
Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors among a Health Examination Population in Wuhu (China)



Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Data Collection Procedure
2.3. Study Definitions
2.4. Data Analysis
3. Results
3.1. Prevalence of DM and IFG in Different Sexes
3.2. Characteristics of IFG and DM
3.3. Risk Factors of Hyperglycaemia
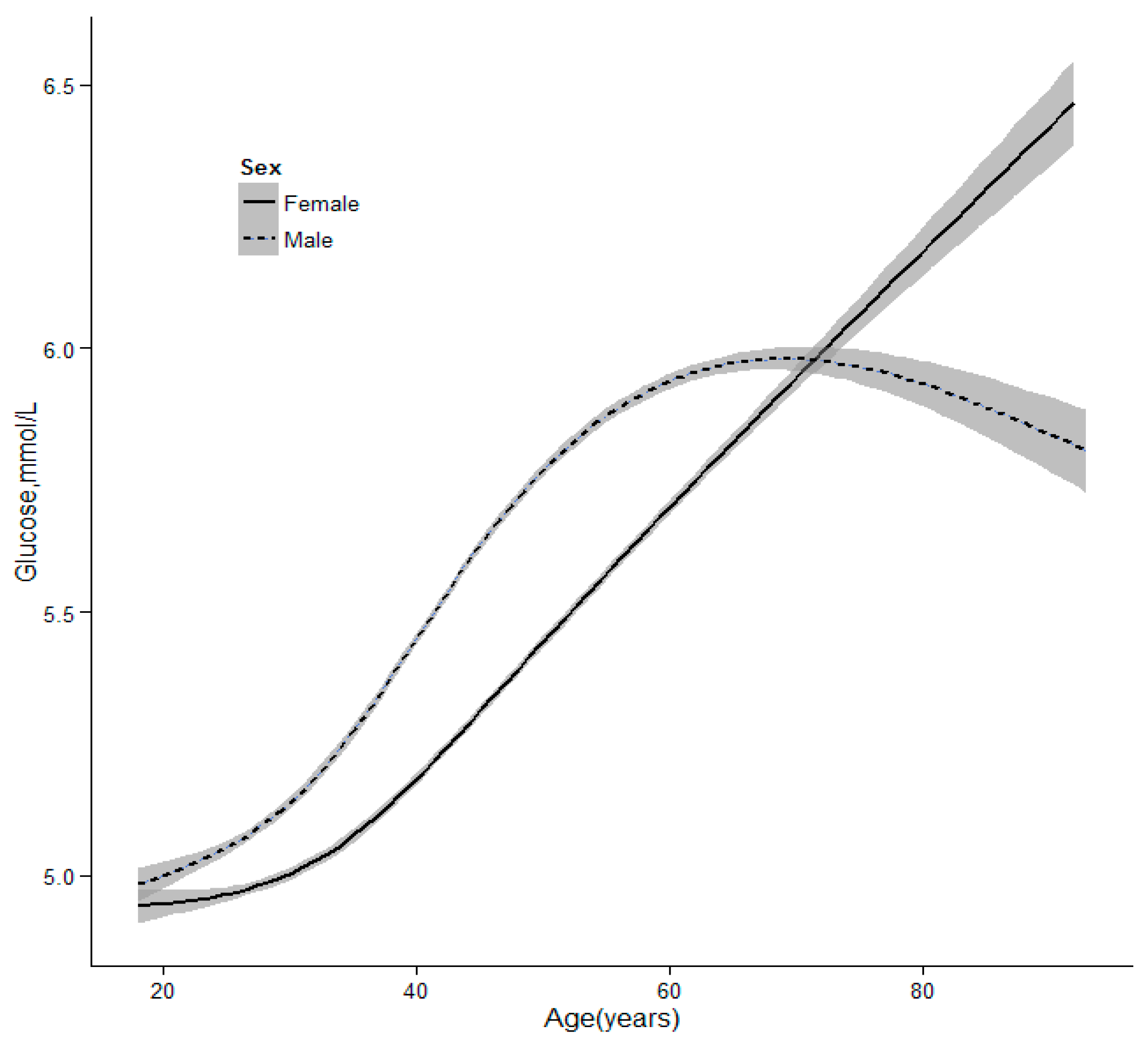
3.4. The Trends of Glucose as Age
4. Discussion
5. Limitations
6. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| DM | diabetes mellitus |
| FPG | impaired glucose tolerance |
| HDL | high density lipoprotein |
| LDL | low density lipoprotein |
| TG | triglyceride |
| TC | total cholesterol |
| OGTT | oral glucose tolerance test |
References
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in Chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Davis-Ajami, M.L.; Wu, J.; Fink, J.C. Differences in health services utilization and costs between antihypertensive medication users versus nonusers in adults with diabetes and concomitant hypertension from Medical Expenditure Panel Survey pooled years 2006 to 2009. Value Health 2014, 17, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.R.; Guariguata, L.; Weil, C.; Shaw, J. IDF diabetes atlas: Global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes Res. Clin. Pract. 2011, 94, 311–321. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.; Lu, J.; Weng, J.; Jia, W.; Ji, L.; Xiao, J.; Shan, Z.; Liu, J.; Tian, H.; Ji, Q.; et al. Prevalence of diabetes among men and women in China. N. Engl. J. Med. 2010, 362, 1090–1101. [Google Scholar] [CrossRef] [PubMed]
- Boyko, E.J. World Diabetes Congress Vancouver 2015: Public health and epidemiology stream. Diabetes Res. Clin. Pract. 2015, 109, 450. [Google Scholar] [CrossRef] [PubMed]
- Maruthur, N.M.; Ma, Y.; Delahanty, L.M.; Nelson, J.A.; Aroda, V.; White, N.H.; Marrero, D.; Brancati, F.L.; Clark, J.M. Diabetes Prevention Program Research Group. Early response to preventive strategies in the diabetes prevention program. J. Gen. Intern. Med. 2013, 28, 1629–1636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perreault, L.; Pan, Q.; Mather, K.J.; Watson, K.E.; Hamman, R.F.; Kahn, S.E. Diabetes Prevention Program Research Group. Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: Results from the Diabetes Prevention Program Outcomes Study. Lancet 2012, 379, 2243–2251. [Google Scholar] [CrossRef]
- Lin, A.; Zhang, G.; Liu, Z.; Gu, J.; Chen, W.; Luo, F. Community-based lifestyle intervention for reducing blood pressure and glucose among middle-aged and older adults in China: A Pilot Study. Int. J. Environ. Res. Public Health 2014, 11, 11645–11663. [Google Scholar] [CrossRef] [PubMed]
- Qi, L.; Feng, L.; Tang, W.; Ma, X.; Ding, X.; Mao, D.; Li, J.; Wang, Y.; Xiong, H. A community-based comprehensive intervention program for 7200 patients with type 2 diabetes mellitus in Chongqing (China). Int. J. Environ. Res. Public Health 2014, 11, 11450–11463. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Definition, Diagnosis and Classification of Diabetes Mellitus and Its Complications, Part 1: Diagnosis and Classification of Diabetes Mellitus; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Liu, L.S. 2010 Chinese guidelines for the management of hypertension. Chin. J. Epidemiol. 2011, 39, 579–615. [Google Scholar]
- Rathmann, W.; Giani, G. Global prevalence of diabetes: Estimates for the year 2000 and projections for 2030. Diabetes Care 2004, 27, 2568–2569. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.Y.; Li, L.; Dai, F.; Li, X.J.; Xu, X.X.; Fan, J.G. Prevalence of and risk factors for type 2 diabetes mellitus in hyperlipidemia in China. Med. Sci. Monit. 2015, 21, 2476–2484. [Google Scholar] [PubMed]
- Li, S.; Guo, S.; He, F.; Zhang, M.; He, J.; Yan, Y.; Ding, Y.; Zhang, J.; Liu, J.; Guo, H.; Xu, S.; Ma, R. Prevalence of diabetes mellitus and impaired fasting glucose, associated with risk factors in rural Kazakh adults in Xinjiang, China. Int. J. Environ. Res. Public Health 2015, 12, 554–565. [Google Scholar] [CrossRef] [PubMed]
- Yin, Y.; Han, W.; Wang, Y.; Zhang, Y.; Wu, S.; Zhang, H.; Jiang, L.; Wang, R.; Zhang, P.; Yu, Y.; et al. Identification of risk factors affecting impaired fasting glucose and diabetes in adult patients from northeast China. Int. J. Environ. Res. Public Health 2015, 12, 12662–12678. [Google Scholar] [CrossRef] [PubMed]
- Jimenez Mejias, E.; Olvera Porcel, M.C.; Amezcua Prieto, C.; Olmedo-Requena, R.; Martinez Ruiz, V.; Jimenez Moleon, J.J. Effect of age on the prevalence of diabetes mellitus in Spain between 2001 and 2012. Nutr. Hosp. 2014, 29, 1335–1338. [Google Scholar] [PubMed]
- Yu, S.; Sun, Z.; Zheng, L.; Guo, X.; Yang, H.; Sun, Y. Prevalence of diabetes and impaired fasting glucose in hypertensive adults in rural China: Far from leveling-off. Int. J. Environ. Res. Public Health 2015, 12, 14764–14779. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Cui, X.; Li, F.; Wang, S.; Liu, X.; Hui, L.; Song, N.; Li, N. Association between diabetes mellitus with metabolic syndrome and diabetic microangiopathy. Exp. Ther. Med. 2014, 8, 1867–1873. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, A.; Sardarinia, M.; Khalili, D.; Momenan, A.A.; Azizi, F.; Hadaegh, F. Sex specific incidence rates of type 2 diabetes and its risk factors over 9 years of follow-up: Tehran Lipid and Glucose Study. PLoS ONE 2014, 9, e102563. [Google Scholar] [CrossRef] [PubMed]
- Wandell, P.E.; Carlsson, A.C. Gender differences and time trends in incidence and prevalence of type 2 diabetes in Sweden—A model explaining the diabetes epidemic worldwide today? Diabetes Res. Clin. Pract. 2014, 106, e90–e92. [Google Scholar] [CrossRef] [PubMed]
- Krag, M.O.; Hasselbalch, L.; Siersma, V.; Nielsen, A.B.; Reventlow, S.; Malterud, K.; de Fine Olivarius, N. The impact of gender on the long-term morbidity and mortality of patients with type 2 diabetes receiving structured personal care: A 13 year follow-up study. Diabetologia 2016, 59, 275–285. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhang, R.Y.; Chen, R.P.; Chen, L.S.; Lin, S.D.; Liang, G.X.; Hu, B.C.; Zhu, Z.Z.; Wang, Y.L.; Yan, L.; et al. Prevalence and risk factors for dyslipidemia in diabetics with overweight or obesity. Chin. J. Epidemiol. 2013, 93, 2851–2856. [Google Scholar]
- Esser, N.; Legrand-Poels, S.; Piette, J.; Scheen, A.J.; Paquot, N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabetes Res. Clin. Pract. 2014, 105, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Arnaud, J.; de Lorgeril, M.; Akbaraly, T.; Salen, P.; Arnout, J.; Cappuccio, F.P.; van Dongen, M.C.; Donati, M.B.; Krogh, V.; Siani, A.; et al. Gender differences in copper, zinc and selenium status in diabetic-free metabolic syndrome European population—The IMMIDIET study. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 517–524. [Google Scholar] [CrossRef] [PubMed]
- Morita, A.; Ishigaki, Y. Gender-difference in diabetes mellitus. Nihon Rinsho 2015, 73, 606–610. [Google Scholar] [PubMed]
- Ring, M.; Eriksson, M.J.; Fritz, T.; Nyberg, G.; Ostenson, C.G.; Krook, A.; Zierath, J.R.; Caidahl, K. Influence of physical activity and gender on arterial function in type 2 diabetes, normal and impaired glucose tolerance. Diabetes Vasc. Dis. Res. 2015, 12, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Lipscombe, C.; Smith, K.J.; Gariepy, G.; Schmitz, N. Gender differences in the association between lifestyle behaviors and diabetes distress in a community sample of adults with type 2 diabetes. J. Diabetes 2015. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total (n = 175,122) | Females (n = 72,861) | Male (n = 102,261) | t/χ2 | p |
|---|---|---|---|---|---|
| Age | 40.1 ± 13.9 | 40.4 ± 13.6 | 42.8 ± 13.0 | 7.8 | <0.001 |
| Alcohol | 49,495.9 | <0.001 | |||
| No | 97,297 (63.8) | 58,747 (97.7) | 38,550 (41.8) | ||
| Small | 28,188 (18.5) | 597 (1.0) | 27,591 (29.9) | ||
| Occasionally | 7231 (4.7) | 619 (1.0) | 6612 (7.2) | ||
| Frequently | 19,740 (12.9) | 167 (0.3) | 19,573 (21.2) | ||
| Smoking | 42,879.1 | <0.001 | |||
| No | 105,542 (69.2) | 59,864 (99.6) | 45,678 (49.5) | ||
| Small | 7401 (4.9) | 63 (0.1) | 7338 (7.9) | ||
| Occasionally | 2683 (1.8) | 27 (0.0) | 2656 (2.9) | ||
| Frequently | 36,829 (24.2) | 175 (0.3) | 36,654 (39.7) | ||
| Glucose * | 922.7 | <0.001 | |||
| Normal | 141,509 (80.8) | 58,089 (92.1) | 83,420 (87.3) | ||
| IFG | 10,487 (6.0) | 3193 (5.1) | 7294 (7.6) | ||
| DM | 6580 (3.8) | 1779 (2.8) | 4801 (5.1) |
| Variable | Normal (n = 141,509) | IFG (n = 10,487) | DM (n = 6580) | F/χ2 | p |
|---|---|---|---|---|---|
| Age (years) | 39.52 ± 13.37 | 50.47 ± 12.99 | 53.75 ± 12.00 | 6552.0 | <0.001 |
| BMI (kg/m2) | 23.36 ± 3.38 | 25.18 ± 3.30 | 25.66 ± 3.29 | 2518.2 | <0.001 |
| Glu (mmol/L) | 5.12 ± 0.45 | 6.42 ± 0.24 | 9.26 ± 2.72 | 122,183.0 | <0.001 |
| HDL (mmol/L) | 1.33 ± 0.36 | 1.30± 0.36 | 1.25 ± 0.34 | 172.7 | <0.001 |
| TC (mmol/L) | 4.60 ± 0.86 | 4.95 ± 0.91 | 5.04 ± 1.03 | 1367 | <0.001 |
| TG (mmol/L) | 1.47 ± 1.16 | 1.94 ± 1.64 | 2.38 ± 2.40 | 2016 | <0.001 |
| BP | 7375.1 | <0.001 | |||
| Normal | 58,046 (95.5) | 1803 (3.0) | 935 (1.5) | ||
| Pre-HTN | 57,948 (88.8) | 4605 (7.1) | 2714 (4.2) | ||
| Stage I | 14,327 (77.6) | 2427 (13.1) | 1711 (9.3) | ||
| Stage II | 4972 (73.7) | 1002 (14.9) | 769 (11.4) | ||
| Stage III | 919 (70.7) | 225 (17.3) | 156 (12.0) | ||
| Alcohol | 997.9 | <0.001 | |||
| No | 85,911 (90.6) | 5478 (5.8) | 3448 (3.6) | ||
| Small | 24,214 (87.5) | 2156 (7.8) | 1301 (4.7) | ||
| Occasionally | 6497 (92.6) | 343 (4.9) | 173 (2.5) | ||
| Frequently | 16,172 (83.6) | 1913 (9.9) | 1261 (6.5) | ||
| Smoking | 309.0 | <0.001 | |||
| No | 92,490 (89.8) | 6633 (6.4) | 3857 (3.7) | ||
| Small | 6479 (89.4) | 506 (7.0) | 264 (3.6) | ||
| Occasionally | 2408 (93.1) | 117 (4.5) | 61 (2.4) | ||
| Frequently | 31,419 (87.2) | 2632 (7.3) | 2000 (5.5) |
| Variable | β | SE | Beta | OR | 95% CI | p |
|---|---|---|---|---|---|---|
| Age (years) | 0.06 | 0.00 | 4.72 | 1.07 | 1.06–1.07 | <0.001 |
| BMI (kg/m2) | 0.08 | 0.01 | 1.44 | 1.08 | 1.07–1.10 | <0.001 |
| TG (mmol/L) | 0.18 | 0.02 | 0.93 | 1.19 | 1.15–1.24 | <0.001 |
| TC (mmol/L) | 0.16 | 0.03 | 0.84 | 1.17 | 1.1–1.25 | <0.001 |
| HDL (mmol/L) | −0.61 | 0.09 | −1.28 | 0.54 | 0.45–0.65 | <0.001 |
| BP | ||||||
| Normal | 0 | - | 1 | - | ||
| Pre-HTN | 0.50 | 0.07 | 1.65 | 1.43–1.91 | <0.001 | |
| Stage I | 0.80 | 0.09 | 2.23 | 1.89–2.64 | <0.001 | |
| Stage II | 0.92 | 0.11 | 2.51 | 2.01–3.13 | <0.001 | |
| Stage III | 1.15 | 0.23 | 3.17 | 2.02–4.97 | <0.001 |
| Variable | β | SE | Beta | OR | 95% CI | p |
|---|---|---|---|---|---|---|
| Age (years) | 0.06 | 0.00 | 3.16 | 1.06 | 1.06–1.06 | <0.001 |
| BMI (kg/m2) | 0.09 | 0.01 | 1.22 | 1.09 | 1.08–1.10 | <0.001 |
| TG (mmol/L) | 0.13 | 0.01 | 0.85 | 1.14 | 1.12–1.16 | <0.001 |
| TC (mmol/L) | 0.23 | 0.02 | 0.86 | 1.26 | 1.21–1.31 | <0.001 |
| HDL (mmol/L) | −0.50 | 0.06 | -0.67 | 0.61 | 0.54–0.69 | <0.001 |
| BP | ||||||
| Normal | 0 | - | 1 | - | ||
| Pre-HTN | 0.29 | 0.05 | 1.33 | 1.21–1.47 | <0.001 | |
| Stage I | 0.56 | 0.06 | 1.76 | 1.58–1.96 | <0.001 | |
| Stage II | 0.71 | 0.07 | 2.03 | 1.79–2.31 | <0.001 | |
| Stage III | 0.65 | 0.11 | 1.92 | 1.55–2.40 | <0.001 | |
| Smoking | ||||||
| No | 0 | - | 1 | - | ||
| Small/Occasionally | −0.11 | 0.07 | 0.89 | 0.78–1.02 | 0.085 | |
| Frequently | 0.14 | 0.04 | 1.15 | 1.07–1.24 | <0.001 | |
| Alcohol | ||||||
| No | 0 | - | 1 | - | ||
| Small/Occasionally | −0.01 | 0.04 | 0.99 | 0.91–1.07 | 0.725 | |
| Frequently | 0.16 | 0.04 | 1.17 | 1.07–1.28 | 0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, J.; Zha, X.; Li, H.; Guo, R.; Zhu, Y.; Wen, Y. Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors among a Health Examination Population in Wuhu (China). Int. J. Environ. Res. Public Health 2016, 13, 392. https://doi.org/10.3390/ijerph13040392
Song J, Zha X, Li H, Guo R, Zhu Y, Wen Y. Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors among a Health Examination Population in Wuhu (China). International Journal of Environmental Research and Public Health. 2016; 13(4):392. https://doi.org/10.3390/ijerph13040392
Chicago/Turabian StyleSong, Jiangen, Xiaojuan Zha, Haibo Li, Rui Guo, Yu Zhu, and Yufeng Wen. 2016. "Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors among a Health Examination Population in Wuhu (China)" International Journal of Environmental Research and Public Health 13, no. 4: 392. https://doi.org/10.3390/ijerph13040392
APA StyleSong, J., Zha, X., Li, H., Guo, R., Zhu, Y., & Wen, Y. (2016). Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors among a Health Examination Population in Wuhu (China). International Journal of Environmental Research and Public Health, 13(4), 392. https://doi.org/10.3390/ijerph13040392