
Treatment Nonadherence among Multimorbid Chronic Disease Patients: Evidence from 3515 Subjects in Indonesia

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
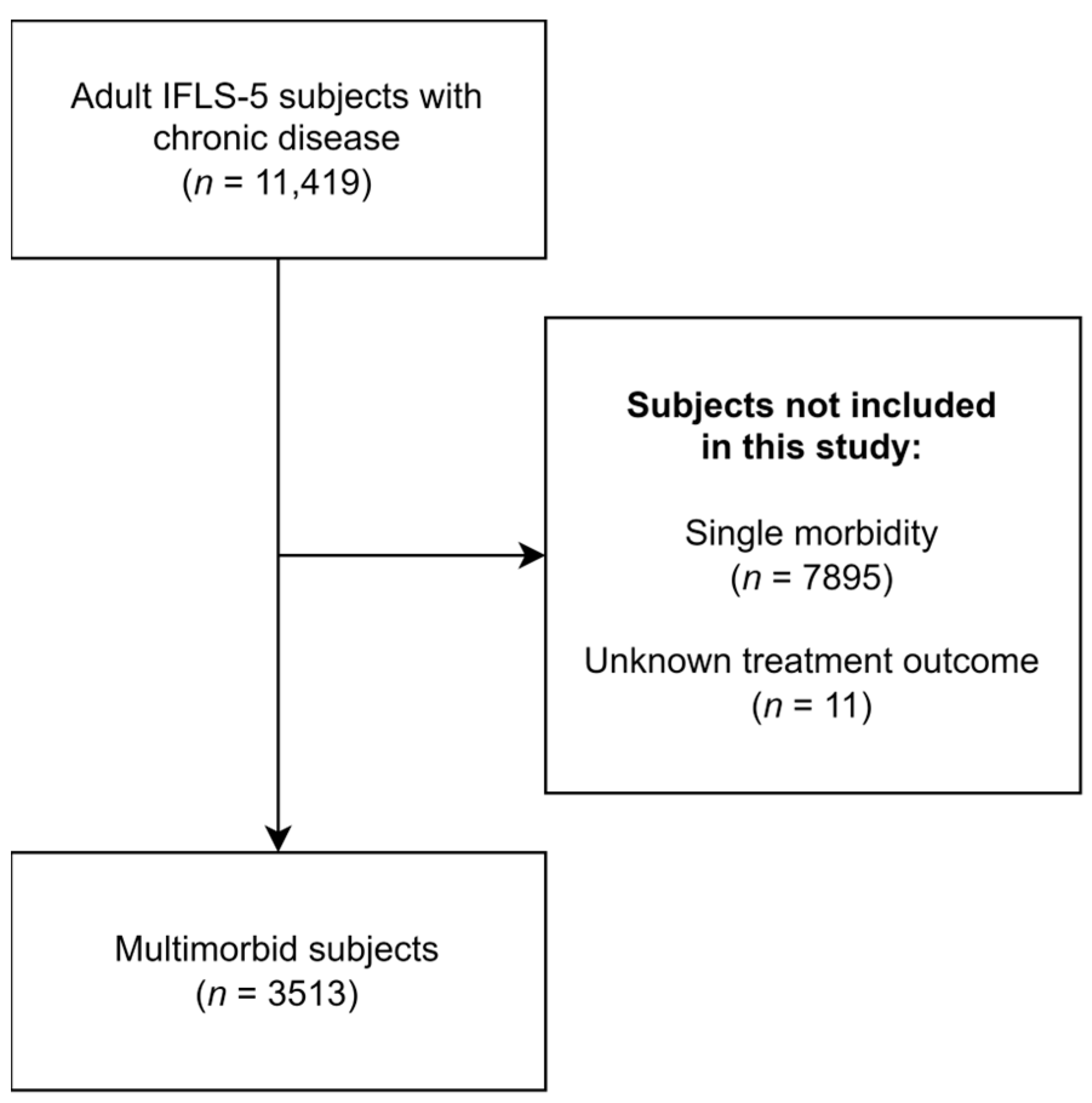
2.1. Study Design and Participants
2.2. Variables and Measures
2.3. Data Analysis
3. Results
4. Discussion
4.1. Multimorbidity Prevalence
4.2. Treatment Nonadherence among Multimorbid Patients
5. Study Implications
6. Strengths and Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 95% CI | 95% confidence interval |
| aOR | Adjusted odds ratio |
| BMI | Body mass index |
| IFLS | Indonesian Family Life Survey project: A longitudinal household survey initiated by RAND Corporation |
| IDR | Indonesian Rupiah |
| IFLS-4 | The fourth Indonesian Family Life Survey, conducted in 2007/2008 |
| IFLS-5 | The fifth Indonesian Family Life Survey, conducted in 2014/2015 |
| OR | Odds ratio |
| STROBE | Strengthening the Reporting of Observational Studies in Epidemiology |
| USD | United States Dollar |
References
- Academy of Medical Sciences. Multimorbidity: A Priority for Global Health Research; Academy of Medical Sciences: London, UK, 2018. [Google Scholar]
- Siswati, T.; Paramashanti, B.A.; Rialihanto, M.P.; Waris, L. Epidemiological Transition in Indonesia and Its Prevention: A Narrative Review. J. Complement. Altern. Med. Res. 2022, 18, 50–60. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.A.; Huxley, R.R.; Al Mamun, A. Multimorbidity Prevalence and Pattern in Indonesian Adults: An Exploratory Study Using National Survey Data. BMJ Open 2015, 5, e009810. [Google Scholar] [CrossRef]
- World Health Organization. Political Declaration of the Third High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Wolff, J.L.; Starfield, B.; Anderson, G. Prevalence, Expenditures, and Complications of Multiple Chronic Conditions in the Elderly. Arch. Intern. Med. 2002, 162, 2269. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Poblador-Plou, B.; González-Rubio, F.; Gimeno-Feliu, L.A.; Abad-Díez, J.M.; Prados-Torres, A. Multimorbidity, Polypharmacy, Referrals, and Adverse Drug Events: Are We Doing Things Well? Br. J. Gen. Pract. 2012, 62, e821–e826. [Google Scholar] [CrossRef] [PubMed]
- Marengoni, A.; Onder, G. Guidelines, Polypharmacy, and Drug-Drug Interactions in Patients with Multimorbidity. BMJ 2015, 350, h1059. [Google Scholar] [CrossRef]
- Kadam, U.; Croft, P. North Staffordshire GP Consortium Group Clinical Multimorbidity and Physical Function in Older Adults: A Record and Health Status Linkage Study in General Practice. Fam. Pract. 2007, 24, 412–419. [Google Scholar] [CrossRef]
- Arokiasamy, P.; Uttamacharya, U.; Jain, K.; Biritwum, R.B.; Yawson, A.E.; Wu, F.; Guo, Y.; Maximova, T.; Espinoza, B.M.; Salinas Rodríguez, A.; et al. The Impact of Multimorbidity on Adult Physical and Mental Health in Low- and Middle-Income Countries: What Does the Study on Global Ageing and Adult Health (SAGE) Reveal? BMC Med. 2015, 13, 178. [Google Scholar] [CrossRef] [PubMed]
- Ramond-Roquin, A.; Haggerty, J.; Lambert, M.; Almirall, J.; Fortin, M. Different Multimorbidity Measures Result in Varying Estimated Levels of Physical Quality of Life in Individuals with Multimorbidity: A Cross-Sectional Study in the General Population. BioMed Res. Int. 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Wei, M.Y.; Kawachi, I.; Okereke, O.I.; Mukamal, K.J. Diverse Cumulative Impact of Chronic Diseases on Physical Health–Related Quality of Life: Implications for a Measure of Multimorbidity. Am. J. Epidemiol. 2016, 184, 357–365. [Google Scholar] [CrossRef]
- Marthias, T.; Anindya, K.; Ng, N.; McPake, B.; Atun, R.; Arfyanto, H.; Hulse, E.S.; Zhao, Y.; Jusril, H.; Pan, T.; et al. Impact of Non-Communicable Disease Multimorbidity on Health Service Use, Catastrophic Health Expenditure and Productivity Loss in Indonesia: A Population-Based Panel Data Analysis Study. BMJ Open 2021, 11, e041870. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Si, L.; Cocker, F.; Palmer, A.J.; Sanderson, K. A Systematic Review of Cost-of-Illness Studies of Multimorbidity. Appl. Health Econ. Health Policy 2018, 16, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Sum, G.; Hone, T.; Atun, R.; Millett, C.; Suhrcke, M.; Mahal, A.; Koh, G.C.-H.; Lee, J.T. Multimorbidity and Out-of-Pocket Expenditure on Medicines: A Systematic Review. BMJ Glob. Health 2018, 3, e000505. [Google Scholar] [CrossRef] [PubMed]
- Anindya, K.; Ng, N.; Atun, R.; Marthias, T.; Zhao, Y.; McPake, B.; Van Heusden, A.; Pan, T.; Lee, J.T. Effect of Multimorbidity on Utilisation and Out-of-Pocket Expenditure in Indonesia: Quantile Regression Analysis. BMC Health Serv. Res. 2021, 21, 427. [Google Scholar] [CrossRef] [PubMed]
- Tran, P.B.; Kazibwe, J.; Nikolaidis, G.F.; Linnosmaa, I.; Rijken, M.; Van Olmen, J. Costs of Multimorbidity: A Systematic Review and Meta-Analyses. BMC Med. 2022, 20, 234. [Google Scholar] [CrossRef] [PubMed]
- Husnayain, A.; Ekadinata, N.; Sulistiawan, D.; Chia-Yu Su, E. Multimorbidity Patterns of Chronic Diseases among Indonesians: Insights from Indonesian National Health Insurance (INHI) Sample Data. Int. J. Environ. Res. Public Health 2020, 17, 8900. [Google Scholar] [CrossRef] [PubMed]
- Sabaté, E. Adherence to Long-Term Therapies: Evidence for Action; World Health Organization: Geneva, Switzerland, 2003; ISBN 978-92-4-154599-0. [Google Scholar]
- Walsh, C.A.; Cahir, C.; Tecklenborg, S.; Byrne, C.; Culbertson, M.A.; Bennett, K.E. The Association between Medication Non-adherence and Adverse Health Outcomes in Ageing Populations: A Systematic Review and Meta-analysis. Br. J. Clin. Pharmacol. 2019, 85, 2464–2478. [Google Scholar] [CrossRef] [PubMed]
- Cutler, R.L.; Fernandez-Llimos, F.; Frommer, M.; Benrimoj, C.; Garcia-Cardenas, V. Economic Impact of Medication Non-Adherence by Disease Groups: A Systematic Review. BMJ Open 2018, 8, e016982. [Google Scholar] [CrossRef] [PubMed]
- Foley, L.; Larkin, J.; Lombard-Vance, R.; Murphy, A.W.; Hynes, L.; Galvin, E.; Molloy, G.J. Prevalence and Predictors of Medication Non-Adherence among People Living with Multimorbidity: A Systematic Review and Meta-Analysis. BMJ Open 2021, 11, e044987. [Google Scholar] [CrossRef]
- Zelko, E.; KlemencKetis, Z.; TusekBunc, K. Medication Adherence in Elderly with Polypharmacy Living at Home: A Systematic Review of Existing Studies. Mater. Socio Medica 2016, 28, 129. [Google Scholar] [CrossRef]
- Maffoni, M.; Traversoni, S.; Costa, E.; Midão, L.; Kardas, P.; Kurczewska-Michalak, M.; Giardini, A. Medication Adherence in the Older Adults with Chronic Multimorbidity: A Systematic Review of Qualitative Studies on Patient’s Experience. Eur. Geriatr. Med. 2020, 11, 369–381. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Multimorbidity; Technical Series on Safer Primary Care; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-151165-0. [Google Scholar]
- Williams, A.; Manias, E.; Walker, R. Interventions to Improve Medication Adherence in People with Multiple Chronic Conditions: A Systematic Review. J. Adv. Nurs. 2008, 63, 132–143. [Google Scholar] [CrossRef] [PubMed]
- RAND Corporation. The Indonesian Family Life Survey. Available online: https://www.rand.org/well-being/social-and-behavioral-policy/data/FLS/IFLS.html (accessed on 6 October 2023).
- Strauss, J.; Witoelar, F.; Sikoki, B. The Fifth Wave of the Indonesia Family Life Survey: Overview and Field Report: Volume 1; RAND Corporation: Santa Monica, CA, USA, 2016. [Google Scholar]
- Strauss, J.; Witoelar, F.; Sikoki, B. User’s Guide for the Indonesia Family Life Survey, Wave 5: Volume 2; RAND Corporation: Santa Monica, CA, USA, 2016. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- National Institutes of Health. Managing Overweight and Obesity in Adults: Systematic Evidence Review from the Expert Panel; National Institutes of Health: Bethesda, MD, USA, 2013.
- Madley-Dowd, P.; Hughes, R.; Tilling, K.; Heron, J. The Proportion of Missing Data Should Not Be Used to Guide Decisions on Multiple Imputation. J. Clin. Epidemiol. 2019, 110, 63–73. [Google Scholar] [CrossRef] [PubMed]
- IBM Corporation. IBM SPSS Statistics for Windows; IBM Corporation: Armonk, NY, USA, 2013. [Google Scholar]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Muggah, E.; Graves, E.; Bennett, C.; Manuel, D.G. Ascertainment of Chronic Diseases Using Population Health Data: A Comparison of Health Administrative Data and Patient Self-Report. BMC Public Health 2013, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Kriegsman, D.M.W.; Penninx, B.W.J.H.; Van Eijk, J.T.M.; Boeke, A.J.P.; Deeg, D.J.H. Self-Reports and General Practitioner Information on the Presence of Chronic Diseases in Community Dwelling Elderly. J. Clin. Epidemiol. 1996, 49, 1407–1417. [Google Scholar] [CrossRef] [PubMed]
- Frost, M.; Wraae, K.; Gudex, C.; Nielsen, T.; Brixen, K.; Hagen, C.; Andersen, M. Chronic Diseases in Elderly Men: Underreporting and Underdiagnosis. Age Ageing 2012, 41, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.; Manolova, G.; Daskalopoulou, C.; Vitoratou, S.; Prince, M.; Prina, A.M. Prevalence of Multimorbidity in Community Settings: A Systematic Review and Meta-Analysis of Observational Studies. J. Comorbidity 2019, 9, 2235042X1987093. [Google Scholar] [CrossRef]
- Chowdhury, S.R.; Chandra Das, D.; Sunna, T.C.; Beyene, J.; Hossain, A. Global and Regional Prevalence of Multimorbidity in the Adult Population in Community Settings: A Systematic Review and Meta-Analysis. eClinicalMedicine 2023, 57, 101860. [Google Scholar] [CrossRef]
- Kokubo, Y.; Iwashima, Y. Higher Blood Pressure as a Risk Factor for Diseases Other Than Stroke and Ischemic Heart Disease. Hypertension 2015, 66, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Levy, P.D.; Cline, D. Asymptomatic Hypertension in the Emergency Department: A Matter of Critical Public Health Importance. Acad. Emerg. Med. 2009, 16, 1251–1257. [Google Scholar] [CrossRef] [PubMed]
- Agustina, R.; Dartanto, T.; Sitompul, R.; Susiloretni, K.A.; Suparmi; Achadi, E.L.; Taher, A.; Wirawan, F.; Sungkar, S.; Sudarmono, P.; et al. Universal Health Coverage in Indonesia: Concept, Progress, and Challenges. Lancet 2019, 393, 75–102. [Google Scholar] [CrossRef] [PubMed]
- Alkaff, F.F.; Illavi, F.; Salamah, S.; Setiyawati, W.; Ramadhani, R.; Purwantini, E.; Tahapary, D.L. The Impact of the Indonesian Chronic Disease Management Program (PROLANIS) on Metabolic Control and Renal Function of Type 2 Diabetes Mellitus Patients in Primary Care Setting. J. Prim. Care Community Health 2021, 12, 215013272098440. [Google Scholar] [CrossRef] [PubMed]
- Alkaff, F.F.; Sukmajaya, W.P.; Intan, R.E.; Salamah, S. Effectivity of Indonesia Chronic Disease Management Program (PROLANIS) to Control Hypertension and Its Comorbidities at Primary Health Care: Effectivity of PROLANIS to Control Hypertension. Open Access Maced. J. Med. Sci. 2020, 8, 224–227. [Google Scholar] [CrossRef]
- Schröders, J.; Wall, S.; Hakimi, M.; Dewi, F.S.T.; Weinehall, L.; Nichter, M.; Nilsson, M.; Kusnanto, H.; Rahajeng, E.; Ng, N. How Is Indonesia Coping with Its Epidemic of Chronic Noncommunicable Diseases? A Systematic Review with Meta-Analysis. PLoS ONE 2017, 12, e0179186. [Google Scholar] [CrossRef] [PubMed]
- Walsh, C.A.; Bennett, K.E.; Wallace, E.; Cahir, C. Identifying Adherence Patterns Across Multiple Medications and Their Association with Health Outcomes in Older Community-Dwelling Adults with Multimorbidity. Value Health 2020, 23, 1063–1071. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Bennett, K.; Wallace, E.; Fahey, T.; Cahir, C. Measuring Medication Adherence in Older Community-Dwelling Patients with Multimorbidity. Eur. J. Clin. Pharmacol. 2018, 74, 357–364. [Google Scholar] [CrossRef]
- Félix, I.B.; Henriques, A. Medication Adherence and Related Determinants in Older People with Multimorbidity: A Cross-sectional Study. Nurs. Forum 2021, 56, 834–843. [Google Scholar] [CrossRef]
- Almutairi, A.S.; Alhazmi, T.M.; Alotaibi, Y.H.; Alfraidi, A.A.; Alsaad, A.M.; Matrood, R.A.; Al-khatir, A.N.; Alsubaie, A.A.; Alotibi, W.M. Medication Adherence Among Multimorbid Patients with Polypharmacy and Its Relation to Social Support at National Guard Primary Health Care Centers, Riyadh. Cureus 2022, 14, e30679. [Google Scholar] [CrossRef]
- González-Bueno, J.; Sevilla-Sánchez, D.; Puigoriol-Juvanteny, E.; Molist-Brunet, N.; Codina-Jané, C.; Espaulella-Panicot, J. Factors Associated with Medication Non-Adherence among Patients with Multimorbidity and Polypharmacy Admitted to an Intermediate Care Center. Int. J. Environ. Res. Public Health 2021, 18, 9606. [Google Scholar] [CrossRef] [PubMed]
- Inauen, J.; Bierbauer, W.; Lüscher, J.; König, C.; Tobias, R.; Ihle, A.; Zimmerli, L.; Holzer, B.M.; Battegay, E.; Siebenhüner, K.; et al. Assessing Adherence to Multiple Medications and in Daily Life among Patients with Multimorbidity. Psychol. Health 2017, 32, 1233–1248. [Google Scholar] [CrossRef] [PubMed]
- Schüz, B.; Marx, C.; Wurm, S.; Warner, L.M.; Ziegelmann, J.P.; Schwarzer, R.; Tesch-Römer, C. Medication Beliefs Predict Medication Adherence in Older Adults with Multiple Illnesses. J. Psychosom. Res. 2011, 70, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Afshar, S.; Roderick, P.J.; Kowal, P.; Dimitrov, B.D.; Hill, A.G. Multimorbidity and the Inequalities of Global Ageing: A Cross-Sectional Study of 28 Countries Using the World Health Surveys. BMC Public Health 2015, 15, 776. [Google Scholar] [CrossRef] [PubMed]
- Van Den Akker, M.; Dieckelmann, M.; Hussain, M.A.; Bond-Smith, D.; Muth, C.; Pati, S.; Saxena, S.; Silva, D.; Skoss, R.; Straker, L.; et al. Children and Adolescents Are Not Small Adults: Toward a Better Understanding of Multimorbidity in Younger Populations. J. Clin. Epidemiol. 2022, 149, 165–171. [Google Scholar] [CrossRef]
- Whitty, C.J.M.; MacEwen, C.; Goddard, A.; Alderson, D.; Marshall, M.; Calderwood, C.; Atherton, F.; McBride, M.; Atherton, J.; Stokes-Lampard, H.; et al. Rising to the Challenge of Multimorbidity. BMJ 2020, 368, l6964. [Google Scholar] [CrossRef] [PubMed]
- Pai, A.; Ostendorf, H.M. Treatment Adherence in Adolescents and Young Adults Affected by Chronic Illness during the Health Care Transition from Pediatric to Adult Health Care: A Literature Review. Child. Health Care 2011, 40, 16–33. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Drew, S.; Yeo, M.S.; Britto, M.T. Adolescents with a Chronic Condition: Challenges Living, Challenges Treating. Lancet 2007, 369, 1481–1489. [Google Scholar] [CrossRef] [PubMed]
- Venning, A.; Eliott, J.; Wilson, A.; Kettler, L. Understanding Young Peoples’ Experience of Chronic Illness: A Systematic Review. Int. J. Evid. Based Healthc. 2008, 6, 321–336. [Google Scholar] [CrossRef]
- Sinaga, I.O.Y.; Barliana, M.I.; Pradipta, I.S.; Iskandarsyah, A.; Abdulah, R.; Alfian, S.D. Depression Is Associated with the Increase Risk of Multimorbidity Among the General Population in Indonesia. J. Multidiscip. Healthc. 2022, 15, 1863–1870. [Google Scholar] [CrossRef]
- Fortin, M. Psychological Distress and Multimorbidity in Primary Care. Ann. Fam. Med. 2006, 4, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Cavalcanti, G.; Doring, M.; Portella, M.R.; Bortoluzzi, E.C.; Mascarelo, A.; Dellani, M.P. Multimorbidity Associated with Polypharmacy and Negative Self-Perception of Health. Rev. Bras. Geriatr. E Gerontol. 2017, 20, 634–642. [Google Scholar] [CrossRef]
- Kolling, M.; Winkley, K.; Von Deden, M. “For Someone Who’s Rich, It’s Not a Problem”. Insights from Tanzania on Diabetes Health-Seeking and Medical Pluralism among Dar Es Salaam’s Urban Poor. Glob. Health 2010, 6, 8. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.; Schlundt, D.; Larson, C.; Wang, H.; Brown, A.; Hargreaves, M. Chronic Illness and Smoking Cessation. Nicotine Tob. Res. 2009, 11, 933–939. [Google Scholar] [CrossRef] [PubMed]
- Kalkhoran, S.; Kruse, G.R.; Chang, Y.; Rigotti, N.A. Smoking-Cessation Efforts by US Adult Smokers with Medical Comorbidities. Am. J. Med. 2018, 131, 318.e1–318.e8. [Google Scholar] [CrossRef] [PubMed]
- Gwaltney, C.J.; Metrik, J.; Kahler, C.W.; Shiffman, S. Self-Efficacy and Smoking Cessation: A Meta-Analysis. Psychol. Addict. Behav. 2009, 23, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Martinez, E.; Tatum, K.L.; Glass, M.; Bernath, A.; Ferris, D.; Reynolds, P.; Schnoll, R.A. Correlates of Smoking Cessation Self-Efficacy in a Community Sample of Smokers. Addict. Behav. 2010, 35, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Galvin, K.T. A Critical Review of the Health Belief Model in Relation to Cigarette Smoking Behaviour. J. Clin. Nurs. 1992, 1, 13–18. [Google Scholar] [CrossRef]
- Friis, K.; Lasgaard, M.; Pedersen, M.H.; Duncan, P.; Maindal, H.T. Health Literacy, Multimorbidity, and Patient-Perceived Treatment Burden in Individuals with Cardiovascular Disease. A Danish Population-Based Study. Patient Educ. Couns. 2019, 102, 1932–1938. [Google Scholar] [CrossRef]
- Rosenstock, I.M. The Health Belief Model and Preventive Health Behavior. Health Educ. Monogr. 1974, 2, 354–386. [Google Scholar] [CrossRef]
- Wang, T.; Wang, H.; Zeng, Y.; Cai, X.; Xie, L. Health Beliefs Associated with Preventive Behaviors against Noncommunicable Diseases. Patient Educ. Couns. 2022, 105, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Widayanti, A.W.; Green, J.A.; Heydon, S.; Norris, P. Health-Seeking Behavior of People in Indonesia: A Narrative Review. J. Epidemiol. Glob. Health 2020, 10, 6–15. [Google Scholar] [CrossRef]
- Foley, L.; Hynes, L.; Murphy, A.W.; Molloy, G.J. ‘Just Keep Taking Them, Keep Hoping They’Ll Work’: A Qualitative Study of Adhering to Medications for Multimorbidity. Br. J. Health Psychol. 2022, 27, 691–715. [Google Scholar] [CrossRef] [PubMed]
- Duguay, C.; Gallagher, F.; Fortin, M. The Experience of Adults with Multimorbidity: A Qualitative Study. J. Comorbidity 2014, 4, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Zhu, S.; Lee, D.T.F.; Chair, S.Y. Interventions for Improving Medication Adherence in Community-Dwelling Older People with Multimorbidity: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2022, 126, 104154. [Google Scholar] [CrossRef] [PubMed]
- González-Bueno, J.; Sevilla-Sánchez, D.; Puigoriol-Juvanteny, E.; Molist-Brunet, N.; Codina-Jané, C.; Espaulella-Panicot, J. Improving Medication Adherence and Effective Prescribing through a Patient-Centered Prescription Model in Patients with Multimorbidity. Eur. J. Clin. Pharmacol. 2022, 78, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.U.; Sherifali, D.; Fitzpatrick-Lewis, D.; Kenny, M.; Lamarche, L.; Raina, P.; Mangin, D. Interventions to Address Polypharmacy in Older Adults Living with Multimorbidity: Review of Reviews. Can. Fam. Physician 2022, 68, e215–e226. [Google Scholar] [CrossRef] [PubMed]
- Ulley, J.; Harrop, D.; Ali, A.; Alton, S.; Fowler Davis, S. Deprescribing Interventions and Their Impact on Medication Adherence in Community-Dwelling Older Adults with Polypharmacy: A Systematic Review. BMC Geriatr. 2019, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Payne, R.A.; Avery, A.J.; Duerden, M.; Saunders, C.L.; Simpson, C.R.; Abel, G.A. Prevalence of Polypharmacy in a Scottish Primary Care Population. Eur. J. Clin. Pharmacol. 2014, 70, 575–581. [Google Scholar] [CrossRef]
- Lozano-Hernández, C.M.; López-Rodríguez, J.A.; Leiva-Fernández, F.; Calderón-Larrañaga, A.; Barrio-Cortes, J.; Gimeno-Feliu, L.A.; Poblador-Plou, B.; Cura-González, I.D.; MULTIPAP GROUP. Social Support, Social Context and Nonadherence to Treatment in Young Senior Patients with Multimorbidity and Polypharmacy Followed-up in Primary Care. MULTIPAP Study. PLoS ONE 2020, 15, e0235148. [Google Scholar] [CrossRef]
- Giardini, A.; Maffoni, M.; Kardas, P.; Costa, E. A Cornerstone of Healthy Aging: Do We Need to Rethink the Concept of Adherence in the Elderly? Patient Prefer. Adherence 2018, 12, 1003–1005. [Google Scholar] [CrossRef] [PubMed]
- The Shed-MEDS Team; Vasilevskis, E.E.; Shah, A.S.; Hollingsworth, E.K.; Shotwell, M.S.; Mixon, A.S.; Bell, S.P.; Kripalani, S.; Schnelle, J.F.; Simmons, S.F. A Patient-Centered Deprescribing Intervention for Hospitalized Older Patients with Polypharmacy: Rationale and Design of the Shed-MEDS Randomized Controlled Trial. BMC Health Serv. Res. 2019, 19, 165. [Google Scholar] [CrossRef]
- Laferton, J.A.C.; Kube, T.; Salzmann, S.; Auer, C.J.; Shedden-Mora, M.C. Patients’ Expectations Regarding Medical Treatment: A Critical Review of Concepts and Their Assessment. Front. Psychol. 2017, 8, 233. [Google Scholar] [CrossRef] [PubMed]
- Farley, H. Promoting Self-efficacy in Patients with Chronic Disease beyond Traditional Education: A Literature Review. Nurs. Open 2020, 7, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Dwarswaard, J.; Bakker, E.J.M.; Van Staa, A.; Boeije, H.R. Self-management Support from the Perspective of Patients with a Chronic Condition: A Thematic Synthesis of Qualitative Studies. Health Expect. 2016, 19, 194–208. [Google Scholar] [CrossRef]
- Lawn, S.; McMillan, J.; Pulvirenti, M. Chronic Condition Self-Management: Expectations of Responsibility. Patient Educ. Couns. 2011, 84, e5–e8. [Google Scholar] [CrossRef]
- RAND Corporation. IFLS Project Teams and Funding. Available online: https://www.rand.org/well-being/social-and-behavioral-policy/data/FLS/IFLS/teamfund.html (accessed on 5 October 2023).
- WMA General Assembly. WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects; World Medical Association: Fortaleza, Brazil, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Order | Disease Dyads | n (%) | Disease Triads | n (%) |
|---|---|---|---|---|
| 1 | Hypertension—Digestive disease | 185 (14.5%) | Hypertension—Digestive disease—Arthritis | 20 (1.6%) |
| 2 | Hypertension—Arthritis | 118 (9.2%) | Hypertension—Digestive disease—High cholesterol | 17 (1.3%) |
| 3 | Hypertension—High cholesterol | 75 (5.9%) | Hypertension—Arthritis—High cholesterol | 12 (0.9%) |
| 4 | Arthritis—Digestive disease | 55 (4.3%) | Hypertension—Arthritis—Asthma | 6 (0.5%) |
| 5 | Digestive disease—Asthma | 47 (3.7%) | Digestive disease—Asthma—Other lung disease | 6 (0.5%) |
| No. | Characteristics | Proportion (%) | ||
|---|---|---|---|---|
| 1. | Socioeconomic-related factors | |||
| Female sex * | 61.7% | |||
| Age (years) | ||||
| 15–65 | 81.0% | |||
| >65 | 19.0% | |||
| Obtained formal education * | 91.7% | |||
| Non-Javanese ethnicity * | 57.5% | |||
| Non-Java residence * | 43.1% | |||
| Rural residence * | 34.0% | |||
| Household size (people) | ||||
| 1 | 2.0% | |||
| 2–6 | 58.6% | |||
| >6 | 39.5% | |||
| Annual income (IDR) * | ||||
| Not working | 39.6% | |||
| <40 million | 51.4% | |||
| 40–100 million | 6.9% | |||
| >100 million | 1.4% | |||
| No health insurance ownership * | 42.1% | |||
| 2. | Patient-related factors | |||
| Healthy current self-perceived health status | 50.2% | |||
| Healthy future self-perceived health status * | 76.9% | |||
| ≤7 days of missing active days in the last month * | 82.1% | |||
| No depressive symptoms * | 61.9% | |||
| 3. | Disease-related factors | |||
| Body mass index * | ||||
| Obese | 15.0% | |||
| Overweight | 30.0% | |||
| Normal | 39.4% | |||
| Underweight | 8.9% | |||
| Smoking behavior | ||||
| Ex-smoker | 11.7% | |||
| Non-smoker | 67.5% | |||
| Active smoker | 20.8% | |||
| 4. | Nonadherent subjects | 36.4% | ||
| No. | Characteristics | Adherent (n = 2236) | Nonadherent (n = 1277) | Bivariate | Multivariate | ||
|---|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | aOR (95% CI) | p-Value | ||||
| 1 | Socioeconomic factors | ||||||
| Female | 1402 (64.7%) | 766 (35.3%) | 0.89 (0.77–1.03) | 0.107 * | 0.87 (0.73–1.10) | 0.303 | |
| Age (years) | |||||||
| 15–65 | 1752 (61.5) | 1095 (38.5%) | 1.66 (1.38–2.00) | 0.000 * | 1.25 (1.01–1.55) | 0.045 ** | |
| >65 | 484 (72.7%) | 182 (27.3%) | Ref | ||||
| Obtained formal education | 2038 (63.3%) | 1183 (36.7%) | 1.30 (0.99–1.71) | 0.055 * | 1.02 (0.76–1.36) | 0.901 | |
| Non-Javanese ethnicity | 1277 (63.2%) | 743 (36.8%) | 1.05 (0.92–1.21) | 0.470 | N/A | ||
| Non-Java residence | 948 (62.7%) | 565 (37.3%) | 1.08 (0.94–1.24) | 0.293 | N/A | ||
| Rural residence | 752 (62.9%) | 443 (37.1%) | 1.05 (0.91–1.21) | 0.530 | N/A | ||
| Household size (people) | |||||||
| 1 | 44 (62.9%) | 26 (37.1%) | 1.23 (0.75–2.03) | 0.409 | 1.02 (0.62–1.70) | 0.930 | |
| 2–6 | 1255 (61.0%) | 802 (39.0%) | 1.33 (1.16–1.54) | 0.000 * | 1.17 (1.01–1.36) | 0.046 ** | |
| >6 | 937 (67.6%) | 449 (32.4%) | Ref | ||||
| Annual income (IDR) | |||||||
| Not working | 959 (68.9%) | 432 (31.1%) | Ref | ||||
| <40 million | 1085 (60.1%) | 721 (39.9%) | 1.48 (1.27–1.71) | 0.000 * | 1.23 (1.04–1.46) | 0.015 ** | |
| 40–100 million | 153 (62.7%) | 91 (37.3%) | 1.32 (1.00–1.75) | 0.054 * | 1.00 (0.73–1.36) | 0.982 | |
| >100 million | 25 (52.1%) | 23 (47.9%) | 2.04 (1.15–3.64) | 0.015 * | 1.52 (0.83–2.77) | 0.174 | |
| No health insurance ownership | 915 (61.9%) | 564 (38.1%) | 1.14 (0.99–1.30) | 0.075 * | 1.20 (1.04–1.39) | 0.015 ** | |
| 2 | Patient-related factors | ||||||
| Healthy current self-perceived health status | 985 (55.8%) | 780 (44.2%) | 1.99 (1.73–2.29) | 0.000 * | 1.79 (1.54–2.08) | 0.000 ** | |
| Healthy future self-perceived health status | N/A | ||||||
| ≤7 days of missing active days in the last month | 1763 (61.2%) | 1120 (38.8%) | 1.90 (1.56–2.31) | 0.000 * | 1.36 (1.10–1.68) | 0.005 ** | |
| No depressive symptoms | N/A | ||||||
| 3 | Condition-related factors | ||||||
| Body mass index | |||||||
| Obese | 347 (65.8%) | 180 (34.2%) | Ref | N/A | |||
| Overweight | 682 (64.8%) | 371 (35.2%) | 1.05 (0.84–1.31) | 0.672 | |||
| Normal | 862 (62.3%) | 522 (37.7%) | 1.17 (0.95–1.44) | 0.149 | |||
| Underweight | 192 (61.1%) | 122 (38.9%) | 1.23 (0.92–1.64) | 0.170 | |||
| Smoking behavior | |||||||
| Ex-smoker | 300 (72.8%) | 112 (27.2%) | Ref | ||||
| Non-smoker | 1510 (63.7%) | 861 (36.3%) | 1.53 (1.21–1.93) | 0.000 * | 1.44 (1.08–1.90) | 0.012 ** | |
| Active smoker | 426 (58.4%) | 304 (41.6%) | 1.91 (1.47–2.49) | 0.000 * | 1.51 (1.14–1.99) | 0.004 ** | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pradipta, I.S.; Aprilio, K.; Ningsih, Y.F.; Pratama, M.A.A.; Alfian, S.D.; Abdulah, R. Treatment Nonadherence among Multimorbid Chronic Disease Patients: Evidence from 3515 Subjects in Indonesia. Medicina 2024, 60, 634. https://doi.org/10.3390/medicina60040634
Pradipta IS, Aprilio K, Ningsih YF, Pratama MAA, Alfian SD, Abdulah R. Treatment Nonadherence among Multimorbid Chronic Disease Patients: Evidence from 3515 Subjects in Indonesia. Medicina. 2024; 60(4):634. https://doi.org/10.3390/medicina60040634
Chicago/Turabian StylePradipta, Ivan Surya, Kevin Aprilio, Yozi Fiedya Ningsih, Mochammad Andhika Aji Pratama, Sofa Dewi Alfian, and Rizky Abdulah. 2024. "Treatment Nonadherence among Multimorbid Chronic Disease Patients: Evidence from 3515 Subjects in Indonesia" Medicina 60, no. 4: 634. https://doi.org/10.3390/medicina60040634
APA StylePradipta, I. S., Aprilio, K., Ningsih, Y. F., Pratama, M. A. A., Alfian, S. D., & Abdulah, R. (2024). Treatment Nonadherence among Multimorbid Chronic Disease Patients: Evidence from 3515 Subjects in Indonesia. Medicina, 60(4), 634. https://doi.org/10.3390/medicina60040634