
Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
Background
2. Methods
2.1. Design
2.2. Quality Appraisal
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Search Outcomes
3.2. Study Characteristics
3.3. Factors Eligible for Meta-Analysis








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Factors | Overall DSM Performance | Physical Activity | Taking Medications | SMBG | Foot Care | Regulating Highs and Lows in Blood Glucose | Diet Modification | Smoking |
|---|---|---|---|---|---|---|---|---|
| Overall Coping Score | 0.33 (0.25, 0.41) | 0.29 (0.21, 0.38) | NS | 0.18 (0.09, 0.27) | 0.30 (0.22, 0.39) | 0.27 (0.18, 0.36) | 0.22 (0.08, 0.35) | |
| Avoidance | 0.11 (0.03, 0.19) | NS | NS | NS | 0.13 (0.05, 0.21) | NS | NS | |
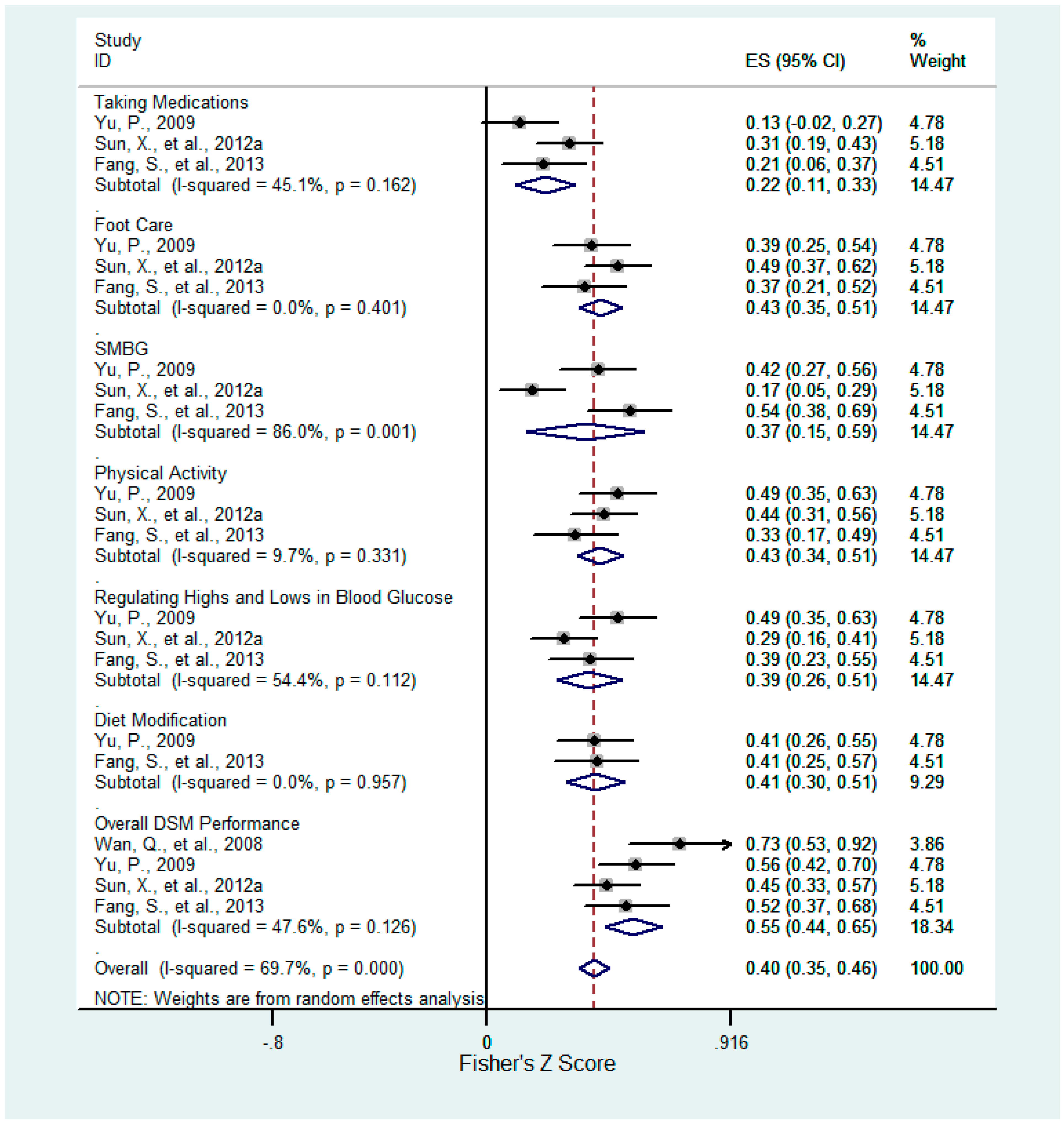
| Confrontation | 0.50 (0.42, 0.57) | 0.40 (0.33, 0.47) | 0.22 (0.11, 0.32) | 0.35 (0.15, 0.53) | 0.40 (0.33, 0.47) | 0.37 (0.26, 0.47) | 0.39 (0.29, 0.47) | |
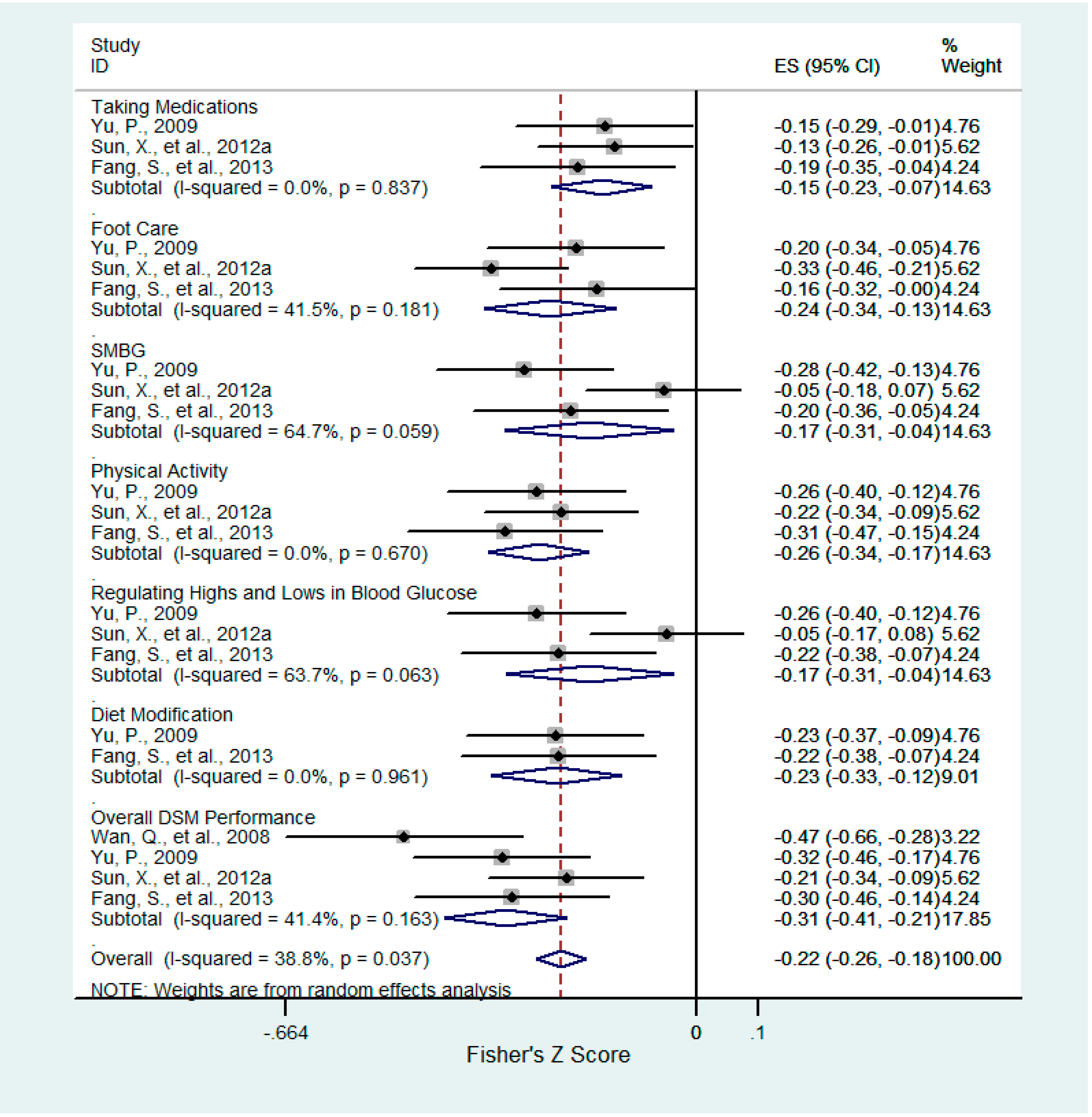
| Acceptance−Resignation | −0.30 (−0.39, −0.21) | −0.25 (−0.32, −0.17) | −0.15 (−0.23, −0.07) | −0.17 (−0.30, −0.04) | −0.23 (−0.33, −0.13) | −0.17 (−0.30, −0.04) | −0.22 (−0.32, −0.12) | |
| Overall Health Beliefs | 0.42 (0.35, 0.48) | 0.23 (0.15, 0.30) | 0.30 (0.24, 0.36) | 0.30 (0.20, 0.40) | 0.36 (0.30, 0.42) | 0.35 (0.22, 0.46) | 0.34 (0.25, 0.41) | |
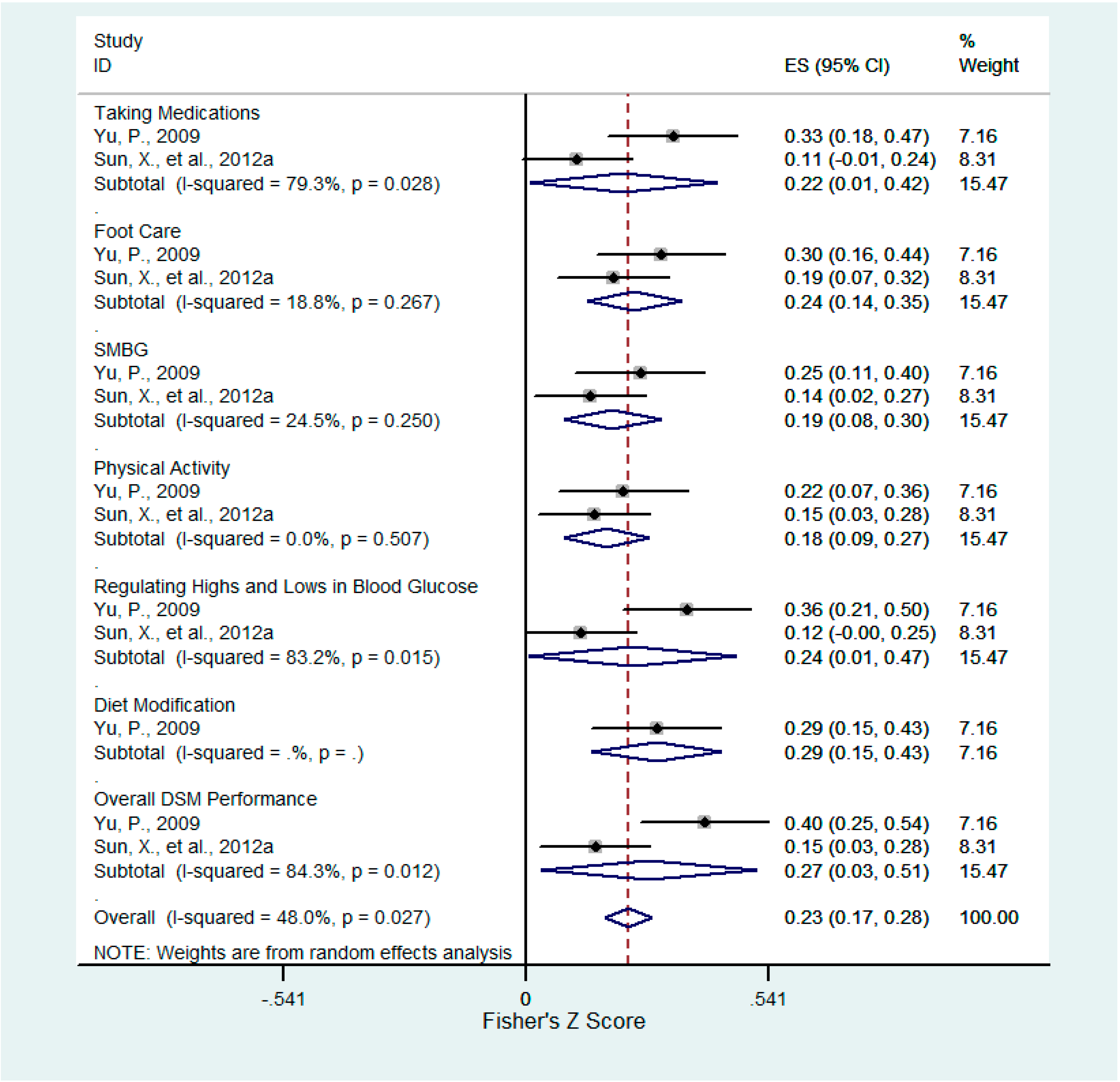
| Perceived Susceptibility | 0.27 (0.03, 0.47) | 0.18 (0.09, 0.27) | 0.21 (0.01, 0.40) | 0.19 (0.08, 0.29) | 0.24 (0.14, 0.33) | 0.23 (0.01, 0.44) | 0.28 (0.15, 0.41) | |
| Perceived Benefits | 0.41 (0.30, 0.51) | 0.26 (0.17, 0.34) | 0.31 (0.23, 0.39) | 0.21 (0.08, 0.34) | 0.37 (0.29, 0.45) | NS | 0.37 (0.24, 0.49) | |
| Perceived Barriers | 0.36 (0.27, 0.45) | 0.25 (0.16, 0.33) | 0.28 (0.20, 0.37) | 0.27 (0.18, 0.35) | 0.34 (0.22, 0.46) | 0.32 (0.02, 0.57) | 0.24 (0.10, 0.37) | |
| Perceived Severity | NS | NS | NS | NS | NS | NS | NS | |
| Cues to Action | 0.26 (0.11, 0.41) | 0.26 (0.17, 0.35) | 0.20 (0.10, 0.28) | 0.14 (0.04, 0.23) | 0.20 (0.06, 0.33) | NS | 0.41 (0.29, 0.52) | |
| Chance Externality | NS | NS | −0.13 (−0.22, −0.03) | NS | −0.08 (−0.15, −0.01) | NS | ||
| Internality | 0.15 (0.05, 0.24) | NS | NS | NS | NS | NS | ||
| Powerful Others Externality | 0.33 (0.24, 0.41) | NS | NS | 0.23 (0.06, 0.37) | NS | NS | ||
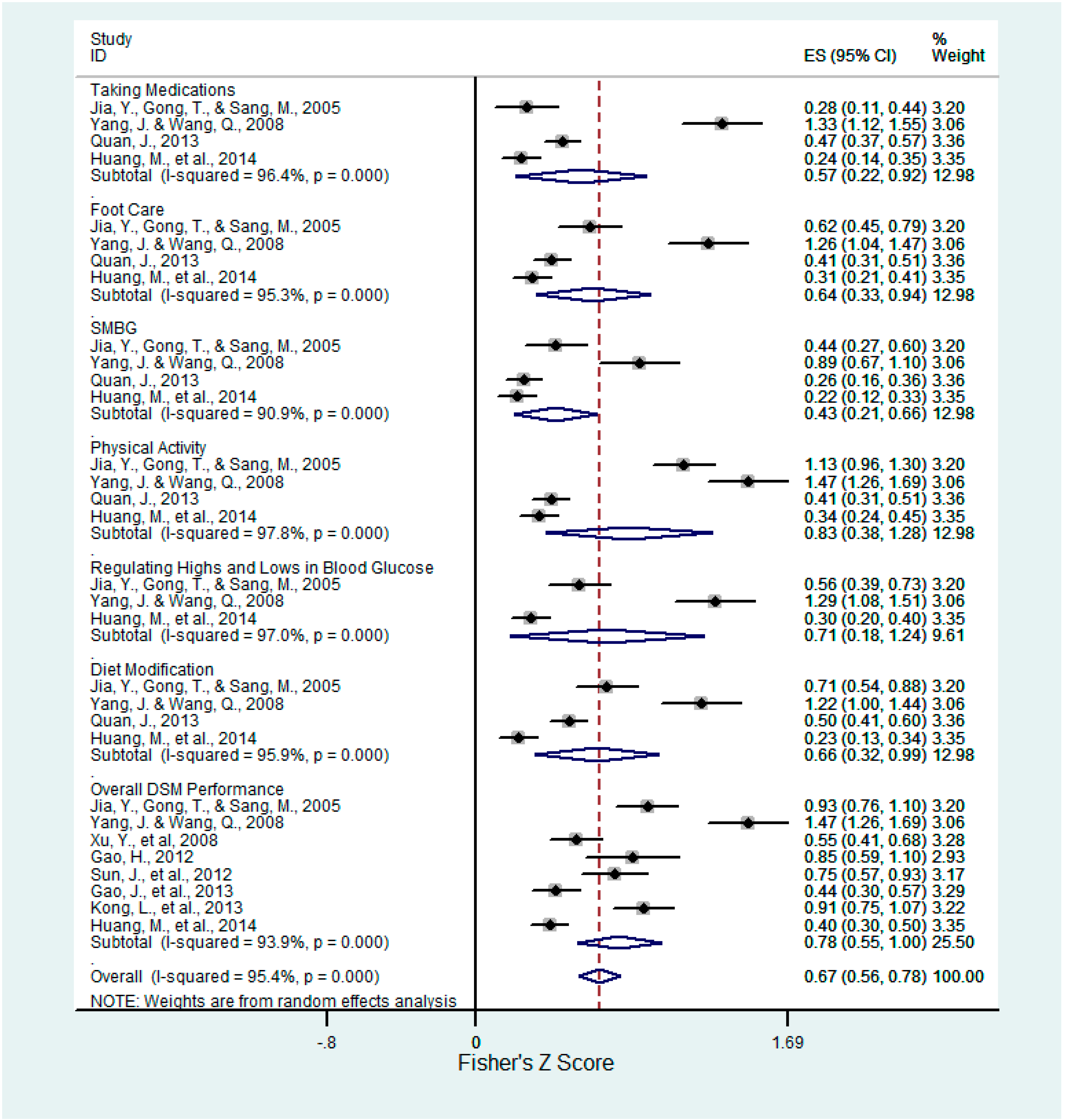
| Self−Efficacy | 0.70 (0.56, 0.80) | 0.68 (0.36, 0.86) | 0.52 (0.22, 0.73) | 0.41 (0.21, 0.58) | 0.56 (0.31, 0.74) | 0.61 (0.18, 0.84) | 0.58 (0.31, 0.76) | |
| Social Support | 0.45 (0.15, 0.67) | 0.21 (0.14, 0.28) | NS | 0.29 (0.11, 0.45) | 0.27 (0.11, 0.41) | 0.22 (0.13, 0.31) | NS | |
| Depressive Symptoms | −0.37 (−0.48, −0.25) | NS | NS | −0.28 (−0.40, −0.16) | −0.34 (−0.47, −0.19) | NS | −0.28 (−0.36, −0.19) | |
| Diabetes Knowledge | 0.23 (0.08, 0.38) | NS | 0.11 (0.04, 0.18) | 0.19 (0.08, 0.30) | 0.16 (0.08, 0.24) | 0.25 (0.12, 0.38) | NS | −0.26 (−0.39, −0.13) |
| Complications * | NS | |||||||
| Female * | 1.89 (0.98, 2.79) | |||||||
| Health Education * | NS | 1.97 (0.11, 3.83) | NS | NS | 2.14 (1.18, 3.10) | 2.00 (0.05, 3.95) | NS | |
| Living Alone * | −2.74 (−4.01, 1.47) | |||||||
| Admission History * | −1.53 (−6.90, 3.83) |
| Factors | Overall DSM Performance | Physical Activity | Taking Medication | SMBG | Foot Care | Regulating Highs and Lows in Blood Glucose | Diet Modification | Smoking |
|---|---|---|---|---|---|---|---|---|
| Overall Coping Score | NS | NS | p = 0.023 (80.6%) | NS | NS | NS | ||
| Avoidance | NS | NS | NS | NS | NS | NS | NS | |
| Confrontation | NS | NS | NS | p = 0.001 (86.0%) | NS | NS | NS | |
| Acceptance-Resignation | NS | NS | NS | NS | NS | NS | NS | |
| Overall Health Beliefs | NS | NS | NS | NS | NS | p = 0.009 (74.3%) | NS | |
| Perceived Susceptibility | p = 0.012 (84.3%) | NS | p = 0.028 (79.3%) | NS | NS | p = 0.015 (83.2%) | ||
| Perceived Benefits | NS | NS | NS | NS | NS | p < 0.001 (93.1%) | ||
| Perceived Barriers | NS | NS | NS | NS | NS | p = 0.001 (90.7%) | ||
| Perceived Severity | NS | NS | p = 0.014 (83.3%) | p = 0.020 (81.5%) | NS | p = 0.010 (85.1%) | ||
| Cues to Action | NS | NS | NS | NS | NS | p = 0.007 (86.0%) | ||
| Chance Externality | NS | NS | NS | NS | NS | |||
| Internality | p = 0.015 (83.1%) | NS | p = 0.035 (77.6%) | NS | ||||
| Powerful Others Externality | p < 0.001 (95.0%) | p = 0.017 (82.3%) | p = 0.000 (93.7%) | p < 0.001 (90.3%) | ||||
| Self-Efficacy | p < 0.001 (95.3%) | p < 0.001 (97.8%) | p < 0.001 (96.4%) | p < 0.001 (90.9%) | p = 0.000 (95.3%) | p < 0.001 (97.0%) | p < 0.000 (95.9%) | |
| Social Support | p < 0.001 (95.4%) | NS | p = 0.001 (81.0%) | p < 0.001 (84.5%) | p = 0.002 (79.6%) | p = 0.000 (92.1%) | ||
| Depressive Symptoms | NS | p = 0.001 (95.8%) | p = 0.002 (83.9%) | NS | NS | p < 0.001 (88.4%) | NS | |
| Diabetes Knowledge | p = 0.000 (82.7%) | NS | NS | NS | NS | p < 0.001 (98.1%) | ||
| Complications | p < 0.001 (88.9%) | |||||||
| Female Gender | NS | |||||||
| Health Education | p < 0.001 (96.5%) | p < 0.001 (93.9%) | p = 0.002 (89.7%) | p < 0.001 (97.2%) | p = 0.030 (78.8%) | p < 0.001 (95.3%) | p < 0.001 (98.5%) | |
| Living Alone | NS | |||||||
| Admission History | p < 0.001 (95.1%) |
3.3.1. Coping Strategy
3.3.2. Health Beliefs
3.3.3. Locus of Control
3.3.4. Self-Efficacy
3.3.5. Social Support
3.3.6. Depressive Symptoms
3.3.7. Diabetes Knowledge
3.3.8. Complications
3.3.9. Female Gender
3.3.10. Health Education
3.3.11. Living Alone
3.3.12. Admission History
3.4. Factors not Eligible for Meta-Analysis
3.4.1. Age
3.4.2. Duration of Diabetes
3.4.3. Educational Level
3.4.4. Household income Level
3.4.5. Provider-Patient Communication
3.4.6. Health Insurance Coverage
3.4.7. CIRU
3.4.8. Marital Status
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlet. Available online: http://www.idf.org/diabetesatlas/introduction (accessed on 18 June 2014).
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J. Prevalence and control of diabetes in Chinese adults. J. Amer. Med. Assoc. 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- International Diabetes Federation. China Spends RMB 173.4 Billion (U.S.$25 Billion) a Year on Diabetes Treatment. Available online: http://www.idf.org/china-spends-rmb-1734-billion-us25-billion-year-diabetes-treatment (accessed on 21 August 2014).
- Centers for Disease Control and Prevention. Awareness of prediabetes—United States, 2005–2010. Morb. Mortal. Wkly. Rep. 2013, 62, 209–212. [Google Scholar]
- Anderson, R.M.; Funnell, M.M.; Butler, P.M.; Arnold, M.S.; Fitzgerald, J.T.; Feste, C.C. Patient empowerment. Results of a randomized controlled trial. Diabetes Care 1995, 18, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Anderson, R.M. In diabetes care, moving from compliance to adherence is not enough. Something entirely different is needed. Diabetes Care 1999, 22, 2090–2092. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Role of self-care in management of diabetes mellitus. J. Diabetes Metab. Disorder. 2013. [Google Scholar] [CrossRef] [PubMed]
- Haas, L.; Maryniuk, M.; Beck, J.; Cox, C.E.; Duker, P.; Edwards, L.; Fisher, E.B.; Hanson, L.; Kent, D.; Kolb, L.; et al. National standards for diabetes self-management education and support. Diabetes Care 2013, 36, S100–S108. [Google Scholar] [CrossRef] [PubMed]
- Norris, S.L.; Lau, J.; Smith, S.J.; Schmid, C.H.; Engelgau, M.M. Self-management education for adults with type 2 diabetes: A meta-analysis of the effect on glycemic control. Diabetes Care 2002, 25, 1159–1171. [Google Scholar] [CrossRef] [PubMed]
- Cochran, J.; Conn, V.S. Meta-analysis of quality of life outcomes following diabetes self-management training. Diabetes Educ. 2008, 34, 815–823. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Huang, X.; Yuan, C.; Cui, Y. The relationship between coping strategy and self-management behavior among patients with type 2 diabetes. J. Nurs. Train. 2012, 27, 1084–1086. (In Chinese) [Google Scholar]
- Sun, X.; Huang, X.; Yuan, C.; Cui, Y. The influence of health belief and coping style on self-management behavior in patients with type 2 diabetes mellitus. J. Nurs. 2012, 19, 8–11. (In Chinese) [Google Scholar]
- Guo, X.H.; Yuan, L.; Lou, Q.Q.; Shen, L.; Sun, Z.L.; Zhao, F.; Dai, X.; Huang, J.; Yang, H.Y. A nationwide survey of diabetes education, self-management and glycemic control in patients with type 2 diabetes in China. Chin. Med. J. 2012, 125, 4175–4180. [Google Scholar] [PubMed]
- Center for Review and Dissemination. CRD’s Guidance for Undertaking Reviews in Health Care, 2009. Available online: http://www.york.ac.uk/inst/crd/pdf/Systematic_Reviews.pdf (accessed on 2 July 2014).
- West, S.L.; King, V.; Carey, T.S.; Lohr, K.N.; McKoy, N.; Sutton, S.F.; Lux, L. Systems to Rate the Strength of Scientific Evidence; Evidence Report/Technology Assessment; U.S. Department of Health and Human Services: Washington, DC, USA, 2002; pp. 1–11.
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Commun. Health 1998, 52, 377–384. [Google Scholar] [CrossRef]
- Reisch, J.S.; Tyson, J.E.; Mize, S.G. Aid to the evaluation of therapeutic studies. Pediatrics 1989, 84, 815–827. [Google Scholar] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Internal Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Gao, J.; Wang, J.; Zhu, Y.; Yu, J. Validation of an information-motivation-behavioral skills model of self-care among Chinese adults with type 2 diabetes. BMC Public Health 2013. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Wang, J.; Zheng, P.; Haardörfer, R.; Kegler, M.C.; Zhu, Y.; Fu, H. Effects of self-care, self-efficacy, social support on glycemic control in adults with type 2 diabetes. BMC Fam. Pract. 2013. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Liao, L.; Sun, M.; He, G. Self-care practices of Chinese individuals with diabetes. Exp. Ther. Med. 2013, 5, 1137–1142. [Google Scholar] [PubMed]
- Xu, Y. Understanding the Factors Influencing Diabetes Self-Management in Chinese People with Type 2 Diabetes using Structural Equation Modeling. The Ph.D. Dissertation, University of Cincinnati, Cincinnati, OH, USA, 2005. [Google Scholar]
- Xu, Y.; Toobert, D.; Savage, C.; Pan, W.; Whitmer, K. Factors influencing diabetes self-management in Chinese people with type 2 diabetes. Res. Nurs. Health 2008, 31, 613–625. [Google Scholar] [CrossRef] [PubMed]
- Fang, S.; Yu, Z.; Tao, Y. The relationship between coping strategy, self-efficacy, and diabetes self-management among people living in rural areas. World Health Dig. Med. Period. 2013, 10, 79–80. (In Chinese) [Google Scholar]
- Wan, Q.; Wang, Q.; Shang, S. Correlation of self-management behavior and coping patterns of patients with type 2 diabetes. Nurs. J. Chin. People Lib. Army 2008, 25, 18–21. (In Chinese) [Google Scholar]
- Yu, P. The Relationship between Coping Strategy, Health Beliefs and Self-Management among People with Type 2 Diabetes in Changsha. The Master’s Thesis, Central South University, Changsha, China, 2009. [Google Scholar]
- Wan, Q.; Shaomei, S.; Yu, L. A study of factors of the self-care behaviors of the elderly with type 2 diabetes. Chin. General Pract. 2003, 6, 659–662. [Google Scholar]
- Huang, M.; Zhao, R.; Li, S.; Jiang, X. Self-management behavior in patients with type 2 diabetes: A cross-sectional survey in western urban China. PLoS ONE 2014. [Google Scholar] [CrossRef] [PubMed]
- Hua, L. The Social Ecological Model of Self-Management Activities in Type 2 Diabetes: A Structual Equation Modeling Analysis. The Mmaster’s Thesis, Zhejiang University, Hangzhou, China, 2010. [Google Scholar]
- Quan, J. The Research about the Current Status and Influencing Factors of Self-Management Behavior in Middle-Aged and over Patients Who with Type 2 Diabetes Mellitus; Yanbian University: Yanji, China, 2013. [Google Scholar]
- Jia, Y.; Gong, T.; Sang, M. Investigating on self-management and self-efficacy of patients with type 2 diabetes mellitus. Mod. Nurs. 2005, 11, 1586–1588. (In Chinese) [Google Scholar]
- Yang, J.; Wang, Q. Survey on self-care behavior and self-efficacy among type 2 diabetes patients in community. Chin. J. Pract. Nurs. 2008, 24, 7–10. (In Chinese) [Google Scholar]
- Gao, H. The relationship between diabetes self-efficacy and self-care behavior in patients with type 2 diabetes. Jilin Med. J. 2012, 33, 7646–7647. (In Chinese) [Google Scholar]
- Sun, J.; Zhang, X.; Yu, M.; Wang, L.; Yang, H.Y.; Zhu, L.; Huang, X.; Zou, B. Mediating effect analysis of self-efficacy between health literracy and self-management in patients with type 2 diabetes in the community. J. Nurs. Adm. 2012, 12, 778–780. (In Chinese) [Google Scholar]
- Kong, L.; Ye, Y.; Ding, F.; Tu, L. The relationship between diabetes knowledge, self-efficaicy, and self-management practice among individuals with type 2 diabetes in community. J. Hubei Univ. Sci. Technol. 2013, 27, 334–338. (In Chinese) [Google Scholar]
- Wang, J.Q.A.; Tak-Ying, S. Diabetes self-efficacy and self-care behaviour of Chinese patients living in Shanghai. J. Clin. Nurs. 2004, 13, 771–772. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Lin, T.; Liu, X. Study on correlation between social support and self-care behavior of type 2 diabetes mellitus patients. Chin. Nurs. Res. 2012, 388, 697–699. (In Chinese) [Google Scholar]
- Jia, Y.; Wang, J.; Teng, X. Study on the correlation between psychological health level and self-management in patients with type 2 diabetes mellitus. Shanghai Nurs. 2004, 4, 1–3. (In Chinese) [Google Scholar]
- Lin, T.; Lin, X.; Wan, L. A study on correlation between self-care behavior and psychological concordance and depression of type 2 diabetes mellitus patients. Chin. Nurs. Res. 2009, 23, 22–24. (In Chinese) [Google Scholar]
- Wang, Q.; Wan, Q.; Shang, S. Correlation of self-management behavior and depression in patients with type 2 diabetes. J. Nurs. Sci. 2009, 24, 14–15. (In Chinese) [Google Scholar]
- Huang, J.; Liu, Y.; Zhang, Y.; Yao, H. Correlation between self-management and knowledge of and attitude to diabetes in type 2 diabetic patients in Changsha. J. Central South Univ. 2013, 38, 176–181. (In Chinese) [Google Scholar]
- Hu, J.; Gruber, K.J.; Liu, H.; Zhao, H.; Garcia, A.A. Diabetes knowledge among older adults with diabetes in Beijing, China. J. Clin. Nurs. 2012, 22, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lv, W.; Ding, Y.; Zhu, M.; Gao, L.; Xu, Y. Study on correlation between self-management behaviors of elderly type 2 diabetic patients and diabetes knowledge level. Chin. Nurs. Res. 2013, 27, 2973–2974. (In Chinese) [Google Scholar]
- Wang, X.; Lan, W.; Liu, J.; Gao, L.; Wei, Q.; Zhang, J.; Chang, S.; Wei, X.; Yu, S. Evaluation analysis of influencing factors of type II diabetes patients self-management in Shanxi Province. J. Qiqihar Med. Coll. 2012, 33, 1065–1069. (In Chinese) [Google Scholar]
- Wang, X.; Zhang, J.F.; Li, Z.J.; Wang, F.Y.; Jiang, M.; Yang, J. An investigation of elf-management behavior with a sample of 2 diabetic patients living in the community. Chin. Nurs. Manag. 2012, 12, 52–56. (In Chinese) [Google Scholar]
- Wang, L.; Zhang, J. Self-management of elderly patients with type 2 diabetes and its influencing factors. J. Nurs. 2012, 19, 39–42. (In Chinese) [Google Scholar]
- Mu, Y. A Survey of Type 2 Diabetes Mellitus Prevalence and Self-Management in Aged in Gushan Town, Fuzhou. The Master’s Thesis, Fujian Medical University, Fuzhou, China, 2008. [Google Scholar]
- Wang, J.; Zhang, X. Survey of self-care behavior among 2 type diabetes patients. J. Nurs. Train. 2002, 17, 663–665. (In Chinese) [Google Scholar]
- Meng, F. Research on Health Education and Self-Managing Level of Community Non-Insulin Dependent Diabetic Patients. The Master’s Thesis, Sun Yat-Sen University, Guangzhou, China, 2010. [Google Scholar]
- Jia, Y.; Wang, J.; Liu, W. Study on self-care level of patients with type 2 diabetes mellitus and analysis of related factors. Nurs. J. Chin. People Lib. Army 2005, 22, 21–23. (In Chinese) [Google Scholar]
- Wang, J.S.; Wang, R.H.; Lin, C.C. Self-care behavior and related factors in outpatients newly diagnosed with non-insulin-dependent diabetes mellitus. J. Nurs. 1998, 45, 60–74. (In Chinese) [Google Scholar]
- Zhao, W. In investigation on self-management practice among empty nesters with type 2 diabetes. Shandong Med. J. 2007, 47, 135–136. (In Chinese) [Google Scholar]
- Ma, J.; Mo, G. Investigation of selfcontrol level and nursing needs in old empty nester patientswith diabetes mellitus. Nurs. Pract. Res. 2010, 7, 107–109. (In Chinese) [Google Scholar]
- Kong, Y.; Chen, Y. An investigation of self-management among hospitalized elderly wioth type 2 diabetes. Chin. J. Geriatr. Care 2009, 7, 91–92. (In Chinese) [Google Scholar]
- Lin, T.; Wang, J.; Qin, X. Study on self-care behaviors and its related factors in patients with type 2 diabetes. Chin. J. Mod. Nurs. 2008, 14, 1254–1256. (In Chinese) [Google Scholar]
- Zhu, F.; Yan, S.Z.; Li, R.; Zhang, H.Y. Self-management of the patients with type 2 diabetes mellitus in Zhongwei city of Ningxia. J. Ningxia Med. Univ. 2011, 33, 835–837. (In Chinese) [Google Scholar]
- Liang, Y.; Han, G.; Meng, Q. Self-care behavior and related factors in patients with type 2 diabetes. J. Qilu Nurs. 2009, 15, 28–30. (In Chinese) [Google Scholar]
- Xia, Z.; Yang, T. Diabetes self-management behaviors and related factors among patients with type 2 diabetes in Xiuying district, Haikou. Seek Med. Ask Med. 2011, 9, 526–527. (In Chinese) [Google Scholar]
- Yu, Z.; Yang, C.H.; Qiu, L.R.; Xie, X.H.; Cao, L.S. A study of self-management of 168 type 2 diabetic patients of Yi-people. Pract. J. Clin. Med. 2012, 9, 106–108. (In Chinese) [Google Scholar]
- Wang, Y.; Xiangyun, C.; Shulan, L.; Xiuyu, S.; Bei, Y. Relation between social resources uilization and self-management behavior in community-residing type 2 diabetes patients. J. Nurs. Sci. 2013, 28, 20–22. (In Chinese) [Google Scholar]
- Glasgow, R.E.; Strycker, L.A.; Toobert, D.J.; Eakin, E. A social-ecologic approach to assessing support for disease self-management: The chronic illness resources survey. J. Behav. Med. 2000, 23, 559–583. [Google Scholar] [CrossRef] [PubMed]
- Hochbaum, G.M. Public Participation in Medical Screening Programs: A Socio-Psychological study; Government Printing Office: Washington, DC, USA, 1958.
- Janz, N.K.; Becker, M.H. The health belief model: A decade later. Health Educ. Q. 1984, 11, 1–47. [Google Scholar] [CrossRef] [PubMed]
- Hayes, R.P.; Bernard, A.M.; Slocum, W.; Imad, E.K.; Ziemer, D.; Gallina, D.; Phillips, L.S. Diabetes in urban African Americans: Assessment of diabetes-specific locus of control in patients with type 2 diabetes. Diabetes Educ. 2000, 26, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Macrodimitris, S.D.; Endler, N.S. Coping, control, and adjustment in type 2 diabetes. Health Psychol. 2001, 20, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Rodin, J. Aging and health: Effects of the sense of control. Science 1986, 233, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Liu, T. A concept analysis of self-efficacy among Chinese elderly with diabetes mellitus. Nurs. Forum 2012, 47, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Wan, Q.; Li, F. Study of the correlation between self-care activities of patients with diabetes and participation activities of thier relatives. J. Nurs. Adm. 2010, 10, 159–161. (In Chinese) [Google Scholar]
- Zeng, B.; Sun, W.; Gary, R.A.; Li, C.; Liu, T. Towards a conceptual model of diabetes self-management among Chinese immigrants in the United States. Int. J. Environ. Res. Public Health 2014, 11, 6727–6742. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Richardson, C.R.; Avripas, S.A.; Neal, D.L.; Marcus, S.M. Increasing lifestyle physical activity in patients with depression or other serious mental illness. J. Psychiatr. Pract. 2005, 11, 379–388. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y. Study on Compliance and Influence Factors of the Re-Hospitalized Patients with Diabetes Mellitus. The Master’s Thesis, Central South Universtiy, Changsha, China, 2007. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, X.; Liu, T.; Yuan, X.; Ge, S.; Yang, J.; Li, C.; Sun, W. Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 11304-11327. https://doi.org/10.3390/ijerph120911304
Luo X, Liu T, Yuan X, Ge S, Yang J, Li C, Sun W. Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2015; 12(9):11304-11327. https://doi.org/10.3390/ijerph120911304
Chicago/Turabian StyleLuo, Xiaoping, Tingting Liu, Xiaojing Yuan, Song Ge, Jing Yang, Changwei Li, and Wenjie Sun. 2015. "Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 12, no. 9: 11304-11327. https://doi.org/10.3390/ijerph120911304
APA StyleLuo, X., Liu, T., Yuan, X., Ge, S., Yang, J., Li, C., & Sun, W. (2015). Factors Influencing Self-Management in Chinese Adults with Type 2 Diabetes: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 12(9), 11304-11327. https://doi.org/10.3390/ijerph120911304