Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
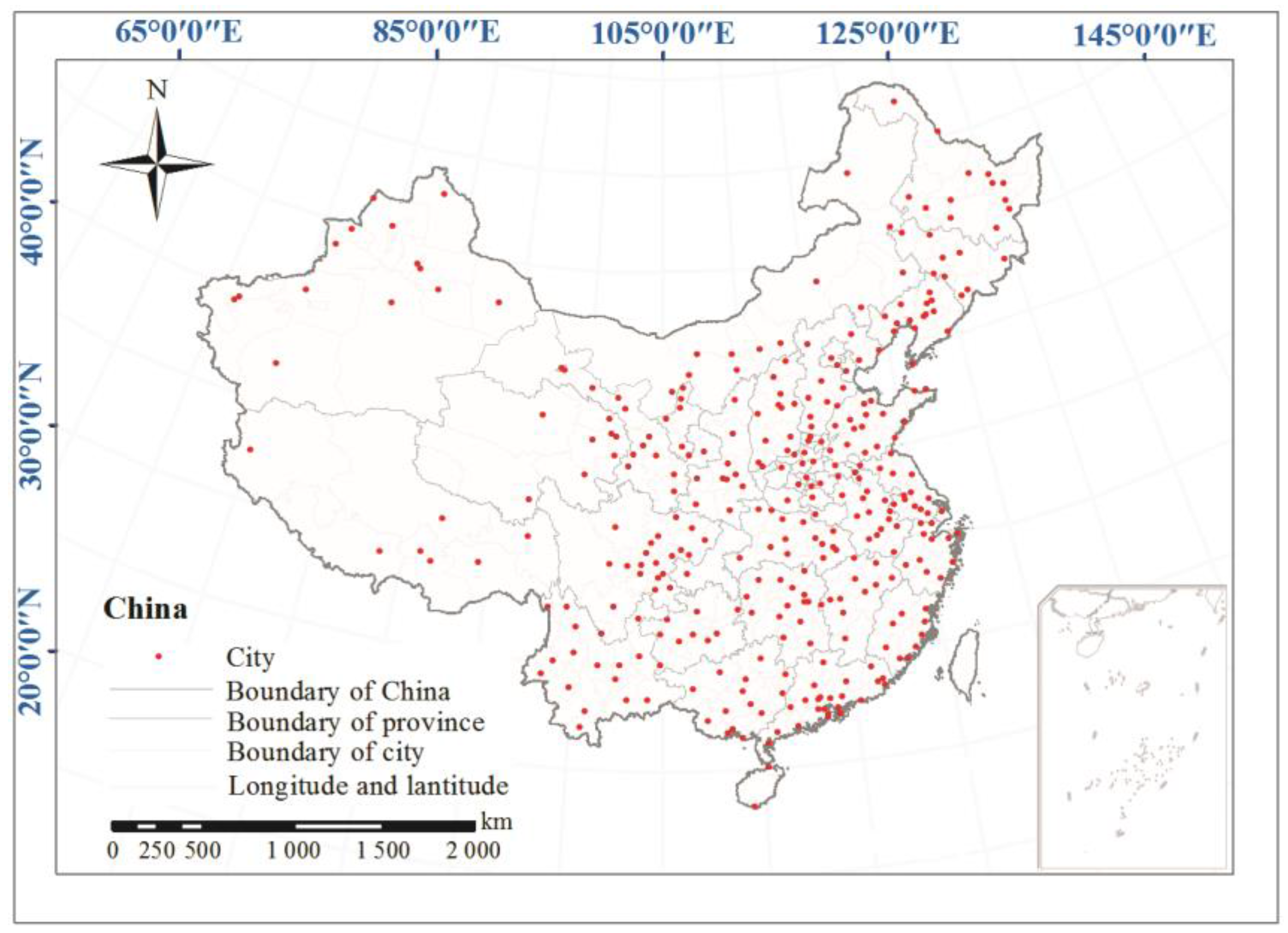
2.1.1. Ground Monitoring PM2.5 Data
2.1.2. Population and Mortality Data
2.2. Methods
2.2.1. Kriging Model
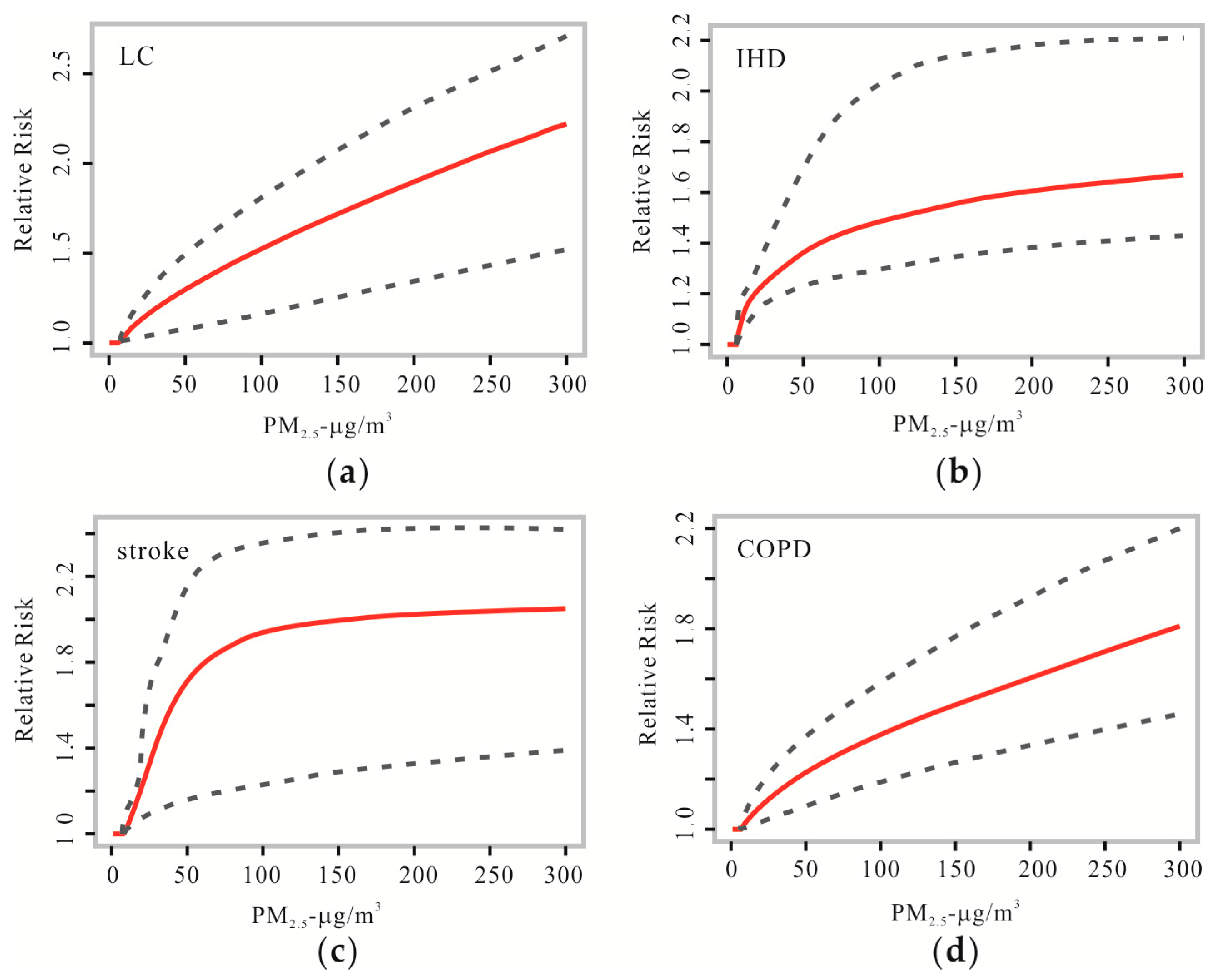
2.2.2. Integrated Exposure–Response (IER) Model
2.2.3. Estimates of Health Impacts and Mortality Due to Exposure to PM2.5
3. Results and Discussion
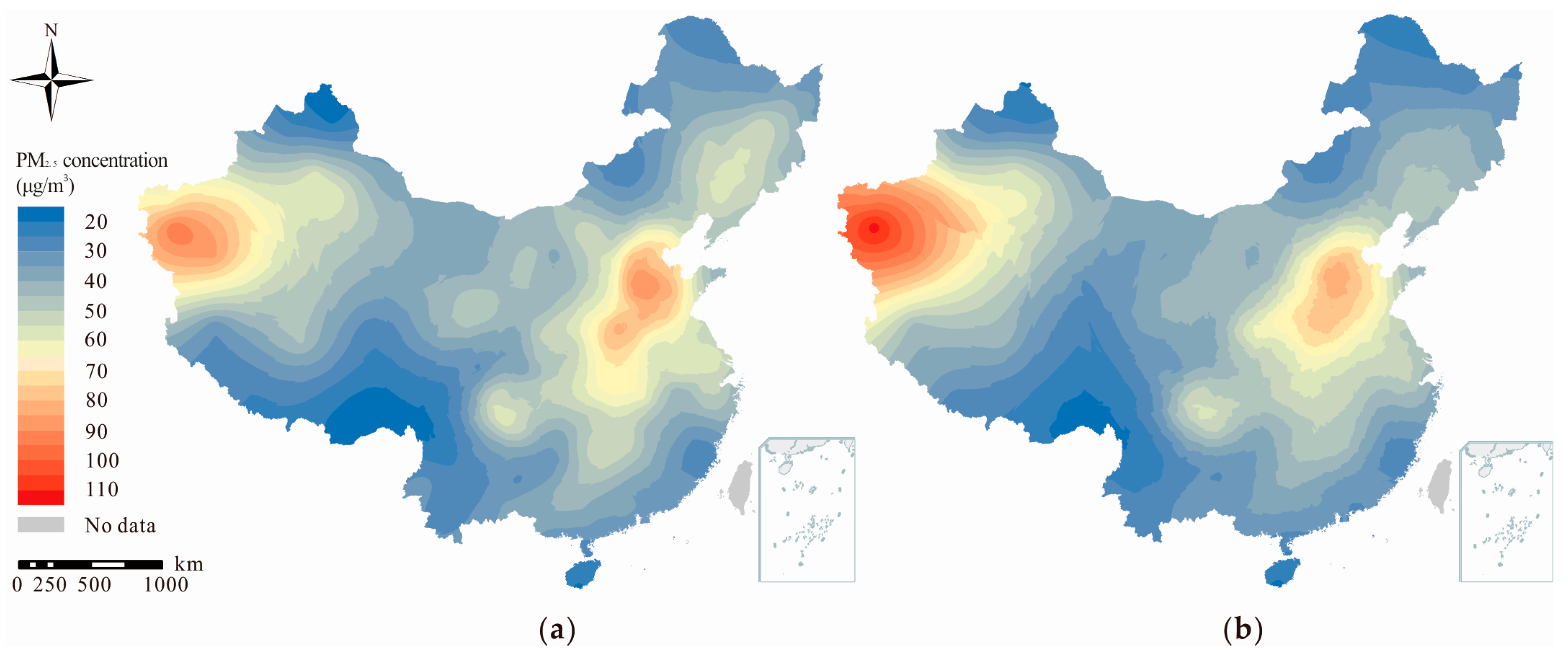
3.1. Spatial Distribution of PM2.5
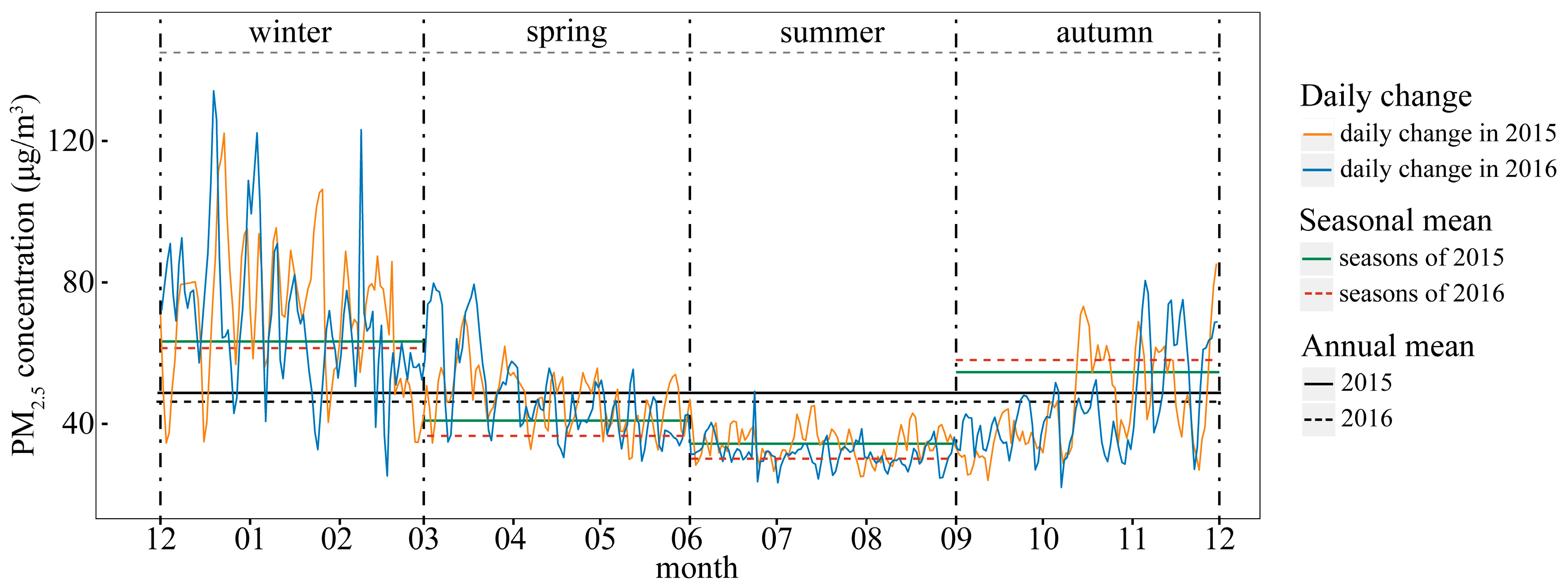
3.2. Temporal Trends of PM2.5
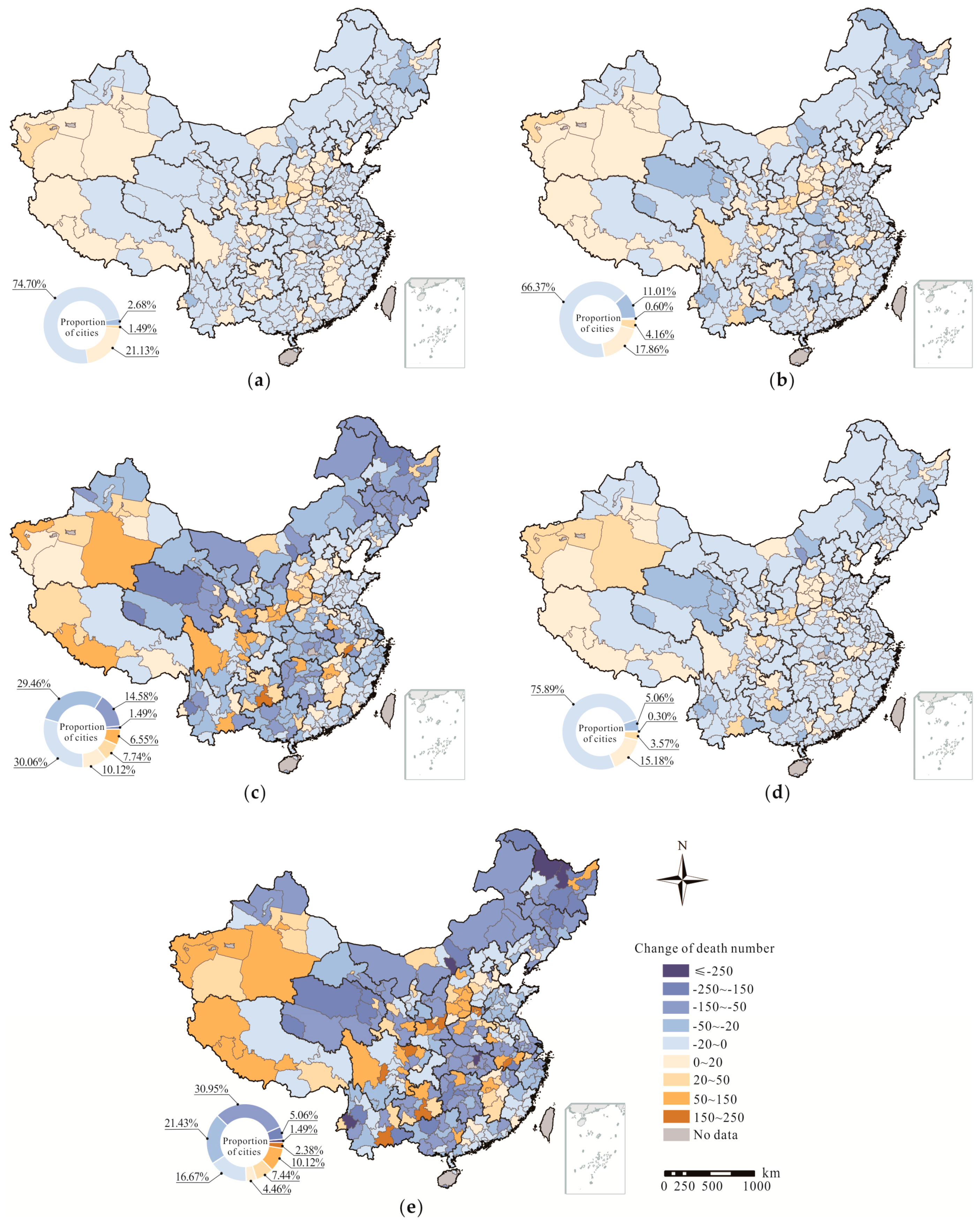
3.3. Disease Burden of PM2.5
3.4. Strengths and Limitations
4. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Forouzanfar, M.H.; Afshin, A.; Alexander, L.T.; Anderson, H.R.; Bhutta, Z.A.; Biryukov, S.; Brauer, M.; Burnett, R.; Cercy, K.; Charlson, F.J.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Pope, C.A.; Burnett, R.T.; Thun, M.J.; Calle, E.E.; Krewski, D.; Ito, K.; Thurston, G.D. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA J. Am. Med. Assoc. 2002, 287, 1132–1141. [Google Scholar] [CrossRef]
- Haley, V.B.; Talbot, T.O.; Felton, H.D. Surveillance of the short-term impact of fine particle air pollution on cardiovascular disease hospitalizations in new york state. Environ. Health 2009, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Burnett, R.T.; Kwong, J.C.; Villeneuve, P.J.; Goldberg, M.S.; Brook, R.D.; van Donkelaar, A.; Jerrett, M.; Martin, R.V.; Kopp, A.; et al. Spatial association between ambient fine particulate matter and incident hypertension. Circulation 2014, 129, 562–569. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, A.M.C.D.; Mattos, I.E.; Freitas, S.R.; Longo, K.M.; Hacon, S.S. Particulate matter (PM2.5) of biomass burning emissions and respiratory diseases in the south of the Brazilian Amazon. Rev. Bras. Epidemiol. 2010, 13, 337–351. [Google Scholar]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA J. Am. Med. Assoc. 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Stieb, D.M.; Chen, L.; Beckerman, B.S.; Jerrett, M.; Crouse, D.L.; Omariba, D.W.R.; Peters, P.A.; van Donkelaar, A.; Martin, R.V.; Burnett, R.T.; et al. Associations of pregnancy outcomes and PM2.5 in a national Canadian study. Environ. Health Perspect. 2016, 124, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, S. Environmental regulations on air pollution in China and their impact on infant mortality. J. Health Econ. 2015, 42, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Mundial, B. World Development Report 2007; World Bank: Washington, DC, USA, 2006. [Google Scholar]
- National Bureau of Statistics of the People’s Republic of China. Available online: http://www.stats.gov.cn/ (accessed on 10 January 2017).
- Wang, Z.; Pan, L.; Li, Y.; Zhang, D.; Ma, J.; Sun, F.; Xu, W.; Wang, X. Assessment of air quality benefits from the national pollution control policy of thermal power plants in China: A numerical simulation. Atmos. Environ. 2015, 106, 288–304. [Google Scholar] [CrossRef]
- Xue, B.; Mitchell, B.; Geng, Y.; Ren, W.; Müller, K.; Ma, Z.; Oliveira, J.A.P.D.; Fujita, T.; Tobias, M. A review on China’s pollutant emissions reduction assessment. Ecol. Ind. 2014, 38, 272–278. [Google Scholar] [CrossRef]
- Chen, Y.; Schleicher, N.; Fricker, M.; Cen, K.; Liu, X.L.; Kaminski, U.; Yu, Y.; Wu, X.F.; Norra, S. Long-term variation of black carbon and PM2.5 in Beijing, China with respect to meteorological conditions and governmental measures. Environ. Pollut. 2016, 212, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Liu, S.; Castro, R.; Pan, X. PM2.5 monitoring and mitigation in the cities of China. Environ. Sci. Technol. 2012, 46, 3627. [Google Scholar] [CrossRef] [PubMed]
- Zhang, A.; Qi, Q.; Jiang, L.; Zhou, F.; Wang, J. Population exposure to PM2.5 in the urban area of Beijing. PLoS ONE 2013, 8, e63486. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.L.; Qiao, L.P.; Lou, S.R.; Zhou, M.; Ding, A.J.; Huang, H.Y.; Chen, J.M.; Wang, Q.; Tao, S.; Chen, C.H.; et al. Chemical composition of PM2.5 and meteorological impact among three years in urban Shanghai, China. J. Clean. Prod. 2016, 112, 1302–1311. [Google Scholar] [CrossRef]
- Ding, Y.; Liu, Y. Analysis of long-term variations of fog and haze in China in recent 50 years and their relations with atmospheric humidity. Sci. China Earth Sci. 2014, 57, 36–46. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Y.; Ying, Q.; Zhang, H. Spatial and temporal variability of PM2.5 and PM10 over the North China Plain and the Yangtze River Delta, China. Atmos. Environ. 2014, 95, 598–609. [Google Scholar] [CrossRef]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environ. Int. 2007, 33, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Peng, X.; Huang, W.; Chen, R.; Xu, Z.; Chen, B.; Kan, H. A time-stratified case-crossover study of fine particulate matter air pollution and mortality in Guangzhou, China. Int. Arch. Occup. Environ. Health 2012, 85, 579–585. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Xu, H.; Xu, Q.; Chen, B.; Kan, H. Fine particulate matter constituents and cardiopulmonary mortality in a heavily polluted Chinese city. Environ. Health Perspect. 2012, 120, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Chen, R.; Pan, G.; Xu, X.; Song, W.; Chen, B.; Kan, H. Fine particulate air pollution and daily mortality in Shenyang, China. Sci. Total Environ. 2011, 409, 2473–2477. [Google Scholar] [CrossRef] [PubMed]
- Ezzati, M.; Lopez, A.D.; Rodgers, A.; Murray, C.J.L. Comparative quantification of health risks. Can. Nurse 2005, 1, 1. [Google Scholar]
- Ministry of Environmental Protection of the People’s Republic of China. Available online: http://kjs.mep.gov.cn/hjbhbz/bzwb/jcffbz/201109/t20110914_217272.shtml (accessed on 2 August 2017).
- China National Environmental Monitoring Center. Available online: http://www.cnemc.cn/ (accessed on 10 January 2017).
- He, J.; Gong, S.; Yu, Y.; Yu, L.; Wu, L.; Mao, H.; Song, C.; Zhao, S.; Liu, H.; Li, X.; et al. Air pollution characteristics and their relation to meteorological conditions during 2014–2015 in major Chinese cities. Environ. Pollut. 2017, 223, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-T. Introduction to Geographic Information Systems; McGraw-Hill: New York, NY, USA, 2006; pp. 429–444. [Google Scholar]
- Furrer, R.; Genton, M.G.; Nychka, D. Covariance tapering for interpolation of large spatial datasets. J. Comput. Graph. Stat. 2006, 15, 502–523. [Google Scholar] [CrossRef]
- Guo, M.; Wang, X.F.; Li, J.; Yi, K.P.; Zhong, G.S.; Wang, H.M.; Tani, H. Spatial distribution of greenhouse gas concentrations in arid and semi-arid regions: A case study in East Asia. J. Arid Environ. 2013, 91, 119–128. [Google Scholar] [CrossRef]
- Schneider, K.; Huisman, J.A.; Breuer, L.; Frede, H.G. Ambiguous effects of grazing intensity on surface soil moisture: A geostatistical case study from a steppe environment in Inner Mongolia, PR China. J. Arid Environ. 2008, 72, 1305–1319. [Google Scholar] [CrossRef]
- Yin, S.; Wang, X.; Xiao, Y.; Tani, H.; Zhong, G.; Sun, Z. Study on spatial distribution of crop residue burning and PM2.5 change in China. Environ. Pollut. 2017, 220, 204. [Google Scholar] [CrossRef] [PubMed]
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; Turner, M.C.; Rd, P.C.; Thurston, G.; Calle, E.E. Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality. Res. Rep. 2009, 140, 5. [Google Scholar]
- Burnett, R.T.; Pope, C.A., III; Ezzati, M.; Olives, C.; Lim, S.S.; Mehta, S.; Shin, H.H.; Singh, G.; Hubbell, B.; Brauer, M.; et al. An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environ. Health Perspect. 2014, 122, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Wang, Z.; Zhang, W. Exploring spatiotemporal patterns of PM2.5 in China based on ground-level observations for 190 cities. Environ. Pollut. 2016, 216, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Shi, M.; Gao, S.; Li, S.; Mao, J.; Zhang, H.; Sun, Y.; Bai, Z.; Wang, Z. Assessment of population exposure to PM2.5 for mortality in China and its public health benefit based on benmap. Environ. Pollut. 2017, 221, 311–317. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.; Wang, Q.-G.; Li, H.; Yu, Y.; Lu, Y.; Qian, X. Mortality effects assessment of ambient PM2.5 pollution in the 74 leading cities of China. Sci. Total Environ. 2016, 569, 1545–1552. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Xie, X.; Cai, J.; Chen, D.; Gao, B.; He, B.; Cheng, N.; Xu, B. Understanding meteorological influences on PM2.5 concentrations across China: A temporal and spatial perspective. Atmos. Chem. Phys. 2017, 1–30. [Google Scholar] [CrossRef]
- Peng, J.; Chen, S.; Lu, H.; Liu, Y.; Wu, J. Spatiotemporal patterns of remotely sensed PM2.5 concentration in China from 1999 to 2011. Remote Sens. Environ. 2016, 174, 109–121. [Google Scholar] [CrossRef]
- Han, L.; Zhou, W.; Li, W. City as a major source area of fine particulate (PM2.5) in China. Environ. Pollut. 2015, 206, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Cheng, T.; Gu, X.; Wang, Y.; Chen, H.; Bao, F.; Shi, S.; Xu, B.; Wang, W.; Zuo, X.; et al. Assessment of PM2.5 concentrations and exposure throughout China using ground observations. Sci. Total Environ. 2017, 601, 1024. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Wu, L.; Xie, Y.; He, J.; Chen, X.; Wang, T.; Lin, Y.; Jin, T.; Wang, A.; Liu, Y.; et al. Air pollution in China: Status and spatiotemporal variations. Environ. Pollut. 2017, 227, 334–347. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.Q.; Zhang, X.Y.; Sun, J.Y.; Zhang, X.C.; Che, H.Z.; Li, Y. Spatial and temporal variations of the concentrations of PM10, PM2.5 and PM1 in China. Atmos. Chem. Phys. 2015, 15, 13585–13598. [Google Scholar] [CrossRef]
- Wang, S.; Zhou, C.; Wang, Z.; Feng, K.; Hubacek, K. The characteristics and drivers of fine particulate matter (PM2.5) distribution in China. J. Clean. Prod. 2017, 142, 1800–1809. [Google Scholar] [CrossRef]
- Wang, P.; Cao, J.J.; Shen, Z.X.; Han, Y.M.; Lee, S.C.; Huang, Y.; Zhu, C.S.; Wang, Q.Y.; Xu, H.M.; Huang, R.J. Spatial and seasonal variations of PM2.5 mass and species during 2010 in Xi’an, China. Sci. Total Environ. 2015, 508, 477–487. [Google Scholar] [CrossRef] [PubMed]
- Yao, L.; Lu, N. Spatiotemporal distribution and short-term trends of particulate matter concentration over China, 2006–2010. Environ. Sci. Pollut. Res. Int. 2014, 21, 9665. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Zhang, X.; Xu, X.; Xu, J.; Meng, W.; Pu, W. Seasonal and diurnal variations of ambient PM2.5 concentration in urban and rural environments in Beijing. Atmos. Environ. 2009, 43, 2893–2900. [Google Scholar] [CrossRef]
- Chen, W.; Tang, H.; Zhao, H. Diurnal, weekly and monthly spatial variations of air pollutants and air quality of Beijing. Atmos. Environ. 2015, 119, 21–34. [Google Scholar] [CrossRef]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the global burden of diseases study 2015. Lancet 2017, 389, 1907. [Google Scholar] [CrossRef]
- Liu, M.; Huang, Y.; Ma, Z.; Jin, Z.; Liu, X.; Wang, H.; Liu, Y.; Wang, J.; Jantunen, M.; Bi, J.; et al. Spatial and temporal trends in the mortality burden of air pollution in China: 2004–2012. Environ. Int. 2017, 98, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Han, Y.; Tang, X.; Zhu, J.; Zhu, T. Estimating adult mortality attributable to PM2.5 exposure in China with assimilated PM2.5 concentrations based on a ground monitoring network. Sci. Total Environ. 2016, 568, 1253. [Google Scholar] [CrossRef] [PubMed]
- Rohde, R.A.; Muller, R.A. Air pollution in China: Mapping of concentrations and sources. PLoS ONE 2015, 10, e0135749. [Google Scholar] [CrossRef] [PubMed]
- Lelieveld, J.; Evans, J.S.; Fnais, M.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Province | Population (×106) | Attributable Deaths in 2015 (×103) | Attributable Deaths in 2016 (×3) | Change from 2015 to 2016 a | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2015−2016 | LC | IHD | Stroke | COPD | SUM | LC | IHD | Stroke | COPD | SUM | LC | IHD | Stroke | COPD | SUM | ||
| Heilongjiang | 38.12 | 37.99 | 3.18 | 11.20 | 21.59 | 3.21 | 39.17 | 2.64 | 10.11 | 17.36 | 2.66 | 32.78 | −539 | −1084 | −4225 | −543 | −6391 |
| Hunan | 67.83 | 68.22 | 7.19 | 23.07 | 46.41 | 7.27 | 83.94 | 6.54 | 21.95 | 43.48 | 6.68 | 78.64 | −659 | −1122 | −2930 | −594 | −5304 |
| Hubei | 58.52 | 58.85 | 6.02 | 17.89 | 36.08 | 6.06 | 66.06 | 5.24 | 17.10 | 33.60 | 5.42 | 61.35 | −784 | −797 | −2481 | −643 | −4705 |
| Jilin | 27.53 | 27.33 | 2.35 | 7.55 | 15.18 | 2.38 | 27.47 | 1.96 | 6.68 | 13.01 | 2.05 | 23.70 | −394 | −866 | −2177 | −326 | −3762 |
| Guangxi | 47.96 | 48.38 | 3.24 | 8.77 | 22.96 | 6.59 | 41.56 | 2.87 | 8.30 | 20.81 | 5.94 | 37.92 | −363 | −476 | −2155 | −642 | −3636 |
| Jiangsu | 79.76 | 79.99 | 10.40 | 12.86 | 23.95 | 4.03 | 51.23 | 9.48 | 12.21 | 22.46 | 3.72 | 47.87 | −919 | −643 | −1493 | −312 | −3366 |
| Guangdong | 108.49 | 109.99 | 6.08 | 9.01 | 15.34 | 2.32 | 32.74 | 5.58 | 8.52 | 13.68 | 2.21 | 29.99 | −503 | −484 | −1654 | −115 | −2756 |
| Yunnan | 47.42 | 47.71 | 2.57 | 7.78 | 18.09 | 5.28 | 33.71 | 2.30 | 7.52 | 16.33 | 4.93 | 31.08 | −272 | −254 | −1757 | −347 | −2630 |
| Shandong | 98.47 | 99.47 | 14.27 | 16.44 | 29.82 | 5.45 | 65.98 | 13.36 | 15.84 | 29.07 | 5.13 | 63.40 | −911 | −606 | −749 | −312 | −2578 |
| Inner Mongolia | 25.11 | 25.20 | 1.47 | 4.07 | 10.51 | 2.98 | 19.03 | 1.29 | 3.71 | 8.97 | 2.68 | 16.65 | −171 | −356 | −1544 | −304 | −2376 |
| Liaoning | 43.82 | 43.78 | 4.98 | 6.37 | 11.87 | 1.94 | 25.16 | 4.64 | 6.18 | 10.87 | 1.77 | 23.46 | −337 | −183 | −1001 | −171 | −1691 |
| Henan | 94.80 | 95.32 | 12.92 | 37.49 | 73.49 | 13.22 | 137.11 | 12.68 | 36.84 | 73.05 | 12.86 | 135.43 | −238 | −649 | −443 | −356 | −1686 |
| Zhejiang | 55.39 | 55.90 | 4.98 | 6.58 | 11.89 | 1.90 | 25.35 | 4.67 | 6.26 | 11.09 | 1.73 | 23.75 | −313 | −319 | −800 | −165 | −1597 |
| Shanghai | 24.15 | 24.20 | 2.17 | 2.75 | 5.07 | 0.82 | 10.81 | 1.89 | 2.53 | 4.53 | 0.72 | 9.67 | −276 | −219 | −548 | −106 | −1148 |
| Gansu | 26.00 | 26.10 | 1.75 | 4.75 | 12.45 | 3.57 | 22.53 | 1.62 | 4.62 | 11.86 | 3.40 | 21.50 | −134 | −130 | −586 | −174 | −1024 |
| Hebei | 74.25 | 74.70 | 9.34 | 10.76 | 19.52 | 3.56 | 43.18 | 9.17 | 10.58 | 19.18 | 3.47 | 42.39 | −172 | −186 | −338 | −98 | −795 |
| Qinghai | 5.88 | 5.93 | 0.41 | 1.11 | 2.89 | 0.81 | 5.21 | 0.35 | 1.01 | 2.53 | 0.73 | 4.62 | −60 | −92 | −357 | −79 | −588 |
| Fujian | 38.39 | 38.74 | 2.67 | 4.02 | 6.45 | 1.03 | 14.18 | 2.54 | 4.06 | 6.18 | 0.97 | 13.75 | −125 | 37 | −275 | −65 | −429 |
| Anhui | 61.44 | 61.96 | 5.78 | 18.09 | 36.68 | 5.90 | 66.46 | 5.65 | 18.25 | 36.49 | 5.70 | 66.09 | −133 | 153 | −190 | −198 | −369 |
| Hainan | 9.11 | 9.17 | 0.44 | 0.76 | 0.89 | 0.16 | 2.25 | 0.37 | 0.73 | 0.72 | 0.15 | 1.96 | −70 | −33 | −174 | −17 | −294 |
| Beijing | 21.71 | 21.73 | 2.33 | 2.69 | 4.88 | 0.89 | 10.79 | 2.28 | 2.69 | 4.83 | 0.86 | 10.66 | −54 | 3 | −51 | −29 | −132 |
| Ningxia | 6.68 | 6.75 | 0.36 | 0.95 | 2.53 | 0.71 | 4.55 | 0.36 | 0.96 | 2.55 | 0.72 | 4.60 | 4 | 10 | 27 | 7 | 48 |
| Tibet | 3.24 | 3.31 | 0.13 | 0.41 | 0.86 | 0.25 | 1.64 | 0.13 | 0.41 | 0.93 | 0.27 | 1.75 | 3 | 8 | 71 | 26 | 107 |
| Guizhou | 35.30 | 35.55 | 2.23 | 6.82 | 16.29 | 4.64 | 29.97 | 2.24 | 6.87 | 16.41 | 4.67 | 30.19 | 16 | 49 | 118 | 33 | 217 |
| Tianjin | 15.47 | 15.62 | 1.82 | 2.14 | 3.86 | 0.68 | 8.50 | 1.88 | 2.16 | 4.00 | 0.71 | 8.75 | 65 | 21 | 132 | 31 | 249 |
| Chongqing | 30.17 | 30.48 | 2.82 | 7.19 | 19.20 | 5.67 | 34.88 | 2.85 | 7.26 | 19.40 | 5.73 | 35.24 | 30 | 76 | 203 | 60 | 369 |
| Xinjiang | 23.60 | 23.98 | 1.38 | 3.53 | 9.42 | 2.78 | 17.11 | 1.59 | 3.78 | 10.36 | 3.20 | 18.92 | 203 | 251 | 939 | 414 | 1807 |
| Jiangxi | 45.66 | 45.92 | 3.84 | 12.98 | 25.51 | 3.80 | 46.13 | 4.01 | 13.45 | 26.92 | 4.02 | 48.41 | 171 | 471 | 1411 | 223 | 2277 |
| Shaanxi | 37.93 | 38.13 | 3.02 | 7.74 | 20.75 | 6.01 | 37.51 | 3.23 | 8.21 | 22.03 | 6.59 | 40.06 | 218 | 472 | 1283 | 580 | 2553 |
| Shanxi | 36.64 | 36.82 | 3.23 | 10.10 | 20.48 | 3.29 | 37.10 | 3.55 | 10.70 | 21.97 | 3.59 | 39.80 | 320 | 597 | 1489 | 292 | 2697 |
| Sichuan | 82.04 | 82.62 | 6.64 | 17.72 | 47.06 | 13.27 | 84.69 | 6.94 | 18.37 | 48.12 | 14.03 | 87.46 | 295 | 650 | 1062 | 762 | 2769 |
| SUM | 1371 | 1380 | 130 | 284 | 592 | 120 | 1126 | 124 | 278 | 573 | 117 | 1092 | −6102 | −5701 | −19,193 | −3168 | −34,164 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feng, L.; Ye, B.; Feng, H.; Ren, F.; Huang, S.; Zhang, X.; Zhang, Y.; Du, Q.; Ma, L. Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016. Int. J. Environ. Res. Public Health 2017, 14, 1321. https://doi.org/10.3390/ijerph14111321
Feng L, Ye B, Feng H, Ren F, Huang S, Zhang X, Zhang Y, Du Q, Ma L. Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016. International Journal of Environmental Research and Public Health. 2017; 14(11):1321. https://doi.org/10.3390/ijerph14111321
Chicago/Turabian StyleFeng, Luwei, Bo Ye, Huan Feng, Fu Ren, Shichun Huang, Xiaotong Zhang, Yunquan Zhang, Qingyun Du, and Lu Ma. 2017. "Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016" International Journal of Environmental Research and Public Health 14, no. 11: 1321. https://doi.org/10.3390/ijerph14111321
APA StyleFeng, L., Ye, B., Feng, H., Ren, F., Huang, S., Zhang, X., Zhang, Y., Du, Q., & Ma, L. (2017). Spatiotemporal Changes in Fine Particulate Matter Pollution and the Associated Mortality Burden in China between 2015 and 2016. International Journal of Environmental Research and Public Health, 14(11), 1321. https://doi.org/10.3390/ijerph14111321