
Sacroiliac Screw Placement with Ease: CT-Guided Pelvic Fracture Osteosynthesis in the Elderly


Abstract
:1. Introduction
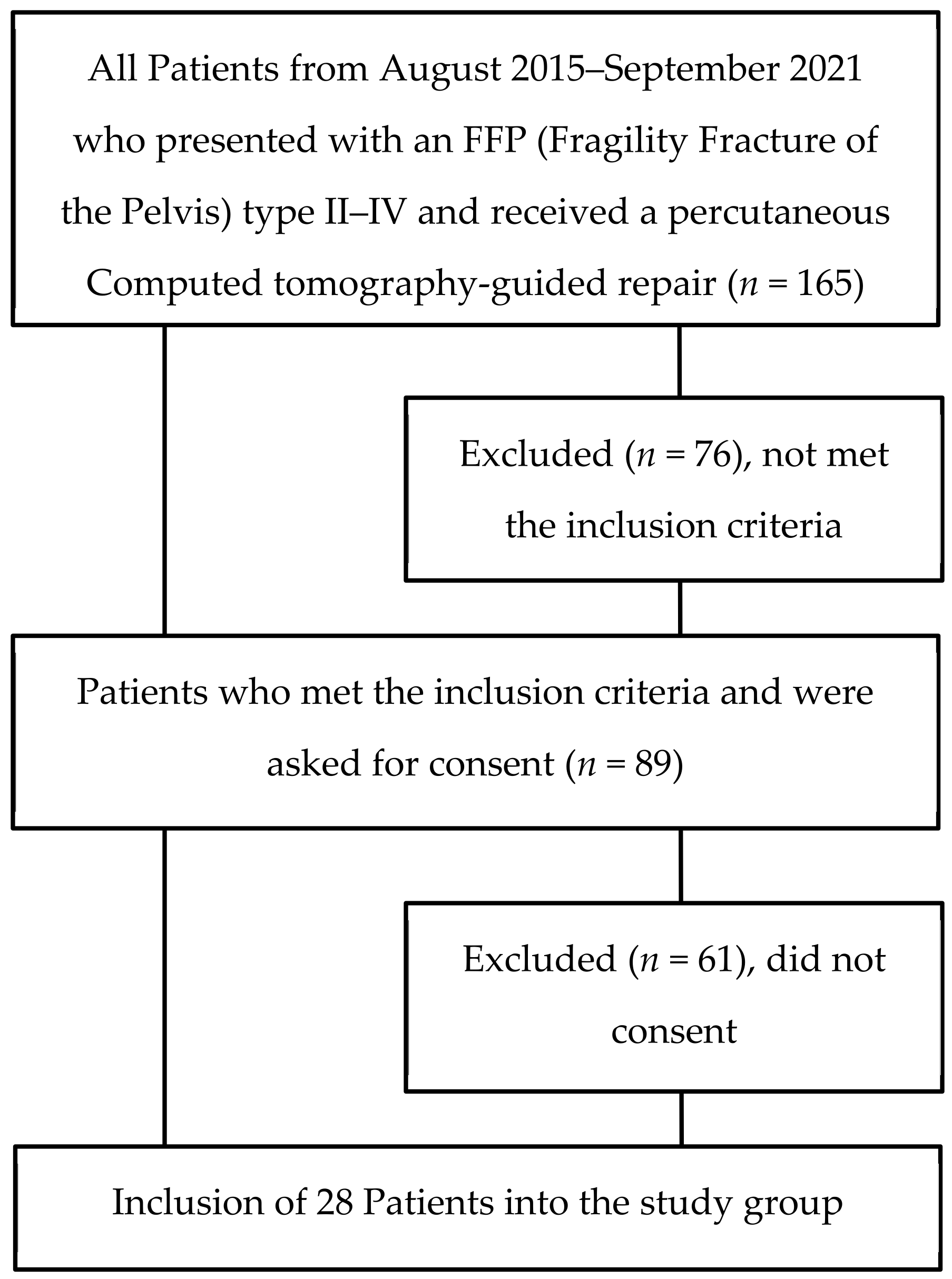
2. Materials and Methods
3. Results
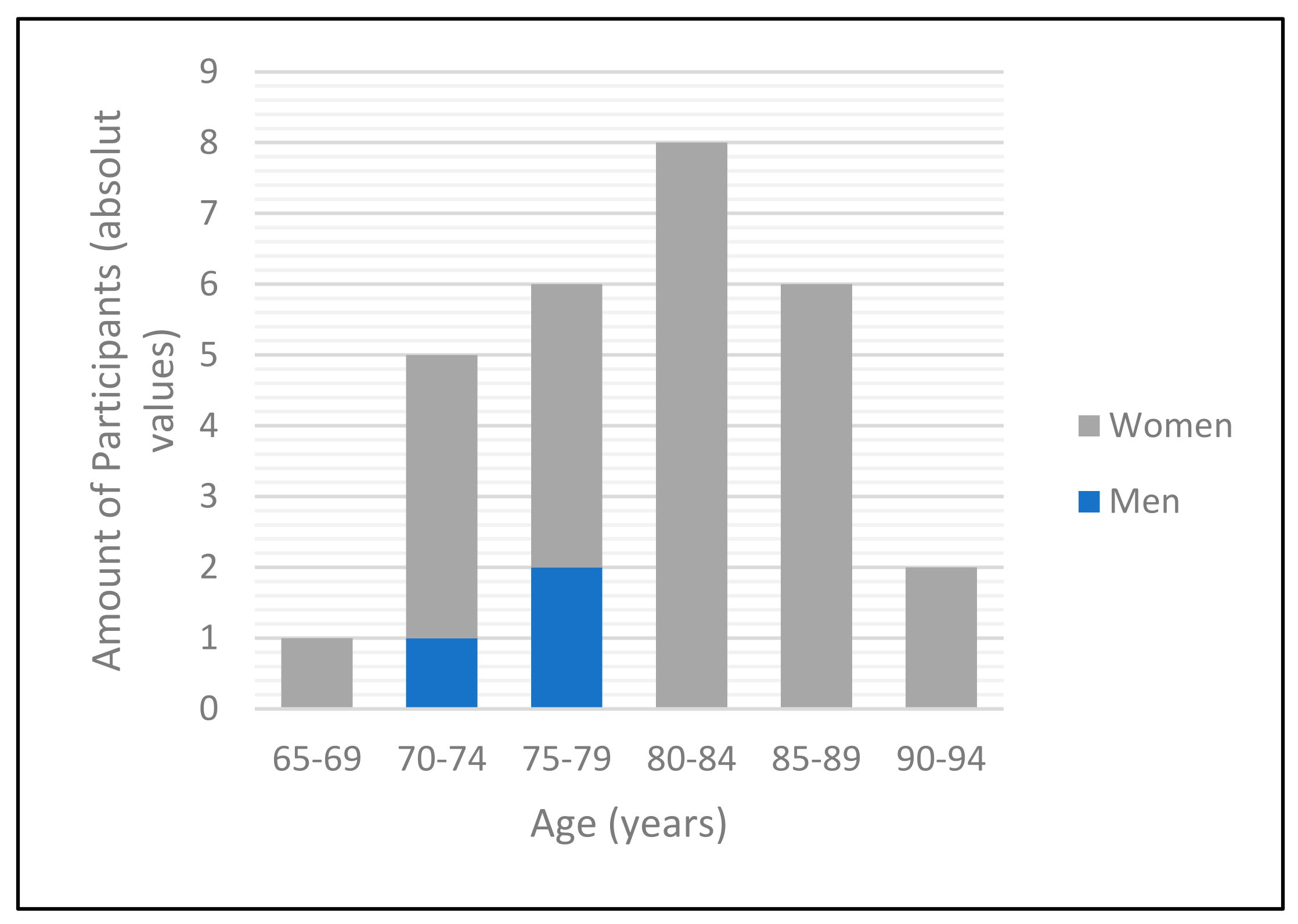
3.1. Demographics
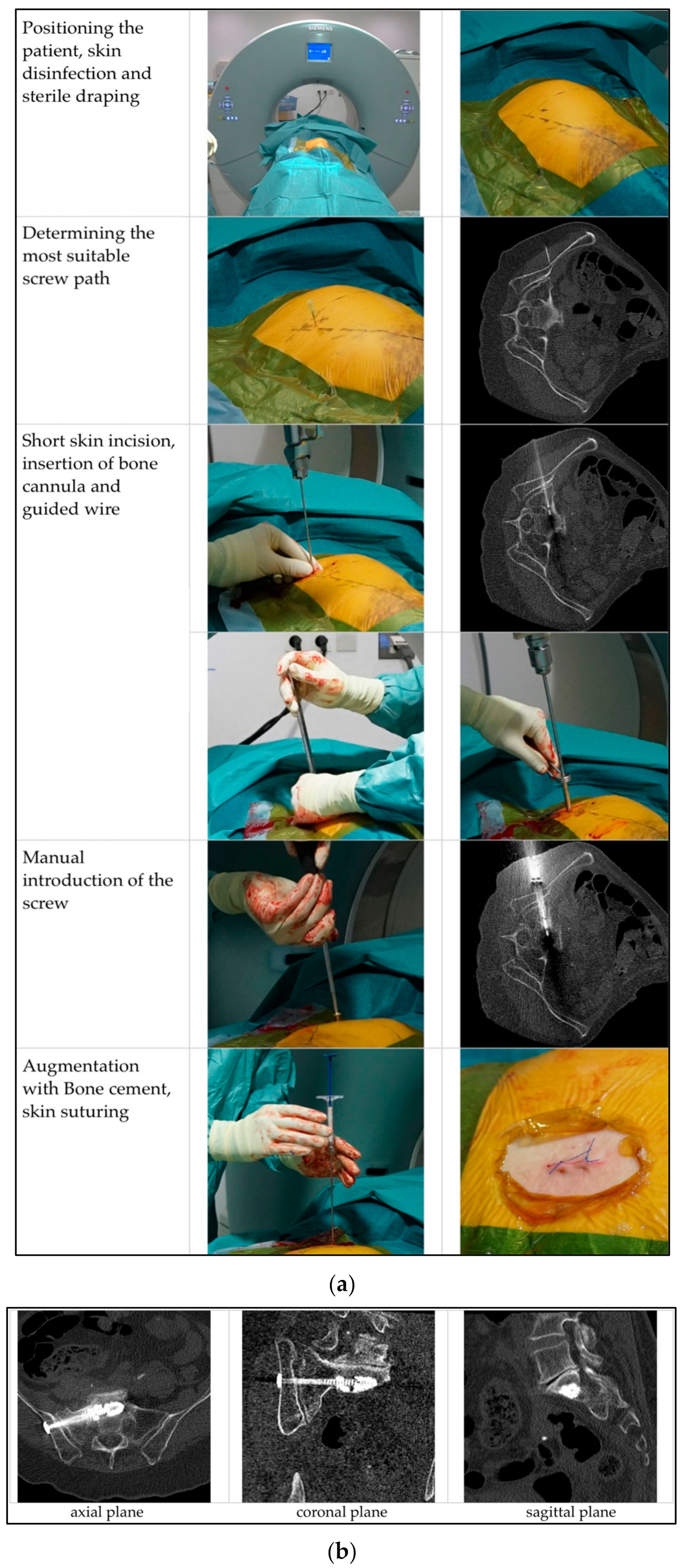
3.2. The Operative Procedure
3.3. Postoperative Course
3.4. Discharge
3.5. Outcome Measures
4. Discussion
4.1. Precision
4.2. Speed
4.3. Safety
4.4. Clinical Outcomes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andrich, S.; Haastert, B.; Neuhaus, E.; Neidert, K.; Arend, W.; Ohmann, C.; Grebe, J.; Vogt, A.; Jungbluth, P.; Rösler, G.; et al. Epidemiology of Pelvic Fractures in Germany: Considerably High Incidence Rates among Older People. PLoS ONE 2015, 10, e0139078. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T.; Rottbeck, U.; Hofbauer, V.; Raschke, M.; Stange, R. Beckenfrakturen im Alter. Die unterschätzte osteoporotische Fraktur. Unfallchirurg 2011, 114, 663. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.P.; Ahn, J. Epidemiology and Demographics. In Fragility Fractures of the Pelvis; Rommens, P.M., Hofmann, A., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 3–8. ISBN 978-3-319-66572-6. [Google Scholar]
- Frey, M.E.; DePalma, M.J.; Cifu, D.X.; Bhagia, S.M.; Carne, W.; Daitch, J.S. Percutaneous Sacroplasty for Osteoporotic Sacral Insufficiency Fractures: A Prospective, Multicenter, Observational Pilot Study. Spine J. 2008, 8, 367–373. [Google Scholar] [CrossRef] [PubMed]
- Rommens, P.M.; Hofmann, A. Personality of Fragility Fractures of the Pelvis. In Fragility Fractures of the Pelvis; Rommens, P.M., Hofmann, A., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 9–22. ISBN 978-3-319-66572-6. [Google Scholar]
- World Health Organization. Guidlines for Preclinical Evaluation and Clinical Trials in Osteoporosis; WHO: Geneva, Switzerland, 1998; ISBN 92-4-154522-4. [Google Scholar]
- Rommens, P.M.; Hofmann, A. Comprehensive Classification of Fragility Fractures of the Pelvic Ring: Recommendations for Surgical Treatment. Injury 2013, 44, 1733–1744. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.B. Preventing Secondary Complications in Trauma Patients with Implementation of a Multidisciplinary Mobilization Team. J. Trauma Nurs. Off. J. Soc. Trauma Nurses 2015, 22, 170–175, quiz E3-4. [Google Scholar] [CrossRef] [PubMed]
- Reuther, G.; Röhner, U.; Will, T.; Dehne, I.; Petereit, U. CT-Guided Screw Fixation of Vertical Sacral Fractures in Local Anaesthesia Using a Standard CT. RöFo - Fortschritte Auf Dem Geb. Röntgenstrahlen Bildgeb. Verfahr. 2014, 186, 1134–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richards, A.M.; Mears, S.C.; Knight, T.A.; Dinah, A.F.; Belkoff, S.M. Biomechanical Analysis of Sacroplasty: Does Volume or Location of Cement Matter? Am. J. Neuroradiol. 2009, 30, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Mehling, I.; Hessmann, M.H.; Rommens, P.M. Stabilization of Fatigue Fractures of the Dorsal Pelvis with a Trans-Sacral Bar. Operative Technique and Outcome. Injury 2012, 43, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Gänsslen, A.; Hüfner, T.; Krettek, C. Percutaneous Iliosacral Screw Fixation of Unstable Pelvic Injuries by Conventional Fluoroscopy. Oper. Orthopadie Traumatol. 2006, 18, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Wähnert, D.; Raschke, M.J.; Fuchs, T. Cement Augmentation of the Navigated Iliosacral Screw in the Treatment of Insufficiency Fractures of the Sacrum. A New Method Using Modified Implants. Int. Orthop. 2013, 37, 1147–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gras, F.; Marintschev, I.; Wilharm, A.; Klos, K.; Mückley, T.; Hofmann, G.O. 2D-Fluoroscopic Navigated Percutaneous Screw Fixation of Pelvic Ring Injuries—A Case Series. BMC Musculoskelet. Disord. 2010, 11, 153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konrad, G.; Zwingmann, J.; Kotter, E.; Südkamp, N.; Oberst, M. Variabilität Der Schraubenlage Bei 3D-Navigierter Sakrumverschraubung. Unfallchirurg 2010, 113, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Falzarano, G.; Rollo, G.; Bisaccia, M.; Pace, V.; Lanzetti, R.M.; Garcia-Prieto, E.; Pichierri, P.; Meccariello, L. Percutaneous Screws CT Guided to Fix Sacroiliac Joint in Tile C Pelvic Injury. Outcomes at 5 Years of Follow-Up. SICOT-J 2018, 4, 52. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Klaiberg, A.; Brähler, E.; König, H.-H. Der Lebensqualitätsfragebogen EQ-5D: Modelle Und Normwerte Für Die Allgemeinbevölkerung. Psychother. Psychosom. Med. Psychol. 2006, 56, 42–48. [Google Scholar] [CrossRef] [PubMed]
- EuroQol Group. EuroQol—A New Facility for the Measurement of Health-Related Quality of Life. Health Policy Amst. Neth. 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Rommens, P.; Ossendorf, C.; Pairon, P.; Dietz, S.-O.; Wagner, D.; Hofmann, A. Clinical Pathways for Fragility Fractures of the Pelvic Ring: Personal Experience and Review of the Literature. J. Orthop. Sci. Off. J. Jpn. Orthop. Assoc. 2014, 20, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, P.H.; Rahmanzadeh, T.; Gebhard, F.; Arand, M.; Weckback, S.; Kraus, M. Schraubenlage bei navigierter perkutaner Verschraubung des Sakroiliakalgelenks. Dtsch. Ärzte-Verl. 2012, 1, 292–297. [Google Scholar]
- Rommens, P.M.; Hofmann, A.; Kraemer, S.; Kisilak, M.; Boudissa, M.; Wagner, D. Operative Treatment of Fragility Fractures of the Pelvis: A Critical Analysis of 140 Patients. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Alpay, Y.; Aykin, N.; Korkmaz, P.; Gulduren, H.M.; Caglan, F.C. Urinary Tract Infections in the Geriatric Patients. Pak. J. Med. Sci. 2018, 34, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Janssen, M.F.; Szende, A.; Cabases, J.; Ramos-Goñi, J.M.; Vilagut, G.; König, H.H. Population Norms for the EQ-5D-3L: A Cross-Country Analysis of Population Surveys for 20 Countries. Eur. J. Health Econ. 2019, 20, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | 65–74 | 75–84 | 85–94 | Total | |
|---|---|---|---|---|---|
| Gender | Male | 1 (3.57%) | 2 (7.14%) | 0 (0.00%) | 3 (10.71%) |
| Female | 5 (17.86%) | 12 (42.86%) | 8 (28.57%) | 25 (89.29%) | |
| ASA 1 score | 1 | 0 | 0 | 0 | 0 (0.00%) |
| 2 | 1 | 6 | 1 | 8 (28.57%) | |
| 3 | 5 | 8 | 7 | 20 (71.42%) | |
| 4 | 0 | 0 | 0 | 0 (0.00%) | |
| 5 | 0 | 0 | 0 | 0 (0.00%) | |
| Comorbidities | Average number of comorbidities | 3.67 ± 1.51 | 3.07 ± 1.54 | 3.63 ± 1.51 | 3.57 ± 1.50 |
| art. hypertension | 3 | 13 | 7 | 23 (82.14%) | |
| chronic pain syndrome | 3 | 2 | 1 | 6 (21.42%) | |
| coronary heart disease | 1 | 2 | 6 | 9 (32.14%) | |
| diabetes mellitus | 2 | 1 | 1 | 4 (14.29%) | |
| obesity | 2 | 4 | 3 | 9 (32.14%) | |
| atrial fibrillation | 1 | 1 | 2 | 4 (14.29%) | |
| Others | 5 | 7 | 6 | 18 (64.29%) | |
| Fracture Type | FFP IIa 2 | 0 | 0 | 0 | 0 (0.00%) |
| FFP IIb 3 | 4 | 8 | 3 | 15 (53.47%) | |
| FFP IIc 4 | 0 | 0 | 0 | 0 (0.00%) | |
| FFP IIIa 5 | 0 | 1 | 1 | 2 (7.14%) | |
| FFP IIIb 6 | 0 | 1 | 1 | 2 (7.14%) | |
| FFP IIIc 7 | 0 | 0 | 2 | 2 (7.14%) | |
| FFP Iva 8 | 0 | 0 | 0 | 0 (0.00%) | |
| FFP IVb 9 | 0 | 1 | 1 | 2 (7.14%) | |
| FFP IVc 10 | 2 | 3 | 0 | 5 (17.86%) | |
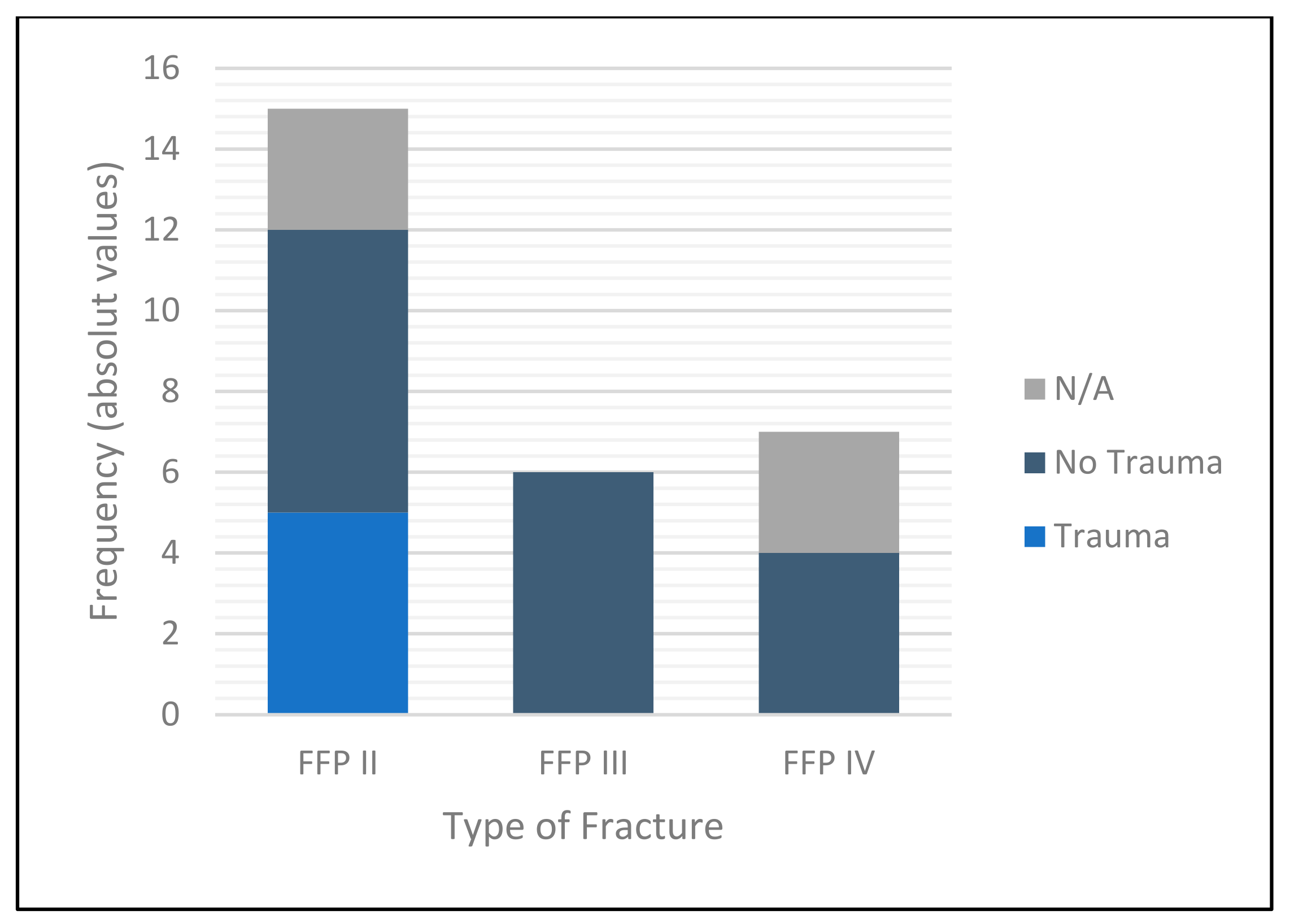
| Mechanism of Injury | Trauma | 2 | 3 | 0 | 5 (17.85%) |
| No Trauma | 3 | 6 | 8 | 17 (60.71%) | |
| Not classified | 1 | 5 | 0 | 6 (21.43%) |
| Surgeon | Number of Procedures | Average Time (min) | Radiation Exposure (mGy*cm) |
|---|---|---|---|
| Unilateral procedure | |||
| 1 | 5 | 40 | 558.14 |
| 3 | 14 | 30 | 264.72 |
| 4 | 2 | 30 | 236.60 |
| 5 | 0 | N/A 1 | N/A |
| Mean 32.38 ± 9.57 (p = 0.12) | Mean 265.17 ± 142.68 (p = 0.61) | ||
| Bilateral procedures | |||
| 1 | 2 | 40 | 379.00 |
| 2 | 1 | 55 | 780.00 |
| 3 | 2 | 45 | 267.54 |
| 4 | 1 | 75 | 287.00 |
| 5 | 1 | 55 | N/A |
| Mean 50.71 ± 17.42 | Mean 393.35 ± 201.30 | ||
| Distance (mm) to: | Posterior Cortex | Anterior Cortex | Caudal Cortex | Cranial Cortex | Neuroforamina |
|---|---|---|---|---|---|
| Average values (mm) | 10.14 ± 4.54 | 4.69 ± 3.77 | 11.75 ± 4.61 | 7.09 ± 4.61 | 4.33 ± 3.44 |
| Age | 65–74 | 75–84 | 85–94 | Total | |
|---|---|---|---|---|---|
| Total hospitalization (days) | Mean | 10.17 | 13.36 | 11.25 | 12.07 |
| Standard deviation | ±6.52 | ±4.24 | ±3.30 | ±4.59 | |
| Median | 8.00 | 13.00 | 12.00 | 12.00 | |
| IQR 1 | 5–16 | 11–16 | 9–14 | 9–15.5 | |
| p = 0.32 | |||||
| Postoperative hospitalization (days) | Mean | 5.83 | 6.71 | 3.00 | 5.21 |
| Standard deviation | ±2.73 | ±3.77 | ±2.00 | ±3.46 | |
| Median | 3.50 | 9.50 | 3.00 | 4.00 | |
| IQR | 3–7 | 4–10 | 1–4.5 | 3–7.5 | |
| p = 0.04 |
| Age | Unilateral Procedure | Bilateral Procedure | Total | |
|---|---|---|---|---|
| Total hospitalization (days) | Mean | 12.43 | 11.00 | 12.07 |
| Standard deviation | ±4.30 | ±5.60 | ±4.59 | |
| Median | 12.00 | 9.00 | 12.00 | |
| IQR | 9.5–15.5 | 7–16 | 9–15.5 | |
| p = 0.50 | ||||
| Postoperative hospitalization (days) | Mean | 10.17 | 13.36 | 5.21 |
| Standard deviation | ±6.52 | ±4.24 | ±3.46 | |
| Median | 8.00 | 13.00 | 4.00 | |
| IQR | 5–16 | 11–16 | 3–7.5 | |
| p = 0.50 |
| Time Interval Post-Surgery (Months) | 6 | 7–12 | 13–23 | 24–35 | 36–47 | 48–59 | >60 |
|---|---|---|---|---|---|---|---|
| Quantity (absolute values) | 1 | 3 | 6 | 1 | 1 | 2 | 3 |
| Mobility | 1.00 | 1.67 | 1.50 | 2.00 | 3.00 | 1.50 | 1.67 |
| Self-Care | 1.00 | 1.67 | 1.17 | 2.00 | 3.00 | 2.00 | 1.67 |
| Usual activities | 1.00 | 1.67 | 1.17 | 3.00 | 3.00 | 2.50 | 2.00 |
| Pain/Discomfort | 2.00 | 1.67 | 1.67 | 2.00 | 2.00 | 2.00 | 2.00 |
| Anxiety Depression | 1.00 | 2.00 | 1.67 | 1.00 | 3.00 | 2.00 | 1.67 |
| Visual Analogue Scale | 85.00 | 75.00 | 66.67 | 50.00 | 10.00 | 35.00 | 25.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kress, H.; Klein, R.; Pohlemann, T.; Wölfl, C.G. Sacroiliac Screw Placement with Ease: CT-Guided Pelvic Fracture Osteosynthesis in the Elderly. Medicina 2022, 58, 809. https://doi.org/10.3390/medicina58060809
Kress H, Klein R, Pohlemann T, Wölfl CG. Sacroiliac Screw Placement with Ease: CT-Guided Pelvic Fracture Osteosynthesis in the Elderly. Medicina. 2022; 58(6):809. https://doi.org/10.3390/medicina58060809
Chicago/Turabian StyleKress, Hannah, Roman Klein, Tim Pohlemann, and Christoph Georg Wölfl. 2022. "Sacroiliac Screw Placement with Ease: CT-Guided Pelvic Fracture Osteosynthesis in the Elderly" Medicina 58, no. 6: 809. https://doi.org/10.3390/medicina58060809
APA StyleKress, H., Klein, R., Pohlemann, T., & Wölfl, C. G. (2022). Sacroiliac Screw Placement with Ease: CT-Guided Pelvic Fracture Osteosynthesis in the Elderly. Medicina, 58(6), 809. https://doi.org/10.3390/medicina58060809