
High Cancer Burden in Elderly Chinese, 2005–2011

Abstract
:1. Introduction
2. Methods
2.1. Data Sources

2.2. Calculation of Indices
Potential Years of Life Lost
2.3. Potential Years of life Lost Rate
2.4. Disability-Adjusted Life Years
2.5. Disability Weight
2.6. Disability-Adjusted Life Year Rate
2.7. Relative Ratio of the Cancer Burden between the Elderly and Young Subjects
2.8. Statistical Analysis
2.9. Role of the Funding Source
2.10. Ethics Statement
3. Results
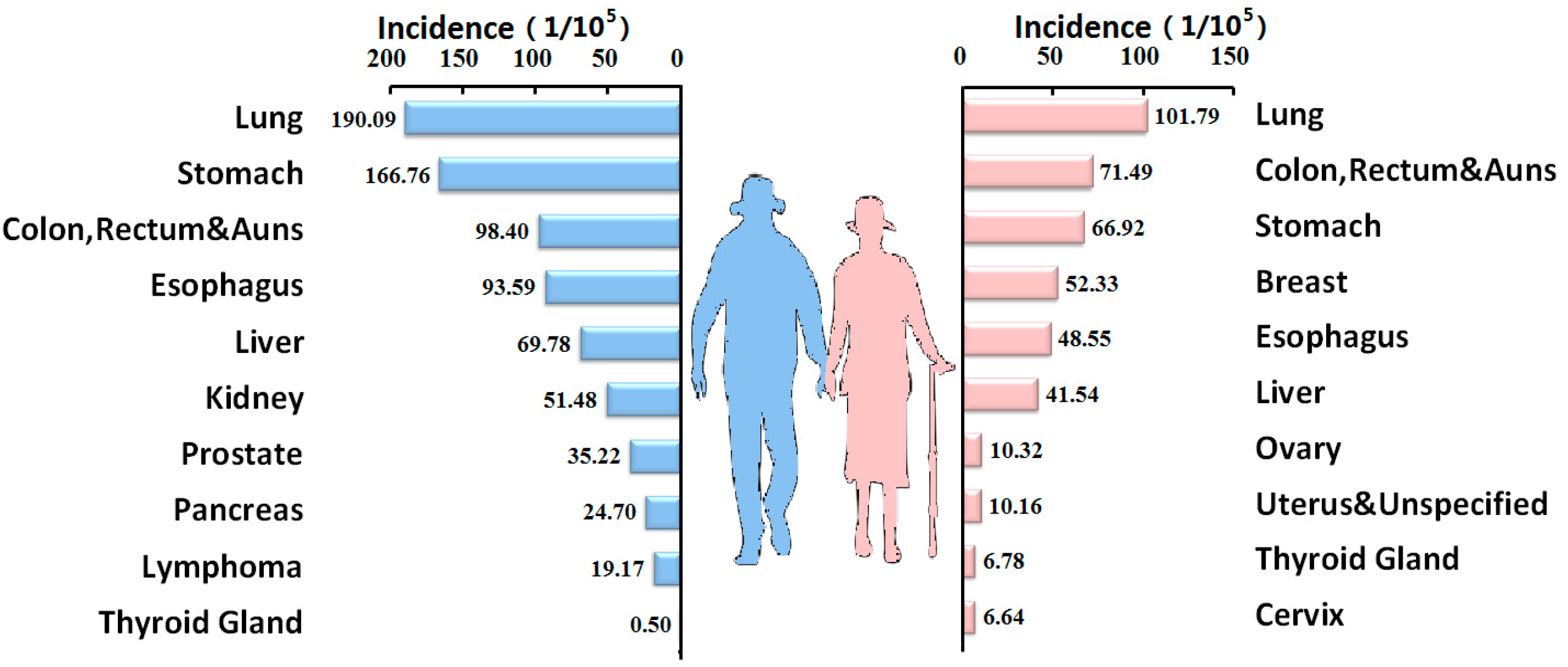
3.1. Cancer Incidence in the Elderly Population

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Age Group | All Districts | Urban Districts | Rural Districts | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Total | Male | Female | Total | Male | Female | Total | ||
| 2005 | ≥60 | 1310.93 | 789.78 | 1042.20 | 1247.38 | 792.42 | 1012.78 | 1523.81 | 744.67 | 1122.05 |
| <60 | 113.88 | 118.54 | 116.17 | 104.80 | 124.45 | 114.47 | 145.44 | 101.62 | 123.87 | |
| RR | 11.51 | 6.66 | 8.97 | 11.90 | 6.37 | 8.85 | 10.48 | 7.33 | 9.06 | |
| 2006 | ≥60 | 1344.62 | 792.05 | 1063.86 | 1295.83 | 792.95 | 1040.31 | 1552.05 | 787.71 | 1163.68 |
| <60 | 121.78 | 129.87 | 125.75 | 52.11 | 58.77 | 55.44 | 89.73 | 64.88 | 77.31 | |
| RR | 11.04 | 6.10 | 8.46 | 24.87 | 13.49 | 18.76 | 17.30 | 12.14 | 15.05 | |
| 2007 | ≥60 | 1316.00 | 791.96 | 1049.82 | 1323.40 | 837.49 | 1020.12 | 1535.06 | 783.63 | 1153.38 |
| <60 | 126.77 | 134.45 | 130.54 | 117.91 | 139.38 | 128.44 | 160.05 | 120.00 | 140.41 | |
| RR | 10.38 | 5.89 | 8.04 | 11.22 | 6.01 | 7.94 | 9.59 | 6.53 | 8.21 | |
| 2008 | ≥60 | 1359.93 | 824.08 | 1087.72 | 1472.00 | 918.93 | 1075.01 | 1480.57 | 797.01 | 1133.33 |
| <60 | 130.71 | 141.72 | 136.10 | 125.28 | 147.84 | 136.33 | 155.63 | 118.41 | 137.40 | |
| RR | 10.40 | 5.81 | 7.99 | 11.75 | 6.22 | 7.89 | 9.51 | 6.73 | 8.25 | |
| 2009 | ≥60 | 1326.41 | 804.97 | 1062.69 | 1566.30 | 971.95 | 1076.66 | 1311.66 | 739.83 | 1022.45 |
| <60 | 132.37 | 139.89 | 136.05 | 130.47 | 149.69 | 139.88 | 137.55 | 118.61 | 128.27 | |
| RR | 10.02 | 5.75 | 7.81 | 12.01 | 6.49 | 7.70 | 9.54 | 6.24 | 7.97 | |
| 2010 | ≥60 | 1297.55 | 727.21 | 1006.73 | 1523.32 | 893.49 | 1034.53 | 962.74 | 1302.32 | 1135.89 |
| <60 | 117.42 | 114.41 | 115.96 | 111.50 | 120.19 | 115.71 | 115.06 | 126.96 | 120.83 | |
| RR | 11.05 | 6.36 | 8.68 | 13.66 | 7.43 | 8.94 | 8.37 | 10.26 | 9.40 | |
| 2011 | ≥60 | 1760.32 | 688.54 | 1212.01 | 1291.49 | 978.97 | 1131.61 | 1283.72 | 890.98 | 1082.80 |
| <60 | 136.16 | 124.43 | 130.49 | 112.54 | 98.54 | 105.77 | 120.84 | 83.27 | 102.67 | |
| RR | 12.93 | 5.53 | 9.29 | 11.48 | 9.93 | 10.70 | 10.62 | 10.70 | 10.55 | |
| Total | ≥60 | 1390.32 * | 773.88 * | 1076.24 | 1280.78 | 820.89 | 1046.46 # | 1399.86 | 864.43 | 1127.06 # |
| <60 | 125.67 | 129.03 | 127.11 | 115.38 | 128.24 | 121.47 | 143.21 | 113.38 | 128.42 | |
| RR | 11.06 | 6.00 | 8.47 | 11.10 | 6.40 | 8.62 | 9.77 | 7.62 | 8.78 | |

| Rank | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICD10 | Incidence | ICD10 | Incidence | ICD10 | Incidence | ICD10 | Incidence | ICD10 | Incidence | ICD10 | Incidence | ICD10 | Incidence | |
| 1 | C33~34 | 47.34 | C33~34 | 49.7 | C33~34 | 51.25 | C33~34 | 54.75 | C33~34 | 53.57 | C33~34 | 46.08 | C33~34 | 48.32 |
| 2 | C16 | 32.23 | C16 | 35.02 | C16 | 33.68 | C16 | 37.88 | C16 | 36.21 | C50 | 32.43 | C50 | 37.86 |
| 3 | C22 | 26.89 | C18~21 | 29.07 | C18~21 | 29.62 | C18~21 | 31.39 | C18~21 | 29.44 | C16 | 30.77 | C16 | 31.21 |
| 4 | C18~21 | 26.89 | C22 | 26.6 | C22 | 27.11 | C22 | 28.17 | C22 | 28.71 | C22 | 27.29 | C22 | 26.39 |
| 5 | C50 | 20.13 | C50 | 21.05 | C50 | 21.59 | C50 | 23.82 | C15 | 22.14 | C15 | 21.88 | C18~21 | 23.03 |
| 6 | C15 | 19.55 | C15 | 18.79 | C15 | 19.86 | C15 | 20.85 | C50 | 21.21 | C18~21 | 20.90 | C15 | 21.62 |
| 7 | C25 | 6.59 | C25 | 7.45 | C25 | 7.28 | C25 | 8.55 | C25 | 7.28 | C53 | 11.98 | C53 | 13.4 |
| 8 | C67 | 6.41 | C67 | 6.85 | C67 | 6.98 | C67 | 7.49 | C81~85, 88, 90, 96 | 6.68 | C54~55 | 7.44 | C54~55 | 8.79 |
| 9 | C81~85, 88, 90, 96 | 6.16 | C81~85, 88, 90, 96 | 6.43 | C70~72 | 6.79 | C81~85, | 7.21 | C67 | 6.61 | C56 | 6.47 | C61 | 7.1 |
| 88, 90, 96 | ||||||||||||||
| 10 | C70~72 | 5.91 | C70~72 | 6.39 | C81~85, 88, 90, 96 | 6.06 | C70~72 | 7.03 | C73 | 6.56 | C70~72 | 6.00 | C56 | 6.89 |
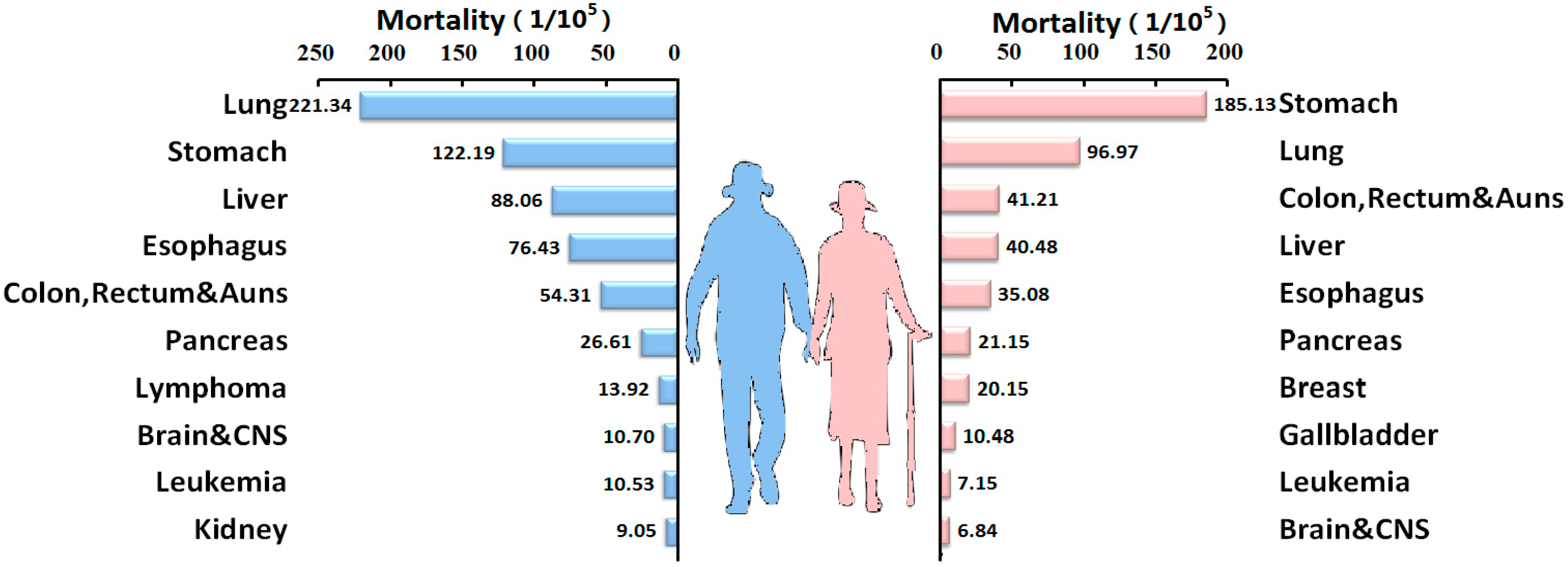
3.2. Cancer-Related Mortality in the Elderly Population
| Year | Age Group | All Districts | Urban District | Rural District | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Total | Male | Female | Total | Male | Female | Total | ||
| 2005 | ≥60 | 1054.66 | 591.13 | 815.64 | 949.53 | 572.18 | 754.95 | 1307.74 | 655.04 | 971.18 |
| <60 | 67.88 | 40.97 | 54.64 | 56.50 | 36.86 | 46.83 | 105.72 | 54.59 | 80.56 | |
| RR | 15.54 | 14.43 | 14.93 | 16.81 | 15.52 | 16.12 | 12.37 | 12.00 | 12.06 | |
| 2006 | ≥60 | 1042.03 | 575.40 | 804.93 | 980.75 | 558.20 | 766.05 | 1310.35 | 651.28 | 975.47 |
| <60 | 71.64 | 42.60 | 57.38 | 28.33 | 16.91 | 22.62 | 64.89 | 33.61 | 49.25 | |
| RR | 14.55 | 13.51 | 14.03 | 34.62 | 33.01 | 33.87 | 20.19 | 19.38 | 19.81 | |
| 2007 | ≥60 | 1025.83 | 573.51 | 796.08 | 996.27 | 580.16 | 743.73 | 1322.58 | 658.20 | 985.11 |
| <60 | 74.60 | 42.77 | 58.98 | 64.99 | 39.18 | 52.33 | 109.05 | 55.92 | 82.98 | |
| RR | 13.75 | 13.41 | 13.50 | 15.33 | 14.81 | 14.21 | 12.13 | 11.77 | 11.87 | |
| 2008 | ≥60 | 1016.81 | 565.05 | 787.32 | 1064.44 | 608.57 | 751.71 | 1247.22 | 630.46 | 933.91 |
| <60 | 73.58 | 44.07 | 59.13 | 67.06 | 41.18 | 54.39 | 101.38 | 56.75 | 79.52 | |
| RR | 13.82 | 12.82 | 13.32 | 15.87 | 14.78 | 13.82 | 12.30 | 11.11 | 11.74 | |
| 2009 | ≥60 | 1016.70 | 566.45 | 788.98 | 1149.20 | 659.30 | 766.66 | 1104.36 | 469.52 | 783.29 |
| <60 | 75.22 | 44.45 | 60.15 | 69.48 | 41.63 | 55.84 | 88.34 | 51.25 | 70.18 | |
| RR | 13.52 | 12.74 | 13.12 | 16.54 | 15.84 | 13.73 | 12.50 | 9.16 | 11.16 | |
| 2010 | ≥60 | 989.67 | 529.83 | 755.20 | 1120.87 | 628.02 | 748.37 | 1020.56 | 516.96 | 763.78 |
| <60 | 68.31 | 41.00 | 55.07 | 60.61 | 37.95 | 49.63 | 76.35 | 44.23 | 60.78 | |
| RR | 14.49 | 12.92 | 13.71 | 18.49 | 16.55 | 15.08 | 13.37 | 11.69 | 12.57 | |
| 2011 | ≥60 | 1345.95 | 474.91 | 900.34 | 949.53 | 572.18 | 754.95 | 951.18 | 602.72 | 772.92 |
| <60 | 78.09 | 40.56 | 59.94 | 56.50 | 36.86 | 46.83 | 61.17 | 25.19 | 43.77 | |
| RR | 17.24 | 11.71 | 15.02 | 16.81 | 15.52 | 16.12 | 15.55 | 23.93 | 17.66 | |
| Total | ≥60 | 1071.48 * | 553.15 * | 807.38 | 950.02 | 556.30 | 749.42 # | 1206.81 | 607.02 | 901.21 # |
| <60 | 72.80 | 42.34 | 57.82 | 62.43 | 36.53 | 49.69 | 96.65 | 51.02 | 74.23 | |
| RR | 14.72 | 13.06 | 13.96 | 15.22 | 15.23 | 15.08 | 12.49 | 11.90 | 12.14 | |
| Rank | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICD10 | Mortality | ICD10 | Mortality | ICD10 | Mortality | ICD10 | Mortality | ICD10 | Mortality | ICD10 | Mortality | ICD10 | Mortality | |
| 1 | C33~C34 | 42.59 | C33~C34 | 44.15 | C33~C34 | 45.5 | C33~C34 | 46.07 | C33~C34 | 45.57 | C33~34 | 37 | C33~34 | 39.27 |
| 2 | C22 | 25.04 | C16 | 26.08 | C22 | 25.91 | C16 | 26.58 | C22 | 26.04 | C22 | 23.76 | C22 | 23.93 |
| 3 | C16 | 23.9 | C22 | 25.83 | C16 | 24.59 | C22 | 25.84 | C16 | 25.88 | C16 | 21.89 | C16 | 22.08 |
| 4 | C15 | 15.78 | C15 | 15.26 | C15 | 15.8 | C15 | 16.24 | C15 | 16.77 | C15 | 15.85 | C15 | 16.25 |
| 5 | C18~21 | 12.83 | C18~21 | 13.39 | C18~21 | 14.15 | C18~21 | 14.82 | C18~21 | 14.23 | C18~21 | 10.05 | C18~21 | 11.11 |
| 6 | C25 | 6.09 | C25 | 7.02 | C25 | 7.15 | C25 | 7.56 | C25 | 6.61 | C50 | 8.65 | C50 | 9.21 |
| 7 | C50 | 4.85 | C50 | 4.59 | C50 | 4.67 | C50 | 5.23 | C50 | 5.13 | C25 | 4.39 | C25 | 5.4 |
| 8 | C91~95 | 3.77 | C91~95 | 4.09 | C91~95 | 4.04 | C91~95 | 3.99 | C91~95 | 4.28 | C70~72 | 3.55 | C70~72 | 3.77 |
| 9 | C70~72 | 3.46 | C70~72 | 4.08 | C70~72 | 3.95 | C70~72 | 3.99 | C70~72 | 3.87 | C91~95 | 3.47 | C53 | 3.56 |
| 10 | C81~85, 88, 90, 96 | 3.4 | C81~85, 88, 90, 96 | 3.63 | C81~85, 88, 90, 96 | 3.64 | C81~85, 88, 90, 96 | 3.96 | C81~85, 88, 90, 96 | 3.75 | C53 | 3.37 | C91~95 | 3.53 |

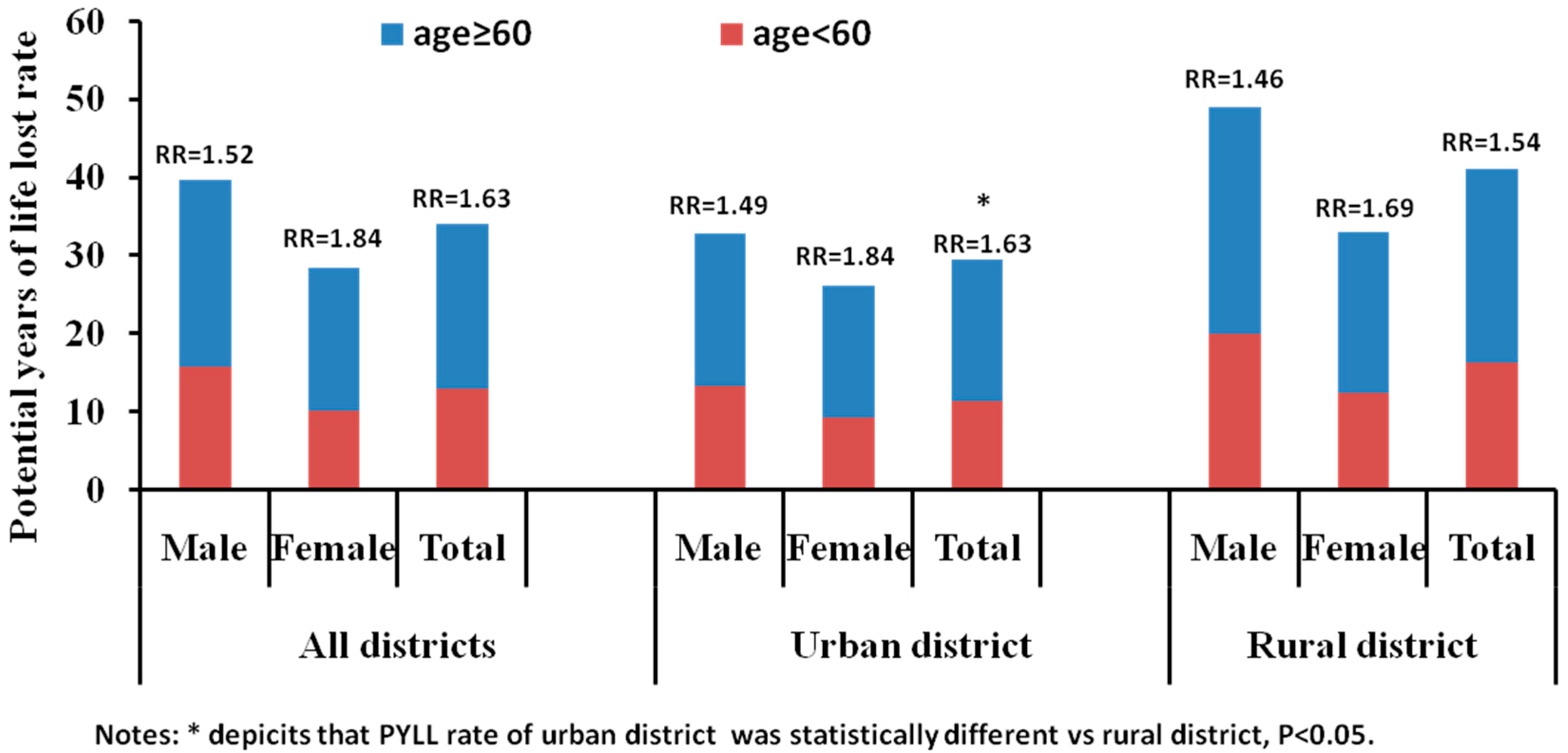
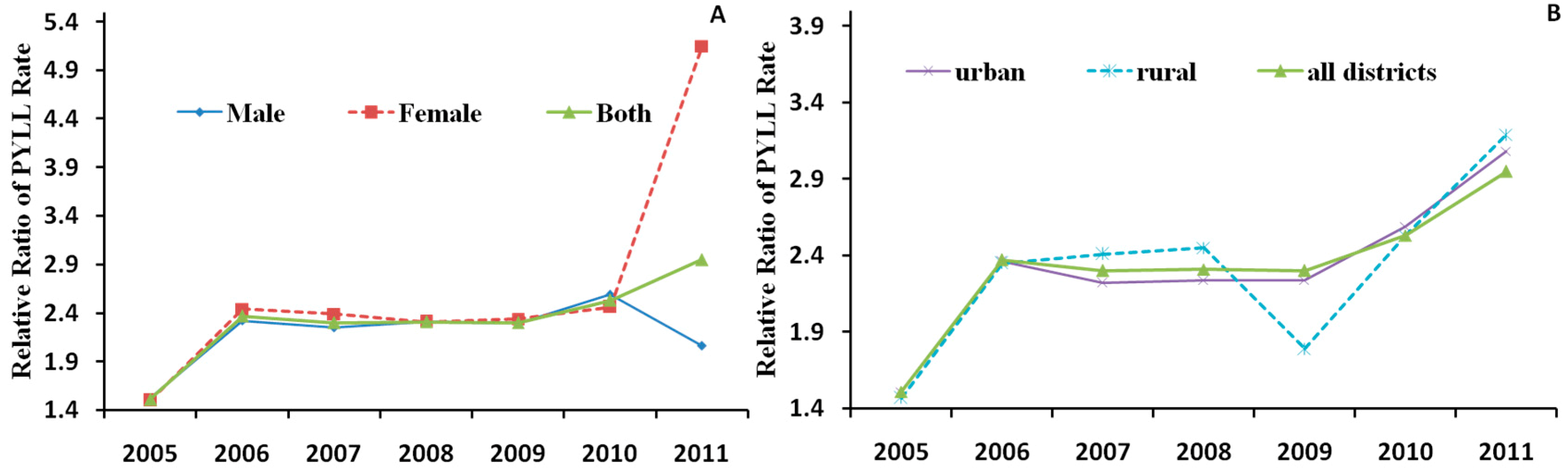
3.3. Potential Years of Life Lost in the Elderly Population
| Year | Age Group | All Districts | Urban District | Rural District | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | Total | Male | Female | Total | Male | Female | Total | ||
| 2005 | ≥60 | 1,940,975 | 1,435,404 | 3,376,379 | 712,643 | 554,254 | 1,266,896 | 1,585,342 | 1,083,912 | 2,669,253 |
| <60 | 8,576,569 | 5,898,270 | 14,474,840 | 3,114,428 | 2,315,123 | 5,429,551 | 7,399,534 | 4,342,268 | 11,741,801 | |
| 2006 | ≥60 | 1,710,157 | 1,176,729 | 2,886,887 | 662,942 | 464,683 | 1,127,625 | 1,399,645 | 938,557 | 2,338,202 |
| <60 | 8,545,603 | 5,639,417 | 14,185,020 | 3,288,525 | 2,265,025 | 5,553,550 | 7,284,433 | 4,294,740 | 11,579,174 | |
| 2007 | ≥60 | 1,760,106 | 1,178,332 | 2,938,438 | 673,990 | 469,998 | 1,143,988 | 1,415,688 | 896,830 | 2,312,518 |
| <60 | 8,846,914 | 5,568,689 | 14,415,603 | 3,494,023 | 2,323,737 | 5,817,760 | 6,976,145 | 3,864,941 | 10,841,085 | |
| 2008 | ≥60 | 1,804,156 | 1,213,281 | 3,017,437 | 730,199 | 509,699 | 1,239,898 | 1,409,673 | 873,989 | 2,283,662 |
| <60 | 8,650,169 | 5,764,012 | 14,414,180 | 3,615,622 | 2,483,624 | 6,099,245 | 6,361,681 | 3,897,853 | 10,259,535 | |
| 2009 | ≥60 | 1,930,328 | 1,296,997 | 3,227,326 | 810,936 | 553,286 | 1,364,222 | 1,238,603 | 304,030 | 1,542,633 |
| <60 | 8,827,847 | 5,735,294 | 14,563,141 | 3,816,134 | 2,524,816 | 6,340,951 | 5,480,623 | 3,466,208 | 8,946,831 | |
| 2010 | ≥60 | 1,852,363 | 1,182,459 | 3,034,822 | 851,231 | 555,158 | 1,406,389 | 1,025,772 | 636,823 | 1,662,595 |
| <60 | 8,420,369 | 5,464,164 | 13,884,533 | 3,736,408 | 2,541,385 | 6,277,793 | 4,676,751 | 2,923,219 | 7,599,970 | |
| 2011 | ≥60 | 3,977,573 | 4,442,974 | 8,420,547 | 1,324,583 | 2,057,240 | 3381823 | 1,524,159 | 2,387,994 | 3,912,153 |
| <60 | 12,804,070 | 5,125,377 | 17,929,447 | 4,392,512 | 2,504,467 | 6,896,979 | 5,058,449 | 2,636,394 | 7,694,843 | |
| Total | ≥60 | 14,975,658 | 11,926,176 | 26,901,836 | 5,766,524 | 5,164,318 | 10,930,841 | 9,598,882 | 7,122,135 | 16,721,016 |
| <60 | 64,671,541 | 39,195,223 | 103,866,764 | 25,457,652 | 16,958,177 | 42,415,829 | 43,237,616 | 25,425,623 | 68,663,239 | |


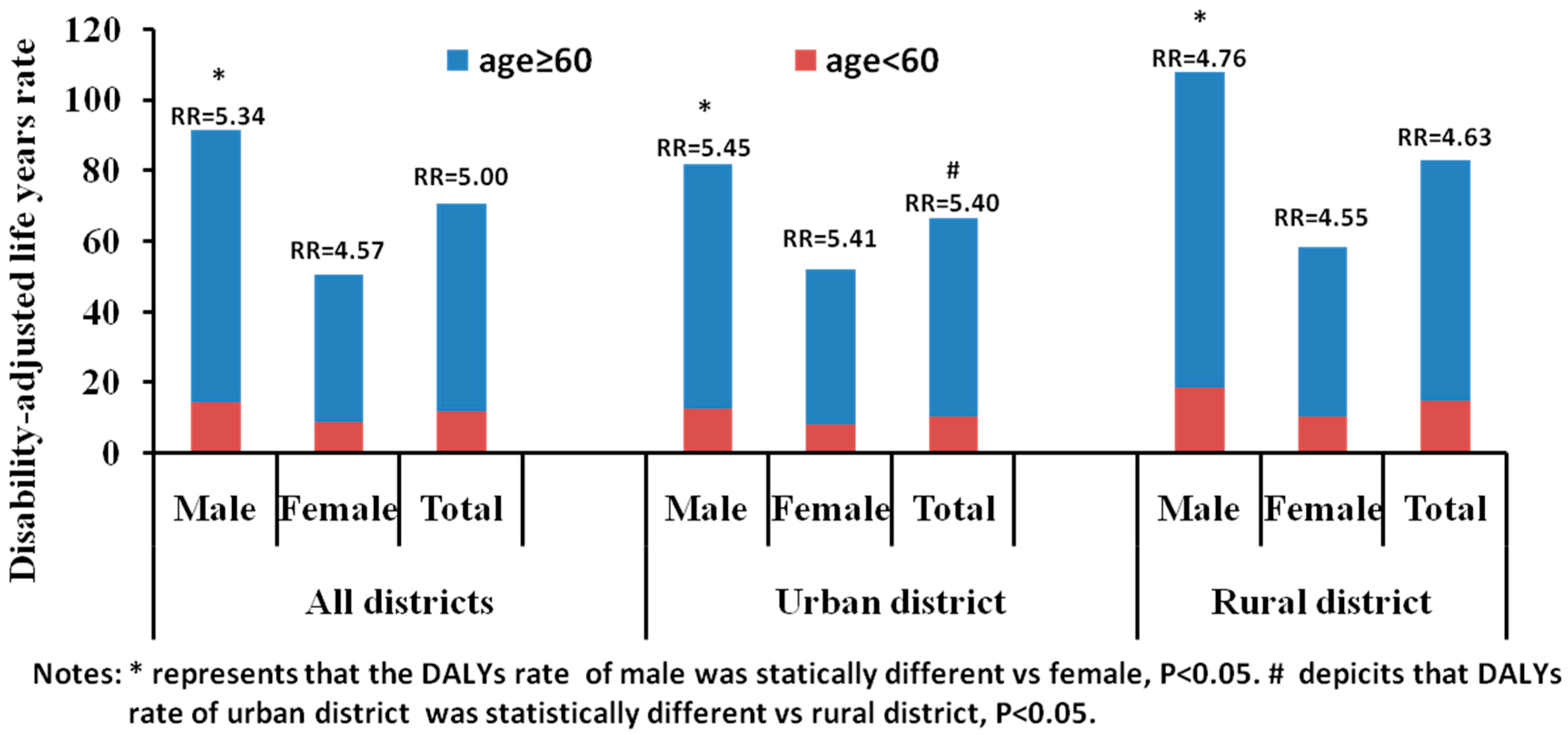
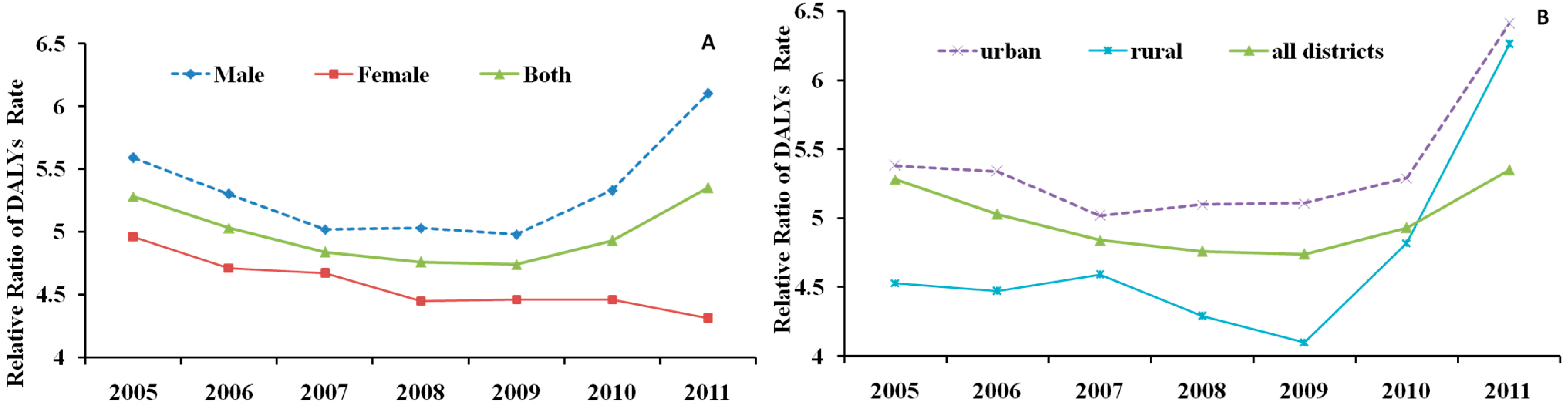
3.4. Disability-Adjusted Life Years in the Elderly Population


4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO. GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012. Available online: http://globocan.iarc.fr (accessed on 17 May 2015).
- Ferlay, J.; Shin, H.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D. GLOBOCAN 2008, Cancer Incidence and Mortality Worldwide; IARC Cancer Base No. 10; International Agency for Research on Cancer: Lyon, France, 2010; Volume 2010, p. 29. [Google Scholar]
- Liu, L. The global significance of China’s cancer burden and control effort. Ann. Transl. Med. 2014, 2. [Google Scholar] [CrossRef]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Ezzati, M.; Flaxman, A.D.; Lim, S.; Lozano, R.; Michaud, C.; Naghavi, M.; Salomon, J.A.; Shibuya, K.; Vos, T.; Wikler, D.; Lopez, A.D. GBD 2010: Design, definitions, and metrics. Lancet 2012, 380, 2063–2066. [Google Scholar] [CrossRef]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2011; China Statistics Press: Beijing, China, 2012. [Google Scholar]
- Chen, W.; Zheng, R.; Zeng, H.; Zhang, S. Trend analysis of the changes of male/female, urban/rural incidences and average age of cancer patients in China 1989–2008. Chin. J. Oncol. 2014, 36, 796–800. [Google Scholar]
- Leng, S.X.; Tian, X.P.; Durso, S.; Lazarus, G.; Lu, C.; Park, E.; Xie, H.; Kang, L.; Li, D.; Shen, T.; Fried, L.P. The aging population and development of geriatrics in China. J. Am. Geriatr. Soc. 2008, 56, 571–573. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Zheng, R.; Zhang, S.; Zhao, P.; Zeng, H.; Zou, X. Annual report on status of cancer in China, 2012. Chin. J. Cancer Res. 2014, 26, 48–58. [Google Scholar] [PubMed]
- Chen, W.; Zheng, R.; Zeng, H.; Zhang, S.; He, J. Annual report on status of cancer in China, 2011. Chi. J. Cancer Res. 2015, 27, 2–12. [Google Scholar]
- Chen, W.Q.; Zheng, R.S.; Zhang, S.W.; Zhao, P.; Zeng, H.M.; Zou, X.N.; He, J. Annual report on status of cancer in China, 2010. Chin. J. Cancer Res. 2014, 26, 48–58. [Google Scholar] [PubMed]
- Chen, W.; Zheng, R.; Zhang, S.; Zhao, P.; Zeng, H.; Zou, X. Annual report on status of cancer in China, 2009. Chin. J. Cancer Res. 2011, 23, 43–53. [Google Scholar]
- Chen, W.; Zheng, R.; Zhang, S.; Zhao, P.; Zeng, H.; Zou, X. Annual report on status of cancer in China, 2008. Chin. J. Cancer Res. 2010, 22, 42–52. [Google Scholar]
- Chen, W.; Zheng, R.; Zhang, S.; Zhao, P.; Li, G.; Wu, L. Report of cancer incidence and mortality in China, 2011. Chin. J. Cancer Res. 2014, 24, 1–10. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2006; China Statistics Press: Beijing, China, 2007. [Google Scholar]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2007; China Statistics Press: Beijing, China, 2008. [Google Scholar]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2008; China Statistics Press: Beijing, China, 2009. [Google Scholar]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2009; China Statistics Press: Beijing, China, 2010. [Google Scholar]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2010; China Statistics Press: Beijing, China, 2011. [Google Scholar]
- National Bureau of Statistics of China. China Population and Employment Statistics Yearbook, 2012; China Statistics Press: Beijing, China, 2013. [Google Scholar]
- Morrow, R.H.; Hyder, A.A.; Murray, C.J.; Lopez, A.D. Measuring the burden of disease. Lancet 1998, 352, 1859–1861. [Google Scholar] [CrossRef]
- WHO. WHO Methods and Data Sources for Global Burden of Disease Estimates 2000–2011. Available online: http://www.who.int/healthinfo/statistics/GlobalDALYmethods_2000_2011.pdf?ua=1 (accessed on 10 May 2015).
- WHO. Global Burden of Disease 2004 Update: Disability Weights for Diseases and Conditions. Available online: http://www.who.int/healthinfo/global_burden_disease/GBD2004_DisabilityWeights.pdf (accessed on 10 May 2015).
- World Health Organization. Available online: www.who.int/healthinfo/global_burden_disease/tools_software/en/Weights.pdf (accessed on 10 May 2015).
- Chen, H.; Wang, H.; Crimmins, E.M.; Chen, G.; Huang, C.; Zheng, X. The contributions of diseases to disability burden among the elderly population in China. J. Aging Health 2014, 26, 261–282. [Google Scholar] [CrossRef] [PubMed]
- Wong, G.; Lim, W.H.; Lewis, J.; Craig, J.C.; Turner, R.; Zhu, K.; Lim, E.M.; Prince, R. Vitamin D and cancer mortality in elderly women. BMC Cancer 2015, 15. [Google Scholar] [CrossRef] [PubMed]
- Kidane, D.; Chae, W.J.; Czochor, J.; Eckert, K.A.; Glazer, P.M.; Bothwell, A.L.; Sweasy, J.B. Interplay between DNA repair and inflammation, and the link to cancer. Crit. Rev. Biochem. Mol. Biol. 2014, 49, 116–139. [Google Scholar] [CrossRef] [PubMed]
- Wolfgang, C.L.; Herman, J.M.; Laheru, D.A.; Klein, A.P.; Erdek, M.A.; Fishman, E.K.; Hruban, R.H. Recent progress in pancreatic cancer. CA Cancer J. Clin. 2013, 63, 318–348. [Google Scholar] [CrossRef] [PubMed]
- Zeeneldin, A.A.; Ramadan, H.; El Gammal, M.M.; Saber, M.M.; Elgamal, D.; Sherisher, M.A. Gastric carcinoma at Tanta Cancer Center: A comparative retrospective clinico-pathological study of the elderly versus the non-elderly. J. Egypt. Natl. Cancer Inst. 2014, 26, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.M.; Wei, C.; Ensor, J.E.; Smolenski, D.J.; Amos, C.I.; Levin, B.; Berry, D.A. Meta-analyses of colorectal cancer risk factors. Cancer Cause. Control 2013, 24, 1207–1222. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Lopez, A.D. The utility of DALYs for public health policy and research: A reply. Bull. World Health Organ. 1997, 75, 377–381. [Google Scholar] [PubMed]
- Soerjomataram, I.; Lortet-Tieulent, J.; Parkin, D.M.; Ferlay, J.; Mathers, C.; Forman, D.; Bray, F. Global burden of cancer in 2008: A systematic analysis of disability-adjusted life-years in 12 world regions. Lancet 2012, 380, 1840–1850. [Google Scholar] [CrossRef]
- Long, M. The restriction of population aging on the population development strategy of China and the solution. Popul. Dev. 2013, 19, 52–63. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Zhang, X.; Yan, Y.; Wang, K.; Rui, D.; Pang, L.; Li, F. High Cancer Burden in Elderly Chinese, 2005–2011. Int. J. Environ. Res. Public Health 2015, 12, 12196-12211. https://doi.org/10.3390/ijerph121012196
Li S, Zhang X, Yan Y, Wang K, Rui D, Pang L, Li F. High Cancer Burden in Elderly Chinese, 2005–2011. International Journal of Environmental Research and Public Health. 2015; 12(10):12196-12211. https://doi.org/10.3390/ijerph121012196
Chicago/Turabian StyleLi, Shugang, Xuefei Zhang, Yizhong Yan, Kui Wang, Dongsheng Rui, Lijuan Pang, and Feng Li. 2015. "High Cancer Burden in Elderly Chinese, 2005–2011" International Journal of Environmental Research and Public Health 12, no. 10: 12196-12211. https://doi.org/10.3390/ijerph121012196
APA StyleLi, S., Zhang, X., Yan, Y., Wang, K., Rui, D., Pang, L., & Li, F. (2015). High Cancer Burden in Elderly Chinese, 2005–2011. International Journal of Environmental Research and Public Health, 12(10), 12196-12211. https://doi.org/10.3390/ijerph121012196