
Determinants of Arterial Stiffness in Patients with Morbid Obesity. The Role of Echocardiography and Carotid Ultrasound Imaging
 ,
,  ,
,  , , , and
, , , and
Abstract
:1. The role of Imaging Methods in Cardiovascular Risk Assessment
2. Materials and Methods
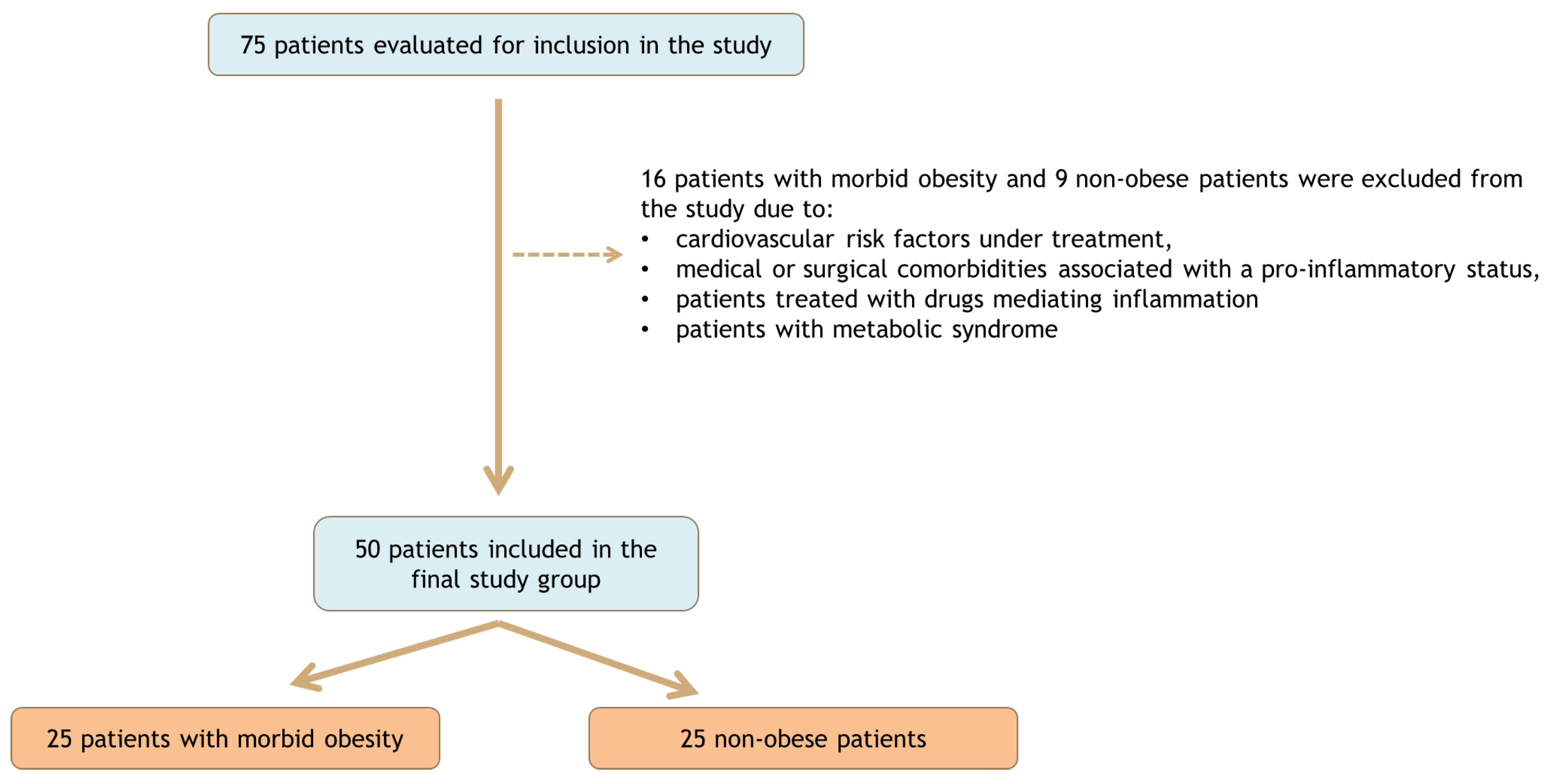
2.1. Study Design and Population
2.2. Laboratory Measurements
2.3. Arterial Stiffness Evaluation
2.4. Transthoracic Echocardiography and Carotid Doppler Ultrasound
2.5. Intraoperative Biopsy for Local Adipocytes Evaluation
2.6. Statistical Analysis
2.7. Ethics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; Pilbrow, A.P.; Liew, O.W.; Chong, J.P.C.; Sluyter, J.; Lewis, L.K.; Lassé, M.; Frampton, C.M.; Jackson, R.; Poppe, K.; et al. Circulating Cardiac Biomarkers Improve Risk Stratification for Incident Cardiovascular Disease in Community Dwelling Populations. eBioMedicine 2022, 82, 104170. [Google Scholar] [CrossRef] [PubMed]
- Flora, G.D.; Nayak, M.K. A Brief Review of Cardiovascular Diseases, Associated Risk Factors and Current Treatment Regimes. Curr. Pharm. Des. 2019, 25, 4063–4084. [Google Scholar] [CrossRef] [PubMed]
- Anghel, R.; Adam, C.A.; Marcu, D.T.M.; Mitu, O.; Mitu, F. Cardiac Rehabilitation in Patients with Peripheral Artery Disease—A Literature Review in COVID-19 Era. J. Clin. Med. 2022, 11, 416. [Google Scholar] [CrossRef]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990–2019. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Münzel, T.; Hahad, O.; Sørensen, M.; Lelieveld, J.; Duerr, G.D.; Nieuwenhuijsen, M.; Daiber, A. Environmental Risk Factors and Cardiovascular Diseases: A Comprehensive Expert Review. Cardiovasc. Res. 2022, 118, 2880–2902. [Google Scholar] [CrossRef]
- Anghel, R.; Adam, C.A.; Marcu, D.T.M.; Mitu, O.; Roca, M.; Tinica, G.; Mitu, F. Cardiac Rehabilitation in Peripheral Artery Disease in a Tertiary Center—Impact on Arterial Stiffness and Functional Status after 6 Months. Life 2022, 12, 601. [Google Scholar] [CrossRef]
- Tarsitano, M.G.; Pandozzi, C.; Muscogiuri, G.; Sironi, S.; Pujia, A.; Lenzi, A.; Giannetta, E. Epicardial Adipose Tissue: A Novel Potential Imaging Marker of Comorbidities Caused by Chronic Inflammation. Nutrients 2022, 14, 2926. [Google Scholar] [CrossRef]
- Anghel, R.; Adam, C.A.; Mitu, O.; Marcu, D.T.M.; Onofrei, V.; Roca, M.; Costache, A.D.; Miftode, R.S.; Tinica, G.; Mitu, F. Cardiac Rehabilitation and Mortality Risk Reduction in Peripheral Artery Disease at 6-Month Outcome. Diagnostics 2022, 12, 1500. [Google Scholar] [CrossRef] [PubMed]
- Aljafary, M.A.; Al-Suhaimi, E.A. Adiponectin System (Rescue Hormone): The Missing Link between Metabolic and Cardiovascular Diseases. Pharmaceutics 2022, 14, 1430. [Google Scholar] [CrossRef]
- Menzaghi, C.; Trischitta, V. The Adiponectin Paradox for All-Cause and Cardiovascular Mortality. Diabetes 2018, 67, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Rochlani, Y.; Pothineni, N.V.; Kovelamudi, S.; Mehta, J.L. Metabolic Syndrome: Pathophysiology, Management, and Modulation by Natural Compounds. Ther. Adv. Cardiovasc. Dis. 2017, 11, 215–225. [Google Scholar] [CrossRef] [Green Version]
- Dobrowolski, P.; Prejbisz, A.; Kuryłowicz, A.; Baska, A.; Burchardt, P.; Chlebus, K.; Dzida, G.; Jankowski, P.; Jaroszewicz, J.; Jaworski, P.; et al. Metabolic Syndrome—A New Definition and Management Guidelines. A Joint Position Paper by the Polish Society of Hypertension, Polish Society for the Treatment of Obesity, Polish Lipid Association, Polish Association for Study of Liver, Polish Society of Family Medicine, Polish Society of Lifestyle Medicine, Division of Prevention and Epidemiology Polish Cardiac Society, “Club 30” Polish Cardiac Society, and Division of Metabolic and Bariatric Surgery Society of Polish Surgeons. Arch. Med. Sci. 2022, 18, 1133–1156. [Google Scholar] [CrossRef]
- Luo, W.; Guo, Z.; Wu, M.; Hao, C.; Zhou, Z.; Yao, X. Index of Central Obesity as a Parameter to Replace Waist Circumference for the Definition of Metabolic Syndrome in Predicting Cardiovascular Disease. J. Cardiovasc. Med. 2014, 15, 738. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Gutch, M.; Kumar, S.; Razi, S.; Gupta, K.; Gupta, A. Assessment of Insulin Sensitivity/Resistance. Indian J. Endocrinol. Metab. 2015, 19, 160. [Google Scholar] [CrossRef]
- Mattern, A.; Zellmann, T.; Beck-Sickinger, A.G. Processing, Signaling, and Physiological Function of Chemerin. IUBMB Life 2014, 66, 19–26. [Google Scholar] [CrossRef]
- Para, I.; Albu, A.; Porojan, M.D. Adipokines and Arterial Stiffness in Obesity. Med. Kaunas Lith. 2021, 57, 653. [Google Scholar] [CrossRef]
- Aursulesei, V.; Timofte, D.; Tarau, L.M.; Mocanu, V.; Namat, R.A.; Aursulesei, V.C.; Costache, I.I. Circulating Chemerin Levels, Anthropometric Indices and Metabolic Profile in Morbid Obesity. Rev. Chim. 2018, 69, 1419–1423. [Google Scholar] [CrossRef]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.K.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.S.; Protogerou, A.D.; et al. Expert Consensus Document on the Measurement of Aortic Stiffness in Daily Practice Using Carotid-Femoral Pulse Wave Velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef] [Green Version]
- Lancellotti, P.; Zamorano, J.L.; Habib, G.; Badano, L. The EACVI Textbook of Echocardiography; Oxford University Press: Oxford, UK, 2016; ISBN 978-0-19-103889-1. [Google Scholar]
- Eroğlu, S. How Do We Measure Epicardial Adipose Tissue Thickness by Transthoracic Echocardiography? Anatol. J. Cardiol. 2015, 15, 416–419. [Google Scholar] [CrossRef] [Green Version]
- Parisi, V.; Conte, M.; Petraglia, L.; Grieco, F.V.; Bruzzese, D.; Caruso, A.; Grimaldi, M.G.; Campana, P.; Gargiulo, P.; Paolillo, S.; et al. Echocardiographic Epicardial Adipose Tissue Thickness for Risk Stratification of Patients With Heart Failure. Front. Physiol. 2020, 11, 43. [Google Scholar] [CrossRef]
- Aursulesei Onofrei, V.; Ceasovschih, A.; Anghel, R.C.; Roca, M.; Marcu, D.T.M.; Adam, C.A.; Mitu, O.; Cumpat, C.; Mitu, F.; Crisan, A.; et al. Subendocardial Viability Ratio Predictive Value for Cardiovascular Risk in Hypertensive Patients. Medicina 2023, 59, 24. [Google Scholar] [CrossRef]
- Casella, I.B.; Presti, C.; Porta, R.M.P.; Sabbag, C.R.D.; Bosch, M.A.; Yamazaki, Y. A Practical Protocol to Measure Common Carotid Artery Intima-Media Thickness. Clinics 2008, 63, 515–520. [Google Scholar] [CrossRef] [Green Version]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. Endorsed by the Society for Vascular Medicine. American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2008, 21, 93–111; quiz 189–190. [Google Scholar] [CrossRef]
- Britton, K.A.; Massaro, J.M.; Murabito, J.M.; Kreger, B.E.; Hoffmann, U.; Fox, C.S. Body Fat Distribution, Incident Cardiovascular Disease, Cancer, and All-Cause Mortality. J. Am. Coll. Cardiol. 2013, 62, 921–925. [Google Scholar] [CrossRef] [Green Version]
- Mahabadi, A.A.; Berg, M.H.; Lehmann, N.; Kälsch, H.; Bauer, M.; Kara, K.; Dragano, N.; Moebus, S.; Jöckel, K.-H.; Erbel, R.; et al. Association of Epicardial Fat with Cardiovascular Risk Factors and Incident Myocardial Infarction in the General Population: The Heinz Nixdorf Recall Study. J. Am. Coll. Cardiol. 2013, 61, 1388–1395. [Google Scholar] [CrossRef] [Green Version]
- Al-Talabany, S.; Mordi, I.; Graeme Houston, J.; Colhoun, H.M.; Weir-McCall, J.R.; Matthew, S.Z.; Looker, H.C.; Levin, D.; Belch, J.J.F.; Dove, F.; et al. Epicardial Adipose Tissue Is Related to Arterial Stiffness and Inflammation in Patients with Cardiovascular Disease and Type 2 Diabetes. BMC Cardiovasc. Disord. 2018, 18, 31. [Google Scholar] [CrossRef]
- Nerlekar, N.; Brown, A.J.; Muthalaly, R.G.; Talman, A.; Hettige, T.; Cameron, J.D.; Wong, D.T.L. Association of Epicardial Adipose Tissue and High-Risk Plaque Characteristics: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2017, 6, e006379. [Google Scholar] [CrossRef]
- Yang, M.-C.; Liu, H.-K.; Tsai, C.-C.; Su, Y.-T.; Wu, J.-R. Epicardial Adipose Tissue Was Highly Associated with Reduction in Left Ventricular Diastolic Function as Early as in Adolescence. Acta Cardiol. Sin. 2022, 38, 601–611. [Google Scholar] [CrossRef]
- Shimabukuro, M.; Hirata, Y.; Tabata, M.; Dagvasumberel, M.; Sato, H.; Kurobe, H.; Fukuda, D.; Soeki, T.; Kitagawa, T.; Takanashi, S.; et al. Epicardial Adipose Tissue Volume and Adipocytokine Imbalance Are Strongly Linked to Human Coronary Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1077–1084. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, A.; Sharma, H.; Yuan, D.; Trollope, A.F.; Chilton, L. The Role of Epicardial Adipose Tissue in the Development of Atrial Fibrillation, Coronary Artery Disease and Chronic Heart Failure in the Context of Obesity and Type 2 Diabetes Mellitus: A Narrative Review. J. Cardiovasc. Dev. Dis. 2022, 9, 217. [Google Scholar] [CrossRef]
- Choi, T.-Y.; Ahmadi, N.; Sourayanezhad, S.; Zeb, I.; Budoff, M.J. Relation of Vascular Stiffness with Epicardial and Pericardial Adipose Tissues, and Coronary Atherosclerosis. Atherosclerosis 2013, 229, 118–123. [Google Scholar] [CrossRef]
- Natale, F.; Tedesco, M.A.; Mocerino, R.; de Simone, V.; Di Marco, G.M.; Aronne, L.; Credendino, M.; Siniscalchi, C.; Calabrò, P.; Cotrufo, M.; et al. Visceral Adiposity and Arterial Stiffness: Echocardiographic Epicardial Fat Thickness Reflects, Better than Waist Circumference, Carotid Arterial Stiffness in a Large Population of Hypertensives. Eur. J. Echocardiogr. J. Work. Group Echocardiogr. Eur. Soc. Cardiol. 2009, 10, 549–555. [Google Scholar] [CrossRef]
- Cabrera-Rego, J.O.; Iacobellis, G.; Castillo-Herrera, J.A.; Valiente-Mustelier, J.; Gandarilla-Sarmientos, J.C.; Marín-Juliá, S.M.; Navarrete-Cabrera, J. Epicardial Fat Thickness Correlates With Carotid Intima-Media Thickness, Arterial Stiffness, and Cardiac Geometry in Children and Adolescents. Pediatr. Cardiol. 2014, 35, 450–456. [Google Scholar] [CrossRef]
- Gilardini, L.; Pasqualinotto, L.; Di Matteo, S.; Caffetto, K.; Croci, M.; Girola, A.; Invitti, C. Factors Associated with Early Atherosclerosis and Arterial Calcifications in Young Subjects with a Benign Phenotype of Obesity. Obes. Silver Spring Md 2011, 19, 1684–1689. [Google Scholar] [CrossRef]
- Demir, K.; Avcı, A.; Ergulu Esmen, S.; Tuncez, A.; Yalcın, M.U.; Yılmaz, A.; Yılmaz, S.; Altunkeser, B.B. Assessment of Arterial Stiffness and Epicardial Adipose Tissue Thickness in Predicting the Subclinical Atherosclerosis in Patients with Ankylosing Spondylitis. Clin. Exp. Hypertens. 2021, 43, 169–174. [Google Scholar] [CrossRef]
- Korkmaz, L.; Cirakoglu, O.F.; Ağaç, M.T.; Erkan, H.; Korkmaz, A.A.; Acar, Z.; Kul, S.; Hatem, E.; Çelik, Ş. Relation of Epicardial Adipose Tissue With Arterial Compliance and Stiffness in Patients With Hypertension. Angiology 2014, 65, 691–695. [Google Scholar] [CrossRef]
- Liu, Z.; Hu, W.; Zhang, H.; Tao, H.; Lei, P.; Liu, J.; Yu, Y.; Dong, Q.; Gao, L.; Zhang, D. EAT Thickness as a Predominant Feature for Evaluating Arterial Stiffness in Patients with Heart Failure with Preserved Ejection Fraction. Diabetes Metab. Syndr. Obes. 2022, 15, 1217–1226. [Google Scholar] [CrossRef]
- Altin, C.; Sade, L.E.; Gezmis, E.; Yilmaz, M.; Ozen, N.; Muderrisoglu, H. Assessment of Epicardial Adipose Tissue and Carotid/Femoral Intima Media Thickness in Insulin Resistance. J. Cardiol. 2017, 69, 843–850. [Google Scholar] [CrossRef]
- Sen, T.; Tufekcioglu, O.; Ozdemir, M.; Tuncez, A.; Uygur, B.; Golbasi, Z.; Kisacik, H. A New Echocardiographic Parameter of Aortic Stiffness and Atherosclerosis in Patients with Coronary Artery Disease: Aortic Propagation Velocity. J. Cardiol. 2013, 62, 236–240. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Chowienczyk, P.J.; Spector, T.D.; Jiang, B. Relation of Arterial Stiffness to Left Ventricular Structure and Function in Healthy Women. Cardiovasc. Ultrasound 2018, 16, 21. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.-Y.; Chen, D.; Bluemke, D.A.; Wu, C.O.; Teixido-Tura, G.; Chugh, A.; Vasu, S.; Lima, J.A.C.; Hundley, W.G. Evolution of Aortic Wall Thickness and Stiffness with Atherosclerosis: Long-Term Follow up from the Multi-Ethnic Study of Atherosclerosis (MESA). Hypertension 2015, 65, 1015–1019. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Shigematsu, Y.; Hamada, M.; Hiwada, K. Relative Wall Thickness Is an Independent Predictor of Left Ventricular Systolic and Diastolic Dysfunctions in Essential Hypertension. Hypertens. Res. 2001, 24, 493–499. [Google Scholar] [CrossRef] [Green Version]
- Schott, A.; Kluttig, A.; Mikolajczyk, R.; Greiser, K.H.; Werdan, K.; Sedding, D.; Nuding, S. Association of Arterial Stiffness and Heart Failure with Preserved Ejection Fraction in the Elderly Population—Results from the CARLA Study. J. Hum. Hypertens. 2022, 1–9. [Google Scholar] [CrossRef]
- Adam, C.A.; Anghel, R.; Marcu, D.T.M.; Mitu, O.; Roca, M.; Mitu, F. Impact of Sodium–Glucose Cotransporter 2 (SGLT2) Inhibitors on Arterial Stiffness and Vascular Aging—What Do We Know So Far? (A Narrative Review). Life 2022, 12, 803. [Google Scholar] [CrossRef]
- Mehta, S.; Khoury, P.R.; Madsen, N.L.; Dolan, L.M.; Kimball, T.R.; Urbina, E.M. Arterial Thickness and Stiffness Are Independently Associated with Left Ventricular Strain. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2018, 31, 99–104. [Google Scholar] [CrossRef]
- Simons, P.C.G.; Algra, A.; Bots, M.L.; Grobbee, D.E.; van der Graaf, Y. Common Carotid Intima-Media Thickness and Arterial Stiffness. Circulation 1999, 100, 951–957. [Google Scholar] [CrossRef] [Green Version]
- Cecelja, M.; Jiang, B.; Keehn, L.; Hussain, T.; Silva Vieira, M.; Phinikaridou, A.; Greil, G.; Spector, T.D.; Chowienczyk, P. Arterial Stiffening Is a Heritable Trait Associated with Arterial Dilation but Not Wall Thickening: A Longitudinal Study in the Twins UK Cohort. Eur. Heart J. 2018, 39, 2282–2288. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of Clinical Cardiovascular Events With Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Øygarden, H. Carotid Intima-Media Thickness and Prediction of Cardiovascular Disease. J. Am. Heart Assoc. 2017, 6, e005313. [Google Scholar] [CrossRef] [Green Version]
- Paul, J.; Shaw, K.; Dasgupta, S.; Ghosh, M.K. Measurement of Intima Media Thickness of Carotid Artery by B-Mode Ultrasound in Healthy People of India and Bangladesh, and Relation of Age and Sex with Carotid Artery Intima Media Thickness: An Observational Study. J. Cardiovasc. Dis. Res. 2012, 3, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Alvarez, V.; Linares Sánchez, M.; López Alvarez, F.; Suárez Nieto, C.; Mäkitie, A.A.; Olsen, K.D.; Ferlito, A. Evaluation of Intima-Media Thickness and Arterial Stiffness as Early Ultrasound Biomarkers of Carotid Artery Atherosclerosis. Cardiol. Ther. 2022, 11, 231–247. [Google Scholar] [CrossRef]
- Uejima, T.; Dunstan, F.D.; Arbustini, E.; Łoboz-Grudzień, K.; Hughes, A.D.; Carerj, S.; Favalli, V.; Antonini-Canterin, F.; Vriz, O.; Vinereanu, D.; et al. Age-Specific Reference Values for Carotid Arterial Stiffness Estimated by Ultrasonic Wall Tracking. J. Hum. Hypertens. 2020, 34, 214–222. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S. Arterial Wall Hypertrophy and Stiffness in Essential Hypertensive Patients. Hypertension 1995, 26, 355–362. [Google Scholar] [CrossRef]
- Asmar, R. Effects of Pharmacological Intervention on Arterial Stiffness Using Pulse Wave Velocity Measurement. J. Am. Soc. Hypertens. 2007, 1, 104–112. [Google Scholar] [CrossRef]
- Boutouyrie, P.; Laurent, S.; Girerd, X.; Benetos, A.; Lacolley, P.; Abergel, E.; Safar, M. Common Carotid Artery Stiffness and Patterns of Left Ventricular Hypertrophy in Hypertensive Patients. Hypertension 1995, 25, 651–659. [Google Scholar] [CrossRef]
- Fernberg, U.; op ‘t Roodt, J.; Fernström, M.; Hurtig-Wennlöf, A. Body Composition Is a Strong Predictor of Local Carotid Stiffness in Swedish, Young Adults—The Cross Sectional Lifestyle, Biomarkers, and Atherosclerosis Study. BMC Cardiovasc. Disord. 2019, 19, 205. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Obese Patients (n = 25) | Non-Obese Patients (n = 25) | p | |
|---|---|---|---|
| Demographics, antropometric and hemodynamic parameters | |||
| Age (y) | 39.24 ± 8.74 | 43.36 ± 13.9 | 0.021 |
| Female sex (%) | 21 (84%) | 17 (68%) | - |
| BMI (kg/m2) | 43.9 ± 6.07 | 24.24 ± 3.15 | 0.0001 |
| Systolic blood pressure (mmHg) | 129.36 ± 13.03 | 118.04 ± 11.72 | 0.002 |
| Diastolic blood pressure (mmHg) | 75.28 ± 11.12 | 67.08 ± 7.89 | 0.004 |
| Pulse pressure (mmHg) | 59.08 ± 11.28 | 51.32 ± 9.98 | 0.013 |
| Biological parameters | |||
| Fasting glucose (mg/dL) | 99.28 ± 14.62 | 88.32 ± 8.80 | 0.002 |
| Insulinemia (µU/mL) | 24.47 ± 6.16 | 8.23 ± 7.98 | 0.0004 |
| Insulin sensitivity* | 6.45 ± 3.73 | 1.82 ± 1.87 | 0.0001 |
| Insulin resistance (M/mU/l) | 0.13 ± 0.02 | 0.16 ± 0.12 | 0.001 |
| Uric acid (mg/dL) | 6.79 ± 2.19 | 5.29 ± 1.48 | 0.006 |
| Arterial stiffness parameters | |||
| Aortic AIx (%) | 24.1 ± 12.1 | 35.1 ± 16.2 | 0.090 |
| Brachial AIx (%) | −26.7 ± 0.24 | −5.5 ± 0.32 | 0.110 |
| Aortic SBP (mmHg) | 128.74 ± 20.81 | 119.42 ± 20.18 | 0.114 |
| Aortic PP (mmHg) | 52.26 ± 10.76 | 50.66 ± 12.69 | 0.633 |
| DRA | 49.68 ± 11.38 | 45.32 ± 18.82 | 0.321 |
| SAI (%) | 48.82 ± 3.81 | 46.41 ± 6.36 | 0.112 |
| DAI (%) | 51.28 ± 3.80 | 53.61 ± 6.06 | 0.111 |
| SEVR | 1.06 ± 0.16 | 1.19 ± 0.28 | 0.054 |
| PWVAo (m/s) | 9.59 ± 2.38 | 8.92 ± 2.14 | 0.305 |
| Perivisceral adipose tissue parameters | |||
| Adipocyte size (µm) | 9.34 ± 2.11 | 6.62 ± 1.78 | 0.027 |
| Blood vessel wall thickness (µm) | 8.79 ± 2.12 | 6.92 ± 1.48 | 0.0001 |
| Echocardiographic data | |||
| LV mass index (g/m2) | 75.10 ± 18.85 | 70.25 ± 12.16 | 0.2851 |
| Aortic ring (mm) | 17.20 ± 1.50 | 17.36 ± 3.13 | 0.7112 |
| LVEF (%) | 60.72 ± 5.49 | 64.40 ± 3.51 | 0.0073 |
| Epicardial fat thickness (mm) | 0.53 ± 0.13 | 0.32 ± 0.08 | 0.0001 |
| LV diastole diameter (mm) | 50.44 ± 4.38 | 44.48 ± 3.22 | 0.0001 |
| LV posterior wall (mm) | 9.19 ± 1.48 | 8.10 ± 0.78 | 0.0024 |
| Interventricular septum (mm) | 10.10 ± 1.59 | 9.02 ± 1.20 | 0.0096 |
| Relative wall thickness | 0.37 ± 0.06 | 0.37 ± 0.04 | 0.9702 |
| Carotid Doppler Ultrasound | |||
| Carotid intima–media thickness (mm) | 0.72 ± 0.21 | 0.57 ± 0.07 | 0.0033 |
| Systolic thickness of the media (mm) | 7.19 ± 1.05 | 6.78 ± 0.58 | 0.0888 |
| Diastolic thickness of the media (mm) | 6.75 ± 0.72 | 6.27 ± 0.63 | 0.0159 |
| Relative wall thickness | 0.21 ± 0.06 | 0.18 ± 0.03 | 0.0295 |
| Wall-to-lumen thickness ratio | 0.12 ± 0.04 | 0.11 ± 0.02 | 0.0930 |
| Carotid cross-sectional area (mm2) | 20.05 ± 7.68 | 14.98 ± 2.82 | 0.0042 |
| Patients with Morbid Obesity | ||||
|---|---|---|---|---|
| Parameters | Chemerin | Chemerin/Adiponectin Ratio | ||
| r | p | r | p | |
| Echocardiographic data | ||||
| LV mass index (g/m2) | 0.373 | 0.072 | 0.319 | 0.120 |
| Aortic ring (mm) | 0.283 | 0.202 | 0.365 | 0.086 |
| LVEF (%) | −0.044 | 0.839 | 0.103 | 0.626 |
| Epicardial adipose tissue thickness (mm) | 0.198 | 0.354 | 0.030 | 0.886 |
| Carotid Doppler Ultrasound | ||||
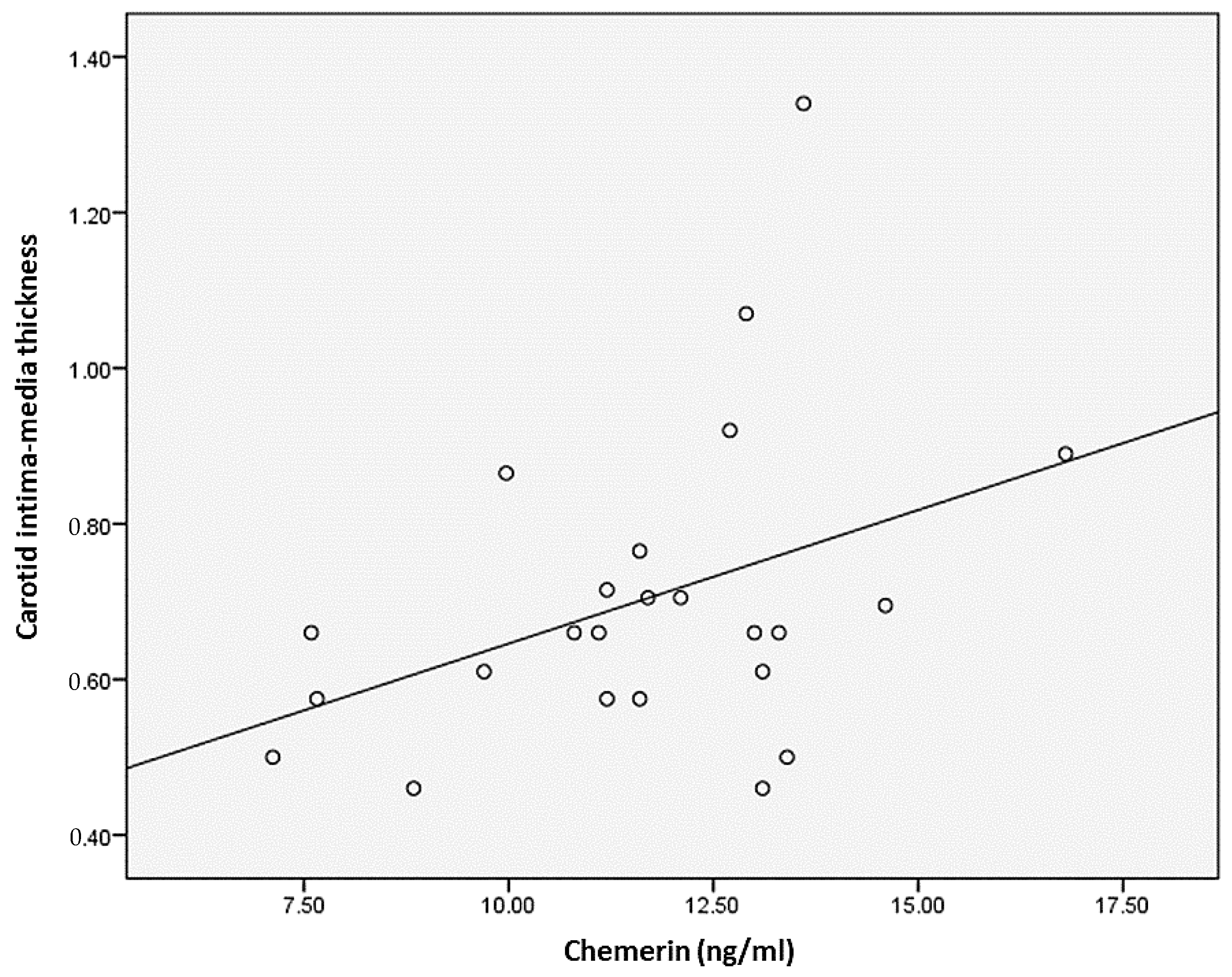
| Carotid intima–media thickness (mm) | 0.404 | 0.050 | 0.447 | 0.025 |
| Systolic thickness of the media (mm) | 0.492 | 0.015 | 0.480 | 0.015 |
| Diastolic thickness of the media (mm) | 0.620 | 0.001 | 0.480 | 0.015 |
| Relative wall thickness | 0.165 | 0.441 | 0.286 | 0.166 |
| Wall-to-lumen thickness ratio | 0.106 | 0.632 | 0.246 | 0.247 |
| Carotid cross-sectional area (mm2) | 0.045 | 0.834 | 0.320 | 0.119 |
| Non-Obese Patients | Patients with Morbid Obesity | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameters | Adipocyte Size | Blood Vessel Wall Thickness | Adipocyte Size | Blood Vessel Wall Thickness | ||||
| r | p | r | p | r | p | r | p | |
| Echocardiographic data | ||||||||
| LV mass index (g/m2) | −0.220 | 0.123 | 0.218 | 0.128 | −0.217 | 0.129 | 0.380 | 0.008 |
| Aortic ring (mm) | −0.147 | 0.336 | 0.093 | 0.547 | 0.132 | 0.402 | 0.273 | 0.084 |
| LVEF (%) | 0.234 | 0.135 | −0.135 | 0.390 | 0.177 | 0.241 | −0.007 | 0.962 |
| Epicardial adipose tissue thickness (mm) | −0.14 | 0.925 | 0.044 | 0.761 | 0.242 | 0.092 | −0.057 | 0.691 |
| Carotid Doppler Ultrasound | ||||||||
| Carotid intima–media thickness | −0.059 | 0.689 | 0.167 | 0.258 | 0.206 | 0.158 | 0.257 | 0.078 |
| Systolic thickness of the media | −0.104 | 0.468 | 0.149 | 0.303 | 0.13 | 0.925 | 0.372 | 0.009 |
| Diastolic thickness of the media | −0.132 | 0.361 | −0.007 | 0.963 | −0.060 | 0.674 | 0.385 | 0.007 |
| Relative wall thickness | 0.00 | 0.889 | 0.050 | 0.726 | 0.324 | 0.023 | 0.093 | 0.513 |
| Wall-to-lumen thickness ratio | −0.043 | 0.761 | 0.047 | 0.743 | 0.210 | 0.141 | 0.153 | 0.283 |
| Carotid cross-sectional area | −0.130 | 0.362 | 0.047 | 0.743 | 0.023 | 0.870 | 0.473 | 0.001 |
| Dependent Variable | Independent Variable | Coefficient | p-Value | p-Value Model | R2 Adjusted |
|---|---|---|---|---|---|
| Adipocyte size | Constant | −2.021 | 0.543 | 0.0001 | 0.73 |
| Chemerine/adiponectine ratio | 0.379 | 0.858 | |||
| Triglycerides | 0.015 | 0.001 | |||
| SEVR | 6.198 | 0.001 | |||
| Carotid cross-sectional area | 0.085 | 0.025 | |||
| Epicardial fat thickness | 6.724 | 0.008 | |||
| Carotid intima–media thickness | Constant | −0.691 | 0.007 | 0.0001 | 0.61 |
| Adipocyte size | 0.035 | 0.014 | |||
| Blood vessel wall thickness | 0.007 | 0.645 | |||
| Diastolic thickness of the media | 0.09 | 0.007 | |||
| Wall-to-lumen thickness ratio | 2.995 | 0.001 | |||
| PWVAo | Constant | 5.712 | 0.032 | 0.0001 | |
| Adipocyte size | 0.065 | 0.422 | |||
| Blood vessel wall thickness | 0.077 | 0.294 | |||
| Waist circumference | 0.063 | 0.001 | 0.91 | ||
| White blood cells | 0 | 0.003 | |||
| TNF-α | 0.11 | 0.042 | |||
| SEVR | Constant | 2.985 | 0.000001 | 0.0001 | 0.99 |
| Adipocyte size | 0.003 | 0.052 | |||
| Blood vessel wall thickness | −0.002 | 0.115 | |||
| Waist circumference | 0.001 | 0.043 | |||
| Basophils | 0.062 | 0.003 | |||
| Serum fibrinogen | 0 | 0.023 | |||
| Serum creatinine | 0.077 | 0.011 | |||
| Insulin sensitivity | 0.687 | 0.009 | |||
| SAI | −0.043 | 0.000001 | |||
| Aortic Aix | Constant | 65.554 | 0.009 | 0.0001 | 0.85 |
| Adipocyte size | 1.653 | 0.011 | |||
| Blood vessel wall thickness | −0.547 | 0.415 | |||
| HDL cholesterol | 0.398 | 0.016 | |||
| Heart rate | −0.542 | 0.003 | |||
| DRA | −0.569 | 0.000001 | |||
| LV mass index | 0.503 | 0.000001 | |||
| Ao ring dimmensions | −2.377 | 0.007 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Onofrei, V.A.; Zamfir, C.L.; Anisie, E.; Ceasovschih, A.; Constantin, M.; Mitu, F.; Adam, C.A.; Grigorescu, E.-D.; Petroaie, A.D.; Timofte, D. Determinants of Arterial Stiffness in Patients with Morbid Obesity. The Role of Echocardiography and Carotid Ultrasound Imaging. Medicina 2023, 59, 428. https://doi.org/10.3390/medicina59030428
Onofrei VA, Zamfir CL, Anisie E, Ceasovschih A, Constantin M, Mitu F, Adam CA, Grigorescu E-D, Petroaie AD, Timofte D. Determinants of Arterial Stiffness in Patients with Morbid Obesity. The Role of Echocardiography and Carotid Ultrasound Imaging. Medicina. 2023; 59(3):428. https://doi.org/10.3390/medicina59030428
Chicago/Turabian StyleOnofrei, Viviana Aursulesei, Carmen Lacramioara Zamfir, Ecaterina Anisie, Alexandr Ceasovschih, Mihai Constantin, Florin Mitu, Cristina Andreea Adam, Elena-Daniela Grigorescu, Antoneta Dacia Petroaie, and Daniel Timofte. 2023. "Determinants of Arterial Stiffness in Patients with Morbid Obesity. The Role of Echocardiography and Carotid Ultrasound Imaging" Medicina 59, no. 3: 428. https://doi.org/10.3390/medicina59030428
APA StyleOnofrei, V. A., Zamfir, C. L., Anisie, E., Ceasovschih, A., Constantin, M., Mitu, F., Adam, C. A., Grigorescu, E. -D., Petroaie, A. D., & Timofte, D. (2023). Determinants of Arterial Stiffness in Patients with Morbid Obesity. The Role of Echocardiography and Carotid Ultrasound Imaging. Medicina, 59(3), 428. https://doi.org/10.3390/medicina59030428