Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review

 ,
,  ,
, 

 ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Application Protocol and Website Recording Data
2.2. Target Questions
- What are the overall treatment outcomes of reconstructive procedures using bone substitutes in the place of autologous bone?
- As an alternative focused question, does marine collagene use provide beneficial clinical outcomes applied as scaffolds for growth factors?
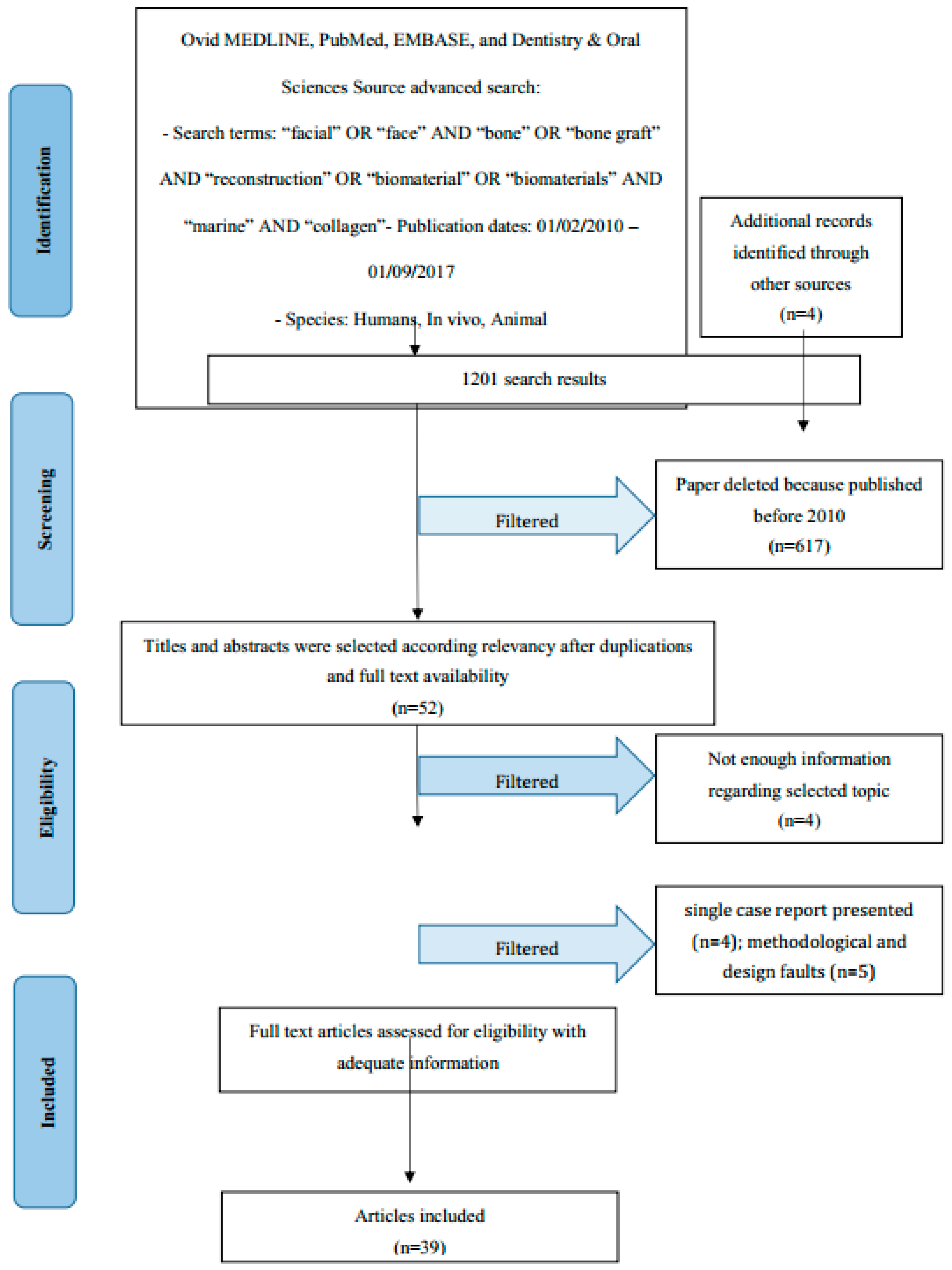
2.3. Search Strategy
2.4. Collection Data
2.5. Manuscript Selections
2.6. Manuscripts Selection
2.7. Research Classifications
2.8. Statement of the Problem
2.9. Exclusion and Inclusion Criteria
- Investigated surgical bone regenerative procedures in patients with vertical and horizontal defect of the jaws.
- Studies involving animals in which the created bone defects were vertical and horizontal.
- Clinical human prospective or retrospective follow-up research and trials, cohort studies, case-control investigations, and case series papers with at least six months follow-up
- Animal or in vitro studies
- Research treating patients with general specific diseases, heart disease, bloody pressure disease, virus infected patients, osteoporosis, immunologic disorders, uncontrolled diabetes mellitus, or other surgical risk related systemic conditions;
- Not enough information regarding the selected topic;
- Articles published prior to 1 February 2010;
- No access to the title and abstract number in the English language.
2.10. Strategy for Collecting Data
2.11. Record of the Extracted and Collected Data Extraction
2.12. Risk of Bias Assessment
- Selection bias;
- Performance bias and detection bias;
- Attrition bias;
- Reporting bias;
- Examiner blinding, examiner calibration, standardized follow-up description, standardized residual graft measurement, standardized radiographic assessment.
3. Results
3.1. Manuscript Collection
3.2. Study Characteristics
3.3. Risk of Bias within Studies
3.4. Risk of Bias across Studies
3.5. Autogenous Bone
3.6. Allogeneic Bone
3.7. Xenograft and Synthetic Bone
3.8. Marine Collagen and Derived Bone
4. Discussion
Limitations
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Herford, A.S.; Tandon, R.; Stevens, T.W.; Stoffella, E.; Cicciù, M. Immediate distraction osteogenesis: The sandwich technique in combination with rhBMP-2 for anterior maxillary and mandibular defects. J. Craniofac. Surg. 2013, 24, 1383–1387. [Google Scholar] [CrossRef] [PubMed]
- Boccaccini, A.R.; Maquet, V. Bioresorbable and bioactive polymer/Bioglass composites with tailored pore structure for tissue engineering applications. Compos. Sci. Technol. 2003, 63, 2417–2429. [Google Scholar] [CrossRef]
- Zhang, C.Y.; Lu, H.; Zhuang, Z.; Wang, X.P.; Fang, Q.F. Nano-hydroxyapatite/poly(l-lactic acid) composite synthesized by a modified in situ precipitation: Preparation and properties. J. Mater. Sci. 2010, 21, 3077–3083. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Lu, M.; Akin, L.; Cicciù, M. Evaluation of a porcine matrix with and without platelet-derived growth factor for bone graft coverage in pigs. Int. J. Oral Maxillofac. Implants 2012, 27, 1351–1358. [Google Scholar] [PubMed]
- Cicciù, M.; Herford, A.S.; Stoffella, E.; Cervino, G.; Cicciù, D. Protein-signaled guided bone regeneration using titanium mesh and Rh-BMP2 in oral surgery: A case report involving left mandibular reconstruction after tumor resection. Open Dent. J. 2012, 6, 51–55. [Google Scholar] [CrossRef] [PubMed]
- Hong, L.; Wang, Y.L.; Jia, S.R.; Huang, Y.; Gao, C.; Wan, Y.Z. Hydroxyapatite/bacterial cellulose composites synthesized via a biomimetic route. Mater. Lett. 2006, 60, 1710–1713. [Google Scholar] [CrossRef]
- Nge, T.T.; Sugiyama, J. Surface functional group dependent apatite formation on bacterial cellulose microfibrils network in a simulated body fluid. J. Biomed. Mater. Res. A 2007, 81, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Herford, A.S.; Cicciù, M. Recombinant human bone morphogenetic protein type 2 jaw reconstruction in patients affected by giant cell tumor. J. Craniofac. Surg. 2010, 21, 1970–1975. [Google Scholar] [CrossRef] [PubMed]
- Fama, F.; Cicciu, M.; Sindoni, A.; Nastro-Siniscalchib, E.; Falzea, R.; Cervino, G.; Polito, F.; De Ponte, F.; Gioffre-Florioa, M. Maxillofacial and concomitant serious injuries: An eight-year single center experience. Chin. J. Traumatol. 2017, 20, 4–8. [Google Scholar] [CrossRef] [PubMed]
- De Ponte, F.S.; Falzea, R.; Runci, M.; Siniscalchi, E.N.; Lauritano, F.; Bramanti, E.; Cervino, G.; Cicciu, M. Histomorhological and clinical evaluation of maxillary alveolar ridge reconstruction after craniofacial trauma by applying combination of allogeneic and autogenous bone graft. Chin. J. Traumatol. 2017, 20, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Hollister, S.J. Porous scaffold design for tissue engineering. Nat. Mater. 2005, 4, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Hollister, S.J.; Lin, C.Y.; Saito, E.; Lin, C.Y.; Schek, R.D.; Taboas, J.M. Engineering craniofacial scaffolds. Orthod. Craniofac. Res. 2005, 8, 162–173. [Google Scholar] [CrossRef] [PubMed]
- Hong, P.; Boyd, D.; Beyea, S.D.; Bezuhly, M. Enhancement of bone consolidation in mandibular distraction osteogenesis: A contemporary review of experimental studies involving adjuvant therapies. J. Plast. Reconstr. Aesthet. Surg. 2013, 66, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janner, S.F.; Bosshardt, D.D.; Cochran, D.L.; Chappuis, V.; Huynh-Ba, G.; Jones, A.A.; Buser, D. The influence of collagen membrane and autogenous bone chips on bone augmentation in the anterior maxilla: A preclinical study. Clin. Oral Implants Res. 2016. [Google Scholar] [CrossRef] [PubMed]
- Emodi, O.; Shilo, D.; Israel, Y.; Rachmiel, A. Three-dimensional planning and printing of guides and templates for reconstruction of the mandibular ramus and condyle using autogenous costochondral grafts. Br. J. Oral Maxillofac. Surg. 2017, 55, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Du Toit, J.; Siebold, A.; Dreyer, A.; Gluckman, H. Choukroun Platelet-Rich Fibrin as an Autogenous Graft Biomaterial in Preimplant Surgery: Results of a Preliminary Randomized, Human Histomorphometric, Split-Mouth Study. Int. J. Periodontics Restor. Dent. 2016, 36, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Nadon, F.; Chaput, B.; Périssé, J.; de Bérail, A.; Lauwers, F.; Lopez, R. Interest of Mineralized Plasmatic Matrix in Secondary Autogenous Bone Graft for the Treatment of Alveolar Clefts. J. Craniofac. Surg. 2015, 26, 2148–2151. [Google Scholar] [CrossRef]
- Bande, C.R.; Daware, S.; Lambade, P.; Patle, B. Reconstruction of Orbital Floor Fractures with Autogenous Bone Graft Application from Anterior Wall of Maxillary Sinus: A Retrospective Study. J. Maxillofac. Oral Surg. 2015, 14, 605–610. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.E.; Hartnett, C.; Hickey-Dwyer, M.; Kearns, G.J. Reconstruction of orbital floor blow-out fractures with autogenous iliac crest bone: A retrospective study including maxillofacial and ophthalmology perspectives. J. Craniomaxillofac. Surg. 2015, 43, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Gultekin, B.A.; Bedeloglu, E.; Kose, T.E.; Mijiritsky, E. Comparison of Bone Resorption Rates after Intraoral Block Bone and Guided Bone Regeneration Augmentation for the Reconstruction of Horizontally Deficient Maxillary Alveolar Ridges. Biomed. Res. Int. 2016. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Gu, B.; Hu, J.; Guo, B.; Feng, G.; Zhu, S. Retrospective comparison of autogenous cosotochondral graft and coronoid process graft in the management of unilateral ankylosis of the temporomandibular joint in adults. Br. J. Oral Maxillofac. Surg. 2014, 52, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Neukam, F.W. Autogenous bone harvesting and grafting in advanced jaw resorption: Morbidity, resorption and implant survival. Eur. J. Oral Implantol. 2014, 7 (Suppl. S2), 203–217. [Google Scholar]
- Cicciù, M.; Herford, A.S.; Cicciù, D.; Tandon, R.; Maiorana, C. Recombinant human bone morphogenetic protein-2 promote and stabilize hard and soft tissue healing for large mandibular new bone reconstruction defects. J. Craniofac. Surg. 2014, 25, 860–862. [Google Scholar] [CrossRef] [PubMed]
- Nary Filho, H.; Pinto, T.F.; de Freitas, C.P.; Ribeiro-Junior, P.D.; dos Santos, P.L.; Matsumoto, M.A. Autogenous bone grafts contamination after exposure to the oral cavity. J. Craniofac. Surg. 2014, 25, 412–414. [Google Scholar] [CrossRef] [PubMed]
- Koerdt, S.; Siebers, J.; Bloch, W.; Ristow, O.; Kuebler, A.C.; Reuther, T. Immunohistochemial study on the expression of von Willebrand factor (vWF) after onlay autogenous iliac grafts for lateral alveolar ridge augmentation. Head Face Med. 2013, 11, 40. [Google Scholar] [CrossRef] [PubMed]
- Pereira Rdos, S.; Jorge-Boos, F.B.; Hochuli-Vieira, E.; da Rocha, H.V., Jr.; Homsi, N.; de Melo, W.M. Management of pure medial orbital wall fracture with autogenous bone graft. J. Craniofac. Surg. 2013, 24, e475–e477. [Google Scholar] [CrossRef] [PubMed]
- Krasny, M.; Krasny, K.; Fiedor, P.; Zadurska, M.; Kamiński, A. Long-term outcomes of the use of allogeneic, radiation-sterilised bone blocks in reconstruction of the atrophied alveolar ridge in the maxilla and mandible. Cell Tissue Bank. 2015, 16, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Schlee, M.; Dehner, J.F.; Baukloh, K.; Happe, A.; Seitz, O.; Sader, R. Esthetic outcome of implant-based reconstructions in augmented bone: Comparison of autologous and allogeneic bone block grafting with the pink esthetic score (PES). Head Face Med. 2014, 28, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Monje, A.; Pikos, M.A.; Chan, H.L.; Suarez, F.; Gargallo-Albiol, J.; Hernández-Alfaro, F.; Galindo-Moreno, P.; Wang, H.L. On the Feasibility of Utilizing Allogeneic Bone Blocks for Atrophic Maxillary Augmentation. Biomed. Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Fretwurst, T.; Spanou, A.; Nelson, K.; Wein, M.; Steinberg, T.; Stricker, A. Comparison of four different allogeneic bone grafts for alveolar ridge reconstruction: A preliminary histologic and biochemical analysis. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2014, 118, 424–431. [Google Scholar] [CrossRef] [PubMed]
- Sbordone, C.; Toti, P.; Guidetti, F.; Califano, L.; Pannone, G.; Sbordone, L. Volumetric changes after sinus augmentation using blocks of autogenous iliac bone or freeze-dried allogeneic bone. A non-randomized study. J. Craniomaxillofac. Surg. 2014, 42, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Scheyer, E.T.; Heard, R.; Janakievski, J.; Mandelaris, G.; Nevins, M.L.; Pickering, S.R.; Richardson, C.R.; Pope, B.; Toback, G.; Velásquez, D.; et al. A randomized, controlled, multicentre clinical trial of post-extraction alveolar ridge preservation. J. Clin. Periodontol. 2016, 43, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Le, B.; Borzabadi-Farahani, A.; Nielsen, B. Treatment of Labial Soft Tissue Recession Around Dental Implants in the Esthetic Zone Using Guided Bon Regeneration With Mineralized Allograft: A Retrospective Clinical Case Series. J. Oral Maxillofac. Surg. 2016, 74, 1552–1561. [Google Scholar] [CrossRef] [PubMed]
- Fienitz, T.; Moses, O.; Klemm, C.; Happe, A.; Ferrari, D.; Kreppel, M.; Ormianer, Z.; Gal, M.; Rothamel, D. Histological and radiological evaluation of sintered and non-sintered deproteinized bovine bone substitute materials in sinus augmentation procedures. A prospective, randomized-controlled, clinical multicenter study. Clin. Oral Investig. 2017, 21, 787–794. [Google Scholar] [CrossRef] [PubMed]
- You, D.J.; Yoon, H.J. Bone Regeneration with Bilayer Bone Augmentation Technique for the Treatment of Dehiscence-Type Defects Around Implants: A Preliminary Study in Dogs. Int. J. Oral Maxillofac. Implants 2016, 31, 318–323. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, T.A.; Aloise, A.C.; Orosz, J.E.; de Mello, E.; Oliveira, R.; de Carvalho, P.; Pelegrine, A.A. Double Centrifugation Versus Single Centrifugation of Bon Marrow Aspirate Concentrate in Sinus Floor Elevation: A Pilot Study. Int. J. Oral Maxillofac. Implants 2016, 31, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Ghanaati, S.; Barbeck, M.; Booms, P.; Lorenz, J.; Kirkpatrick, C.J.; Sader, R.A. Potential lack of “standardized” processing techniques for production of allogeneic and xenogeneic bone blocks for application in humans. Acta Biomater. 2014, 10, 3557–3562. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Kim, I.; Cho, H.; Seo, J.; Lee, D.; Jang, J.; Park, S. The healing effect of platelet-rich plasma on xenograft in peri-implant bone defects in rabbits. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Klein, M.O.; Kämmerer, P.W.; Götz, H.; Duschner, H.; Wagner, W. Long-term bony integration and resorption kinetics of a xenogeneic bone substitute after sinus floor augmentation: Histomorphometric analyses of human biopsy specimens. Int. J. Periodontics Restor. Dent. 2013, 33, e101–e110. [Google Scholar] [CrossRef] [PubMed]
- Figueiredo, A.; Coimbra, P.; Cabrita, A.; Guerra, F.; Figueiredo, M. Comparison of a xenogeneic and an alloplastic material used in dental implants in terms of physico-chemical characteristics and in vivo inflammatory response. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 3506–3513. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Yun, P.Y.; Lee, H.J.; Ahn, J.Y.; Kim, S.G. Ridge preservation of the molar extraction socket using collagen sponge and xenogeneic bone grafts. Implant. Dent. 2011, 4, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Zahng, X.; Vecchio, K.S. Conversion of natural marine skeletons as scaffolds for bobe tissue engineering. Front. Mater. Sci. 2013, 7, 103–117. [Google Scholar] [CrossRef]
- Lin, C.C.; Ritch, R.; Lin, S.M.; Ni, M.H.; Chang, Y.C.; Lu, Y.L.; Lai, H.J.; Lin, F.H. A new fish scale-derived scaffold for corneal regeneration. Eur. Cell Mater. 2010, 26, 50–57. [Google Scholar] [CrossRef]
- Hayashi, Y.; Yamada, S.; Yanagi Guchi, K.; Koyama, Z.; Ikeda, T. Chitosan and fish collagen as biomaterials for regenerative medicine. Adv. Food Nutr. Res. 2012, 65, 107–120. [Google Scholar] [PubMed]
- Senni, K.; Gueniche, F.; Changotade, S.; Septier, D.; Sinquin, C.; Ratiskol, J.; Lutomski, D.; Godeau, G.; Guezennec, J.; Colliec-Jouault, S. Unusual glycosaminoglycans from a deep sea hydrothermal bacterium improve fibrillar collagen structuring and fibroblast activities in engineered connective tissues. Mar. Drugs 2013, 11, 1351–1369. [Google Scholar] [CrossRef] [PubMed]
- Fernandes-Silva, S.; Moreira-Silva, J.; Silva, T.H.; Perez-Martin, R.I.; Sotelo, C.G.; Mano, J.F.; Duarte, A.R.; Reis, R.L. Porous hydrogels from shark skin collagen crosslinked under dense carbon dioxide atmosphere. Macromol. Biosci. 2013, 13, 1621–1631. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, K.; Igawa, K.; Sugimoto, K.; Yoshizawa, Y.; Yanagiguchi, K.; Ikeda, T.; Yamada, S.; Hayashi, Y. Biological safety of fish (tilapia) collagen. Biomed. Res. Int. 2014, 2014, 630757. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, Y.; Yamauchi, M.; Kim, S.K.; Kusaoke, H. Biomaterials: Chitosan and collagen for regenerative medicine. Biomed. Res. Int. 2014, 2014, 690485. [Google Scholar] [CrossRef] [PubMed]
- Silva, T.H.; Moreira-Silva, J.; Marques, A.L.; Domingues, A.; Bayon, Y.; Reis, R.L. Marine origin collagens and its potential applications. Mar. Drugs 2014, 12, 5881–5901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jridi, M.; Bardaa, S.; Moalla, D.; Rebaii, T.; Souissi, N.; Sahnoun, Z.; Nasri, M. Microstructure, rheological and wound healing properties of collagen-based gel from cuttlefish skin. Int. J. Biol. Macromol. 2015, 77, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Derkus, B.; Arslan, Y.E.; Emregul, K.C.; Emregul, E. Enhancement of aptamer immobilization using egg shell-derived nano-sized spherical hydroxyapatite for thrombin detection in neuroclinic. Talanta 2016, 158, 100–109. [Google Scholar] [CrossRef] [PubMed]
- Raftery, R.M.; Woods, B.; Marques, A.L.P.; Moreira-Silva, J.; Silva, T.H.; Cryan, S.A.; Reis, R.L.; O’Brien, F.J. Multifunctional biomaterials from the sea: Assessing the effects of chitosan incorporation into collagen scaffolds on mechanical and biological functionality. Acta Biomater. 2016, 43, 160–169. [Google Scholar] [CrossRef] [PubMed]
- Coelho, R.C.G.; Marques, A.L.P.; Oliveira, S.M.; Diogo, G.S.; Pirraco, R.P.; Moreira-Silva, J.; Xavier, J.C.; Reis, R.L.; Silva, T.H.; Mano, J.F. Extraction and characterization of collagen from Antarctic and Sub-Antarctic squid and its potential application in hybrid scaffolds for tissue engineering. Mater. Sci. Eng. C Mater. Biol. Appl. 2017, 78, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.A. An Overview of the Medical Applications of Marine Skeletal Matrix Proteins. Mar. Drugs 2016, 14, 167. [Google Scholar] [CrossRef] [PubMed]
- Tziveleka, L.-A.; Ioannou, E.; Tsiourvas, D.; Berillis, P.; Foufa, E.; Roussis, V. Collagen from the Marine Sponges Axinella cannabina and Suberites carnosus: Isolation and Morphological, Biochemical, and Biophysical Characterization. Mar. Drugs 2017, 15, 152. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, H.; Ilan, M.; Maldonado, M.; Muricy, G.; Bavestrello, G.; Kljajic, Z.; Carballo, J.L.; Shiaparelli, S.; Ereskovsky, A.V.; Schupp, P.; et al. Three-Dimensional chitin-based scaffolds from Verongida sponges (Demospongiae: Porifera). Part I. Isolation and identification of chitin. Int. J. Biol. Macromol. 2010, 47, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, H.; Kaluzhnaya, O.V.; Brunner, E.; Tsurkan, M.V.; Ereskovsky, A.; Ilan, M.; Tabachnick, K.R.; Bazhenov, V.V.; Paasch, S.; Kammer, M.; et al. Identification and first insights into the structure and biosynthesis of chitin from the freshwater sponge Spongilla lacustris. J. Struct. Biol. 2013, 183, 474–483. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, H.; Keith Rigby, J.; Botting, J.P.; Tsurkan, M.V.; Werner, C.; Schwille, P.; Petrášek, Z.; Pisera, A.; Simon, P.; Sivkov, V.N.; et al. Discovery of 505-million-year old chitin in the basal demosponge Vauxia gracilenta. Sci. Rep. 2013, 3, 3497. [Google Scholar] [CrossRef] [PubMed]
- Ehrlich, H. Biological Materials of Marine Origin: Vertebrates; Springer: Berlin, Germany, 2015; p. 594. [Google Scholar]


{kind=link}
| Author and Year | In Vivo vs. In Vitro | Kind of Graft | Follow up after 12 Months |
|---|---|---|---|
| Janner et al., 2016 | In Vivo | Autologous | Yes |
| Emodi et al., 2017 | In Vivo | Autologous | Yes |
| Du Toit et al., 2016 | In Vivo | Autologous | Yes |
| Nadon et al., 2015 | In Vivo | Autologous | Yes |
| Bande et al., 2014 | In Vivo | Autologous | Yes |
| O’Connell et al., 2014 | In Vivo | Autologous | No |
| Gultekin et al., 2016 | In Vivo | Autologous | Yes |
| Zhang et al., 2014 | In Vivo | Autologous | Yes |
| Nkenke et al., 2014 | In Vivo | Autologous | Yes |
| Cicciù et al., 2014 | In Vivo | Autologous | No |
| Nary Filho et al., 2014 | In Vivo | Autologous | Yes |
| Koerdt et al., 2013 | In Vivo | Autologous | Yes |
| Pereira R et al., 2013 | In Vivo | Autologous | Yes |
| Krasny et al., 2015 | In Vivo | Homologous | Yes |
| Schlee et al., 2014 | In Vivo | Homologous | No |
| Monje et al., 2014 | In Vivo | Homologous | No |
| Fretwurst et al., 2014 | In Vivo | Homologous | No |
| Sbordone et al., 2014 | In Vivo/In Vitro | Homologous | Yes |
| Scheyer et al., 2016 | In Vivo/In Vitro | Xenograft/Synthetic | No |
| Le et al., 2016 | In Vivo/In Vitro | Xenograft/Synthetic | Yes |
| Fienitz et al., 2017 | In Vivo/In Vitro | Xenograft/Synthetic | N/A |
| You et al., 2016 | In Vivo/In Vitro | Xenograft/Synthetic | No |
| De oliveira et al., 2016 | In Vivo/In Vitro | Xenograft/Synthetic | Yes |
| Ghanaati et al., 2014 | In Vivo/In Vitro | Xenograft/Synthetic | Yes |
| Peng et al., 2016 | In Vivo/In Vitro | Xenograft/Synthetic | Yes |
| Klein et al., 2014 | In Vivo/In Vitro | Xenograft/Synthetic | No |
| Figueiredo et al., 2013 | In Vivo/In Vitro | Xenograft/Synthetic | No |
| Kim et al., 2011 | In Vivo/In Vitro | Xenograft/Synthetic | No |
| Lin et al., 2010 | In Vivo/In Vitro | Marine Collagen | N/A |
| Hayashi et al., 2012 | In Vivo/In Vitro | Marine Collagen | N/A |
| Senni et al., 2013 | In Vitro | Marine Collagen | N/A |
| Fernandes et al., 2013 | In Vitro | Marine Collagen | N/A |
| Yamamoto et al., 2014 | In Vitro | Marine Collagen | N/A |
| Hayashi et al., 2014 | In Vivo/In Vitro | Marine Collagen | N/A |
| Silva et al., 2014 | In Vivo/In Vitro | Marine Collagen | N/A |
| Jridi et al., 2015 | In Vivo/In Vitro | Marine Collagen | N/A |
| Derkus et al., 2016 | In Vivo/In Vitro | Marine Collagen | N/A |
| Raftery et al. 2016 | In Vivo/In Vitro | Marine Collagen | N/A |
| Coelho et al. 2017 | In Vivo/In Vitro | Marine Collagen | N/A |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cicciù, M.; Cervino, G.; Herford, A.S.; Famà, F.; Bramanti, E.; Fiorillo, L.; Lauritano, F.; Sambataro, S.; Troiano, G.; Laino, L. Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review. Mar. Drugs 2018, 16, 27. https://doi.org/10.3390/md16010027
Cicciù M, Cervino G, Herford AS, Famà F, Bramanti E, Fiorillo L, Lauritano F, Sambataro S, Troiano G, Laino L. Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review. Marine Drugs. 2018; 16(1):27. https://doi.org/10.3390/md16010027
Chicago/Turabian StyleCicciù, Marco, Gabriele Cervino, Alan Scott Herford, Fausto Famà, Ennio Bramanti, Luca Fiorillo, Floriana Lauritano, Sergio Sambataro, Giuseppe Troiano, and Luigi Laino. 2018. "Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review" Marine Drugs 16, no. 1: 27. https://doi.org/10.3390/md16010027
APA StyleCicciù, M., Cervino, G., Herford, A. S., Famà, F., Bramanti, E., Fiorillo, L., Lauritano, F., Sambataro, S., Troiano, G., & Laino, L. (2018). Facial Bone Reconstruction Using both Marine or Non-Marine Bone Substitutes: Evaluation of Current Outcomes in a Systematic Literature Review. Marine Drugs, 16(1), 27. https://doi.org/10.3390/md16010027