

Spontaneous Reversal of Vitiligo, a Rare Phenomenon Reported in a Case in Saudi Arabia with an Insight into Metabolic Biochemical Derangements


Abstract
:1. Introduction
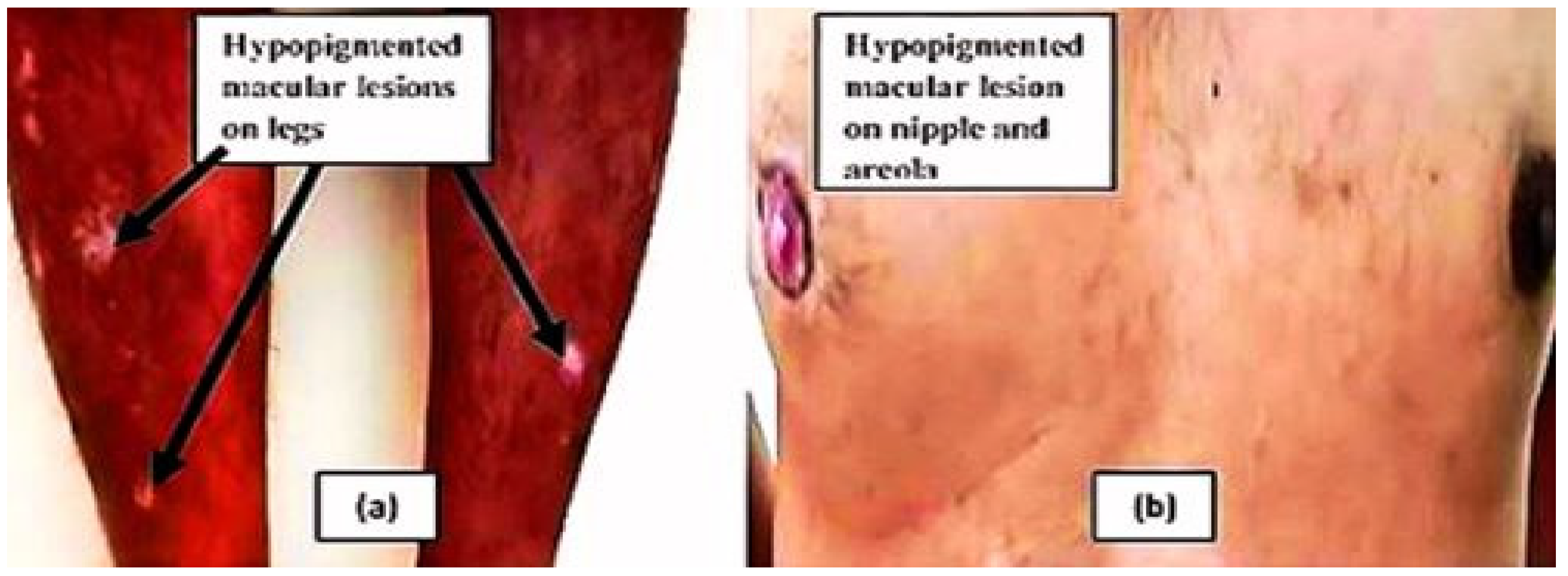
2. Case Presentation
3. Methods
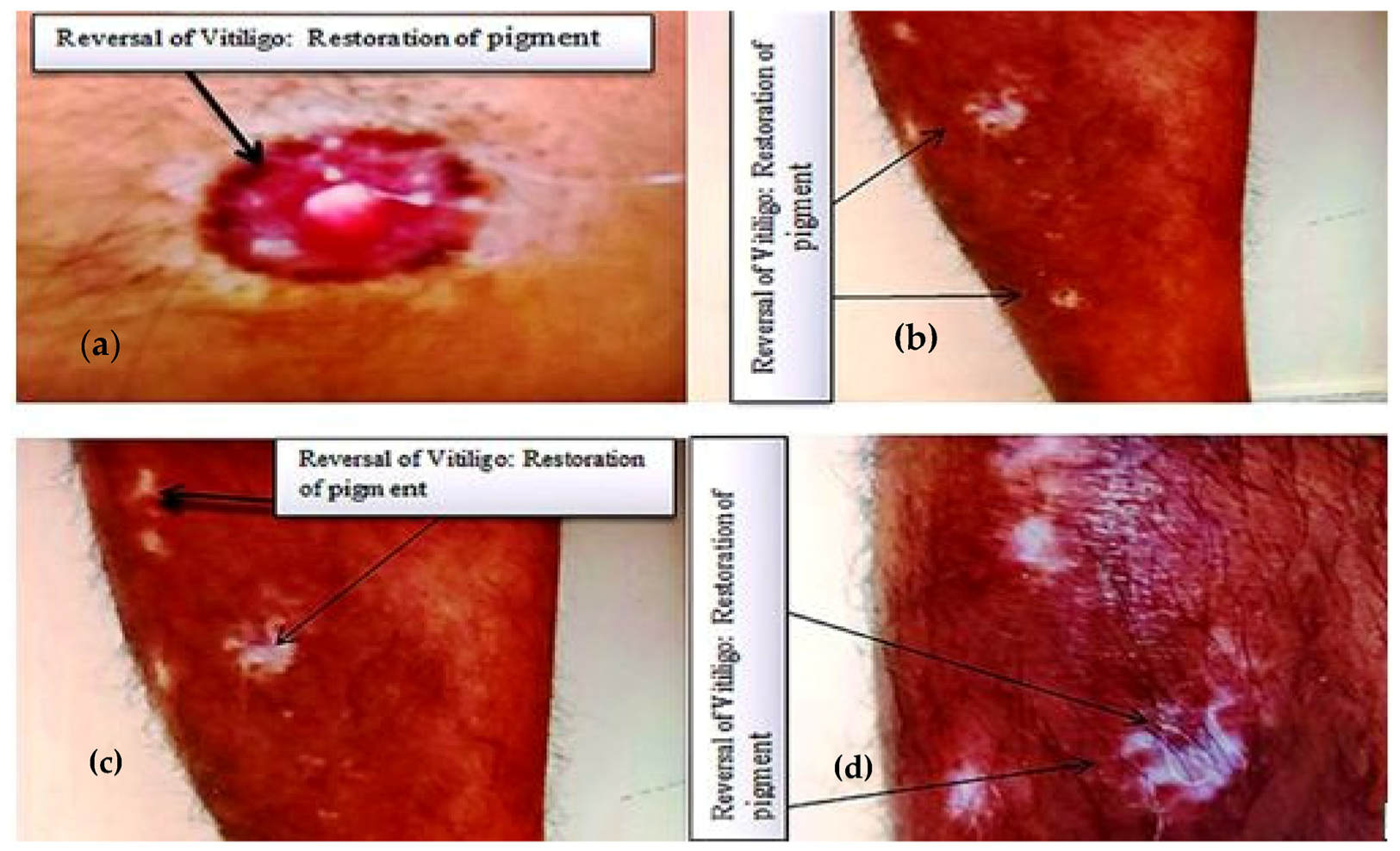
4. Results
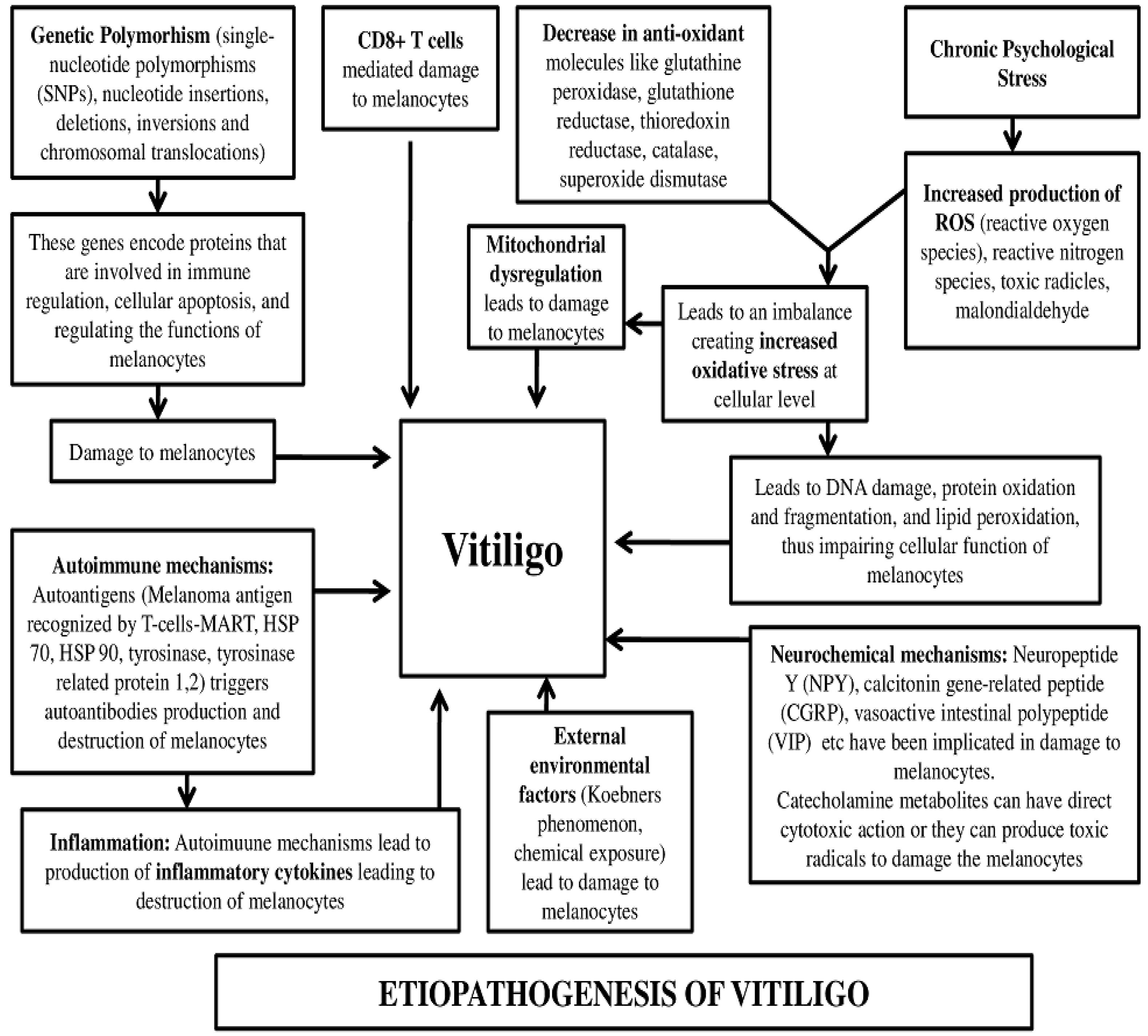
5. Discussion
6. Conclusions
Implications of the Study
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, Y.; Cai, Y.; Shi, M.; Jiang, S.; Cui, S.; Wu, Y.; Gao, X.H.; Chen, H.D. The Prevalence of Vitiligo: A Meta-Analysis. PLoS ONE 2016, 11, e0163806. [Google Scholar] [CrossRef] [Green Version]
- NHS Website. Vitiligo. Available online: https://www.nhs.uk/conditions/vitiligo/ (accessed on 9 May 2022).
- Hamidizadeh, N.; Ranjbar, S.; Ghanizadeh, A.; Parvizi, M.M.; Jafari, P.; Handjani, F. Evaluating prevalence of depression, anxiety and hopelessness in patients with Vitiligo on an Iranian population. Health Qual. Life Outcomes 2020, 18, 20. [Google Scholar] [CrossRef]
- Bergqvist, C.; Ezzedine, K. Vitiligo: A focus on pathogenesis and its therapeutic implications. J. Dermatol. 2021, 48, 252–270. [Google Scholar] [CrossRef]
- Marasca, C.; Fornaro, L.; Martora, F.; Picone, V.; Fabbrocini, G.; Megna, M. Onset of vitiligo in a psoriasis patient on ixekizumab. Dermatol. Ther. 2021, 34, e15102. [Google Scholar] [CrossRef] [PubMed]
- Martora, F.; Battista, T.; Fornaro, L.; Fabbrocini, G.; Megna, M.; Picone, V.; Marasca, C. Generalized versus localized vitiligo after ixekizumab: May previous treatment affect the clinical presentation? Dermatol. Ther. 2022, 35, e15874. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, G.F.; Gomaa, A.H.; Al-Dhubaibi, M.S. Highlights in pathogenesis of vitiligo. World J. Clin. Cases 2015, 3, 221. [Google Scholar] [CrossRef]
- Li, L. The Role of MicroRNAs in Vitiligo: Regulators and Therapeutic Targets. Ann. Dermatol. 2020, 32, 441. [Google Scholar] [CrossRef]
- Basnet, B.; Bhushan, A.; Khan, R.; Kumar, G.; Sharma, V.K.; Sharma, A.; Gupta, S. Plasma & urinary catecholamines & urinary vanillylmandelic acid levels in patients with generalized vitiligo. Indian J. Med. Res. 2018, 147, 384–390. [Google Scholar] [PubMed]
- Alkhateeb, A.; Fain, P.R.; Thody, A.; Bennett, D.C.; Spritz, R.A. Epidemiology of vitiligo and associated autoimmune diseases in Caucasian probands and their families. Pigment Cell Res. 2003, 16, 208–214. [Google Scholar] [CrossRef]
- Majumder, P.P.; Nordlund, J.J.; Nath, S.K. Pattern of familial aggregation of vitiligo. Arch. Dermatol. 1993, 129, 994. [Google Scholar] [CrossRef]
- Spritz, R.A.; Andersen, G.H. Genetics of vitiligo. Dermatol. Clin. 2017, 35, 245–255. [Google Scholar] [CrossRef] [Green Version]
- Aly, D.G.; Salem, S.A.; Amr, K.S.; El-Hamid, M.F.A. A study of the association of glutathione S-transferase M1/T1 polymorphisms with susceptibility to vitiligo in Egyptian patients. An. Bras. Dermatol. 2018, 93, 54–58. [Google Scholar] [CrossRef] [Green Version]
- Karam, R.A.; Zidan, H.E.; Khater, M.H. Genetic variants of interferon-gamma and its mRNA expression and inflammatory parameters in the pathogenesis of vitiligo. Biochem. Cell Biol. 2017, 95, 474–481. [Google Scholar] [CrossRef]
- Richmond, J.M.; Frisoli, M.L.; Harris, J.E. Innate immune mechanisms in vitiligo: Danger from within. Curr. Opin. Immunol. 2013, 25, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Zhu, G.; Yang, Y.; Jian, Z.; Guo, S.; Dai, W.; Shi, Q.; Ge, R.; Ma, J.; Liu, L.; et al. Oxidative stress drives CD8+ T-cell skin trafficking in patients with vitiligo through CXCL16 upregulation by activating the unfolded protein response in keratinocytes. J. Allergy Clin. Immunol. 2017, 140, 177–189.e9. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Zhu, G.; Yang, Y.; Guo, S.; Dai, W.; Wang, G.; Gao, T.; Li, C. Oxidative stress-induced chemokine production mediates CD8(+) T cell skin trafficking in vitiligo. J. Investig. Dermatol. Symp. Proc. 2015, 17, 32–33. [Google Scholar] [CrossRef] [Green Version]
- Cavalli, G.; Hayashi, M.; Jin, Y.; Yorgov, D.; Santorico, S.A.; Holcomb, C.; Rastrou, M.; Erlich, H.; Tengesdal, I.W.; Dagna, L.; et al. MHC class II super-enhancer increases surface expression of HLA-DR and HLA-DQ and affects cytokine production in autoimmune vitiligo. Proc. Natl. Acad. Sci. USA 2016, 113, 1363–1368. [Google Scholar] [CrossRef] [Green Version]
- Zhu, M.C.; Liu, C.G.; Wang, D.X.; Zhan, Z. Detection of serum anti-melanocyte antibodies and identification of related antigens in patients with vitiligo. Genet. Mol. Res. 2015, 14, 16060. [Google Scholar] [CrossRef]
- Kemp, E.H.; Gawkrodger, D.J.; Watson, P.F.; Weetman, A.P. Immunoprecipitation of melanogenic enzyme autoantigens with vitiligo sera: Evidence for cross-reactive autoantibodies to tyrosinase and tyrosinase-related protein-2 (TRP-2). Clin. Exp. Immunol. 1997, 109, 495. [Google Scholar] [CrossRef]
- Dell’Anna, M.L.; Maresca, V.; Briganti, S.; Camera, E.; Falchi, M.; Picardo, M. Mitochondrial impairment in peripheral blood mononuclear cells during the active phase of vitiligo. J. Investig. Dermatol. 2001, 117, 908–913. [Google Scholar] [CrossRef] [Green Version]
- Yi, X.; Guo, W.; Shi, Q.; Yang, Y.; Zhang, W.; Chen, X.; Kang, P.; Chen, J.; Cui, T.; Ma, J.; et al. SIRT3-dependent mitochondrial dynamics remodeling contributes to oxidative stress-induced melanocyte degeneration in vitiligo. Theranostics 2019, 9, 1614–1633. [Google Scholar] [CrossRef]
- Gianfaldoni, S.; Wollina, U.; Tirant, M.; Tchernev, G.; Lotti, J.; Satolli, F.; Rovesti, M.; França, K.; Lotti, T. Herbal Compounds for the Treatment of Vitiligo: A Review. Open Access Maced. J. Med. Sci. 2018, 6, 203. [Google Scholar] [CrossRef] [Green Version]
- Aggarwal, B.B.; Harikumar, K.B. Potential therapeutic effects of curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. Int. J. Biochem. Cell Biol. 2009, 41, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asawanonda, P.; Klahan, S.O. Tetrahydrocurcuminoid cream plus targeted narrowband UVB phototherapy for vitiligo:a preliminary randomized controlled study. Photomed. Laser Surg. 2010, 28, 679–684. [Google Scholar] [CrossRef]
- Irshad, H.; Syed, N.H.S.; Abdul, M.B.; Barkat, A.K.; Rashid, A. Natural herbal vitiligo treatment, honey: An applied case study. Med. Channel 2015, 21, 63–66. [Google Scholar]
- Aparna, A.R.; Rajalakshmi, D. Honey, its characteristics, sensory aspects, and applications. Food Rev. Int. 1999, 15, 455–471. [Google Scholar] [CrossRef]
- Djerrou, Z. Successful treatment of facial vitiligo with honey bee, Allium cepa and Avena sativa combined to sunlight exposure: A case clinical trial. Int. J. Ofpharmaceutical Clin. Res. 2015, 7, 9–14. [Google Scholar]
- Ghaderi, R.; Nezafati, P. A New Biomarker in Patients with Vitiligo: A Case-Control Study. MOJ Immunol. 2016, 3, 00106. [Google Scholar] [CrossRef] [Green Version]
- Shankar, D.S.; Shashikala, K.; Madala, R. Clinical patterns of vitiligo and its associated co morbidities: A prospective controlled cross-sectional study in South India. Indian Derm. Online J. 2012, 3, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Cinegaglia, N.; Acosta-Navarro, J.; Rainho, C.; Antoniazzi, L.; Mattioli, S.; Pimentel, C.; Santos, R.D.; Sandrim, V. Association of Omnivorous and Vegetarian Diets With Antioxidant Defense Mechanisms in Men. J. Am. Heart Assoc. 2020, 9, e015576. [Google Scholar] [CrossRef]
- Das, S.K.; Vasudevan, D.M. Alcohol-induced oxidative stress. Life Sci. 2007, 81, 177. [Google Scholar] [CrossRef]
- Aryanian, Z.; Shirzadian, A.; Farzaneh, S.; Goodarzi, A.; Azizpour, A.; Hatami, P. Metabolic derangement in patients with vitiligo: A cross-sectional study. J. Investig. Med. 2022, 70, 963. [Google Scholar] [CrossRef] [PubMed]
- Damiani, G.; Gironi, L.C.; Kridin, K.; Pacifico, A.; Buja, A.; Bragazzi, N.L.; Spalkowska, M.; Pigatto, P.D.M.; Santus, P.; Young Dermatologists Italian Network; et al. Mask-induced Koebner phenomenon and its clinical phenotypes: A multicenter, real-life study focusing on 873 dermatological consultations during COVID-19 pandemics. Dermatol Ther. 2021, 34, e14823. [Google Scholar] [CrossRef] [PubMed]
- dos Santos Garrett, N.F.M.; da Costa, A.C.C.; Ferreira, E.B.; Damiani, G.; dos Reis, P.E.D.; Vasques, C.I. Prevalence of dermatological toxicities in patients with melanoma undergoing immunotherapy: Systematic review and meta-analysis. PLoS ONE 2021, 16, e0255716. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Previous Data (When Vitiligo Was First Diagnosed in 2019) | Current Data (When Vitiligo Lesions Showed Reversal in 2022) |
|---|---|---|
| Age (years) | 38 | 41 |
| Weight (kg) | 70 | 75 |
| BMI (kg/m2) | 23.7 | 25.4 |
| Smoker | No | No |
| Alcoholic | Occasional | No |
| Dietary habit | Nonvegetarian | Vegetarian |
| % of body surface area covered with macules | <10% | <10% |
| Duration of vitiligo | 6 months | 3 years |
| Leukotrichia | Present | Present |
| Koebner phenomenon | Absent | Absent |
| Mucosal involvement | None | None |
| Diascopy findings | Not available | Uniformly depigmented lesions observed with sharp demarcated margins; no color change observed on diascopy, ruling out nevus depigmentosus |
| On rubbing the lesions | No erythema (nevus anemicus ruled out) | No erythema (nevus anemicus ruled out) |
| Any associated cutaneous disorder such as alopecia areata, halo nevus, lichen planus, plaque psoriasis, alopecia areata, and ichthyosis vulgaris | None | None |
| Any associated systemic disorder such as diabetes, hypothyroidism, hyperthyroidism, and pernicious anemia | None | None |
| Blood pressure; SBP/DBP (mm Hg) | 124/84 | 118/82 |
| Blood group | B+ | B+ |
| Variable | Previous Data (When Vitiligo Was First Diagnosed in 2019) | Current Data (When Vitiligo Lesions Showed Reversal in 2022) |
|---|---|---|
| Hemoglobin (g%) | 14.5 | 15.2 |
| RBC count (million cells/cu mm) | 4.8 | 5.1 |
| WBC count (/cu mm) | 9320 | 7250 |
| Platelet count (/cu mm) | 250,000 | 285,000 |
| ESR (mm/hr) | 22 | 5 |
| hsCRP (mg/L) | 9.2 | 2 |
| FBS (mg/dL) | 102 | 85 |
| HbA1c (%) | 5.2 | 4.8 |
| Total cholesterol (mg/dL) | 250 | 161 |
| Triglyceride (mg/dL) | 130 | 125 |
| LDL (mg/dL) | 105 | 90 |
| HDL (mg/dL) | 38 | 51 |
| LFT | Normal | Normal |
| KFT | Normal | Normal |
| Uric acid (mg/dL) | 5.4 | 5.2 |
| Total T3 (ng/mL) | 1.2 | 1.4 |
| Total T4 (µg/dL) | 7.5 | 8 |
| TSH (µIU/mL) | 3.5 | 3.2 |
| 25-hydroxy vitamin D (ng/mL) | 25 | 28 |
| KOH microscopy | Negative | Not done |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshaikh, A.A.; Bharti, R.K. Spontaneous Reversal of Vitiligo, a Rare Phenomenon Reported in a Case in Saudi Arabia with an Insight into Metabolic Biochemical Derangements. Medicina 2023, 59, 427. https://doi.org/10.3390/medicina59030427
Alshaikh AA, Bharti RK. Spontaneous Reversal of Vitiligo, a Rare Phenomenon Reported in a Case in Saudi Arabia with an Insight into Metabolic Biochemical Derangements. Medicina. 2023; 59(3):427. https://doi.org/10.3390/medicina59030427
Chicago/Turabian StyleAlshaikh, Ayoub Ali, and Rishi Kumar Bharti. 2023. "Spontaneous Reversal of Vitiligo, a Rare Phenomenon Reported in a Case in Saudi Arabia with an Insight into Metabolic Biochemical Derangements" Medicina 59, no. 3: 427. https://doi.org/10.3390/medicina59030427
APA StyleAlshaikh, A. A., & Bharti, R. K. (2023). Spontaneous Reversal of Vitiligo, a Rare Phenomenon Reported in a Case in Saudi Arabia with an Insight into Metabolic Biochemical Derangements. Medicina, 59(3), 427. https://doi.org/10.3390/medicina59030427