The Impact of Socio-Economic Status on Self-Rated Health: Study of 29 Countries Using European Social Surveys (2002–2008)


 ,
,  ,
,
Abstract
:1. Introduction
2. Method
2.1. Data and Variables

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Obs. | Mean | Std. Dev. | Min. | Max. | |
|---|---|---|---|---|---|
| SRH | 184,718 | 3.759 | 0.933 | 1 | 5 |
| Income | 129,344 | 14,217.69 | 24,390.57 | 0 | 180,000 |
| Education | 182,739 | 11.855 | 4.116 | 0 | 56 |
| Occ. status | 160,280 | 42.083 | 16.611 | 16 | 90 |
2.2. Statistical Methodology









3. Results




4. Discussion
5. Conclusions
Acknowledgements
Conflict of Interest
References
- Wilkinson, R.; Marmot, M. Social Determinants of Health: The Solid Facts; World Health Organization: Copenhagen, Denmark, 2003. [Google Scholar]
- Bartley, M.; Sacker, A.; Clarke, P. Employment status, employment conditions, and limiting illness: Prospective evidence from the British household panel survey 1991–2001. J. Epidemiol. Community Health 2004, 58, 501–506. [Google Scholar] [CrossRef]
- Adams, P.; Hurd, M.D.; McFadden, D.; Merril, A.; Ribeiro, T. Health, wealthy and wise. Tests for direct causal paths between health and socioeconomic status. J. Econometrics 2003, 112, 3–56. [Google Scholar] [CrossRef]
- Frijters, P.; Haisken-DeNew, J.P.; Shields, M.A. The causal effect of income on health: Evidence from German reunification. J. Health Econ. 2005, 24, 997–1017. [Google Scholar] [CrossRef]
- Wilkinson, R.G. Unhealthy Societies: The Afflictions of Inequality; Routledge: London, UK, 1996. [Google Scholar]
- Wilkinson, R. Health inequalities: Relative or absolute material standards. Br. Med. J. 1997, 314, 591–595. [Google Scholar]
- Nummela, O.P.; Sulander, T.T.; Heinonen, H.S.; Uutela, A.K. Self-rated health and indicators of SES among the ageing in three types of communities. Scand. J. Publ. Health 2007, 35, 39–47. [Google Scholar] [CrossRef]
- Costa-Font, J.; Hernández-Quevedo, C. Measuring inequalities in health: What do we know? What do we need to know? Health Policy 2012, 106, 195–206. [Google Scholar]
- Eikemo, T.A; Huisman, M.; Bambra, C.; Kunst, A.E. Health inequalities according to educational level in different welfare regimes: A comparison of 23 European countries. Sociology Health Illness 2008, 30, 565–582. [Google Scholar]
- Eikemo, T.A.; Bambra, C.; Joyce, K.; Dahl, E. Welfare state regimes and income-related health inequalities: A comparison of 23 European countries. Eur. J. Publ. Health 2008, 18, 593–599. [Google Scholar] [CrossRef]
- Eikemo, T.A.; Bambra, C.; Judge, K.; Ringdal, K. Welfare state regimes and differences in self-perceived health in Europe: A multilevel analysis. Soc. Sci. Med. 2008, 66, 2281–2295. [Google Scholar] [CrossRef] [Green Version]
- Fritzell, J.; Nermo, M.; Lundberg, O. The impact of income: Assessing the relationship between income and health in Sweden. Scand. J. Publ. Health 2004, 32, 6–16. [Google Scholar] [CrossRef]
- Van Doorslaer, E.; Koolman, X. Explaining the differences in income-related health inequalities across European countries. Health Econ. 2004, 13, 609–628. [Google Scholar] [CrossRef]
- Kunst, A.E.; Bos, V.; Lahelma, E.; Bartley, M.; Lissau, I.; Regidor, E.; Mielck, A.; Cardano, M.; Dalstra, J.A.; Geurts, J.J.; Helmert, U.; Lennartsson, C.; Ramm, J.; Spadea, T.; Stronegger, W.J.; Mackenbach, J.P. Trends in socioeconomic inequalities in self-assessed health in 10 European countries. Int. J. Epidemiol. 2005, 34, 295–305. [Google Scholar] [CrossRef]
- Grossman, M. The human capital model. In Handbook of Health Economics; Culyer, A.J., Newhouse, J.P., Eds.; Elsevier: Amsterdam, The Netherlands, 2000; pp. 347–408. [Google Scholar]
- Smith, J.P. Unravelling the SES health connection. Aging, health and public policy: Demographic and economic perspectives. Popul. Dev. Rev. 2004, 30, 108–132. [Google Scholar] [CrossRef]
- Marmot, M. Fair Society, Healthy Lives. The Marmot Review Final Report; University College London, Department of Epidemiology and Public Health: London, UK, 2010. [Google Scholar]
- Kelleher, C.C.; Friel, S.; Nic Gabhainn, S.; Tay, J.B. Socio-demographic predictors of self-rated health in the Republic of Ireland: Findings from the National Survey on Lifestyle, Attitudes and Nutrition, SLAN. Soc. Sci. Med. 2003, 57, 477–486. [Google Scholar] [CrossRef]
- Eikemo, T.A.; Kunst, A.E.; Judge, K.; Mackenbach, J.P. Class-related health inequalities are not larger in the East: A comparison of four European regions using the new European socioeconomic classification. J. Epidemiol. Community Health 2008, 62, 1072–1078. [Google Scholar]
- Hernandez-Quevedo, C.; Jones, A.M.; Lopez-Nicolás, A.; Rice, N. Socioeconomic inequalities in health: A comparative longitudinal analysis using the European Community Household Panel. Soc. Sci. Med. 2006, 63, 1246–1261. [Google Scholar] [CrossRef]
- Hanibuchi, T.; Nakaya, T.; Murata, C. Socio-economic status and self-rated health in East Asia: A comparison of China, Japan, South Korea and Taiwan. Eur. J. Publ. Health 2012, 22, 47–52. [Google Scholar] [CrossRef]
- ESS Round 1–4: European Social Survey Round 1–4 Data (2002–2008); Norwegian Social Science Data Services: Bergen, Norway. Available online: http://ess.nsd.uib.no/ (accessed on 3 January 2013).
- Yannis, G.; Nicholas, T.; Ping, Y.P. Personal values as mitigating factors in the link between income and life satisfaction: Evidence from the European Social Survey. Soc. Indic. Res. 2009, 91, 329–344. [Google Scholar] [CrossRef]
- Ganzeboom, H.B.G.; Donald, J.T. Internationally comparable measures of occupational status for the 1988 international standard classification of occupations. Soc. Sci. Res. 1996, 25, 201–239. [Google Scholar] [CrossRef]
- International Standard Classification of Occupations: ISCO-88; ILO (International Labour Office): Geneva, Switzerland, 1990.
- Greene, W. Econometric Analysis, 6th ed; Prentice Hall: Upper Saddle River, NJ, USA, 2008; pp. 831–835. [Google Scholar]
- McKelvey, R.D.; Zavoina, W. A statistical model for the analysis of ordinal level dependent variables. J. Math. Sociol. 1975, 4, 103–20. [Google Scholar] [CrossRef]
- Brant, R. Assessing proportionality in the proportional odds model for ordinal logistic regression. Biometrics 1990, 46, 1171–1178. [Google Scholar] [CrossRef]
- Von dem Knesebeck, O.; Verde, P.E.; Dragano, N. Education and health in 22 European countries. Soc. Sci. Med. 2006, 63, 1344–1351. [Google Scholar] [CrossRef]
- Olsen, K.M.; Dahl, S.A. Health differences between European countries. Soc. Sci. Med. 2007, 64, 1665–1678. [Google Scholar] [CrossRef]
- Esping-Andersen, G. Social Foundations of Postindustrial Economies; Oxford University Press: New York, NY, USA, 1999. [Google Scholar]
- Stiglitz, J.E. The Price of Inequality: How Today’s Divided Society Endangers Our Future; W. W. Norton & Company: New York, NY, USA, 2012. [Google Scholar]
- EUROSTAT. General Government Expenditure. Government Expenditure on Culture an Education. European commission, 2012. Available online: http://epp.eurostat.ec.europa.eu/statistics_explained/index.php/General_government_expenditure_statistics#Government_expenditure_on_culture_and_education (accessed on 3 January 2013).
- Bambra, C.; Eikemo, T.A. Welfare state regimes, unemployment and health: A comparative study of the relationship between unemployment and self-reported health in 23 European countries. J. Epidemiol. Community Health 2009, 63, 92–98. [Google Scholar] [CrossRef] [Green Version]
Appendix
| Year 2002 | Year 2004 | Year 2006 | Year 2008 | |
|---|---|---|---|---|
| Austria | ||||
| Income | 1.90 (0.61) *** | 1.64 (0.60) *** | 2.30 (0.53) *** | NA |
| Education | 5.42 (1.32) *** | 7.51 (1.56) *** | 7.06 (1.36) *** | NA |
| Occ. status | 0.82 (0.39) ** | −0.13 (0.42) | 0.65 (0.35) * | NA |
| R2 | 0.02 | 0.02 | 0.03 | NA |
| Belgium | ||||
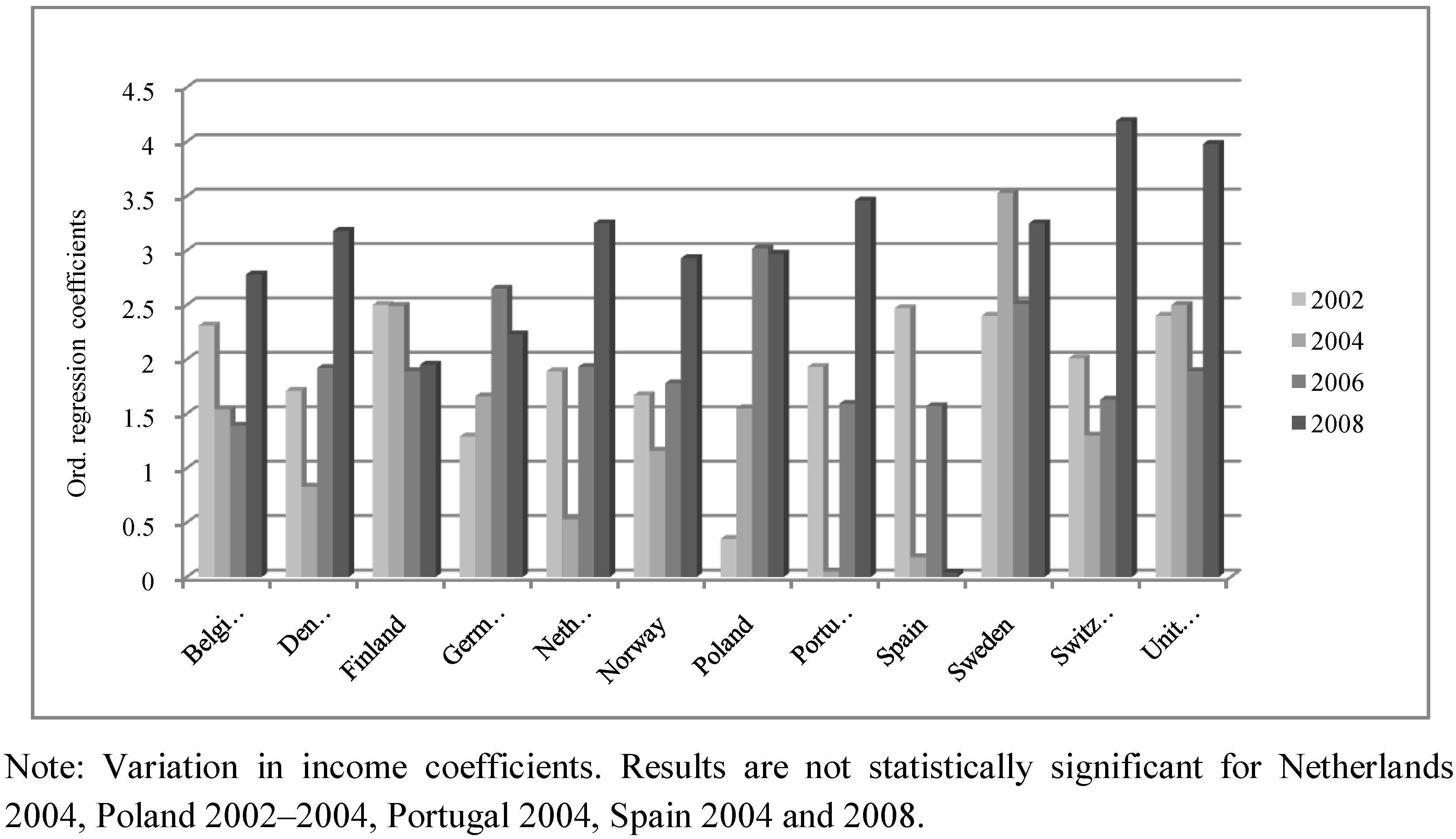
| Income | 2.31 (0.62) *** | 1.54 (0.50) *** | 1.39 (0.50) *** | 2.78 (0.54) *** |
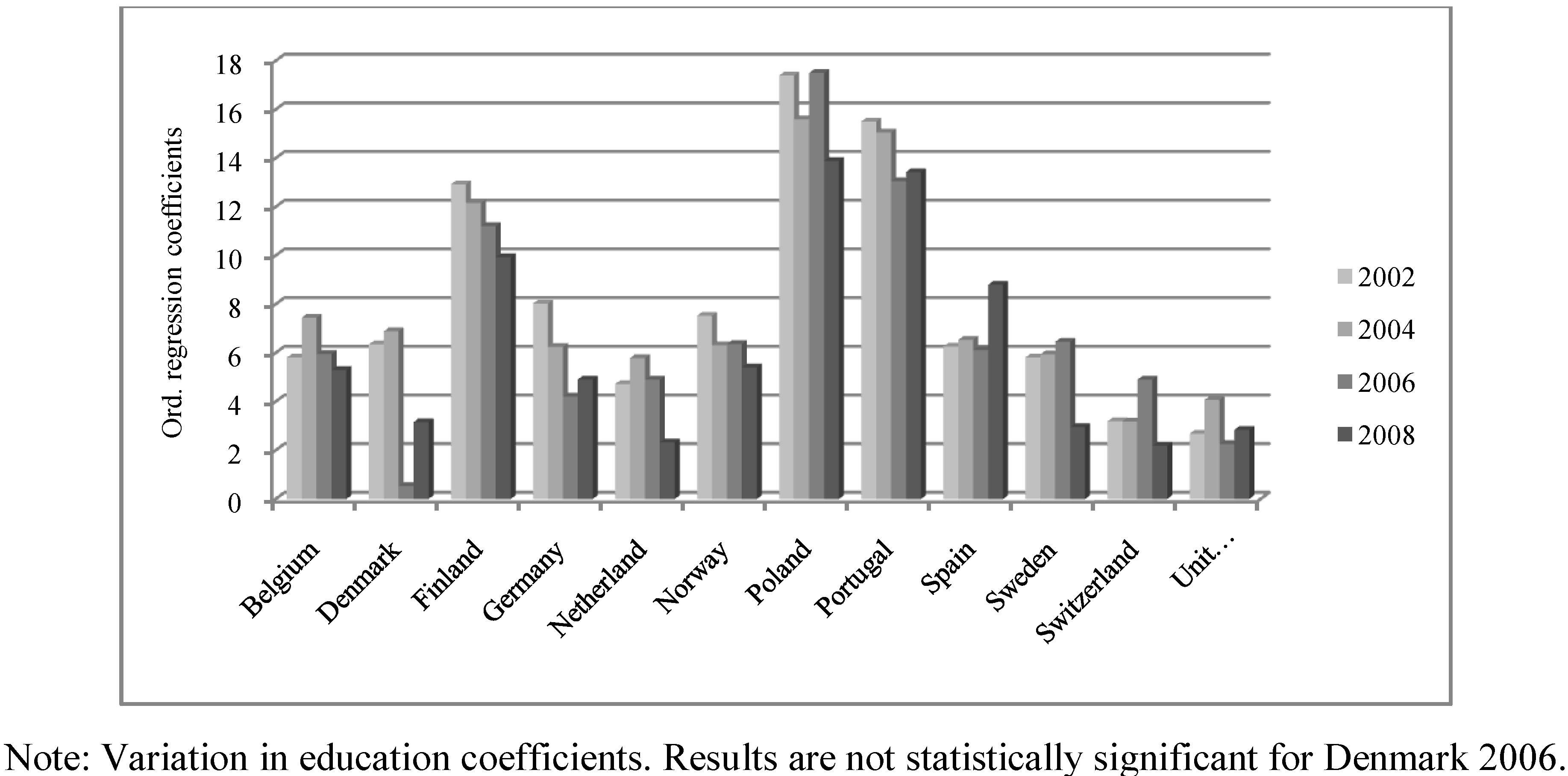
| Education | 5.81 (1.27) *** | 7.45 (1.12) *** | 5.96 (1.17) *** | 5.30 (1.24) *** |
| Occ. status | 0.27 (0.35) | 0.59 (0.36) | 1.06 (0.33) *** | 0.39 (0.34) |
| R2 | 0.02 | 0.03 | 0.03 | 0.03 |
| Bulgaria | ||||
| Income | NA | NA | 62.88 (8.25) *** | NA |
| Education | NA | NA | 10.81 (1.74) *** | NA |
| Occ. status | NA | NA | −1.10 (0.46) ** | NA |
| R2 | NA | NA | 0.06 | NA |
| Cyprus | ||||
| Income | NA | NA | 3.34 *** (1.17) | NA |
| Education | NA | NA | 15.38 *** (1.80) | NA |
| Occ. status | NA | NA | −0.89 (0.57) | NA |
| R2 | NA | NA | 0.09 | NA |
| Czech Republic | ||||
| Income | 6.69 (1.67) *** | 5.01 (0.89) *** | NA | 9.47 (1.70) *** |
| Education | 9.95 (1.83) *** | 12.02 (1.81) *** | NA | 8.45 (2.00) *** |
| Occ. status | −0.22 (0.50) | 0.42 (0.39) | NA | 0.16 (0.41) |
| R2 | 0.03 | 0.03 | NA | 0.03 |
| Denmark | ||||
| Income | 1.71 (0.50) *** | 0.83 (0.43) * | 1.92 (0.45) *** | 3.18 (0.56) *** |
| Education | 6.35 (1.26) *** | 6.89 (1.25) *** | 0.54 (0.84) | 3.16 (0.89) *** |
| Occ. status | −0.59 (0.35) * | 0.22 (0.34) | 1.15 (0.32) *** | 0.15 (0.32) |
| R2 | 0.03 | 0.02 | 0.02 | 0.02 |
| Estonia | ||||
| Income | NA | NA | NA | 5.16 (0.57) *** |
| Education | NA | NA | NA | 11.85 (1.32) *** |
| Occ. status | NA | NA | NA | −0.49 (0.32) |
| R2 | NA | NA | NA | 0.07 |
| Finland | ||||
| Income | 2.50 (0.58) *** | 2.49 (0.51) *** | 1.89 (0.46) *** | 1.95 (0.50) *** |
| Education | 12.93 (1.03) *** | 12.16 (1.01) *** | 11.21 (0.97) *** | 9.93 (0.92) *** |
| Occ. status | −0.45 (0.30) | −0.64 (0.29) ** | −0.56 (0.30) * | −0.20 (0.27) |
| R2 | 0.06 | 0.06 | 0.06 | 0.05 |
| France | ||||
| Income | NA | 1.18 (0.44) *** | 1.48 (0.55) *** | 2.57 (0.51) *** |
| Education | NA | 9.70 (1.03) *** | 7.75 (0.94) *** | 7.47 (0.96) *** |
| Occ. status | NA | −0.34 (0.32) | −0.30 (0.31) | −0.30 (0.30) |
| R2 | 0.03 | 0.03 | 0.03 | 0.03 |
| Germany | ||||
| Income | 1.29 (0.44) *** | 1.66 (0.41) *** | 2.65 (0.47) *** | 2.23 (0.61) *** |
| Education | 8.03 (1.08) *** | 6.25 (1.12) *** | 4.21 (1.04) *** | 4.91 (1.05) *** |
| Occ. status | −0.16 (0.29) | 0.10 (0.30) | 0.73 (0.30) ** | 0.08 (0.29) |
| R2 | 0.02 | 0.02 | 0.02 | 0.01 |
| Greece | ||||
| Income | 3.29 (0.81) *** | 6.29 (1.08) *** | NA | 1.43 (0.84) * |
| Education | 14.09 (1.08) *** | 14.36 (1.09) *** | NA | 13.90 (1.40) *** |
| Occ. status | −1.21 (0.41) *** | −1.50 (0.42) *** | NA | −0.74 (0.49) |
| R2 | 0.08 | 0.10 | NA | 0.06 |
| Hungary | ||||
| Income | NA | 12.25 (2.41) *** | NA | 5.27 (0.86) *** |
| Education | NA | 13.20 (1.67) *** | NA | 6.62 (1.47) *** |
| Occ. status | NA | −0.63 (0.42) | NA | −0.09 (0.46) |
| R2 | NA | 0.05 | NA | 0.04 |
| Ireland | ||||
| Income | NA | 2.52 (0.42) *** | 1.23 (0.40) *** | 2.05 (0.70) *** |
| Education | NA | 6.00 (1.19) *** | 6.07 (1.35) *** | 6.48 (1.11) *** |
| Occ. status | NA | 0.30 (0.33) | 0.15 (0.37) | 0.20 (0.32) |
| R2 | NA | 0.04 | 0.02 | 0.03 |
| Israel | ||||
| Income | 3.60 (0.76) *** | NA | NA | 0.11 (0.54) |
| Education | 3.15 (1.09) *** | NA | NA | 7.05 (1.24) *** |
| Occ. status | −0.15 (0.31) | NA | NA | −0.05 (0.31) |
| R2 | 0.01 | NA | NA | 0.01 |
| Italy | ||||
| Income | 3.40 (1.01) *** | 1.66 (0.61) *** | NA | NA |
| Education | 8.27 (1.77) *** | 9.23 (1.41) *** | NA | NA |
| Occ. status | −0.25 (0.65) | −0.44 (0.49) | NA | NA |
| R2 | 0.05 | 0.04 | NA | NA |
| Luxemburg | ||||
| Income | 1.25 (0.60) ** | 1.02 (0.53) * | NA | NA |
| Education | 4.53 (1.48) *** | 5.99 (1.22) *** | NA | NA |
| Occ. status | 0.83 (0.45) * | 0.31 (0.42) | NA | NA |
| R2 | 0.02 | 0.03 | NA | NA |
| Netherland | ||||
| Income | 1.89 (0.39) *** | 0.53 (0.44) | 1.93 (0.47) *** | 3.25 (0.57) *** |
| Education | 4.72 (0.88) *** | 5.79 (1.06) *** | 4.90 (0.91) *** | 2.33 (0.96) ** |
| Occ. status | 0.41 (0.29) | 0.25 (0.33) | 0.80 (0.33) ** | 0.66 (0.35) * |
| R2 | 0.02 | 0.02 | 0.03 | 0.03 |
| Norway | ||||
| Income | 1.67 (0.34) *** | 1.16 (0.29) *** | 1.78 (0.27) *** | 2.93 (0.52) *** |
| Education | 7.53 (1.11) *** | 6.31 (1.07) *** | 6.37 (1.01) *** | 5.41 (1.05) *** |
| Occ. status | 0.20 (0.31) | 0.25 (0.31) | 0.10 (0.31) | 0.61 (0.32) * |
| R2 | 0.03 | 0.02 | 0.03 | 0.03 |
| Poland | ||||
| Income | 0.35 (0.85) | 1.55 (1.08) | 3.02 (1.17) ** | 2.97 (0.60) *** |
| Education | 17.40 (1.33) *** | 15.60 (1.50) *** | 17.50 (1.52) *** | 13.89 (1.49) *** |
| Occ. status | −0.96 (0.37) ** | −0.69 (0.42) | −0.57 (0.40) | −1.19 (0.40) *** |
| R2 | 0.06 | 0.05 | 0.07 | 0.06 |
| Portugal | ||||
| Income | 1.93 (0.86) ** | 0.05 (0.69) | 1.59 (0.66) ** | 3.46 (1.47) ** |
| Education | 15.51 (1.36) *** | 15.06 (1.29) *** | 13.06 (1.26) *** | 13.43 (1.48) *** |
| Occ. status | −1.37 (0.48) *** | −0.86 (0.48) * | −0.95 (0.50) * | −0.74 (0.57) |
| R2 | 0.09 | 0.08 | 0.07 | 0.08 |
| Russian Federation | ||||
| Income | NA | NA | 31.13 (3.29) *** | 4.84 (0.54) *** |
| Education | NA | NA | 13.52 (1.24) *** | 15.06 (1.24) *** |
| Occ. status | NA | NA | −0.56 (0.32) * | −1.18 (0.30) *** |
| R2 | NA | NA | 0.08 | 0.08 |
| Slovenia | ||||
| Income | 7.82 (1.62) *** | 7.56 (1.69) *** | 8.28 (1.46) *** | 5.23 (0.81) *** |
| Education | 10.63 (1.60) *** | 9.14 (1.80) *** | 8.65 (1.56) *** | 6.43 (1.42) *** |
| Occ. status | −0.61 (0.42) | 0.03 (0.46) | 0.58 (0.44) | −0.19 (0.40) |
| R2 | 0.05 | 0.05 | 0.06 | 0.05 |
| Slovakia | ||||
| Income | NA | 1.78 (1.11) | 7.75 (1.56) *** | NA |
| Education | NA | 7.55 (1.79) *** | 9.11 (1.63) *** | NA |
| Occ. status | NA | −0.73 (0.42) * | −0.02 (0.42) | NA |
| R2 | NA | 0.01 | 0.04 | NA |
| Spain | ||||
| Income | 2.47 (1.24) ** | 0.18 (0.83) | 1.57 (0.64) ** | 0.04 (0.66) |
| Education | 6.26 (1.08) *** | 6.54 (1.08) *** | 6.12 (0.96) *** | 8.80 (0.90) *** |
| Occ. status | −0.30 (0.50) | 0.72 (0.43) * | 0.30 (0.43) | −0.19 (0.37) |
| R2 | 0.03 | 0.04 | 0.04 | 0.04 |
| Sweden | ||||
| Income | 2.40 (0.63) *** | 3.53 (0.57) *** | 2.51 (0.49) *** | 3.25 (0.52) *** |
| Education | 5.82 (1.06) *** | 5.94 (1.07) *** | 6.46 (1.08) *** | 2.96 (1.06) *** |
| Occ. status | 0.32 (0.29) | 0.01 (0.29) | −0.40 (0.30) | 0.49 (0.30) |
| R2 | 0.02 | 0.03 | 0.03 | 0.02 |
| Switzerland | ||||
| Income | 2.01 (0.35) *** | 1.30 (0.34) *** | 1.63 (0.35) *** | 4.19 (0.71) *** |
| Education | 3.19 (1.11) *** | 3.18 (1.10) *** | 4.90 (1.21) *** | 2.19 (1.19) * |
| Occ. status | 0.12 (0.33) | 0.87 (0.31) *** | 0.38 (0.37) | 0.55 (0.38) |
| R2 | 0.02 | 0.02 | 0.03 | 0.03 |
| Turkey | ||||
| Income | NA | −0.90 (1.21) | NA | 2.02 (0.97) ** |
| Education | NA | 7.25 (1.48) *** | NA | 4.91 (1.47) *** |
| Occ. status | NA | −0.27 (0.54) | NA | −0.82 (0.48) * |
| R2 | NA | 0.02 | NA | 0.01 |
| Ukraine | ||||
| Income | NA | NA | NA | 6.46 (0.83) *** |
| Education | NA | NA | NA | 10.26 (1.28) *** |
| Occ. status | NA | NA | NA | −0.31 (0.32) |
| R2 | NA | NA | NA | 0.06 |
| United Kingdom | ||||
| Income | 2.40 (0.34) *** | 2.50 (0.40) *** | 1.89 (0.30) *** | 3.98 (0.47) *** |
| Education | 2.68 (1.07) ** | 4.07 (1.31) *** | 2.26 (0.85) *** | 2.84 (0.92) *** |
| Occ. status | 0.58 (0.28) ** | 0.88 (0.31) *** | 0.88 (0.26) *** | 0.34 (0.26) |
| R2 | 0.03 | 0.03 | 0.02 | 0.03 |
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Alvarez-Galvez, J.; Rodero-Cosano, M.L.; Motrico, E.; Salinas-Perez, J.A.; Garcia-Alonso, C.; Salvador-Carulla, L. The Impact of Socio-Economic Status on Self-Rated Health: Study of 29 Countries Using European Social Surveys (2002–2008). Int. J. Environ. Res. Public Health 2013, 10, 747-761. https://doi.org/10.3390/ijerph10030747
Alvarez-Galvez J, Rodero-Cosano ML, Motrico E, Salinas-Perez JA, Garcia-Alonso C, Salvador-Carulla L. The Impact of Socio-Economic Status on Self-Rated Health: Study of 29 Countries Using European Social Surveys (2002–2008). International Journal of Environmental Research and Public Health. 2013; 10(3):747-761. https://doi.org/10.3390/ijerph10030747
Chicago/Turabian StyleAlvarez-Galvez, Javier, Maria Luisa Rodero-Cosano, Emma Motrico, Jose A. Salinas-Perez, Carlos Garcia-Alonso, and Luis Salvador-Carulla. 2013. "The Impact of Socio-Economic Status on Self-Rated Health: Study of 29 Countries Using European Social Surveys (2002–2008)" International Journal of Environmental Research and Public Health 10, no. 3: 747-761. https://doi.org/10.3390/ijerph10030747
APA StyleAlvarez-Galvez, J., Rodero-Cosano, M. L., Motrico, E., Salinas-Perez, J. A., Garcia-Alonso, C., & Salvador-Carulla, L. (2013). The Impact of Socio-Economic Status on Self-Rated Health: Study of 29 Countries Using European Social Surveys (2002–2008). International Journal of Environmental Research and Public Health, 10(3), 747-761. https://doi.org/10.3390/ijerph10030747