
Do the Number, Size, and Position of Partially Threaded Screws Affect the Radiological Healing of Surgically Treated Displaced Femoral Neck Fractures? A Review of 136 Children


 ,
,
Abstract
:1. Introduction
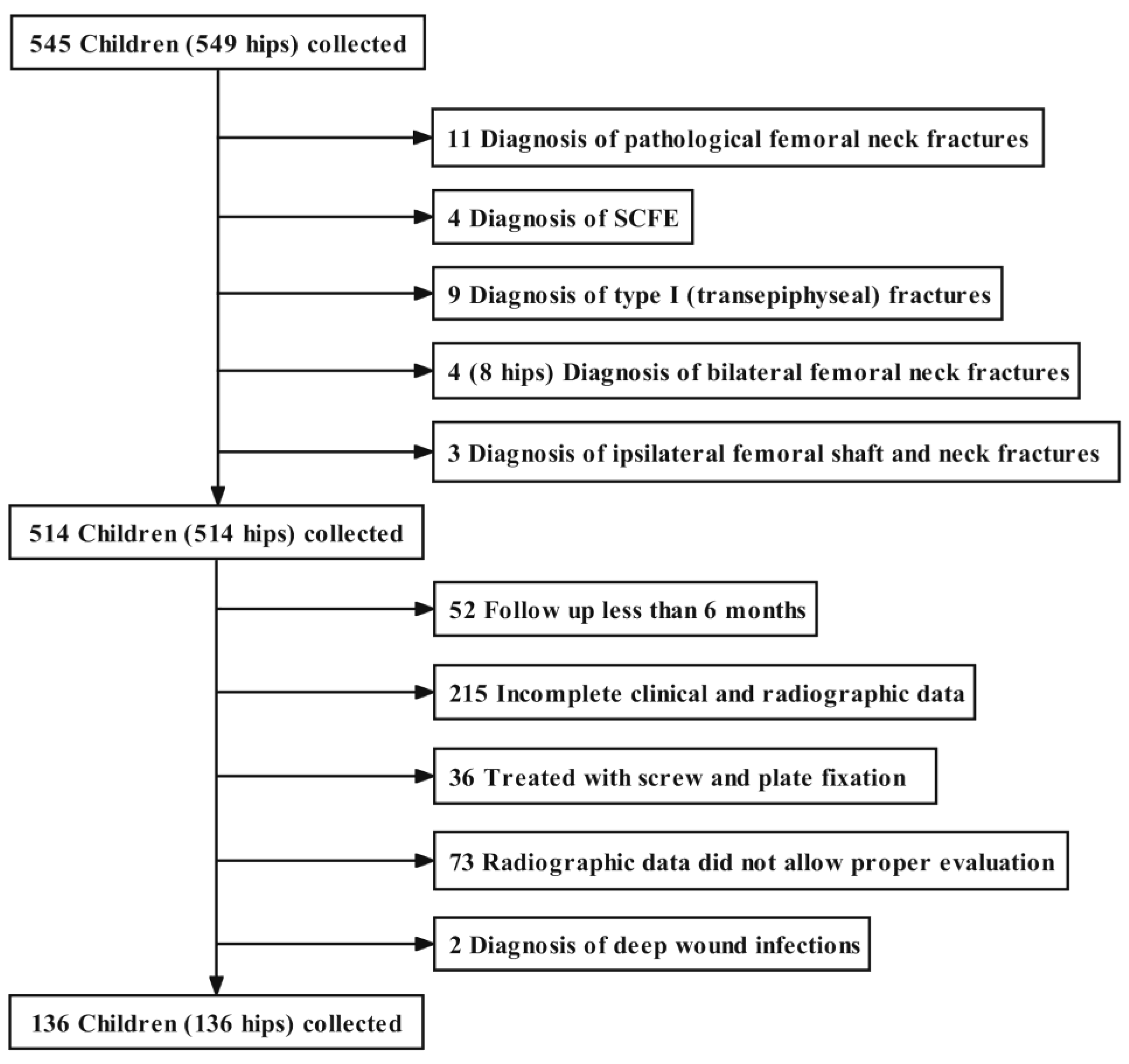
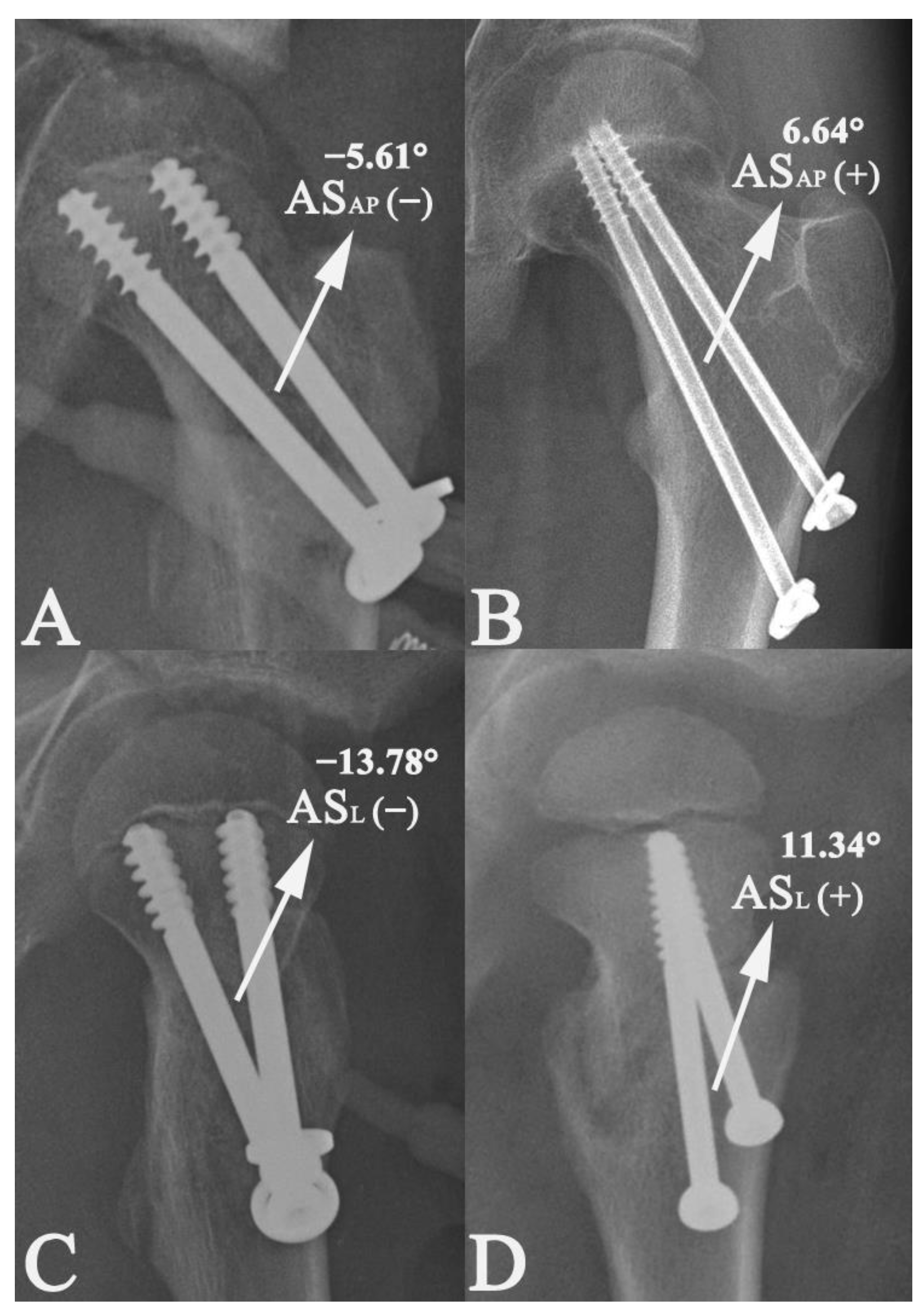
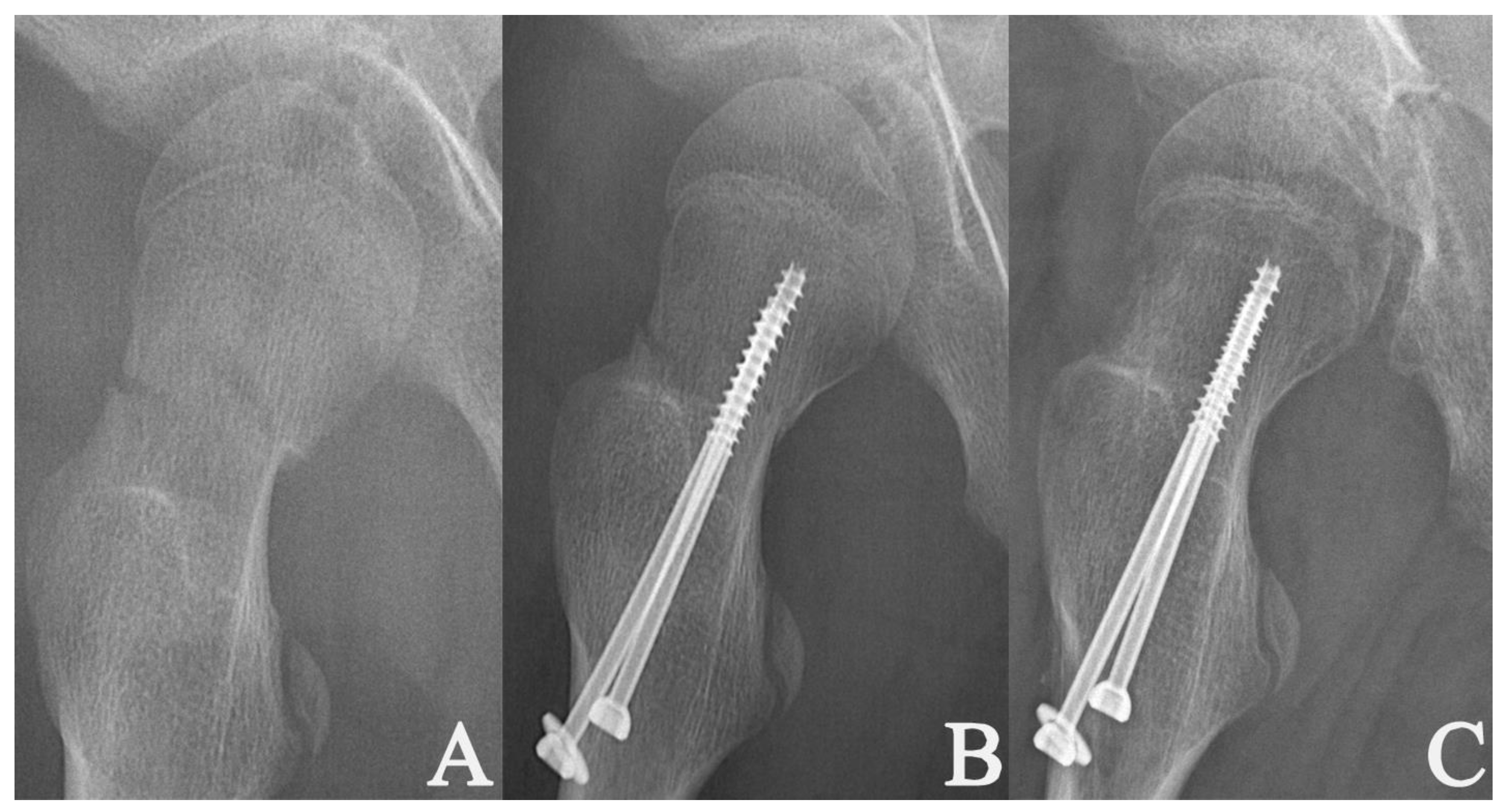
2. Materials and Methods
Statistical Analysis
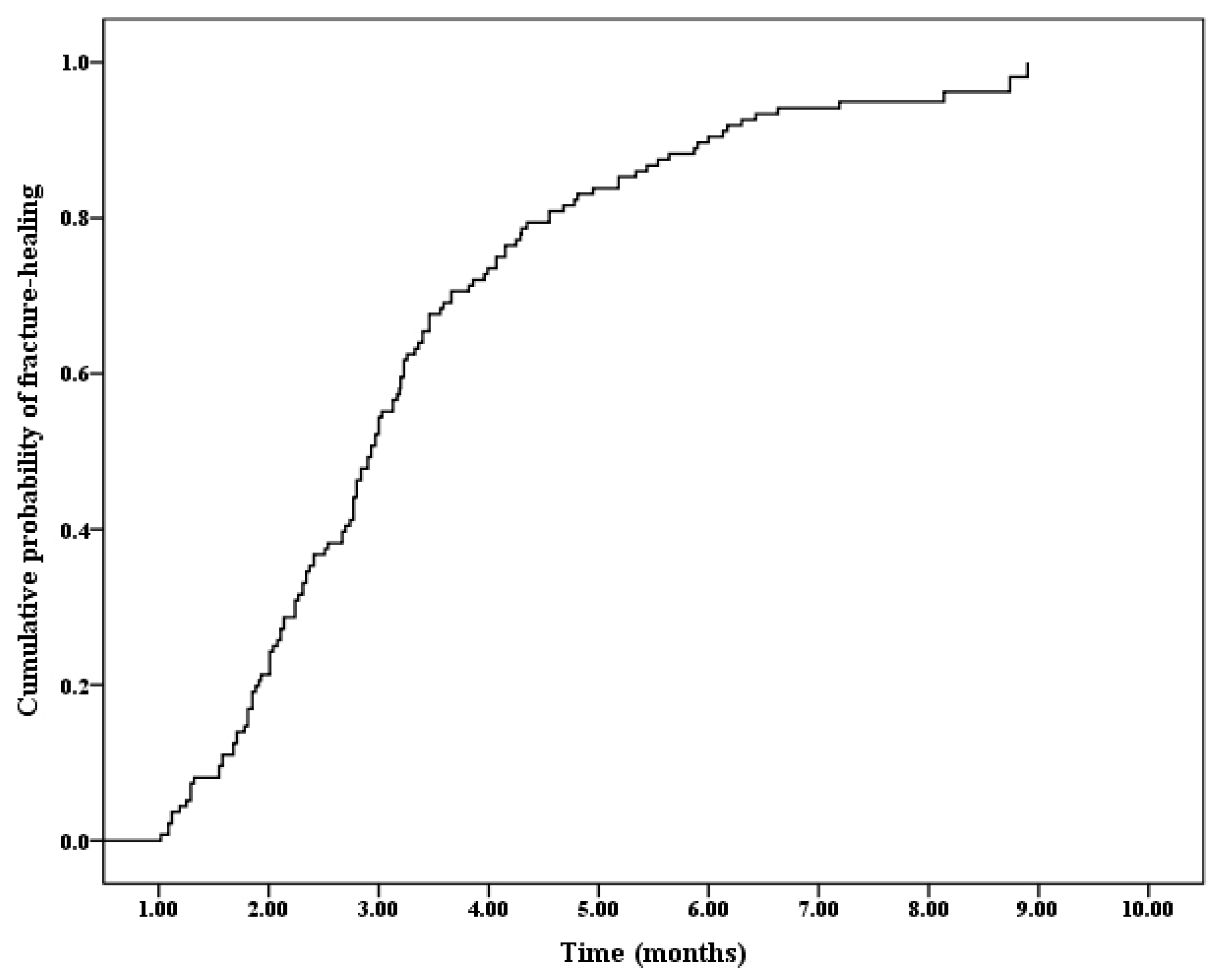
3. Results
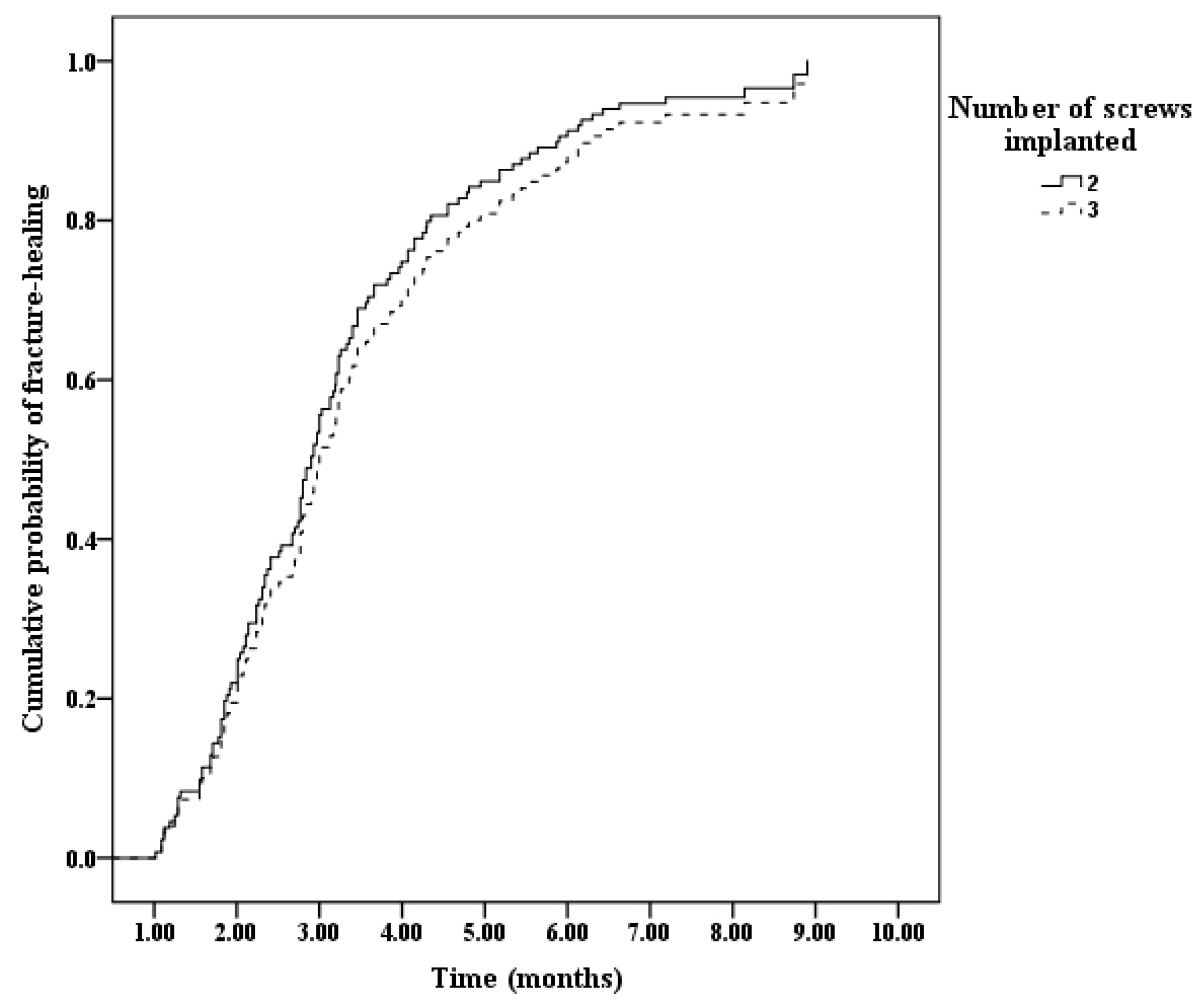
3.1. Time Needed to Achieve Healing in the Fractures Treated by Two or Three PTCSs (n = 132)
3.2. Time Needed to Achieve Healing in the Fractures Treated by Two PTCSs (n = 100)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Bimmel, R.; Bakker, A.; Bosma, B.; Michielsen, J. Paediatric hip fractures: A systematic review of incidence, treatment options and complications. Acta Orthop. Belg. 2010, 76, 7–13. [Google Scholar]
- Wang, W.; Li, Y.; Guo, Y.; Li, M.; Mei, H.; Shao, J.; Xiong, Z.; Li, J.; Canavese, F.; Chen, S.; et al. Initial displacement as a risk factor for avascular necrosis of the femoral head in pediatric femoral neck fractures: A review of one hundred eight cases. Int. Orthop. 2020, 44, 129–139. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xiong, Z.; Li, Y.; Guo, Y.; Li, M.; Mei, H.; Canavese, F.; Chen, S. Chinese Multicenter Pediatric Orthopedic Study Group (CMPOS). Variables influencing radiological fracture healing in children with femoral neck fractures treated surgically: A review of 177 cases. Orthop. Traumatol. Surg. Res. 2022, 108, 103052. [Google Scholar] [CrossRef] [PubMed]
- Togrul, E.; Bayram, H.; Gulsen, M.; Kalaci, A.; Ozbarlas, S. Fractures of the femoral neck in children: Long-term follow-up in 62 hip fractures. Injury 2005, 36, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Song, K.S. Displaced fracture of the femoral neck in children: Open versus closed reduction. J. Bone Jt. Surg. Br. 2010, 92, 1148–1151. [Google Scholar] [CrossRef]
- Rouleau, J.P.; Blasier, R.B.; Tsai, E.; Goldstein, S.A. Cannulated hip screws: A study of fixation integrity, cut-out resistance, and high-cycle bending fatigue performance. J. Orthop. Trauma 1994, 8, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Tian, L.; Yan, Y.; Sang, H.; Ma, Z.; Jie, Q.; Lei, W.; Wu, Z. Biomechanical evaluation of the expansive cannulated screw for fixation of femoral neck fractures. Injury 2011, 42, 1372–1376. [Google Scholar] [CrossRef]
- Pesce, V.; Maccagnano, G.; Vicenti, G.; Notarnicola, A.; Moretti, L.; Tafuri, S.; Vanni, D.; Salini, V.; Moretti, B. The effect of hydroxyapatite coated screw in the lateral fragility fractures of the femur. A prospective randomized clinical study. J. Biol. Regul. Homeost. Agents 2014, 28, 125–132. [Google Scholar]
- Wang, W.; Li, Y.; Xiong, Z.; Guo, Y.; Li, M.; Mei, H.; Shao, J.; Li, J.; Canavese, F.; Chen, S. Effect of the Number, Size, and Location of Cannulated Screws on the Incidence of Avascular Necrosis of the Femoral Head in Pediatric Femoral Neck Fractures: A Review of 153 Cases. J. Pediatr. Orthop. 2022, 42, 149–157. [Google Scholar] [CrossRef]
- Canale, S.T. Fractures of the hip in children and adolescents. Orthop. Clin. N. Am. 1990, 21, 341–352. [Google Scholar] [CrossRef]
- Patterson, J.T.; Tangtiphaiboontana, J.; Pandya, N.K. Management of Pediatric Femoral Neck Fracture. J. Am. Acad. Orthop. Surg. 2018, 26, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Von Keudell, A.; McTague, M.; Rodriguez, E.K.; Weaver, M.J. Ideal length of thread forms for screws used in screw fixation of nondisplaced femoral neck fractures. Injury 2019, 50, 727–732. [Google Scholar] [CrossRef]
- Parker, M.J.; Ali, S.M. Short versus long thread cannulated cancellous screws for intracapsular hip fractures: A randomised trial of 432 patients. Injury 2010, 41, 382–384. [Google Scholar] [CrossRef]
- Miller, W.E. Fractures of the hip in children from birth to adolescence. Clin. Orthop. Relat. Res. 1973, 92, 155–188. [Google Scholar] [CrossRef] [PubMed]
- Colonna, P.C. Fracture of the neck of the femur in children. Am. J. Surg. 1929, 6, 793. [Google Scholar] [CrossRef]
- Clohisy, J.C.; Carlisle, J.C.; Beaulé, P.E.; Kim, Y.J.; Trousdale, R.T.; Sierra, R.J.; Leunig, M.; Schoenecker, P.L.; Millis, M.B. A systematic approach to the plain radiographic evaluation of the young adult hip. J. Bone Jt. Surg. Am. 2008, 90 (Suppl. S4), 47–66. [Google Scholar] [CrossRef]
- Siebenrock, K.A.; Kalbermatten, D.F.; Ganz, R. Effect of pelvic tilt on acetabular retroversion: A study of pelves from cadavers. Clin. Orthop. Relat. Res. 2003, 407, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.T.; Li, Y.Q.; Guo, Y.M.; Li, M.; Mei, H.B.; Shao, J.F.; Xiong, Z.; Li, J.; Canavese, F.; Chen, S.Y. Risk factors for the development of avascular necrosis after femoral neck fractures in children: A review of 239 cases. Bone Jt. J. 2019, 101-B, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- Corrales, L.A.; Morshed, S.; Bhandari, M.; Miclau, T., 3rd. Variability in the assessment of fracture-healing in orthopaedic trauma studies. J. Bone Jt. Surg. Am. 2008, 90, 1862–1868. [Google Scholar] [CrossRef] [PubMed]
- Hammer, R.R.; Hammerby, S.; Lindholm, B. Accuracy of radiologic assessment of tibial shaft fracture union in humans. Clin. Orthop. Relat. Res. 1985, 199, 233–238. [Google Scholar] [CrossRef]
- Maccagnano, G.; Notarnicola, A.; Pesce, V.; Tafuri, S.; Mudoni, S.; Nappi, V.; Moretti, B. Failure Predictor Factors of Conservative Treatment in Pediatric Forearm Fractures. BioMed Res. Int. 2018, 2018, 5930106. [Google Scholar] [CrossRef] [PubMed]
- Eberl, R.; Singer, G.; Ferlic, P.; Weinberg, A.M.; Hoellwarth, M.E. Post-traumatic coxa vara in children following screw fixation of the femoral neck. Acta Orthop. 2010, 81, 442–445. [Google Scholar] [CrossRef] [PubMed]
- Pavone, V.; Testa, G.; Riccioli, M.; Di Stefano, A.; Condorelli, G.; Sessa, G. Surgical treatment with cannulated screws for pediatric femoral neck fractures: A case series. Injury 2019, 50 (Suppl. S2), S40–S44. [Google Scholar] [CrossRef] [PubMed]
- Shrader, M.W.; Jacofsky, D.J.; Stans, A.A.; Shaughnessy, W.J.; Haidukewych, G.J. Femoral neck fractures in pediatric patients: 30 years experience at a level 1 trauma center. Clin. Orthop. Relat. Res. 2007, 454, 169–173. [Google Scholar] [CrossRef]
- Quinlan, W.R.; Brady, P.G.; Regan, B.F. Fracture of the neck of the femur in childhood. Injury 1980, 11, 242–247. [Google Scholar] [CrossRef]
- Hajdu, S.; Oberleitner, G.; Schwendenwein, E.; Ringl, H.; Vécsei, V. Fractures of the head and neck of the femur in children: An outcome study. Int. Orthop. 2011, 35, 883–888. [Google Scholar] [CrossRef]
- Lim, E.J.; Kim, B.S.; Kim, C.H. Parallel and non-parallel cannulated screw fixation complications in femoral neck fractures: A systematic review and meta-analysis. Orthop. Traumatol. Surg. Res. 2021, 107, 103005. [Google Scholar] [CrossRef]
- Spangler, L.; Cummings, P.; Tencer, A.F.; Mueller, B.A.; Mock, C. Biomechanical factors and failure of transcervical hip fracture repair. Injury 2001, 32, 223–228. [Google Scholar] [CrossRef]
- Zlowodzki, M.; Jönsson, A.; Paulke, R.; Kregor, P.J.; Bhandari, M. Shortening after femoral neck fracture fixation: Is there a solution? Clin. Orthop. Relat. Res. 2007, 461, 213–218. [Google Scholar] [CrossRef]
- Uhl, R.L. The biomechanics of screws. Orthop. Rev. 1989, 18, 1302–1307. [Google Scholar]
- Le Corroller, T.; Dediu, M.; Pauly, V.; Pirro, N.; Chabrand, P.; Champsaur, P. The femoral calcar: A computed tomography anatomical study. Clin. Anat. 2011, 24, 886–892. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time (Months) | t/F | p | ||
|---|---|---|---|---|
| Gender | Male (n = 78; 59.1%) | 3.2 ± 1.7 | 0.321 | 0.749 |
| Female (n = 54; 40.9%) | 3.3 ± 1.5 | |||
| Laterality | Left (n = 75; 56.8%) | 3.3 ± 1.7 | 0.618 | 0.538 |
| Right (n = 57; 43.2%) | 3.1 ± 1.4 | |||
| Initial displacement according to Wang et al. [18] | Type-I (n = 22; 16.7%) | 2.3 ± 1.2 | 4.960 | 0.008 * |
| Type-II (n = 74; 56.1%) | 3.3 ± 1.5 | |||
| Type-III (n = 36; 27.3%) | 3.5 ± 1.9 | |||
| Mechanism of injury | Ta (n = 52; 39.4%) | 3.2 ± 1.5 | 1.410 | 0.243 |
| Fa (n = 33; 25.0%) | 2.8 ± 1.2 | |||
| Sp (39; 29.5%) | 3.6 ± 2.0 | |||
| Ots (8; 6.1%) | 3.4 ± 1.7 | |||
| Type of fracture [15] | Delbet–Colonna I (n = 0; 0%) | - | 1.174 | 0.243 |
| Delbet–Colonna II (83; 62.9%) | 3.1 ± 1.8 | |||
| Delbet–Colonna III (n = 49; 37.1%) | 3.4 ± 1.3 | |||
| Delbet–Colonna IV (n = 0; 0%) | - | |||
| Medial or posterior cortex on AP or lateral radiographs | Comminuted (n = 24; 18.2%) | 3.8 ± 1.8 | 2.133 | 0.035 * |
| Without comminution (n = 108; 81.8%) | 3.1 ± 1.5 | |||
| Reduction method | CRIF (n = 79; 59.8%) | 3.2 ± 1.6 | 0.125 | 0.901 |
| ORIF (n = 53; 40.2%) | 3.2 ± 1.7 | |||
| Fixation method | Two cannulated screws (n = 100; 75.8%) | 3.1 ± 1.6 | 0.919 | 0.360 |
| Three cannulated screws (n = 32; 24.2%) | 3.4 ± 1.5 | |||
| Quality of reduction according to Song et al. [5] | Anatomical (n = 65; 49.2%) | 2.6 ± 1.2 | 12.098 | <0.001 * |
| Acceptable (n = 63; 47.7%) | 3.7 ± 1.7 | |||
| Unacceptable (n = 4; 3.0%) | 5.3 ± 2.4 | |||
| Fractures fixed by two cannulated screws | Fragments fully compressed (n = 72; 72%) | 3.0 ± 1.6 | 1.771 | 0.08 |
| Fragments partially compressed (n = 28; 28%) | 3.6 ± 1.6 |
| Coefficient | SE | Wald | p | RR | 95% of CI | |
|---|---|---|---|---|---|---|
| Initial displacement | −0.288 | 0.146 | 3.910 | 0.048 * | 0.750 | 0.564, 0.997 |
| Comminuted medial or posterior cortex on AP or lateral radiographs | −0.500 | 0.234 | 4.558 | 0.033 * | 0.607 | 0.383, 0.960 |
| Quality of reduction | −0.708 | 0.168 | 17.769 | <0.001 * | 0.493 | 0.355, 0.685 |
| Number of Screws Implanted | Time Needed to Achieve Fracture Healing (Months) | t | p | ||
|---|---|---|---|---|---|
| Initial displacement | Type I | 2 | 2.3 ± 1.2 | 0.871 | 0.394 |
| 3 | 1.6 ± 0.4 | ||||
| Type II | 2 | 3.2 ± 1.5 | 1.11 | 0.271 | |
| 3 | 3.6 ± 1.6 | ||||
| Type III | 2 | 3.6 ± 2.0 | 0.258 | 0.798 | |
| 3 | 3.4 ± 1.2 | ||||
| Medial or posterior cortex on AP or lateral radiographs | Comminuted | 2 | 3.9 ± 2.0 | 0.28 | 0.782 |
| 3 | 3.7 ± 1.4 | ||||
| Without comminution | 2 | 3.0 ± 1.5 | 0.928 | 0.356 | |
| 3 | 3.3 ± 1.6 | ||||
| Quality of reduction | Anatomical | 2 | 2.6 ± 1.2 | 0.534 | 0.596 |
| 3 | 2.8 ± 1.3 | ||||
| Non-anatomical | 2 | 3.8 ± 1.8 | 0.139 | 0.89 | |
| 3 | 3.8 ± 1.6 |
| Coefficient | SE | t | p | 95% CI | |
|---|---|---|---|---|---|
| Screw’s diameter (%) | 0.081 | 0.052 | 1.561 | 0.122 | −0.022, 0.184 |
| ASAP (°) | −0.047 | 0.041 | −1.140 | 0.257 | −0.129, 0.035 |
| ASL (°) | −0.021 | 0.035 | −0.605 | 0.547 | −0.090, 0.048 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, W.; Xiong, Z.; Zhao, C.; He, B.; Mei, H.; Li, Y.; Canavese, F.; Pan, Y.; Chen, S. Do the Number, Size, and Position of Partially Threaded Screws Affect the Radiological Healing of Surgically Treated Displaced Femoral Neck Fractures? A Review of 136 Children. Medicina 2022, 58, 1153. https://doi.org/10.3390/medicina58091153
Wang W, Xiong Z, Zhao C, He B, Mei H, Li Y, Canavese F, Pan Y, Chen S. Do the Number, Size, and Position of Partially Threaded Screws Affect the Radiological Healing of Surgically Treated Displaced Femoral Neck Fractures? A Review of 136 Children. Medicina. 2022; 58(9):1153. https://doi.org/10.3390/medicina58091153
Chicago/Turabian StyleWang, Wentao, Zhu Xiong, Chongzhi Zhao, Bo He, Haibo Mei, Yiqiang Li, Federico Canavese, Yuancheng Pan, and Shunyou Chen. 2022. "Do the Number, Size, and Position of Partially Threaded Screws Affect the Radiological Healing of Surgically Treated Displaced Femoral Neck Fractures? A Review of 136 Children" Medicina 58, no. 9: 1153. https://doi.org/10.3390/medicina58091153
APA StyleWang, W., Xiong, Z., Zhao, C., He, B., Mei, H., Li, Y., Canavese, F., Pan, Y., & Chen, S. (2022). Do the Number, Size, and Position of Partially Threaded Screws Affect the Radiological Healing of Surgically Treated Displaced Femoral Neck Fractures? A Review of 136 Children. Medicina, 58(9), 1153. https://doi.org/10.3390/medicina58091153