical correction. J. Pediatr. Orthop. 2002, 22, 583–590. [Google Scholar] [CrossRef]
- Kim, H.T.; Park, B.G.; Suh, J.T.; Yoo, C.I. Chronic radial head dislocation in children, Part 2: Results of open treatment and factors affecting final outcome. J. Pediatr. Orthop. 2002, 22, 591–597. [Google Scholar] [CrossRef]
- Bado, J.L. The Monteggia lesion. Clin. Orthop. Relat. Res. 1967, 50, 71–86. [Google Scholar] [CrossRef]
- Gryson, T.; Van Tongel, A.; Plasschaert, F. The management of chronic paediatric Monteggia fracture-dislocation. J. Orthop. 2021, 24, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Take, M.; Tomori, Y.; Sawaizumi, T.; Majima, T.; Nanno, M.; Takai, S. Ulnar osteotomy and the ilizarov mini-fixator for pediatric chronic monteggia fracture-dislocations. Med. (Baltim) 2019, 98, e13978. [Google Scholar] [CrossRef]
- Bor, N.; Rubin, G.; Rozen, N.; Herzenberg, J.E. Chronic anterior monteggia lesions in children: Report of 4 cases treated with closed reduction by ulnar osteotomy and external fixation. J. Pediatr. Orthop. 2015, 35, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Hirayama, T.; Takemitsu, Y.; Yagihara, K.; Mikita, A. Operation for chronic dislocation of the radial head in children. Reduction by osteotomy of the ulna. J. Bone Jt. Surg. Br. 1987, 69, 639–642. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oka, K.; Tanaka, H.; Shigi, A.; Abe, S.; Miyamura, S.; Shiode, R.; Kazui, A.; Murase, T. Quantitative Analysis for the Change in Lengths of the Radius and Ulna in Missed Bado Type I Monteggia Fracture. J. Pediatr. Orthop. 2020, 40, e922–e926. [Google Scholar] [CrossRef] [PubMed]
- Huang, P.; Zhu, L.; Ning, B. Forearm Deformity and Radial Head Dislocation in Pediatric Patients with Hereditary Multiple Exostoses: A Prospective Study Using Proportional Ulnar Length as a Scale to Lengthen the Shortened Ulna. J. Bone Jt. Surg. Am. 2020, 102, 1066–1074. [Google Scholar] [CrossRef]
- Tan, S.H.S.; Low, J.Y.; Chen, H.; Tan, J.Y.H.; Lim, A.K.S.; Hui, J.H. Surgical Management of Missed Pediatric Monteggia Fractures: A Systematic Review and Meta-Analysis. J. Orthop. Trauma 2022, 36, 65–73. [Google Scholar] [CrossRef]
- Lädermann, A.; Ceroni, D.; Lefèvre, Y.; De Rosa, V.; De Coulon, G.; Kaelin, A. Surgical treatment of missed Monteggia lesions in children. J. Child. Orthop. 2007, 1, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.N.; Chang, W.N. Chronic posttraumatic anterior dislocation of the radial head in children: Thirteen cases treated by open reduction, ulnar osteotomy, and annular ligament reconstruction through a Boyd incision. J. Orthop. Trauma 2006, 20, 1–5. [Google Scholar] [CrossRef]
- Jauregui, J.J.; Ventimiglia, A.V.; Grieco, P.W.; Frumberg, D.B.; Herzenberg, J.E. Regenerate bone stimulation following limb lengthening: A meta-analysis. BMC Musculoskelet. Disord. 2016, 17, 407. [Google Scholar] [CrossRef]
- Hosny, G.A. Limb lengthening history, evolution, complications and current concepts. J. Orthop. Traumatol 2020, 21, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahbek, O.; Deutch, S.R.; Kold, S.; Søjbjerg, J.O.; Møller-Madsen, B. Long-term outcome after ulnar osteotomy for missed Monteggia fracture dislocation in children. J. Child. Orthop. 2011, 5, 449–457. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient | Treatment | Duration of Distraction (Days) | External Fixator Modifications | AU (Degrees) | LU (mm) | Radial Head Reduction | Redislocation | Kim et al. Elbow Performance Score [18,19] |
|---|---|---|---|---|---|---|---|---|
| 1 | UO+GLA | 41 | Days 7–26: L Days 27–48: A | 36 | 19 | Yes | No | Excellent |
| 2 | UO+GLA | 14 | Days 7–21: L+A | 21 | 16 | Yes | No | Excellent |
| 3 | UO+GLA | 28 | Days 7–22: L Days 23–29: A Days 30–35: L | 18 | 19 | Yes | No | Excellent |
| 4 | UO+GLA | 18 | Days 7–10: L+A Days 11–25: L | 23 | 9 | Yes | No | Excellent |
| 5 | UO+GLA | 21 | Days 7–21: L Days 22–28: A | 25 | 12 | Yes | No | Excellent |
| 6 | UO+GLA | 48 | Days 7–41: L Days 42–55: A | 17 | 42 | Yes | No | Excellent |
| 7 | UO+GLA | 49 | Days 7–27: L Days 28–42: A Days 43–56: L | 26 | 22 | Yes | No | Excellent |
| 8 | UO+GLA | 75 | Days 7–14: L Days 15–21: L+A Days 22–82 | 27 | 36 | Yes | No | Excellent |
| 9 | UO+GLA | 52 | Day 0: A Days 7–59: L+A | 35 | 23 | Yes | No | Excellent |
| 10 | UO+GLA | 30 | Days 7–13: A Days 14–37: L | 25 | 17 | Dislocated | - | Poor |
| 11 | UO+GLA | 55 | Day 0: A Days 7–62: L | 32 | 25 | Yes | No | Excellent |
| 12 | UO+GL | 20 | Days 7–27: L | 0 | 18 | Yes | No | Excellent |
| 13 | UO+GL | 18 | Days 7–25: L | 0 | 12 | Yes | No | Excellent |
| 14 | UO+GL | 18 | Days 7–25: L | 0 | 11 | Yes | No | Excellent |
| 15 | UO+GL | 22 | Days 7–29: L | 0 | 25 | Yes | No | Excellent |
| 16 | UO+GL | 10 | Days 7–17: L | 0 | 10 | Yes | No | Excellent |
| 17 | UO+GL | 28 | Days 7–35: L | 3 | 21 | Yes | No | Excellent |
| 18 | UO+GL | 18 | Days 7–25: L | 0 | 8 | Yes | No | Excellent |
| 19 | UO+GL | 12 | Days 7–19: L | 0 | 11 | Yes | No | Excellent |
| 20 | UO+GL | 17 | Days 7–24: L | 2 | 11 | Yes | No | Excellent |
| Parameters | 25 Points | 15 Points | 0 Points |
|---|---|---|---|
| Deformity | No concern | Minor concern | Major concern |
| Pain | No pain | Intermittent mild pain but no limit to activities | Pain |
| Range of movement * | >250° | 200° to 250° | <200° |
| Function | Five activities of daily living: combing hair, feeding self, opening doorknob, grabbing the high object, putting on shoes with hands | Five points for each activity | |
| No. of patients/outcome | 15/good | 2/fair | 2/poor |
| Group A (n = 11) | Group B (n = 9) | p Value | |
|---|---|---|---|
| Gender (male/female) | 8/3 | 6/3 | 1.00 |
| Laterality (left/right) | 3/8 | 3/6 | 1.00 |
| Age at surgery (year) | 8.1 | 7.2 | 0.40 |
| Time between trauma and surgery (months) | 23.3 | 30 | 0.60 |
| Follow-up (months) | 20.8 | 29.4 | 0.10 |
| The duration of radial head reduction | 39.2 | 18.1 | 0.004 |
| Mean angulation of the ulna (degrees) | 25.9 | 0.6 | 0.00 |
| Mean lengthening of the ulna (mm) | 21.8 | 14.1 | 0.05 |
| Kim et al. Elbow Performance Score | 1.00 | ||
| Excellent | 10 | 9 | |
| Good | 0 | 0 | |
| Fair | 0 | 0 | |
| Poor | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, Y.; Zhao, H.; Xu, H.; Shi, W.; Li, J.; Li, Y.; Canavese, F. To Angulate or Not to Angulate the Ulna during the Progressive Distraction Period Performed with a Monolateral External Fixator in Paediatric Patients with a Chronic Monteggia Fracture? Medicina 2022, 58, 1666. https://doi.org/10.3390/medicina58111666
Liu Y, Zhao H, Xu H, Shi W, Li J, Li Y, Canavese F. To Angulate or Not to Angulate the Ulna during the Progressive Distraction Period Performed with a Monolateral External Fixator in Paediatric Patients with a Chronic Monteggia Fracture? Medicina. 2022; 58(11):1666. https://doi.org/10.3390/medicina58111666
Chicago/Turabian StyleLiu, Yanhan, Hai Zhao, Hongwen Xu, Weizhe Shi, Jingchun Li, Yiqiang Li, and Federico Canavese. 2022. "To Angulate or Not to Angulate the Ulna during the Progressive Distraction Period Performed with a Monolateral External Fixator in Paediatric Patients with a Chronic Monteggia Fracture?" Medicina 58, no. 11: 1666. https://doi.org/10.3390/medicina58111666
APA StyleLiu, Y., Zhao, H., Xu, H., Shi, W., Li, J., Li, Y., & Canavese, F. (2022). To Angulate or Not to Angulate the Ulna during the Progressive Distraction Period Performed with a Monolateral External Fixator in Paediatric Patients with a Chronic Monteggia Fracture? Medicina, 58(11), 1666. https://doi.org/10.3390/medicina58111666