Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety after the 2011 Disaster: The Fukushima Health Management Survey

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Procedures and Participants
2.2. Questionnaire
2.2.1. Subjective Well-Being, Reduction in Radiation Anxiety, Radiation Risk Perceptions, and Radiation Risk Acceptance
2.2.2. Participation, Utilization, and Evaluation of Radiological Countermeasures
Participation
Utilization
Evaluation
2.2.3. Other Questionnaire Items
2.3. Data Procedure
2.4. Statistical Analysis
3. Results
3.1. Participation in, Utilization of, and Evaluation of Radiological Countermeasures
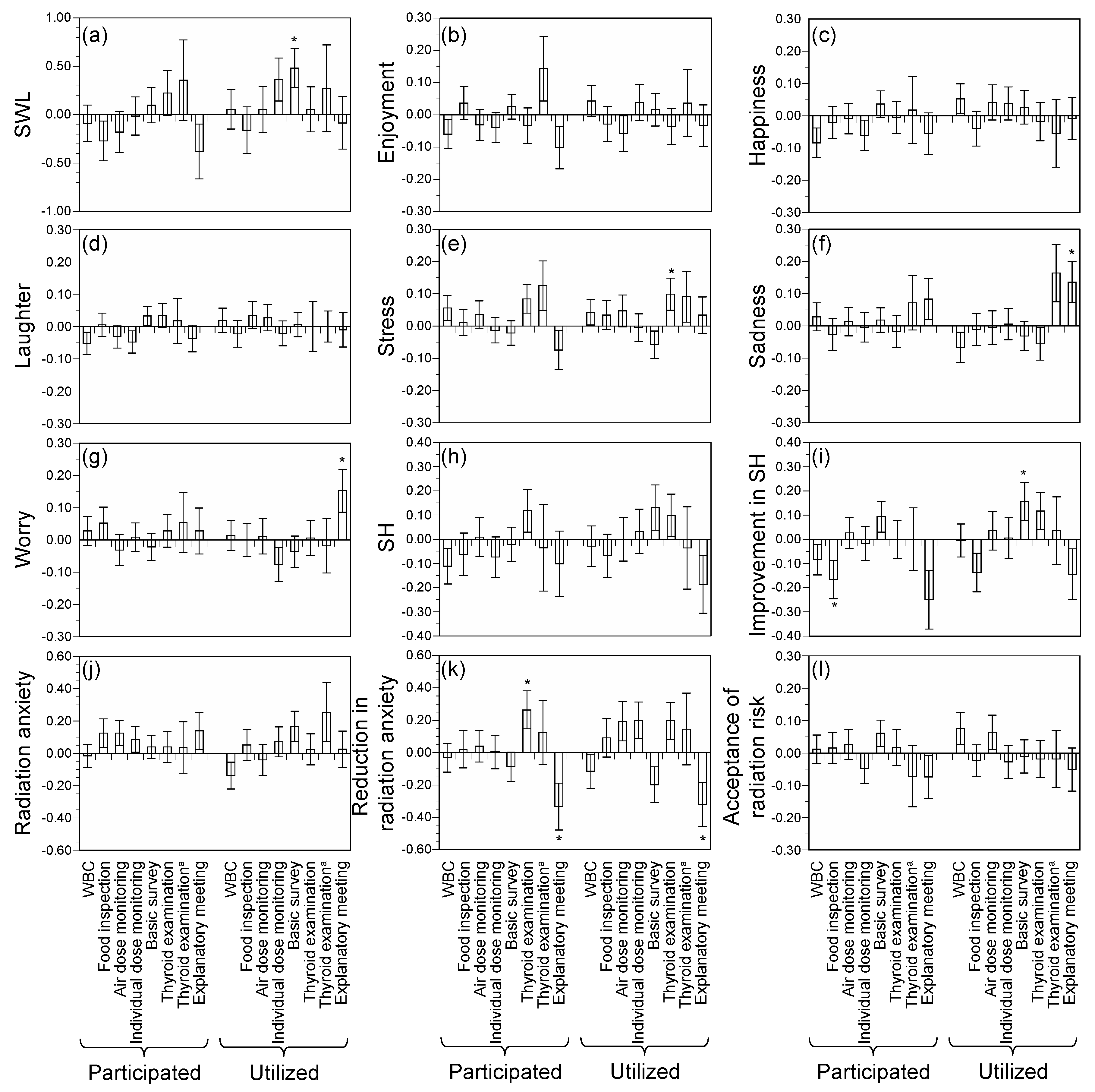
3.2. Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety
4. Discussion
4.1. Implications from Participation in, Utilization of, and Evaluation of Radiological Measures
4.2. Implications from Effects of Radiological Measures on Well-Being and Radiation Anxiety
4.3. Limitations and Future Perspectives
5. Conclusions
- Among radiological countermeasures, thyroid examination, WBC, and air dose monitoring showed higher proportions of participation, utilization, and evaluation, suggesting a high level of public attention.
- Overall, the effects were generally smaller for countermeasures than for individual variations. The basic survey was associated with an improvement of SWL and SH. Thyroid examination was associated with not only a reduction in radiation anxiety but also an increase in stress. Those who participated in food inspection showed a lower improvement in SH. Those who utilized explanatory meetings showed increases in sadness, worry, and radiation anxiety. For a further assessment of causal relationships, continuous surveys with a cohort design are necessary.
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- United Nations Scientific Committee on the Effects of Atomic Radiation. Sources, Effects and Risks of Ionizing Radiation; UNSCEAR 2013 Reports to the General Assembly with Scientific Annexes; United Nations: New York, NY, USA, 2014. [Google Scholar]
- Ishikawa, T. Radiation doses and associated risk from the Fukushima nuclear accident. Asia-Pac. J. Public Health 2017, 29, 18s–28s. [Google Scholar] [CrossRef] [PubMed]
- Normile, D. Epidemic of fear. Science 2016, 351, 1022–1023. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M.; Tanigawa, K.; Murakami, M. After Fukushima: Creating a dialogue. Science 2016, 352, 666. [Google Scholar] [CrossRef] [PubMed]
- Nomura, S.; Blangiardo, M.; Tsubokura, M.; Ozaki, A.; Morita, T.; Hodgson, S. Postnuclear disaster evacuation and chronic health in adults in Fukushima, Japan: A long-term retrospective analysis. BMJ Open 2016, 6, e010080. [Google Scholar] [CrossRef] [PubMed]
- Ebner, D.K.; Ohsawa, M.; Igari, K.; Harada, K.H.; Koizumi, A. Lifestyle-related diseases following the evacuation after the Fukushima Daiichi nuclear power plant accident: A retrospective study of Kawauchi Village with long-term follow-up. BMJ Open 2016, 6, e011641. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Nakano, H.; Nagai, M.; Yumiya, Y.; Zhang, W.; Uemura, M.; Sakai, A.; Hashimoto, S. Changes in cardiovascular risk factors after the Great East Japan Earthquake. Asia-Pac. J. Public Health 2017, 29, 47s–55s. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Tsubokura, M.; Ono, K.; Nomura, S.; Oikawa, T. Additional risk of diabetes exceeds the increased risk of cancer caused by radiation exposure after the Fukushima disaster. PLoS ONE 2017, 12, e0185259. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Yabe, H.; Yasumura, S.; Ohira, T.; Niwa, S.; Ohtsuru, A.; Mashiko, H.; Maeda, M.; Abe, M. Psychological distress and the perception of radiation risks: The Fukushima health management survey. Bull. World Health Organ. 2015, 93, 598–605. [Google Scholar] [CrossRef] [PubMed]
- Oe, M.; Fujii, S.; Maeda, M.; Nagai, M.; Harigane, M.; Miura, I.; Yabe, H.; Ohira, T.; Takahashi, H.; Suzuki, Y.; et al. Three-year trend survey of psychological distress, posttraumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant accident [The Fukushima Health Management Survey]. Psychiatry Clin. Neurosci. 2016, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Tsubokura, M.; Ono, K.; Maeda, M. New “loss of happy life expectancy” indicator and its use in risk comparison after Fukushima disaster. Sci. Total Environ. 2018, 615, 1527–1534. [Google Scholar] [CrossRef] [PubMed]
- Tiefenbach, T.; Kohlbacher, F. Happiness in Japan in times of upheaval: Empirical evidence from the national survey on lifestyle preferences. J. Happiness Stud. 2015, 16, 333–366. [Google Scholar] [CrossRef]
- Rehdanz, K.; Welsch, H.; Narita, D.; Okubo, T. Well-being effects of a major natural disaster: The case of Fukushima. J. Econ. Behav. Organ. 2015, 116, 500–517. [Google Scholar] [CrossRef]
- Hommerich, C. Trust and subjective well-being after the Great East Japan Earthquake, tsunami and nuclear meltdown: Preliminary results. Int. J. Jpn. Sociol. 2012, 21, 46–64. [Google Scholar] [CrossRef]
- Murakami, M.; Harada, S.; Oki, T. Decontamination reduces radiation anxiety and improves subjective well-being after the Fukushima accident. Tohoku J. Exp. Med. 2017, 241, 103–116. [Google Scholar] [CrossRef] [PubMed]
- United Nations. General Assembly Resolution A/RES/70/1, Transforming Our World, the 2030 Agenda for Sustainable Development; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Bok, D. The Politics of Happiness: What Government Can Learn from the New Research on Well-Being; Princeton University Press: Princeton, NJ, USA, 2010. [Google Scholar]
- United Nations Office for Disaster Risk Reduction Sendai Framework for Disaster Risk Reduction. Available online: http://www.unisdr.org/we/coordinate/sendai-framework (accessed on 30 October 2017).
- Hino, Y.; Murakami, M.; Midorikawa, S.; Ohtsuru, A.; Suzuki, S.; Tsuboi, K.; Ohira, T. Explanatory meetings on thyroid examination for the “Fukushima Health Management Survey” after the Great East Japan Earthquake: Reduction of anxiety and improvement of comprehension, and satisfaction. Tohoku J. Exp. Med. 2016, 239, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Sato, A.; Matsui, S.; Goto, A.; Kumagai, A.; Tsubokura, M.; Orita, M.; Takamura, N.; Kuroda, Y.; Ochi, S. Communicating with residents about risks following the Fukushima nuclear accident. Asia-Pac. J. Public Health 2017, 29, 74s–89s. [Google Scholar] [CrossRef] [PubMed]
- Ando, R. Measuring, discussing, and living together: Lessons from 4 years in Suetsugi. Ann. ICRP 2016, 45, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Takamura, N.; Orita, M.; Yamashita, S.; Chhem, R. After Fukushima: Collaboration model. Science 2016, 352, 666. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, M. Using and explaining individual dosimetry data. Asia-Pac. J. Public Health 2017, 29, 110s–119s. [Google Scholar] [CrossRef] [PubMed]
- National Research Council. Improving Risk Communication; National Academy Press: Washington, DC, USA, 1987. [Google Scholar]
- Nomura, S.; Tsubokura, M.; Murakami, M.; Ono, K.; Nishikawa, Y.; Oikawa, T. Towards a long-term strategy for voluntary-based internal radiation contamination monitoring: Representativeness of the monitoring results in Fukushima, Japan. Int. J. Environ. Res. Public Health 2017, 14, 656. [Google Scholar] [CrossRef] [PubMed]
- Tsubokura, M.; Murakami, M.; Nomura, S.; Morita, T.; Nishikawa, Y.; Leppold, C.; Kato, S.; Kami, M. Individual external doses below the lowest reference level of 1 mSv per year five years after the 2011 Fukushima nuclear accident among all children in Soma City, Fukushima: A retrospective observational study. PLoS ONE 2017, 12, e0172305. [Google Scholar] [CrossRef] [PubMed]
- Naito, W.; Uesaka, M.; Yamada, C.; Ishii, H. Evaluation of dose from external irradiation for individuals living in areas affected by the Fukushima Daiichi Nuclear Plant accident. Radiat. Prot. Dosim. 2015, 163, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Yasumura, S.; Ozasa, K.; Kobashi, G.; Yasuda, H.; Miyazaki, M.; Akahane, K.; Yonai, S.; Ohtsuru, A.; Sakai, A.; et al. The Fukushima health management survey: Estimation of external doses to residents in Fukushima prefecture. Sci. Rep. 2015, 5, 12712. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, S. Childhood and adolescent thyroid cancer in Fukushima after the Fukushima Daiichi nuclear power plant accident: 5 years on. Clin. Oncol. 2016, 28, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, A.; Nomura, S.; Tsubokura, M.; Matsumura, T.; Muto, K.; Sato, M.; Gilmour, S. The relationship between media consumption and health-related anxieties after the Fukushima Daiichi nuclear disaster. PLoS ONE 2013, 8, e65331. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Tsubokura, M. Evaluating risk communication after the Fukushima disaster based on nudge theory. Asia-Pac. J. Public Health 2017, 29, 193s–200s. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M. Risk analysis as regulatory science: Toward the establishment of standards. Radiat. Prot. Dosim. 2016, 171, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Nakatani, J.; Oki, T. Evaluation of risk perception and risk-comparison information regarding dietary radionuclides after the 2011 Fukushima nuclear power plant accident. PLoS ONE 2016, 11, e0165594. [Google Scholar] [CrossRef] [PubMed]
- Fukushima Prefecture. Kako no Kekka (Nenrei 5 Sai Kaikyu Betsu Suikei Jjinkou). Available online: https://www.pref.fukushima.lg.jp/sec/11045b/15859.html (accessed on 21 September 2017). (In Japanese).
- Frey, B.S. Happiness: A Revolution in Economics; Massachusetts Institute of Technology Press: Cambridge, MA, USA, 2008. [Google Scholar]
- Kahneman, D.; Deaton, A. High income improves evaluation of life but not emotional well-being. Proc. Natl. Acad. Sci. USA 2010, 107, 16489–16493. [Google Scholar] [CrossRef] [PubMed]
- Nettle, D. Happiness: The Science behind Your Smile; Oxford University Press: Oxford, UK, 2005. [Google Scholar]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Lindell, M.K.; Barnes, V.E. Protective response to technological emergency: Risk perception and behavioral intention. Nucl. Saf. 1989, 27, 457–467. [Google Scholar] [CrossRef]
- Takebayashi, Y.; Lyamzina, Y.; Suzuki, Y.; Murakami, M. Risk perception and anxiety regarding radiation after the 2011 Fukushima nuclear power plant accident: A systematic qualitative review. Int. J. Environ. Res. Public Health 2017, 14, 1306. [Google Scholar] [CrossRef] [PubMed]
- Kurimoto, A.; Awata, S.; Ohkubo, T.; Tsubota-Utsugi, M.; Asayama, K.; Takahashi, K.; Suenaga, K.; Satoh, H.; Imai, Y. Reliability and validity of the Japanese version of the abbreviated Lubben Social Network Scale. Jpn. J. Geriatr. 2011, 48, 149–157. (In Japanese) [Google Scholar] [CrossRef]
- Midorikawa, S.; Tanigawa, K.; Suzuki, S.; Ohtsuru, A. Psychosocial issues related to thyroid examination after a radiation disaster. Asia-Pac. J. Public Health 2017, 29, 63s–73s. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Randolph, J.J.; Falbe, K.; Manuel, A.K.; Balloun, J.L. A step-by-step guide to propensity score matching in R. Pract. Assess. Res. Eval. 2014, 19, 18. [Google Scholar]
- Nakashima, K.; Orita, M.; Fukuda, N.; Taira, Y.; Hayashida, N.; Matsuda, N.; Takamura, N. Radiocesium concentrations in wild mushrooms collected in Kawauchi Village after the accident at the Fukushima Daiichi nuclear power plant. PeerJ 2015, 3, e1427. [Google Scholar] [CrossRef] [PubMed]
- Taira, Y.; Hayashida, N.; Orita, M.; Yamaguchi, H.; Ide, J.; Endo, Y.; Yamashita, S.; Takamura, N. Evaluation of environmental contamination and estimated exposure doses after residents return home in Kawauchi Village, Fukushima Prefecture. Environ. Sci. Technol. 2014, 48, 4556–4563. [Google Scholar] [CrossRef] [PubMed]
- Ohtsuru, A.; Tanigawa, K.; Kumagai, A.; Niwa, O.; Takamura, N.; Midorikawa, S.; Nollet, K.; Yamashita, S.; Ohto, H.; Chhem, R.K.; et al. Nuclear disasters and health: Lessons learned, challenges, and proposals. Lancet 2015, 386, 489–497. [Google Scholar] [CrossRef]
- Hayashida, N.; Imaizumi, M.; Shimura, H.; Furuya, F.; Okubo, N.; Asari, Y.; Nigawara, T.; Midorikawa, S.; Kotani, K.; Nakaji, S.; et al. Thyroid ultrasound findings in a follow-up survey of children from three Japanese prefectures: Aomori, Yamanashi, and Nagasaki. Sci. Rep. 2015, 5, 9046. [Google Scholar] [CrossRef] [PubMed]
- Science Council of Japan, Daiichibu Fukushima Genpatsu Saigai Gono Kagaku to Shakai no Arikata Wotou Bunkakai Kagaku to Shakai no Yoriyoi Kankei ni Mukete: Fukushima Genpatsu Saigaigo no Sinraisousitu wo Fumaete. Available online: http://www.scj.go.jp/ja/info/kohyo/pdf/kohyo-22-t195-6.pdf (accessed on 13 October 2017). (In Japanese)
- Lochard, J. Stakeholder engagement in regaining decent living conditions after Chernobyl. Radioact. Environ. 2013, 19, 311–331. [Google Scholar]
- Lochard, J. Rehabilitation of living conditions in territories contaminated by the Chernobyl accident: The ETHOS project. Health Phys. 2007, 93, 522–526. [Google Scholar] [CrossRef] [PubMed]
- Masunaga, T.; Kozlovsky, A.; Lyzikov, A.; Takamura, N.; Yamashit, S. Mental health status among younger generation around Chernobyl. Arch. Med. Sci. 2013, 9, 1114–1116. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men | Women | 20 s | 30 s | 40 s | 50 s | 60 s | |
|---|---|---|---|---|---|---|---|
| This study | 48% | 52% | 13% | 25% | 28% | 20% | 13% |
| General population | 52% | 48% | 14% | 18% | 21% | 21% | 26% |
| N | Participated a | Participated b | Utilized | Evaluated | |
|---|---|---|---|---|---|
| WBC | 1023 | 31% | 53% | 46% | 54% |
| Food inspection | 1023 | 9% | 22% | 41% | 68% |
| Air dose monitoring | 1023 | 34% | 52% | 52% | 61% |
| Individual dose monitoring | 1023 | 15% | 35% | 36% | 41% |
| Basic survey | 1023 | 31% | 42% | 35% | 38% |
| Thyroid examination | 1023 | 1% | 29% | 33% | 53% |
| Thyroid examination c | 373 | 4% | 79% | 72% | 64% |
| Explanatory meeting | 1023 | 7% | 12% | 15% | 39% |
| Utilized (%) | Evaluated (%) | ||||||
|---|---|---|---|---|---|---|---|
| Participation a | Arithmetic Mean | SE | Arithmetic Mean | SE | |||
| WBC | Did not participate | 15% | 2% | *** | 47% | 2% | *** |
| Participated | 74% | 2% | 61% | 2% | |||
| Food inspection | Did not participate | 26% | 2% | *** | 65% | 2% | *** |
| Participated | 90% | 2% | 79% | 3% | |||
| Air dose monitoring | Did not participate | 11% | 1% | *** | 49% | 2% | *** |
| Participated | 88% | 1% | 72% | 2% | |||
| Individual dose monitoring | Did not participate | 11% | 1% | *** | 35% | 2% | *** |
| Participated | 81% | 2% | 51% | 3% | |||
| Basic survey | Did not participate | 10% | 1% | *** | 34% | 2% | ** |
| Participated | 71% | 2% | 44% | 2% | |||
| Thyroid examination | Did not participate | 13% | 1% | *** | 48% | 2% | *** |
| Participated | 84% | 2% | 65% | 3% | |||
| Thyroid examination b | Did not participate | 29% | 5% | *** | 59% | 6% | ns |
| Participated | 84% | 2% | 65% | 3% | |||
| Explanatory meeting | Did not participate | 6% | 1% | *** | 38% | 2% | * |
| Participated | 85% | 3% | 47% | 4% | |||
| Food Inspection | Air Dose Monitoring | Individual Dose Monitoring | Basic Survey | Thyroid Examination | Explanatory Meeting | |
|---|---|---|---|---|---|---|
| Participated a | ||||||
| WBC | 3.30 (2.38–4.57) | 4.20 (3.23–5.45) | 5.73 (4.26–7.71) | 4.40 (3.36–5.77) | 13.7 (9.16–20.4) | 4.73 (2.95–7.57) |
| Food inspection | - | 10.1 (6.62–15.3) | 3.95 (2.91–5.37) | 3.33 (2.45–4.52) | 2.00 (1.47–2.72) | 3.27 (2.22–4.82) |
| Air dose monitoring | - | - | 5.80 (4.32–7.79) | 5.17 (3.93–6.80) | 3.14 (2.35–4.21) | 4.92 (3.08–7.88) |
| Individual dose monitoring | - | - | - | 3.40 (2.60–4.44) | 4.61 (3.46–6.15) | 4.96 (3.33–7.41) |
| Basic survey | - | - | - | - | 4.81 (3.59–6.44) | 4.40 (2.92–6.65) |
| Thyroid examination | - | - | - | - | - | 5.65 (3.81–8.37) |
| Utilized | ||||||
| WBC | 8.70 (6.53–11.6) | 6.80 (5.16–8.97) | 7.70 (5.74–10.3) | 8.15 (6.05–11.0) | 9.44 (6.91–12.9) | 9.11 (5.73–14.5) |
| Food inspection | - | 18.3 (13.1–25.7) | 9.39 (6.99–12.6) | 8.24 (6.16–11.0) | 7.05 (5.27–9.43) | 9.01 (5.88–13.8) |
| Air dose monitoring | - | - | 14.5 (10.3–20.6) | 10.8 (7.78–15.0) | 7.00 (5.13–9.55) | 8.99 (5.47–14.8) |
| Individual dose monitoring | - | - | - | 10.5 (7.75–14.1) | 8.98 (6.67–12.1) | 8.67 (5.81–12.9) |
| Basic survey | - | - | - | - | 10.5 (7.75–14.2) | 8.18 (5.51–12.1) |
| Thyroid examination | - | - | - | - | - | 12.1 (7.94–18.3) |
| Arithmetic Mean | SD | |
|---|---|---|
| SWL [0–10] | 5.90 | 2.21 |
| Enjoyment [0–1] | 0.54 | 0.50 |
| Happiness [0–1] | 0.56 | 0.50 |
| Laughter [0–1] | 0.81 | 0.39 |
| Stress [0–1] | 0.74 | 0.44 |
| Sadness [0–1] | 0.30 | 0.46 |
| Worry [0–1] | 0.59 | 0.49 |
| SH [1–5] | 3.13 | 0.86 |
| Improvement in SH [1–5] | 2.73 | 0.74 |
| Radiation anxiety [1–4] | 2.45 | 0.87 |
| Reduction in radiation anxiety [1–5] | 3.13 | 1.02 |
| Acceptance of radiation risk [0–1] | 0.52 | 0.50 |
| Countermeasures | Outcomes | Effects (Normalized by SD) |
|---|---|---|
| Basic survey (utilization) | SWL | 0.22 |
| Basic survey (utilization) | Improvement in SH | 0.21 |
| Food inspection (participation) | Improvement in SH | −0.22 |
| Thyroid examination (utilization) | Stress | 0.22 |
| Thyroid examination (participation) | Reduction in radiation anxiety | 0.26 |
| Explanatory meeting (utilization) | Sadness | 0.29 |
| Explanatory meeting (utilization) | Worry | 0.31 |
| Explanatory meeting (participation) | Reduction in radiation anxiety | −0.33 |
| Explanatory meeting (utilization) | Reduction in radiation anxiety | −0.32 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murakami, M.; Takebayashi, Y.; Takeda, Y.; Sato, A.; Igarashi, Y.; Sano, K.; Yasutaka, T.; Naito, W.; Hirota, S.; Goto, A.; et al. Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety after the 2011 Disaster: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2018, 15, 124. https://doi.org/10.3390/ijerph15010124
Murakami M, Takebayashi Y, Takeda Y, Sato A, Igarashi Y, Sano K, Yasutaka T, Naito W, Hirota S, Goto A, et al. Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety after the 2011 Disaster: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2018; 15(1):124. https://doi.org/10.3390/ijerph15010124
Chicago/Turabian StyleMurakami, Michio, Yoshitake Takebayashi, Yoshihito Takeda, Akiko Sato, Yasumasa Igarashi, Kazumi Sano, Tetsuo Yasutaka, Wataru Naito, Sumire Hirota, Aya Goto, and et al. 2018. "Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety after the 2011 Disaster: The Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 15, no. 1: 124. https://doi.org/10.3390/ijerph15010124
APA StyleMurakami, M., Takebayashi, Y., Takeda, Y., Sato, A., Igarashi, Y., Sano, K., Yasutaka, T., Naito, W., Hirota, S., Goto, A., Ohira, T., Yasumura, S., & Tanigawa, K. (2018). Effect of Radiological Countermeasures on Subjective Well-Being and Radiation Anxiety after the 2011 Disaster: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health, 15(1), 124. https://doi.org/10.3390/ijerph15010124