

The Role of Antibiotic Use in Third Molar Tooth Extractions: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
Review Rationale
2. Materials and Methods
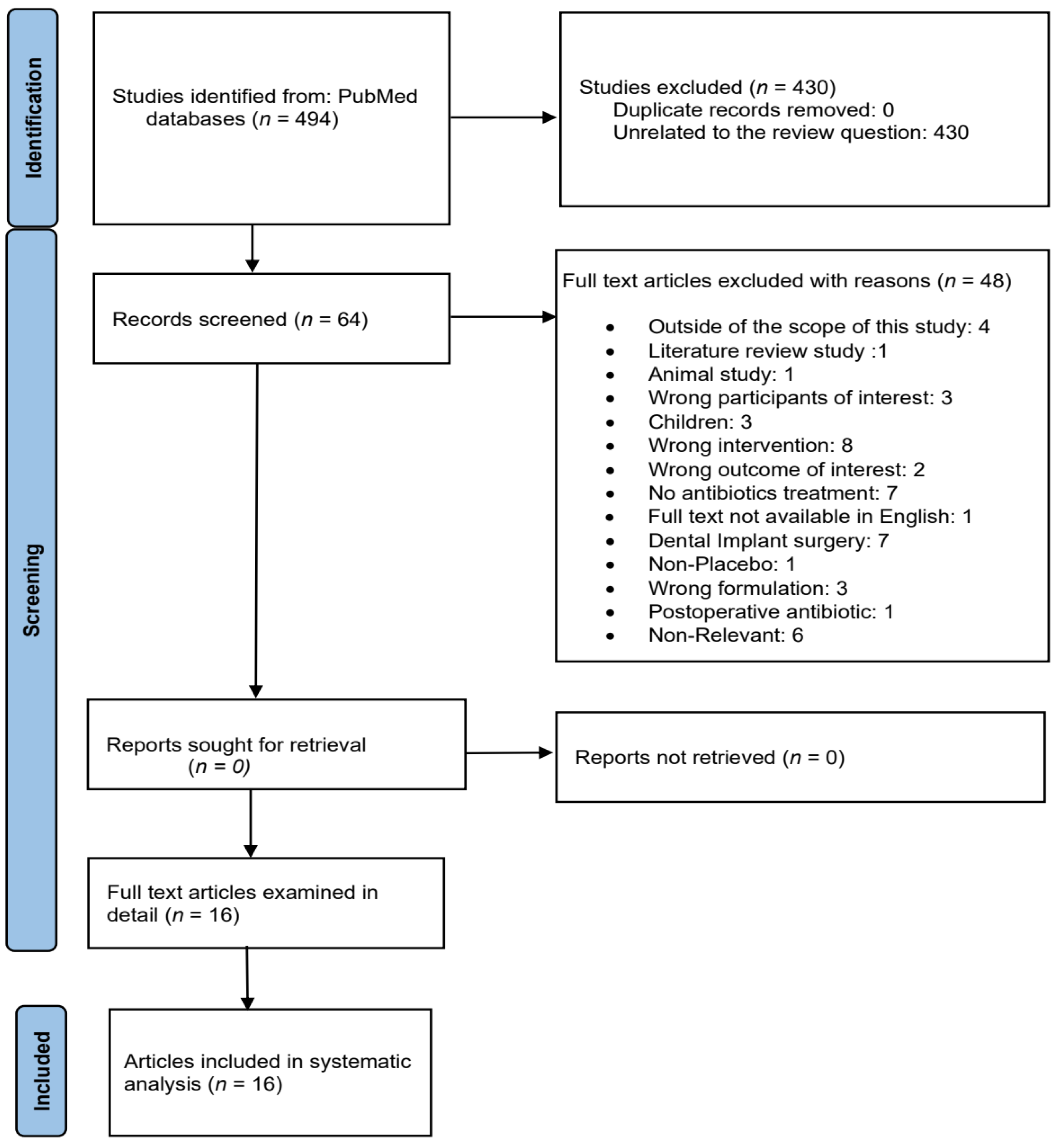
2.1. Search Strategy
- (P):
- Types of participants: Adult healthy patients of any age and gender undergoing uncomplicated single or multiple tooth extraction of any tooth.
- (I):
- Types of interventions: RCTs where oral ABs, independent of the type of ABs used, dose administered, timing of course administration (preoperatively, postoperatively, or both), number of doses administered, and length of the regimen.
- (C):
- Comparing all possible monotherapy AB treatment with either placebo or control or no treatment or no AB.
- (O):
- Type of outcome measures: Primary outcome of interest was postoperative infection. Secondary outcomes: other post-surgical related complications of infectious nature (e.g., alveolar or alveolitis osteitis or dry socket, pain, wound dehiscence, swelling, temperature), AB adverse events (e.g., gastric complications, stomach pain, diarrhoea, headache).
- (S):
- Primary care, community, or hospital setting.
2.2. Selection Criteria
- RCTs, double-blind and placebo-controlled clinical trial.
- Patients undergoing dental extraction.
- Only oral or systemic route of AB administration.
- Studies comparing the use of any AB (independent of the type of ABs used), dose administered, timing of course administration (preoperatively, postoperatively, or both), as part of treatment versus a placebo alone or control or no AB following M3 tooth extraction procedures.
- Adult over 17 years of age.
- Studies published from January 2000 to November 2021.
- Systematic and meta-analysis review or literature review study.
- Non-human or animal study.
- Published in language other than English, where full translated version could not be supplied by the publisher or the author/s.
- Abstracts and conference proceedings.
- Trials which are comparing AB versus non-AB agent/s.
- Unhealthy patients or patients with comorbidities which put them at high risk of infection.
- Trials comparing AB versus another AB/s without a placebo arm.
- Wrong formulation (injections/gels).
2.3. Selected Studies Summary
3. Results
3.1. Statistical Analysis
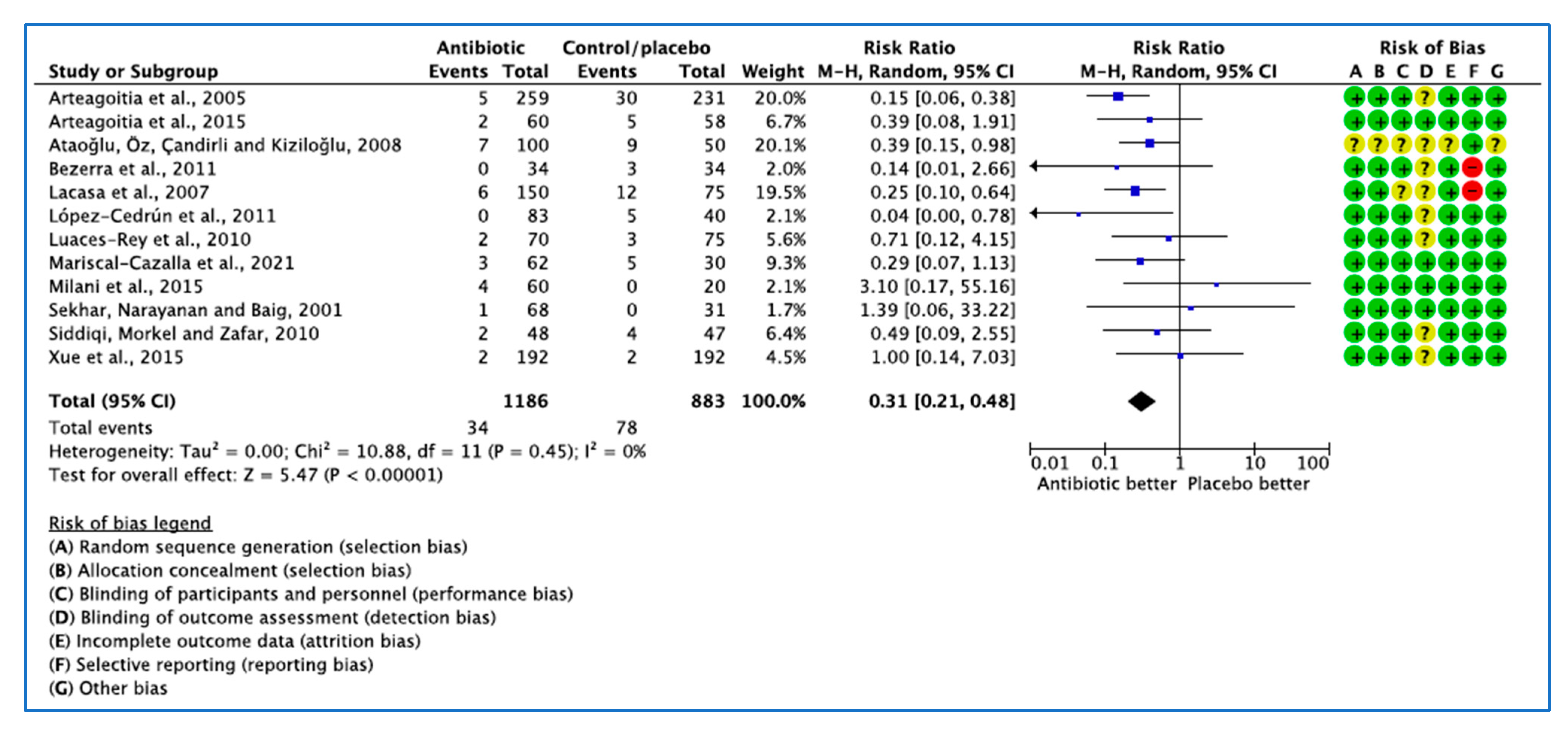
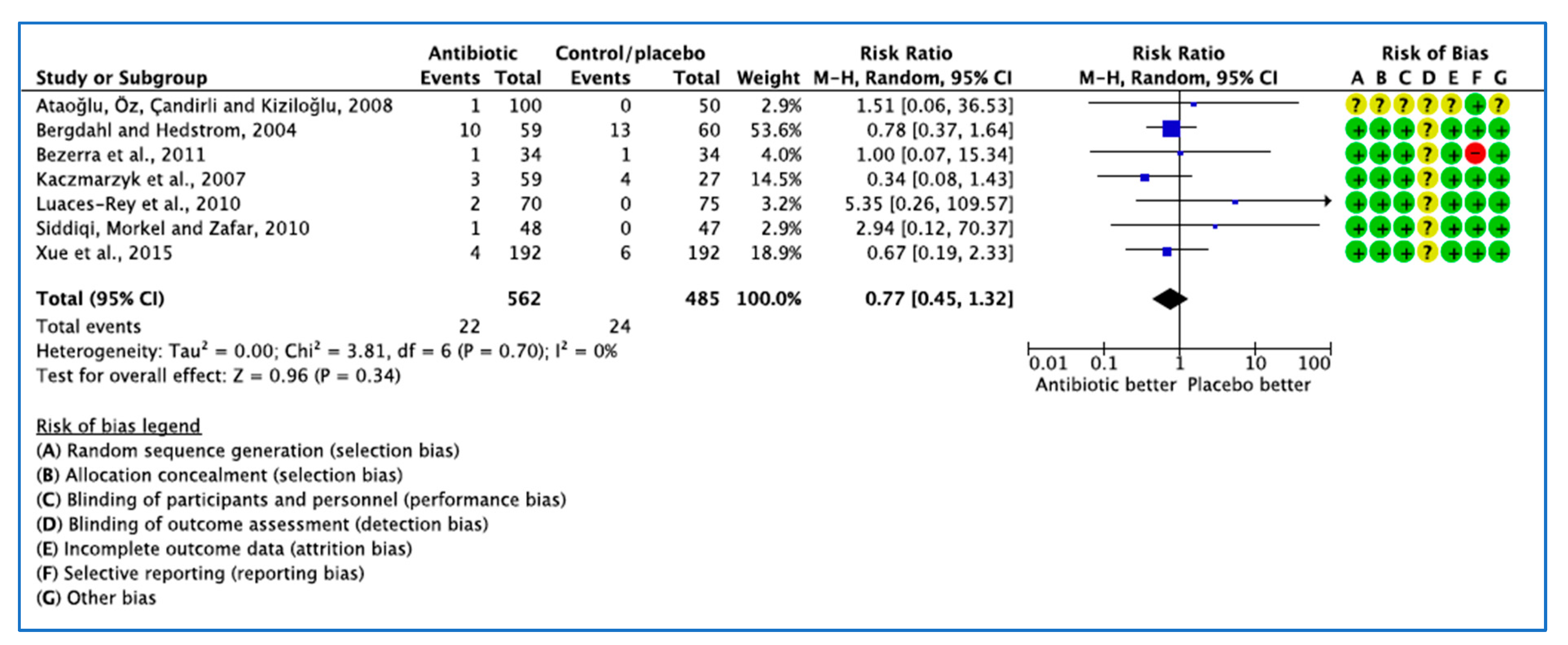
3.1.1. Analysis of Clinical Trials with Infection as the Outcome Measure
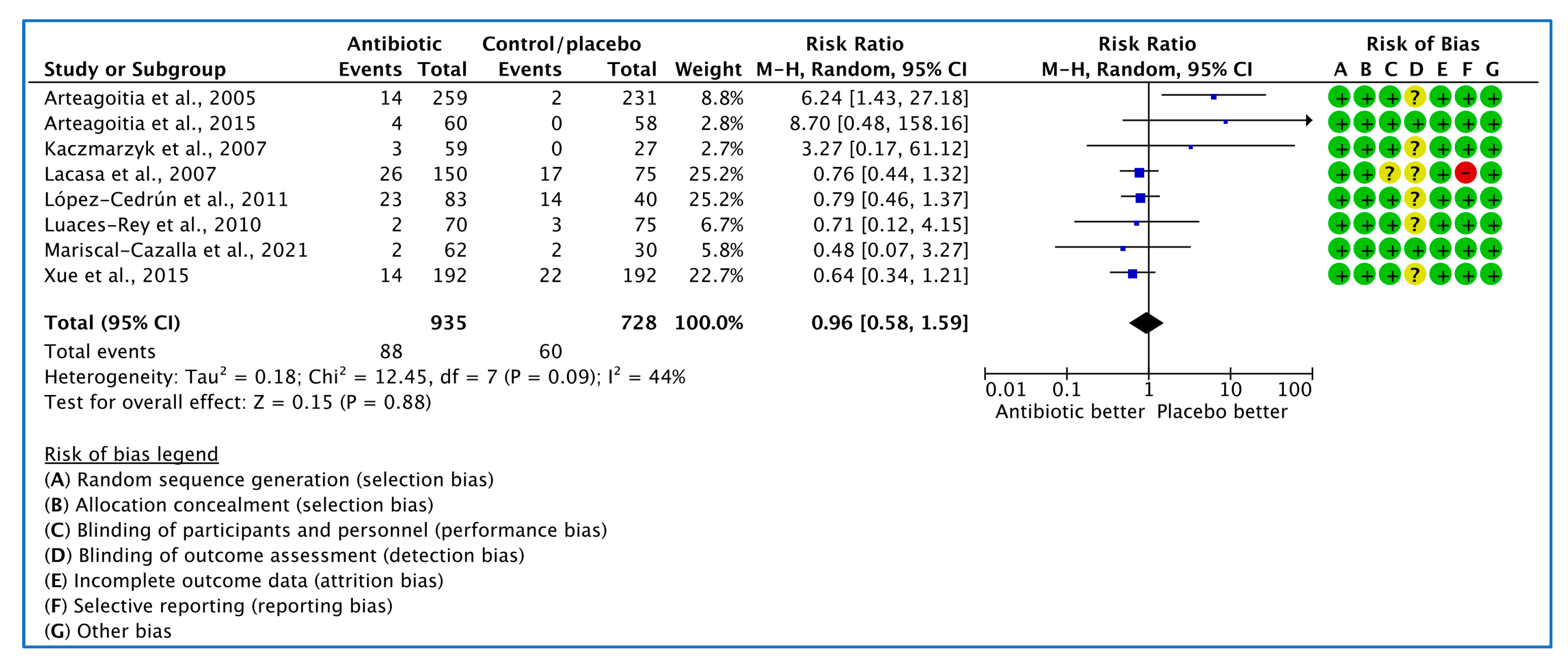
3.1.2. Analysis of Clinical Trials with Dry Socket or Alveolar Osteitis or Alveolitis as the Outcome Measure
3.1.3. Analysis of Clinical Trials with Medication Related Adverse Events as the Outcome Measure
3.2. Narrative Analysis of other Outcomes
3.2.1. Increased the Risk of Infections
3.2.2. Antibiotic Related Adverse Events
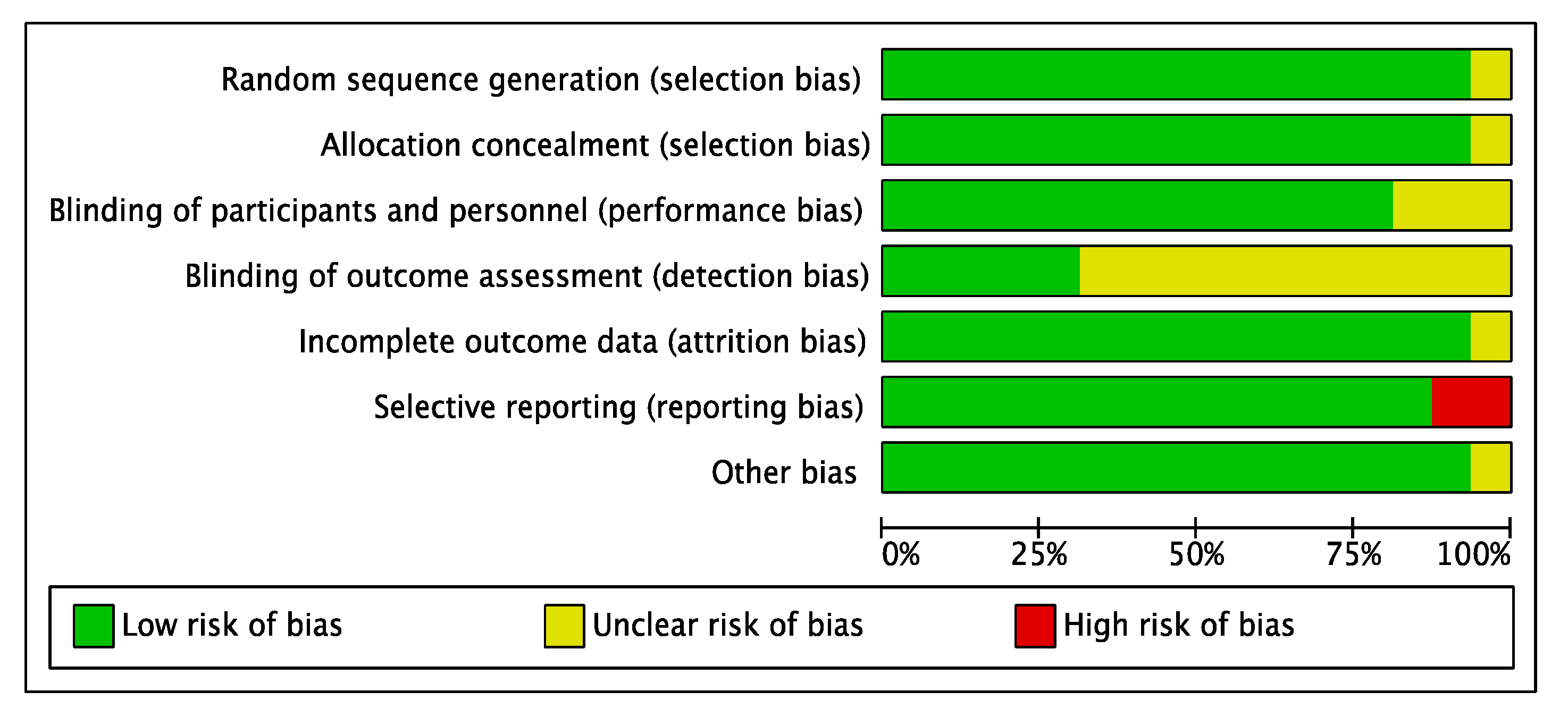
3.3. Risk of Bias
3.4. Number Needed to Treat
- 1.
- To prevent infection events
- 2.
- To prevent dry socket events
- 3.
- To cause adverse events
3.5. Limitations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ahlqwist, M.; Gröndahl, H.G. Prevalence of impacted teeth and associated pathology in middle-aged and older Swedish women. Community Dent. Oral Epidemiol. 1991, 19, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Chen, X.; Zhou, Z.; Hao, Y.; Li, H.; Cheng, Y.; Ren, X.; Wang, X. Effects of Impacted Lower Third Molar Extraction on Periodontal Tissue of the Adjacent Second Molar. Ther. Clin. Risk Manag. 2021, 17, 235–247. [Google Scholar] [CrossRef] [PubMed]
- Doğan, N.; Orhan, K.; Günaydin, Y.; Köymen, R.; Okçu, K.; Uçok, O. Unerupted mandibular third molars: Symptoms, associated pathologies, and indications for removal in a Turkish population. Quintessence Int. 2007, 38, e497–e505. [Google Scholar] [PubMed]
- Renton, T.; Al-Haboubi, M.; Pau, A.; Shepherd, J.; Gallagher, J.E. What has been the United Kingdom’s experience with retention of third molars? J. Oral Maxillofac. Surg. 2012, 70, S48–S57. [Google Scholar] [CrossRef] [PubMed]
- Akarslan, Z.Z.; Kocabay, C. Assessment of the associated symptoms, pathologies, positions and angulations of bilateral occurring mandibular third molars: Is there any similarity? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 108, e26–e32. [Google Scholar] [CrossRef] [PubMed]
- NICE UK. Guidance on the Extraction of Wisdom Teeth. Technology Appraisal TA1. Available online: https://www.nice.org.uk/guidance/ta1 (accessed on 28 January 2022).
- Sayed, N.; Bakathir, A.; Pasha, M.; Al-Sudairy, S. Complications of Third Molar Extraction: A retrospective study from a tertiary healthcare centre in Oman. Sultan Qaboos Univ. Med. J. 2019, 19, e230–e235. [Google Scholar] [CrossRef] [PubMed]
- Mobilio, N.; Vecchiatini, R.; Vasquez, M.; Calura, G.; Catapano, S. Effect of flap design and duration of surgery on acute postoperative symptoms and signs after extraction of lower third molars: A randomized prospective study. J. Dent. Res. Dent. Clin. Dent. Prospect. 2017, 11, 156–160. [Google Scholar] [CrossRef]
- Jaroń, A.; Trybek, G. The Pattern of Mandibular Third Molar Impaction and Assessment of Surgery Difficulty: A Retrospective Study of Radiographs in East Baltic Population. Int. J. Environ. Res. Public Health 2021, 18, 6016. [Google Scholar] [CrossRef]
- Pigott, J.P. Principles of Exodontia as Applied to the Impacted Mandibular Third Molar. Yale J. Biol. Med. 1928, 1, 63. [Google Scholar]
- Jerjes, W.; Upile, T.; Nhembe, F.; Gudka, D.; Shah, P.; Abbas, S.; McCarthy, E.; Patel, S.; Mahil, J.; Hopper, C. Experience in third molar surgery: An update. Br. Dent. J. 2010, 209, E1. [Google Scholar] [CrossRef]
- Jerjes, W.; Swinson, B.; Banu, B.; Al Khawalde, M.; Hopper, C. Paraesthesia of the lip and chin area resolved by endodontic treatment: A case report and review of literature. Br. Dent. J. 2005, 198, 743–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dewhirst, F.E.; Chen, T.; Izard, J.; Paster, B.J.; Tanner, A.C.; Yu, W.H.; Lakshmanan, A.; Wade, W.G. The human oral microbiome. J. Bacteriol. 2010, 192, 5002–5017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuriyama, T.; Karasawa, T.; Nakagawa, K.; Yamamoto, E.; Nakamura, S. Bacteriology and antimicrobial susceptibility of gram-positive cocci isolated from pus specimens of orofacial odontogenic infections. Oral Microbiol. Immunol. 2002, 17, 132–135. [Google Scholar] [CrossRef]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.G. Identifying and measuring heterogeneity across the studies in meta-analysis. J. Hand Surg. Am. 2013, 38, 1449–1450. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G. Chapter 10: Analysing data and undertaking meta-analyses. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.3; Higgins, J.P., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane Collaboration: London, UK, 2022. [Google Scholar]
- Thomas, B.H.; Ciliska, D.; Dobbins, M.; Micucci, S. A process for systematically reviewing the literature: Providing the research evidence for public health nursing interventions. Worldviews Evid. Based Nurs. 2004, 1, 176–184. [Google Scholar] [CrossRef]
- Diz Dios, P.; Tomás Carmona, I.; Limeres Posse, J.; Medina Henríquez, J.; Fernández Feijoo, J.; Alvarez Fernández, M. Comparative efficacies of amoxicillin, clindamycin, and moxifloxacin in prevention of bacteremia following dental extractions. Antimicrob. Agents Chemother. 2006, 50, 2996–3002. [Google Scholar] [CrossRef] [Green Version]
- Rabi, A.; Maheshwari, R.; Srinivasan, B.; Warad, L.P.; Suvarna, C.C.; Tank, K.S. Effectiveness of Antimicrobial Therapy after Extraction of Impacted Mandibular Third Molar: A Randomized Clinical Trial. J. Contemp. Dent. Pract. 2018, 19, 81–85. [Google Scholar] [CrossRef]
- Milani, B.A.; Bauer, H.C.; Sampaio-Filho, H.; Horliana, A.C.; Perez, F.E.; Tortamano, I.P.; Jorge, W.A. Antibiotic therapy in fully impacted lower third molar surgery: Randomized three-arm, double-blind, controlled trial. Oral Maxillofac. Surg. 2015, 19, 341–346. [Google Scholar] [CrossRef]
- Sekhar, C.H.; Narayanan, V.; Baig, M.F. Role of antimicrobials in third molar surgery: Prospective, double blind, randomized, placebo-controlled clinical study. Br. J. Oral Maxillofac. Surg. 2001, 39, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Morkel, J.A.; Zafar, S. Antibiotic prophylaxis in third molar surgery: A randomized double-blind placebo-controlled clinical trial using split-mouth technique. Int. J. Oral Maxillofac. Surg. 2010, 39, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Bezerra, T.P.; Studart-Soares, E.C.; Scaparo, H.C.; Pita-Neto, I.C.; Batista, S.H.; Fonteles, C.S. Prophylaxis versus placebo treatment for infective and inflammatory complications of surgical third molar removal: A split-mouth, double-blind, controlled, clinical trial with amoxicillin (500 mg). J. Oral Maxillofac. Surg. 2011, 69, e333–e339. [Google Scholar] [CrossRef]
- Kaczmarzyk, T.; Wichlinski, J.; Stypulkowska, J.; Zaleska, M.; Panas, M.; Woron, J. Single-dose and multi-dose clindamycin therapy fails to demonstrate efficacy in preventing infectious and inflammatory complications in third molar surgery. Int. J. Oral Maxillofac. Surg. 2007, 36, 417–422. [Google Scholar] [CrossRef]
- Xue, P.; Wang, J.; Wu, B.; Ma, Y.; Wu, F.; Hou, R. Efficacy of antibiotic prophylaxis on postoperative inflammatory complications in Chinese patients having impacted mandibular third molars removed: A split-mouth, double-blind, self-controlled, clinical trial. Br. J. Oral Maxillofac. Surg. 2015, 53, 416–420. [Google Scholar] [CrossRef]
- Luaces-Rey, R.; Arenaz-Búa, J.; Lopez-Cedrun-Cembranos, J.L.; Martínez-Roca, C.; Pértega-Díaz, S.; Sironvalle-Soliva, S. Efficacy and safety comparison of two amoxicillin administration schedules after third molar removal. A randomized, double-blind and controlled clinical trial. Med. Oral Patol. Oral Cir. Bucal. 2010, 15, e633–e638. [Google Scholar] [CrossRef] [Green Version]
- Arteagoitia, I.; Ramos, E.; Santamaria, G.; Barbier, L.; Alvarez, J.; Santamaria, J. Amoxicillin/clavulanic acid 2000/125 mg to prevent complications due to infection following completely bone-impacted lower third molar removal: A clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 119, 8–16. [Google Scholar] [CrossRef]
- López-Cedrún, J.L.; Pijoan, J.I.; Fernández, S.; Santamaria, J.; Hernandez, G. Efficacy of amoxicillin treatment in preventing postoperative complications in patients undergoing third molar surgery: A prospective, randomized, double-blind controlled study. J. Oral Maxillofac. Surg. 2011, 69, e5–e14. [Google Scholar] [CrossRef]
- Mariscal-Cazalla, M.D.M.; Manzano-Moreno, F.J.; García-Vázquez, M.; Vallecillo-Capilla, M.F.; Olmedo-Gaya, M.V. Do perioperative antibiotics reduce complications of mandibular third molar removal? A double-blind randomized controlled clinical trial. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2021, 131, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Ataoğlu, H.; Oz, G.Y.; Candirli, C.; Kiziloğlu, D. Routine antibiotic prophylaxis is not necessary during operations to remove third molars. Br. J. Oral Maxillofac. Surg. 2008, 46, 133–135. [Google Scholar] [CrossRef] [PubMed]
- Bergdahl, M.; Hedström, L. Metronidazole for the prevention of dry socket after removal of partially impacted mandibular third molar: A randomised controlled trial. Br. J. Oral Maxillofac. Surg. 2004, 42, 555–558. [Google Scholar] [CrossRef] [PubMed]
- Arteagoitia, I.; Diez, A.; Barbier, L.; Santamaría, G.; Santamaría, J. Efficacy of amoxicillin/clavulanic acid in preventing infectious and inflammatory complications following impacted mandibular third molar extraction. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2005, 100, e11–e18. [Google Scholar] [CrossRef] [PubMed]
- Lacasa, J.M.; Jiménez, J.A.; Ferrás, V.; Bossom, M.; Sóla-Morales, O.; García-Rey, C.; Aguilar, L.; Garau, J. Prophylaxis versus pre-emptive treatment for infective and inflammatory complications of surgical third molar removal: A randomized, double-blind, placebo-controlled, clinical trial with sustained release amoxicillin/clavulanic acid (1000/62.5 mg). Int. J. Oral Maxillofac. Surg. 2007, 36, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, I. Assessment of patient-reported outcomes in clinical trials: The example of health-related quality of life. Fundam. Clin. Pharmacol. 2004, 18, 351–363. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Lodi, G.; Azzi, L.; Varoni, E.M.; Pentenero, M.; Del Fabbro, M.; Carrassi, A.; Sardella, A.; Manfredi, M. Antibiotics to prevent complications following tooth extractions. Cochrane Database Syst. Rev. 2021, 2, Cd003811. [Google Scholar] [CrossRef]
- Ren, Y.-F.; Malmstrom, H.S. Effectiveness of Antibiotic Prophylaxis in Third Molar Surgery: A Meta-Analysis of Randomized Controlled Clinical Trials. J. Oral. Maxillofac. Surg. 2007, 65, 1909–1921. [Google Scholar] [CrossRef]
- FoPH, UK. Numbers Needed to Treat (NNT)—Calculation, Interpretation, Advantages and Disadvantages. Faculty of Public Health: London, UK. Available online: https://www.healthknowledge.org.uk/public-health-textbook/research-methods/1a-epidemiology/nnts (accessed on 21 January 2023).
- CEBM, UK. Number Needed to Treat. Centre for Evidence-Based Medicine: London, UK. Available online: https://www.cebm.ox.ac.uk/resources/ebm-tools/number-needed-to-treat-nnt (accessed on 23 January 2023).
- Ramos, E.; Santamaría, J.; Santamaría, G.; Barbier, L.; Arteagoitia, I. Do systemic antibiotics prevent dry socket and infection after third molar extraction? A systematic review and meta-analysis. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2016, 122, 403–425. [Google Scholar] [CrossRef]
- Singh Gill, A.; Morrissey, H.; Rahman, A. A Systematic Review and Meta-Analysis Evaluating Antibiotic Prophylaxis in Dental Implants and Extraction Procedures. Medicina 2018, 54, 95. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citation | Design | Sample Age Gender | Study Objectives | Antibiotic | Control | Antibiotic Dosing | Mouthwash Use | Inflammation and Pain Relief | Extraction Reason | Follow Up | Study Period |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Milani et al., 2015 [22] Europe | Double-blind RCT | n = 80 18–30 years. F: 54 M: 26 | Evaluate the presence of mouth opening (trismus) in postoperative period | 1 g amoxicillin + 500 mg 8 hourly for 7 days 1 g amoxicillin + placebo 8 hourly for 7 days | Placebo 1 h before surgery and 500 mg 8 hourly for 7 days. | 1 h before surgery | N/R | Postoperative: For sever pain: 30 mg codeine + paracetamol 6 hourly as required/For less severe pain Metamizole + Adiphenine + Promethazine | Extraction of fully impacted lower 3Ms | 7 days | Jan 2011–Jan 2012 |
| Mariscal-Cazalla et al., 2021 [31] Europe | Double-blind RCT | n = 92 18 to 63 years. F: 55 M: 37 | Evaluate the effectiveness of antibiotic therapy against possible complications (pain, inflammation, infection) of impacted mandibular third molar extraction | G1: (pre+ post antibiotic): 750 mg amoxicillin every 8 h for 2 days before surgery + for 5 days after surgery G2: (post antibiotic): 750 mg oral amoxicillin every 8 h for 5 days after surgery | Methylcellulose Tab for 2 days before surgery + for 5 days after surgery | 2 days before surgery | Preoperative: Chlorhexidine mouthwash for 2 min Postoperative: Chlorhexidine mouthwash after brushing for 1 week after surgery for 7 days | Postoperative: Ibuprofen 600 mg 8 hourly for 2 days after surgery; If not adequate: 1 g paracetamol | Extraction of impacted lower 3Ms | 7 days | Jan 2018–Dec 2018 |
| Lacasa et al., 2007 [35] South Africa | Double-blind RCT, Parallel group phase III | n = 225 ≥18 years. M: 96 F: 129 | Evaluate the efficacy of two SR antibiotic regimens in the reduction of infection after third molar extractive surgery | Prophylaxis G: 2 single dose Amoxicillin/clavulanate 1000/62.5 mg tab before surgery+ two placebo 2000/125 mg, twice daily for 5 days Pre-emptive G: 2 single dose placebos before surgery + 2 amoxicillin/clavulanate 1000/62.5 mg for 5 days | 2 Placebo 1000/62.5 mg single dose before surgery + two placebo 1000/62.5 mg twice daily for 5 days. | N/R | N/R | Postoperative: Metamizol cap one every 8 h, for a minimum of 48 h | Extraction of 3Ms surgery | days 1, 3, and 7 or/and 15 (decided on day 7) | Jan 2022–Dec 2002 |
| Sekhar, Narayanan, and Baig, 2001 [23] India | Double-blind RCT | n = 99 19–36 years. F: 44 M: 55 | Are prophylactic Ab necessary following the removal of 3Ms, and if so, when and what dose should be given, and for how long? | Metronidazole 400 mg every 8 hourly for 5 days or metronidazole 400 mg orally 8 hourly for five days postoperative | Placebo | 1 h before surgery | N/R | Postoperative: Ibuprofen 400 mg tablets as required | Extraction of 3Ms surgery | 5 days | N/R |
| Ataoğlu, Öz, Çandirli, and Kiziloğlu, 2008 [32] Turkey | N/R | n = 150 Mean of 20 years. F: 124 M: 26 | Evaluate the efficacy of Ab prophylaxis during removal of impacted 3Ms | G1: Amoxicillin/clavulanic acid 1 g twice daily after surgery for 5 days G2: Amoxicillin/clavulanic acid 1 g for 5 days before operation | no prophylaxis given | 5 days before surgery | Preoperative rinsed with chlorhexidine mouthwash for 1 min Postoperative: chlorhexidine gluconate mouth rinse twice a day for 5 days | Postoperative: Naproxen sodium 275 mg twice a day for 5 days | Extraction of 3Ms surgery | 7 days | Mar 2001–Feb 2003. |
| Arteagoitia et al., 2015 [29] Europe | Double-blind RCT | n = 118 ≥18 years. F: 60 M: 58 | Assessing the efficacy of antibiotic for extraction of bone impacted lower 3Ms | Two Amoxicillin/clavulanic acid 1000/62.5 mg tablet 2 h before surgery and every 12 h for 4 days. | Two placebo 1000/62.5 mg tablets every 12 h for 4 days | 2 h before surgery | Postoperative chlorhexidine mouthwash | Postoperative: Ibuprofen 600 mg, one sachet 8 hourly as required | Extraction of bone impacted lower 3Ms for any indication | Until week 8 after surgery | Feb 2010–June 2013 |
| Siddiqi, Morkel, and Zafar, 2010 [24] South Africa | Double-blind RCT split-mouth technique | n = 95 Mean of 26 years. F: 62 M: 33 | Evaluate the potential value of prophylactic antibiotic in 3Ms surgery | GI: 1st visit: Amoxicillin 1 g, 1 h before surgery, 2nd visit: placebo or vice versa. | GII: 1st visit: Amoxicillin 1 g, 1 h before surgery + 500 mg amoxicillin every 8 hourly for 2 days, 2nd visit: placebo or vice versa. | 1 h before surgery | Preoperative: chlorhexidine mouthwash Postoperative: chlorhexidine mouthwash 8 hourly for 3 days | Preoperative: Ibuprofen 400 mg Postoperative Ibuprofen 400 mg 6 hourly for 2 days) and paracetamol 500 mg + codeine phosphate 8 mg 6 hourly for 2 days | Extraction of unilateral/contralateral 3Ms surgery | on days 3, 7, and 14 after surgery. | N/R |
| Bezerra et al., 2011 [25] Brazil | Double-blind RCT | n = 34 18–35 years. F: 23 M: 11 | Evaluated the effect of prophylactic dosing of antibiotic on the control of postoperative inflammatory/infectious events associated with 3Ms extraction | Two 500 mg amoxicillin Cap | Placebo consisted of 2 capsules (500 mg of starch) each, orally 1 h before the procedure | 1 h before surgery | N/R | Postoperative: Nimesulid 100 mg every 12 h for 4 days + dipyrone 500 mg every 6 h for 2 days. | Extraction of all 4 3Ms | after 3, 7, and 14 days | Jan 2008–Nov 2008 |
| Kaczmarzyk et al., 2007 [26] Europe | Double-blind RCT | n = 86 18–60 years. F:63 M: 23 | Test the hypotheses that (1) administration of a single dose of 600 mg clindamycin 60 min prior to the surgical extraction of a retained lower 3Ms effectively prevents postoperative inflammation compared to placebo, (2) single dose of 600 mg clindamycin prior to surgical extraction of a retained 3Ms with a subsequent 5-day course of 300 mg clindamycin 8 hourly effectively prevents postoperative inflammation compared to placebo | Single-dose group: 600 mg clindamycin hydrochloride 60 min preoperatively, followed by 300 mg placebo every 8 hourly for 5 days. | 5-day group: 600 mg clindamycin orally 60 min preoperatively, followed by of 300 mg clindamycin 8 hourly for 5 days. | 1 h before surgery | N/R | Postoperative: Ketoprofen in 50 mg cap (Max 200 mg daily). | Extraction of a retained lower 3Ms, (due to orthodontic reasons that required bone removal) | on days 1, 2, and 7 post-operative | Jan 2005–Apr 2006 |
| Xue et al., 2015 [27] China | Double-blind RCT | n = 192 18–60 years. F: 118 M: 74 | 1. To identify whether antibiotics have effect on postoperative inflammatory complications after extraction of impacted mandibular 3Ms in Chinese patients 2. Which antibiotics could be used to prevent and reduce the incidence of postoperative inflammatory complications? 3. When should we give the antibiotic so that it reduces the incidence of postoperative inflammatory complications? | Amoxicillin 0.5 g 1 h preoperatively, or if allergic clindamycin hydrochloride 0.3 g, followed by Amoxicillin 0.5 g, 3 times a day postoperative for 3 days | Placebo 0.5 g (1 h preoperative followed by placebo 0.5 g 3 times a day for 3 days post-operative | 1 h before surgery | N/R | Pre and postoperative: Loxoprofen sodium as required | Extractions of bilaterally symmetrical impacted teeth during two visits. | 2 and 10 days post-operative | Jan 2013–Dec 2013 |
| Arteagoitia et al., 2005 [34] Europe | Double-blind RCT | n = 494 Age: 18–60 years. F: 295 M: 199 | 1. To assess the efficacy of amoxicillin/clavulanic acid 500/125 mg in preventing infectious and inflammatory complications (IC) in M3 subjects 2. To analyse whether variables such as age, sex, smoking, molar depth, and angulation, ostectomy, odontosection, and intervention time, could be considered risk factors associated with postoperative infectious and inflammatory complications | Amoxicillin/clavulanic acid 500/125 mg oral 3 times a day for 4 days after the intervention | Placebo | N/R | Preoperative: chlorhexidine mouthwash for 1 min Postoperative: chlorhexidine mouthwash 3 times a day for 7 days. | Postoperative: Diflunisal cap 500 mg every 12 h for 2 days as required/For moderate to severe pain: Metamizol cap 575 mg every 8 h | A single M3 was extracted from each patient. | 8 weeks | Mar 2001–Feb 2003 |
| Bergdahl and Hedstrom, 2004 [33] Europe | Double-blind RCT | n = 119 Age: 17–30 years. F: 67 M:52 | The aim of this study was to find out whether metronidazole 1600 mg given as a single dose before extraction of partially impacted mandibular molars reduced the incidence of dry socket | Single dose of metronidazole 1600 mg (four 400-mg tablets), | Placebo | 45 min before surgery | N/R | Postoperative: Paracetamol 500 mg with codeine 30 mg | Partially impacted teeth, which had partly broken through the mucosa, and a surgical flap was required to remove the tooth | 4 days later | N/R |
| Luaces-Rey et al., 2010 [28] Europe | Double-blind RCT | n = 145 18–60 years. F: 97 M:48 | Compare two amoxicillin administration patterns (short prophylactic therapy vs. long postoperative regimen | Short prophylactic therapy: 2 doses in 1 day = 2 g of amoxicillin 1 h before surgery in a single dose | Long postoperative regimen (4 days): 2 tablets of placebo in a single dose 1 h before surgery, followed by a second dose of 1 g of amoxicillin 6 h after and one tablet of 1 g amoxicillin every 8 h for 4 days | 1 h before surgery | Postoperative: chlorhexidine mouthwash every 8 h for 7 days | Postoperative: Deflazacort 30 mg one tab every 12 h for 5 days + Dexketoprofen in 25 mg capsule every 8 h as required | Surgical extraction of retained or partially erupted lower third molar due to malposition or any previous infectious or pain episode | 7 days post-operatively | N/R |
| López-Cedrún et al., 2011 [30] Europe | Double-blind RCT | n = 123 18–46 years. F: 90 M: 33 | Evaluate and compare the effectiveness of 2 different regimens of amoxicillin vs. placebo on the postoperative complications of third molar surgery. | Group A: 4 tablets of amoxicillin 500 mg (total 2 g) 2 h before surgery and 15 tablets of placebo, 3 times daily for 5 days Group B: 4 placebos, 2 h preoperatively and 15 tablets of placebo taken 3 times daily for 5 days. | Group C: 4 placebos 2 h preoperatively and 15 tablets of amoxicillin 500 mg to be taken immediately after surgery 3 times daily for 5 days. | 2 h before surgery | Preoperative: a session of professional oral hygiene + chlorhexidine mouth rinse before surgery | Postoperative: Ibuprofen 600 mg immediately after the procedure and every 12 h for 5 days. If not adequate: Metamizol 2 g as required | Patients who had at least one mandibular impacted or partially erupted 3M | 7 days | N/R |
| Rabi et al., 2018 [21] India | Randomized controlled trial | n = 60 20–35 years. Gender N/R | Evaluate the effectiveness of antimicrobial therapy in three groups following extraction of an impacted mandibular third molar | Group 1: 625 mg of combined amoxicillin and clavulanic acid tablet for 5 days Group 2: 625 mg of combined amoxicillin and clavulanic acid tablet + 400 mg metronidazole tablet for 5 days | Group 3: no treatment. | N/R | N/R | No description given to the type of analgesics used. | extraction of similar impacted mandibular 3Ms | N/R | N/R |
| Diz Dios et al., 2006 [20] Europe | Single-double-blinded | n = 221 Over 18–57 years. F: 126 M: 95 | Evaluate the efficacies of oral prophylactic treatment with amoxicillin (AMX), clindamycin (CLI), and moxifloxacin (MXF) in the prevention of bacteraemia following dental extractions (BDE) | AMX group: prophylactic 2 g of AMX orally 1 to 2 h before anaesthesia induction. CLI group: prophylactic 600 mg of CLI orally 1 to 2 h before anaesthesia induction. MXF group: prophylactic 400 mg of MXF orally 1 to 2 h before anaesthesia induction. | Control group did not receive any type of prophylaxis | 1 to 2 h before anaesthesia induction | N/R | N/R | N/R | N/R | Jan 2003–Dec 2004 |
| Citation | Study Conclusion (Direct Quotation) | Reviewer Comments |
|---|---|---|
| Milani et al. (2015) [22] | Pre-operative use of amoxicillin was not effective in reduction of infection, less pain, enabling mouth opening, lymphadenopathy, oedema, and body temperature following removal of fully impacted lower 3Ms in healthy ASA patients. | Only clinically and radiographically evaluated, lower and upper 3Ms impaction, surgeries which involving mandatory osteotomy to access the tooth were included in this study. The study used simple randomisation in which the allocation concealment technique was clearly described. The outcome assessors (surgeon, researcher, and patients) were unaware of group status. The results were standardised by age, gender, participants health condition as well as size, type, and classification of impaction. Amoxicillin was chosen due to its broad antibiotic’s spectrum of activity as well as being first line antibiotic in dentistry. The evaluation performed on the 4th day to allow the finding an infection if occurred. Study limitation: The study was a small study sample of 80 healthy young adults (≥18 years of age up to 30 years), therefore, results may not be generalisable to other population groups. |
| Mariscal-Cazalla et al. (2021) [31] | Administration of 750 mg amoxicillin before the removal of impacted lower 3Ms in healthy patients with no previous history of infection is unnecessary in reduction of possible complications (pain, inflammation, infection) and postoperative 5-day course of antibiotics is sufficient and postoperative 5-day course of antibiotics is sufficient. | Simple randomisation was used to allocate participants to each intervention. Tooth-related variables were the cause of extraction (preventive extraction, orthodontic cause, or damage of adjacent tooth, osteotomy degree, and coronal section, and the groups did not significantly differ in those variables. Study limitation: This research applied to a specific ethnic community (Caucasian) and therefore may not be generalisable to other populations. Another limitation is that antibiotic was administered 2-h before surgery which might be associated with reduction in the serum peak levels of the antibiotic during surgery, which may not allow for the peak blood levels to be achieved to prevent infection. A further limitation is that they did not include a group that received a preoperative dose alone, which would have revealed whether the same benefits could be achieved with a shorter course of treatment. The inclusion criteria were not fully described and was only standardised to the classification of mandibular third molar impaction. The indication of the surgery was varied between the patients including prophylactic, orthodontic and damage which might influence the result of this study. |
| Lacasa et al. (2007) [35] | Prophylactic administration of sustained release amoxicillin/clavulanate seems to be well tolerated and been effective in reduction of infection rate, less pain, less swelling, enabling mouth opening in patients undergoing ostectomy. | Groups were homogeneous in most variables recorded in this study and the planned sample size was obtained in all this study. Study limitation: The result of this study should be interpreted with caution due to missing information. This study did not give a definition of antibiotic adverse events, blinding of personnel and blinding of outcome assessment, timing of antibiotic, and the person performing the surgery. No description given on the surgical protocol in this trial. The descriptions of study population, type, position, and classification of third mandibular molar were not provided. Microbiological isolation, and identification of Gram-positive cocci was not carried out. In addition, this study was supported by a grant from GlaxoSmithKline S.A., Tres Cantos, Madrid, Spain. |
| Sekhar, Narayanan, and Baig (2001) [23] | Administration of pre and postoperative metronidazole 400 mg versus placebo does not seem to add any benefit in reduction of any of the variable measured and no significant differences observed in the outcome between the individual variables of three groups (p = 0.09), expect the degree of swelling which was significantly less in the five-day group (p = 0.03). | The study had a well-defined research question and standard technique regarding classification of impaction. The reason for choosing metronidazole was appropriately described. Study limitation: There is a concern regard the results of the study where the conclusion was not made based on the outcome being measured, in this case, mortality was not among outcomes measured. The description of study population was not clear. The study includes patients between 19 and 36 years of age making the finding not applicable to all ages. Duration of the study or enrolment period was not specified. The surgical technique was not described in this study. |
| Ataoğlu, Öz, Çandirli, and Kiziloğlu (2008) [32] | Routine administration of pre and postoperative antibiotic for removal of 3Ms in healthy patients is not supported. | This study compared three different groups: postoperatively for the first group and preoperatively for the second group versus no antibiotic. Presence or absence of infection, swelling, alveolar osteitis, interincisal mouth opening, and pain were evaluated by the same oral surgeon. Study limitations: The number of females participants included in this study is three times greater than number of males which cannot be applied to global population. Study design, setting, or duration, exclusion criteria, and randomisation method were not described, and infection was not defined explicitly. There was no clear explanation of ethics committee approval and how consent was obtained from patients. |
| Arteagoitia et al. (2015) [29] | Postoperative amoxicillin/clavulanic acid therapy has been more effective for pain relief, reduction in oedema and enabling mouth opening than placebo for extraction of bone impacted lower third molar. | The patients were instructed to self-report their pain, maximum mouth opening, and body temperature and all the post-operative variables were assessed by a single blinded observer. CRP levels were not found to be useful for the diagnosis of infection. The surgical time was measured using a stopwatch from the first incision until the last suture. Study limitation: The mean age between control group and experimental group was statistically significant (p = 0.001). The results can only be generalised to Caucasians. Insufficient information was given about exclusion criteria. |
| Siddiqi, Morkel, and Zafar (2010) [24] | No statistically significant difference in any of variable measured and conclude that administration of preoperative amoxicillin in non-immune-compromised patients versus placebo seems to add no benefit in reduction of infection rate, pain, swelling, trismus, and temperature between the two groups following surgical remove of third molar and routine administration of amoxicillin not recommended. | Each patient acted as their own control using a split-mouth technique. Standard classification of impaction was applied. Study limitation: the number of females included was two times greater than number of males which limit the application of the results to all males. The infection was not stated or defined explicitly. There were eight visits for each patient which potentially affected the compliance for follow-up visits and five patients were unable to complete the follow-up visits for domestic or socioeconomic reasons. No information provided regarding duration of study or time spent in surgery. |
| Bezerra et al. (2011) [25] | Prophylactic administration of amoxicillin 500 mg does not seem to impose additional benefits on reduction on inflammatory/infectious events to a young, healthy adult population, except for pain and mouth opening in which clear significant difference found between the experimental and control groups. | The reason for choosing the split mouth methodology was explicitly described in this study. Standard technique regarding position and degree of impaction between upper and lower 3Ms of the right and left sides of the mouth was applied according to classification and angulation position was described. In addition, inclusion criteria standardised for age and gender of participants. The mean duration of surgery was homogeneous for the experimental and control groups. Type and extent of the surgical procedures adapted for each case. The reassessment of the patients was performed by the one person. Study limitation: The study was a small cohort of patients, of which most were females. The study included patients with alveolitis and those with history of pain and pericoronitis. Confounders were not controlled or not stated. Participants age between 18 and 35 years, therefore, the results of this study may be more applicable to female younger adults and may not be generalisable to a global population. No information provided regarding the surgical protocol. |
| Kaczmarzyk et al. (2007) [26] | A single preoperative dose of clindamycin hydrochloride 600 mg with or without subsequent 5-day therapy 600 mg dose made no benefit in reduction of trismus, facial swelling, lymphadenopathy, and postoperative alveolar osteitis in patients following lower third molar surgical extraction with bone removal, except for body temperature in which statistically significant difference found between groups on the seventh postoperative day (p = 0.03). | The clindamycin was chosen due to its strong antimicrobial action towards strains isolated from odontogenic infection as well as its ability to reach a high concentration in bone tissue. All surgical procedures were carried out in an identical manner by either one of two oral surgeons, using identical sets of instruments. The duration of sugary, the period between incision of the mucosa and making the last suture been recorded. With regards to the timing of surgery, no statistically significant differences (p = 0.48) between groups been revealed. Study limitation: details of the enrolment period were missing. Three patients (3.0%) had clindamycin ceased and replaced by metronidazole due to adverse events; this might affect the results due to intervention inconsistency. There was a lack of clarity in the reporting of adverse events outcome in this study. |
| Xue et al. (2015) [27] | Pre and postoperative 0.5 g amoxicillin versus placebo made no significant effect to prevention of postoperative IC after extraction of bilaterally symmetrical impacted mandibular 3Ms and do not contribute to better wound healing or increased mouth opening, except for pain after extraction score for pain on day 10 (p = 0.005). | The definition of impacted teeth was well defined and classified. This study was well designed as split-mouth. Moreover, the mean extraction time was no longer than 30-min in each group. Study limitation: This study included alveolar osteitis as a sign of postoperative inflammation and infection. The infection was not stated or defined explicitly in sufficient detail in this study. There was a lack of clarity in the reporting of adverse events and criteria of postoperative complications and adverse reactions been mixed and reported as postoperative inflammation, including specific infection and adverse reactions. The results can be generalised to a specific Chinese population. There was lack of clarity in reporting adverse events due to antibiotics or infection and other complications. The dose regimen was not standardised and patients allergic to the used antibiotics received a modified regimen of another antibiotic which may hinder the results accuracy. |
| Arteagoitia et al. (2005) [34] | Supported the use of postoperative amoxicillin/clavulanic acid in 3Ms partially covered by bone and those in a horizontal position | Groups (placebo and antibiotic) were well balanced with respect to age, sex, smoking, molar depth, molar angulation, third molar position, intervention time, and need for sectioning. However, ostectomy was greater in placebo group. Study limitation: Dry socket included as a diagnosis of postoperative infection and inflammatory complication. The timing of postoperative administration antibiotic was not reported. |
| Bergdahl and Hedstrom (2004) [33] | A single dose of preoperative metronidazole was pointless in prevention of postoperative alveolar osteitis in those require removal of partially impacted teeth and does not seem to be beneficial in this case. | The inclusion criteria were only standardised for duration of operation, amount of saline irrigation, and amount of bone removed, both depth and volume. Study limitation: The participants were between the age of 17 and 30 years; therefore, the results of this study may be more applicable to younger adults than the global population. There was insufficient reporting on the inclusion and exclusion criteria. Female participants were taking contraceptive medication or had their menstrual periods during the procedures, and some (males and females) had history of pericoronitis or smoking tobacco which may have affected the patients’ outcomes. This study did not report the duration of study. |
| Luaces-Rey et al. (2010) [28] | Pre-and post-operative use of amoxicillin did not contribute better haematoma appearance, wound healing, less infection and intraoral inflammation, increased trismus and does not seem to reduce intake of rescue analgesics for pain management. | Patients were randomly enrolled to one of the two treatments according to the type of antibiotic treatment (short prophylactic antibiotic regimen or long postoperatively regimen). Patient, surgeon, and observer were unaware of intervention groups during the whole study. Both groups were homogeneous in every evaluated parameter including preoperative radiographic and clinical examination such as the tooth to be extracted (left, right) and the degree of impaction, position, and maximum preoperative oral opening between incisions. Each patient was provided with a form to self-report different numeric score for each outcome; pain score, type of diet (liquid, soft, or normal), corporal temperature, number of analgesic tablets taken every day, trismus (a 5 mm reduction was considered clinically significant). Each procedure was timed from first incision to completion of last suture. Study limitation: The number of females was two times greater than males making the results less applicable to the global population. The details of the duration of the study were not provided. The authors included a variety of definitions for infection using different clinical parameters which may also affected their conclusion. |
| López-Cedrún et al. (2011) [30] | Post-operative amoxicillin therapy versus placebo leads to lower infection, less fever and dysphagia, except intra and extraoral swelling which antibiotic does not seem to be effective in lowering intra and extraoral swelling following mandibular impacted or partially erupted third molar. | The number of ostectomies performed was similar in the three groups. In addition, the operative time was similar in all three groups. The standard surgical procedure been carried out and only one lower 3M was removed at a time. The mean operative time was longer in the infected patients (277 s) than non-infected patients (239 s). The two hours before the surgical procedure was to ensure the therapeutic antibiotic tissue level was reached before surgery. Study limitation: The participants were between the age of 18 and 46 years old; and the number of females included was three times more than males included in the study, therefore, the results may be more applicable to younger female adults, not the global population. The length of a clinical study was not specified. |
| Rabi et al. (2018) [21] | Administration of postoperative antibiotic was not effective in reduction of postoperative clinical infection evaluated between the individuals of all the three study groups following the extraction of impacted mandibular third molar. | There was no statistically significant difference between the mean ages of all study groups. Second group show slightly better satisfaction than other groups. Study limitation: The study was of a small sample. Timing of the antibiotic administered was not described. The infection was not stated or defined in sufficient detail. The authors did not explain whether the study was blinded or not. The study may be more applicable to younger adults; therefore, results may not be generalisable to the global population. Duration of surgery was missing in this study. This study is lacking relevant outcomes measured in this review. |
| Diz Dios et al. (2006) [20] | Amoxicillin and moxifloxacin prophylaxis showed significantly high efficacies (p < 0.001 for both) in reducing the prevalence and duration of bacteraemia whereas clindamycin prophylaxis was noneffective. | The study comprised of patients who, for behavioural reasons (autism, learning disabilities, phobias, etc.), underwent dental extractions under general anaesthesia. No significant differences were found between the different study age, sex, oral health grade, or number of teeth extracted groups. The incidence of bacteraemia was evaluated using peripheral venous blood sample taken from each patient before the dental manipulation and 30-s, 15-min, and 1-h after the final completion of the dental extractions. Study limitation: No description provided on who performed the surgery and the surgical technique was not described. This study did not describe the reasoning for dental extraction, or the duration of surgery and the participants’ inclusion and exclusion criteria were missing. None of this review’s measured outcomes was reported. |
| Citation | Selection Bias | Study Design | Confounders | Blinding | Data Collection Methods | Withdrawals and Dropouts | * Global Rating (Mean Score) |
|---|---|---|---|---|---|---|---|
| Milani et al., 2015 [22] | 3 | 1 | 0 | 1 | 2 | 1 | 1 |
| Mariscal-Cazalla et al., 2021 [31] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Lacasa et al., 2007 [35] | 1 | 1 | 1 | 2 | 2 | 1 | 1 |
| Sekhar, Narayanan, and Baig, 2001 [23] | 1 | 1 | 0 | 1 | 2 | 2 | 1 |
| Ataoğlu, et al., 2008 [32] | 3 | 3 | 0 | 3 | 2 | 3 | 2 |
| Arteagoitia et al., 2015 [29] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Siddiqi, Morkel, and Zafar, 2010 [24] | 1 | 1 | 0 | 1 | 2 | 1 | 1 |
| Bezerra et al., 2011 [25] | 2 | 1 | 0 | 1 | 2 | 1 | 1 |
| Kaczmarzyk et al., 2007 [26] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Xue et al., 2015 [27] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Arteagoitia et al., 2005 [34] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Bergdahl and Hedstrom, 2004 [33] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| Luaces-Rey et al., 2010 [28] | 1 | 1 | 1 | 1 | 2 | 1 | 1 |
| López-Cedrún et al., 2011 [30] | 2 | 1 | 1 | 1 | 2 | 1 | 1 |
| Rabi et al., 2018 [21] | 1 | 2 | 1 | 2 | 2 | 1 | 2 |
| Diz Dios et al., 2006 [20] | 1 | 1 | 1 | 2 | 2 | 1 | 1 |
| Citation | Increased Risk of Infection | Yes/No | Total |
|---|---|---|---|
| Arteagoitia et al., 2005 [34] | Age | Yes | 2, 9.5% |
| López-Cedrún et al., 2011 [30] | Age | Yes | - |
| Milani et al., 2015 [22] | Clinical symptoms | Yes | 1, 5% |
| Luaces-Rey et al., 2010 [28] | Difficult surgery | Yes | 1, 5% |
| López-Cedrún et al., 2011 [30] | Gender | Yes | 1, 5% |
| Arteagoitia et al., 2015 [29] | Inflammation | Yes | 1, 5% |
| López-Cedrún et al., 2011 [30] | Length of procedures | No | 1, 5% |
| Lacasa et al., 2007 [35] | Length of procedures | Yes | 2, 9.5% |
| Luaces-Rey et al., 2010 [28] | Length of procedures | Yes | - |
| Sekhar, Narayanan, and Baig, 2001 [23] | Placebo | No | 5, 24% |
| Siddiqi, Morkel, and Zafar, 2010 [24] | Placebo | No | - |
| Xue et al., 2015 [27] | Placebo | No | - |
| Bezerra et al., 2011 [25] | Placebo | No | - |
| Arteagoitia et al., 2015 [29] | Placebo | No | - |
| Lacasa et al., 2007 [35] | Placebo | Yes | 2, 9.5% |
| Ataoğlu, et al., 2008 [32] | Placebo | Yes | - |
| Mariscal-Cazalla et al., 2021 [31] | Requiring rescue ABs post-surgery | Yes | 1, 5% |
| Citation | Antibiotics vs. Placebo | Total |
|---|---|---|
| Mariscal-Cazalla et al., 2021 [31] | Favour ABs | 2 (12%) |
| Sekhar, Narayanan, and Baig, 2001 [23] | Favour Abs | |
| López-Cedrún et al., 2011 [30] | No difference | 7 (44%) |
| Siddiqi, Morkel, and Zafar, 2010 [24] | No difference | |
| Xue et al., 2015 [27] | No difference | |
| Lacasa et al., 2007 [35] | No difference | |
| Ataoğlu, et al., 2008 [32] | No difference | |
| Kaczmarzyk et al., 2007 [26] | No difference | |
| Milani et al., 2015 [22] | No difference |
| Ramos et al., 2016 [42] | With regard to other published meta-analyses, Ramos et al. (2016) assessed the efficacy of any orally or parenterally administered antibiotics at any dose or regimen, and with regard to comparisons in preventing dry socket and/or infection after third molar extraction. The author included 21 double-blinded RCTs analysed for dry socket and/or infection and 12 studies analysed for adverse events. The author found that antibiotics administered to prevent dry socket and/or infection are beneficial in reducing the risk of infection after third molar extraction by 57% (RR = 0.43; 95% CI 0.33–0.56; p < 0.0001) with NNH of 16 patients. This is comparable with the findings of the current meta-analysis, which found a higher reduction of infection by 69% with NNT of 17. In addition, this review did not combine dry socket with infection in the metanalysis, they were analysed separately. However, with regard to adverse events, the findings are different from the current findings where the risk of adverse reactions from AB administration was found not statistically significant with a smaller NNH of 16 patients. In this metanalysis, the NNT was 55 patients but this metanalysis was limited to RCT studies published since 2000 in which only oral systemic antibiotic use was analysed. |
| Singh Gill et al., 2018 [43] | The systematic review and metanalysis performed by Singh Gill et al. (2018) identified four RCTs published since 2000 until 2013 in their final review to evaluate the effectiveness of antibiotic prophylaxis in preventing infections in extraction procedures in patients requiring single/multiple dental extractions for various indications (impacted wisdom teeth, abscess etc.) undergoing dental extraction and the results showed that there was no clear evidence pointing to the need for prophylactic antibiotics for reduction of infection after third molar extraction. The current findings and recommendations were not congruent with theirs, where a significant reduction of infection with NNT of 17 patients was identified, although the current analysis included a recently published study with a large number of patients. The systematic review and metanalysis conducted by Singh Gill et al. (2018) included three randomised controlled trials (RCTs) which compared the administration of any antibiotic vs. placebo to patients undergoing dental implant placement. The author concluded that prophylactic antibiotics were not beneficial in those undergoing implant surgeries since p value (p = 0.09) with NNT of 33 under normal conditions. This finding differs from the current study, The variation in conclusions is related the inclusion of three additional studies in this analysis. A greater (65%) reduction in risk of implant failure with antibiotic with a smaller NNT was observed in this metanalysis. In addition, the study concluded that there is lack of evidence that antibiotic use reduces the risk of post-operative complications following dental implant placement. These findings and recommendations were similar to theirs, although we included two additional RCTs in our analysis. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torof, E.; Morrissey, H.; Ball, P.A. The Role of Antibiotic Use in Third Molar Tooth Extractions: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 422. https://doi.org/10.3390/medicina59030422
Torof E, Morrissey H, Ball PA. The Role of Antibiotic Use in Third Molar Tooth Extractions: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(3):422. https://doi.org/10.3390/medicina59030422
Chicago/Turabian StyleTorof, Elham, Hana Morrissey, and Patrick A. Ball. 2023. "The Role of Antibiotic Use in Third Molar Tooth Extractions: A Systematic Review and Meta-Analysis" Medicina 59, no. 3: 422. https://doi.org/10.3390/medicina59030422
APA StyleTorof, E., Morrissey, H., & Ball, P. A. (2023). The Role of Antibiotic Use in Third Molar Tooth Extractions: A Systematic Review and Meta-Analysis. Medicina, 59(3), 422. https://doi.org/10.3390/medicina59030422