Trajectories of Emotional Symptoms and Peer Relationship Problems in Children after Nuclear Disaster: Evidence from the Fukushima Health Management Survey

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Assessments
2.3. Analysis Plan
3. Results
3.1. Sociodemographic Characteristics and Disaster-Related Variables
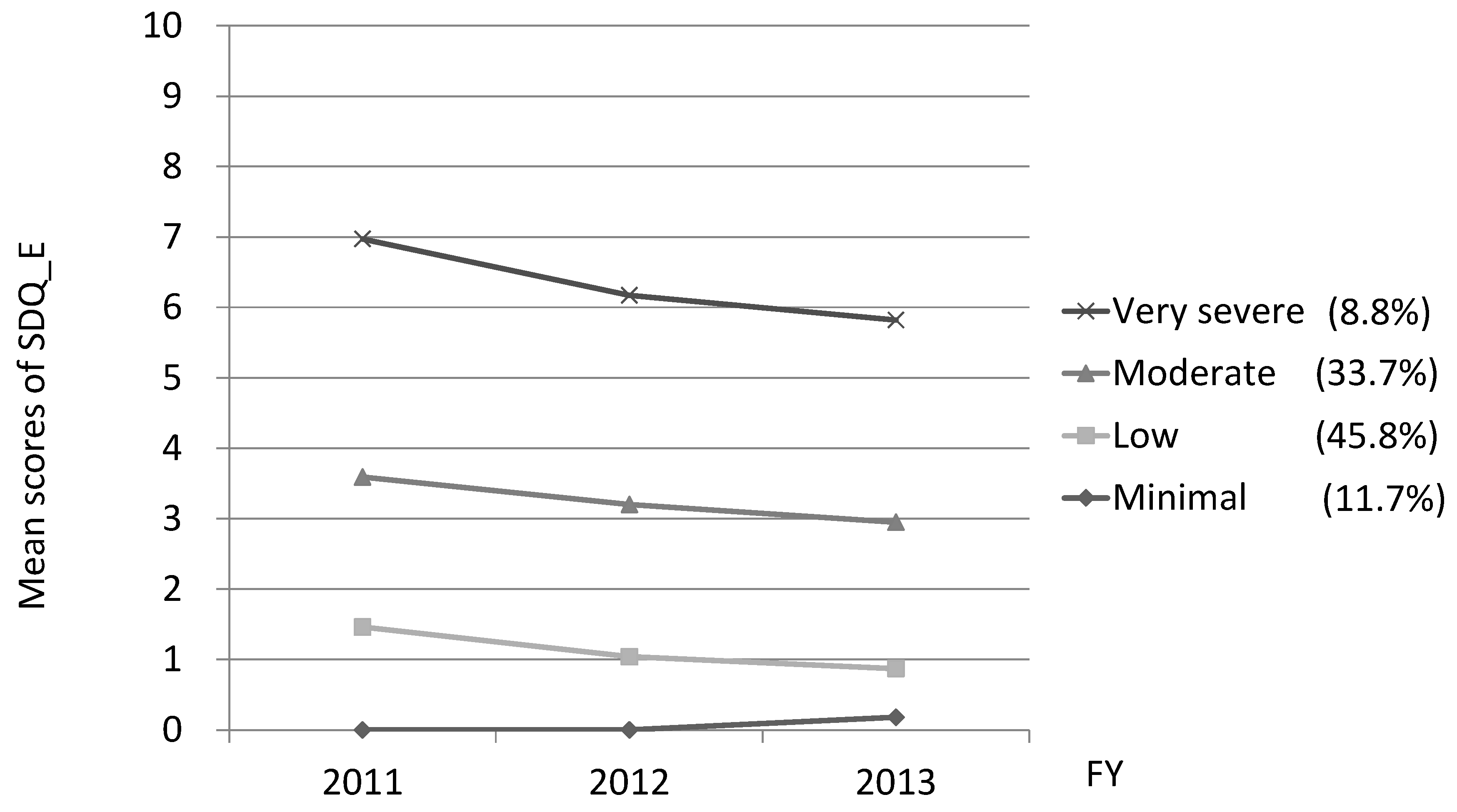
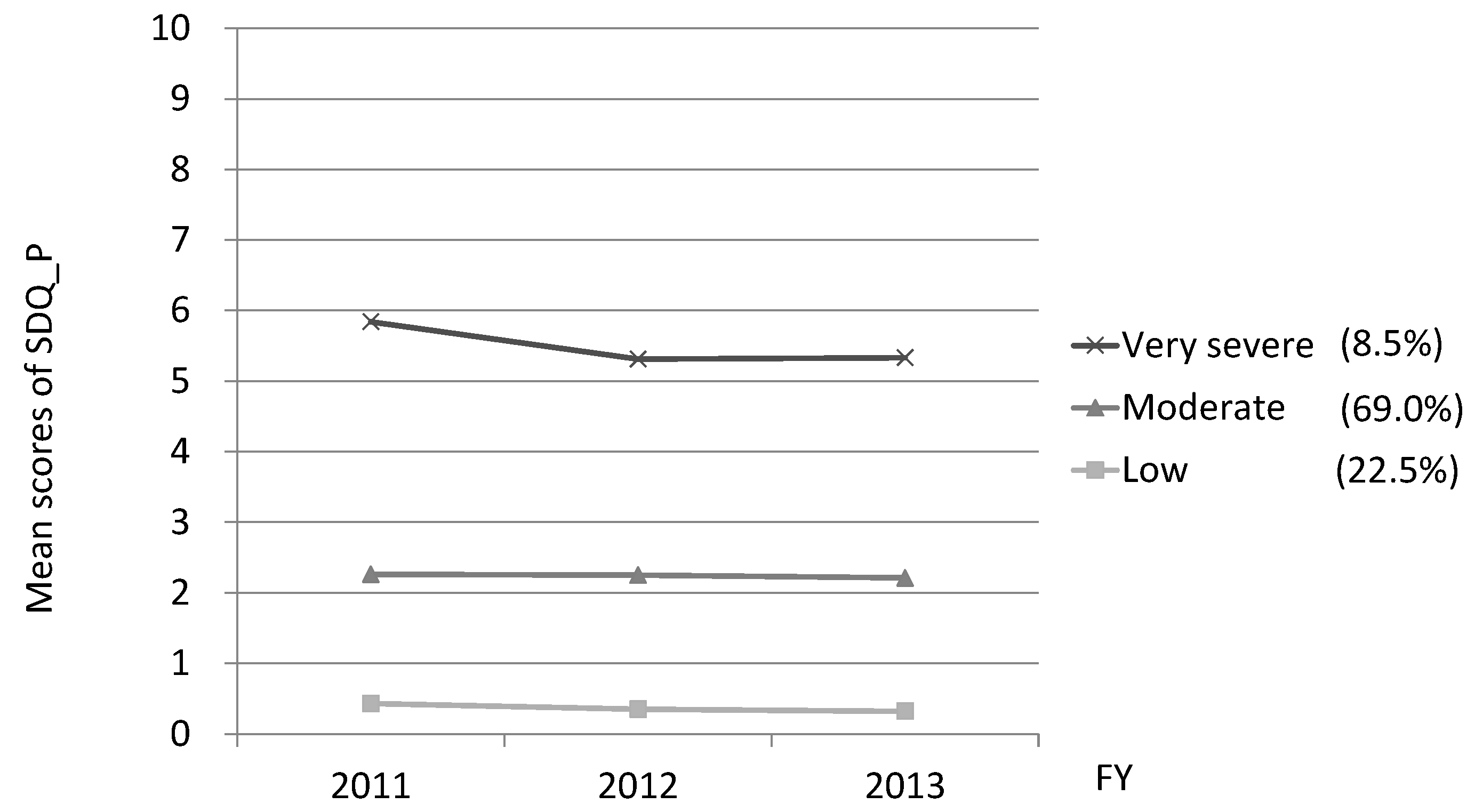
3.2. Trajectories of the Emotional Symptoms and the Peer Relationship Problems
3.3. Sociodemographic Characteristics by Trajectory Group
3.4. Factors Related to the ‘Very Severe’ Trajectory Group
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Usami, M.; Iwadare, Y.; Watanabe, K.; Kodaira, M.; Ushijima, H.; Tanaka, T.; Harada, M.; Tanaka, H.; Sasaki, Y.; Saito, K. Analysis of changes in traumatic symptoms and daily life activity of children affected by the 2011 Japan earthquake and tsunami over time. PLoS ONE 2014, 9, e88885. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Yagi, J.; Homma, H.; Mashiko, H.; Nagao, K.; Okuyama, M.; Great East Japan Earthquake Follow-Up for Children Study Team. Clinically significant behavior problems among young children 2 years after the Great East Japan Earthquake. PLoS ONE 2014, 9, e109342. [Google Scholar] [CrossRef] [PubMed]
- Usami, M.; Iwadare, Y.; Watanabe, K.; Kodaira, M.; Ushijima, H.; Tanaka, T.; Harada, M.; Tanaka, H.; Sasaki, Y.; Okamoto, S.; et al. Prosocial behaviors during school activities among child survivors after the 2011 earthquake and Tsunami in Japan: A retrospective observational study. PLoS ONE 2014, 9, e113709. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Yagi, J.; Homma, H.; Mashiko, H.; Nagao, K.; Okuyama, M.; Great East Japan Earthquake Follow-Up for Children Study Team. Symptoms of Post-Traumatic Stress Disorder among Young Children 2 Years after the Great East Japan Earthquake. Disaster Med. Public Health Prep. 2017, 11, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Ando, S.; Kuwabara, H.; Araki, T.; Kanehara, A.; Tanaka, S.; Morishima, R.; Kondo, S.; Kasai, K. Mental Health Problems in a Community After the Great East Japan Earthquake in 2011: A Systematic Review. Harv. Rev. Psychiatry 2017, 25, 15–28. [Google Scholar] [CrossRef] [PubMed]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K.; Fukushima Health Management Survey Group. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Yabe, H.; Suzuki, Y.; Mashiko, H.; Nakayama, Y.; Hisata, M.; Niwa, S.; Yasumura, S.; Yamashita, S.; Kamiya, K.; Abe, M.; et al. Psychological distress after the Great East Japan Earthquake and Fukushima Daiichi Nuclear Power Plant accident: Results of a mental health and lifestyle survey through the Fukushima Health Management Survey in FY2011 and FY2012. Fukushima J. Med. Sci. 2014, 60, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Hallal, P.C.; Martínez-Mesa, J.; Coll, C.V.; Mielke, G.I.; Mendes, M.A.; Peixoto, M.B.; Munhoz, T.N.; Ramires, V.V.; Assunção, M.C.; Gonçalves, H.; et al. Physical Activity at 11 Years of Age and Incidence of Mental Health Problems in Adolescence: Prospective Study. J. Phys. Act. Health 2015, 12, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Sagatun, A.; Søgaard, A.J.; Bjertness, E.; Selmer, R.; Heyerdahl, S. The association between weekly hours of physical activity and mental health: A three-year follow-up study of 15–16-year-old students in the city of Oslo, Norway. BMC Public Health 2007, 7, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiles, N.J.; Jones, G.T.; Haase, A.M.; Lawlor, D.A.; Macfarlane, G.J.; Lewis, G. Physical activity and emotional problems amongst adolescents: A longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The Strengths and Difficulties Questionnaire: A research note. J. Child Psychol. Psychiatry 1997, 38, 581–586. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R. The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric caseness and consequent burden. J. Child Psychol. Psychiatry 1999, 40, 791–799. [Google Scholar] [CrossRef] [PubMed]
- Goodman, R.; Meltzer, H.; Bailey, V. The Strengths and Difficulties Questionnaire: A pilot study on the validity of the self-report version. Eur. Child Adolesc. Psychiatry 1998, 7, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Matsuishi, T.; Nagano, M.; Araki, Y.; Tanaka, Y.; Iwasaki, M.; Yamashita, Y.; Nagamitsu, S.; Iizuka, C.; Ohya, T.; Shibuya, K.; et al. Scale properties of the Japanese version of the Strengths and Difficulties Questionnaire (SDQ): A study of infant and school children in community samples. Brain Dev. 2008, 30, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Moriwaki, A.; Kamio, Y. Normative data and psychometric properties of the strengths and difficulties questionnaire among Japanese school-aged children. Child Adolesc. Psychiatry Ment. Health 2014, 8, 1. [Google Scholar] [CrossRef] [PubMed]
- Jones, B.L.; Nagin, D.S.; Roeder, K. A SAS procedure based on mixture models for estimating developmental trajectories. Sociol. Methods Res. 2001, 29, 374–393. [Google Scholar] [CrossRef]
- Jones, B.L.; Nagin, D.S. Advances in group-based trajectory modeling and an SAS procedure for estimating them. Sociol. Methods Res. 2007, 35, 542–571. [Google Scholar] [CrossRef]
- McDermott, B.M.; Lee, E.M.; Judd, M.; Gibbon, P. Posttraumatic stress disorder and general psychopathology in children and adolescents following a wildfire disaster. Can. J. Psychiatry 2005, 50, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Usami, M.; Iwadare, Y.; Kodaira, M.; Watanabe, K.; Ushijima, H.; Tanaka, T.; Harada, M.; Tanaka, H.; Sasaki, Y.; Saito, K. Did parents and teachers struggle with child survivors 20 months after the 2011 earthquake and tsunami in Japan? A retrospective observational study. PLoS ONE 2014, 9, e96459. [Google Scholar] [CrossRef] [PubMed]
- Caci, H.; Morin, A.J.; Tran, A. Investigation of a bifactor model of the Strengths and Difficulties Questionnaire. Eur. Child Adolesc. Psychiatry 2015, 24, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.M.; Rubin, K.H.; Laursen, B.; Booth-LaForce, C.; Rose-Krasnor, L. Preference-for-solitude and adjustment difficulties in early and late adolescence. J. Clin. Child Adolesc. Psychol. 2013, 42, 834–842. [Google Scholar] [CrossRef] [PubMed]
- Tobia, V.; Marzocchi, G.M. The Strengths and Difficulties Questionnaire-Parents for Italian School-Aged Children: Psychometric Properties and Norms. Child Psychiatry Hum. Dev. 2017. [Google Scholar] [CrossRef] [PubMed]
- Koskelainen, M. The Strengths and Difficulties Questionnaire among Finnish School-Aged Children and Adolescents; Painosalama Oy: Turku, Finland, 2008. [Google Scholar]
- Litman, L.; Costantino, G.; Waxman, R.; Sanabria-Velez, C.; Rodriguez-Guzman, V.M.; Lampon-Velez, A.; Brown, R.; Cruz, T. Relationship between Peer Victimization and Posttraumatic Stress among Primary School Children. J. Trauma Stress 2015, 28, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Abdulsalam, A.J.; Al Daihani, A.E.; Francis, K. Prevalence and Associated Factors of Peer Victimization (Bullying) among Grades 7 and 8 Middle School Students in Kuwait. Int. J. Pediatr. 2017, 2017, 2862360. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.J.; Rudolph, K.D. A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychol. Bull. 2006, 132, 98–131. [Google Scholar] [CrossRef] [PubMed]
- Allison, K.R.; Adlaf, E.M.; Irving, H.M.; Hatch, J.L.; Smith, T.F.; Dwyer, J.J.; Goodman, J. Relationship of vigorous physical activity to psychologic distress among adolescents. J. Adolesc. Health 2005, 37, 164–166. [Google Scholar] [CrossRef] [PubMed]
- Kirkcaldy, B.D.; Shephard, R.J.; Siefen, R.G. The relationship between physical activity and self-image and problem behaviour among adolescents. Soc. Psychiatry Psychiatr. Epidemiol. 2002, 37, 544–550. [Google Scholar] [CrossRef] [PubMed]
- Page, R.M.; Tucker, L.A. Psychosocial discomfort and exercise frequency: An epidemiological study of adolescents. Adolescence 1994, 29, 183–191. [Google Scholar] [PubMed]
- Oe, M.; Fujii, S.; Maeda, M.; Nagai, M.; Harigane, M.; Miura, I.; Yabe, H.; Ohira, T.; Takahashi, H.; Suzuki, Y.; et al. Three-year trend survey of psychological distress, post-traumatic stress, and problem drinking among residents in the evacuation zone after the Fukushima Daiichi Nuclear Power Plant accident [The Fukushima Health Management Survey]. Psychiatry Clin. Neurosci. 2016, 70, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Tsujiuchi, T.; Masuda, K.; Iwagaki, T.; Ishikawa, N.; Fukuda, C.; Hirata, S.; Inomata, T.; Negayama, K.; Kojima, T.; et al. Social Factors Affecting Psychological Stress of the Evacuees Out of Fukushima Prefecture by the Cause of Nuclear Accident after the Great East Japan Earthquake: Suggestions from Longitudinal Questionnare Survey. Jpn. J. Psychosom. Med. 2016, 56, 819–832. [Google Scholar]
- Bromet, E.J.; Goldgaber, D.; Carlson, G.; Panina, N.; Golovakha, E.; Gluzman, S.F.; Gilbert, T.; Gluzman, D.; Lyubsky, S.; Schwartz, J.E. Children’s well-being 11 years after the Chornobyl catastrophe. Arch. Gen. Psychiatry 2000, 57, 563–571. [Google Scholar] [CrossRef] [PubMed]
- Endo, T.; Shioiri, T.; Toyabe, S.; Akazawa, K.; Someya, T. Parental mental health affects behavioral changes in children following a devastating disaster: A community survey after the 2004 Niigata-Chuetsu earthquake. Gen. Hosp. Psychiatry 2007, 29, 175–176. [Google Scholar] [CrossRef] [PubMed]
- Stone, L.L.; Otten, R.; Engels, R.C.; Vermulst, A.A.; Janssens, J.M. Psychometric properties of the parent and teacher versions of the strengths and difficulties questionnaire for 4- to 12-year-olds: A review. Clin. Child Fam. Psychol. Rev. 2010, 13, 254–274. [Google Scholar] [CrossRef] [PubMed]
- Imamura, K.; Sekiya, Y.; Asai, Y.; Umeda, M.; Horikoshi, N.; Yasumura, S.; Yabe, H.; Akiyama, T.; Kawakami, N. The effect of a behavioral activation program on improving mental and physical health complaints associated with radiation stress among mothers in Fukushima: A randomized controlled trial. BMC Public Health 2016, 16, 1144. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Gender | |
|---|---|
| Male | 4213 |
| Female | 4069 |
| Age at time of disaster (yrs) | |
| 6 | 79 |
| 7 | 1340 |
| 8 | 1362 |
| 9 | 1420 |
| 10 | 1395 |
| 11 | 1390 |
| 12 | 1296 |
| Experience of disaster | |
| Earthquake | 7422 |
| Tsunami | 879 |
| Heard the sound of the nuclear plant explosion | 2971 |
| Missing | 797 |
| Living place (current address) in 2011 | |
| In Fukushima prefecture | 5937 |
| Out of Fukushima prefecture | 1513 |
| Missing | 832 |
| Exercise habits in 2011 | |
| Almost every day | 939 |
| 2–4 times a week | 1500 |
| Once a week | 1081 |
| Very little | 3967 |
| Missing | 795 |
| Predictor | OR (95% CI) for Emotional Symptoms | OR (95% CI) for Peer Relationship Problems |
|---|---|---|
| Gender | ||
| Female | 1.22 (1.03–1.45) * | 0.66 (0.55–0.78) ** |
| Age at time of disaster | ||
| ≤9 years | 1.04 (0.88–1.24) | 0.90 (0.76–1.07) |
| Experience of disaster | ||
| Tsunami | 1.37 (1.08–1.73) * | 1.16 (0.91–1.48) |
| Heard the sound of the nuclear plant explosion | 1.69 (1.42–2.01) ** | 1.21 (1.02–1.44) * |
| Living place (current address) in 2011 | ||
| Out of Fukushima prefecture | 1.25 (1.02–1.52) * | 1.05 (0.85–1.28) |
| Exercise habits in 2011 | ||
| Very little | 1.48 (1.24–1.77) ** | 1.60 (1.34–1.90) ** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oe, M.; Maeda, M.; Ohira, T.; Itagaki, S.; Harigane, M.; Suzuki, Y.; Yabe, H.; Yasumura, S.; Kamiya, K.; Ohto, H. Trajectories of Emotional Symptoms and Peer Relationship Problems in Children after Nuclear Disaster: Evidence from the Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2018, 15, 82. https://doi.org/10.3390/ijerph15010082
Oe M, Maeda M, Ohira T, Itagaki S, Harigane M, Suzuki Y, Yabe H, Yasumura S, Kamiya K, Ohto H. Trajectories of Emotional Symptoms and Peer Relationship Problems in Children after Nuclear Disaster: Evidence from the Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2018; 15(1):82. https://doi.org/10.3390/ijerph15010082
Chicago/Turabian StyleOe, Misari, Masaharu Maeda, Tetsuya Ohira, Shuntaro Itagaki, Mayumi Harigane, Yuriko Suzuki, Hirooki Yabe, Seiji Yasumura, Kenji Kamiya, and Hitoshi Ohto. 2018. "Trajectories of Emotional Symptoms and Peer Relationship Problems in Children after Nuclear Disaster: Evidence from the Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 15, no. 1: 82. https://doi.org/10.3390/ijerph15010082
APA StyleOe, M., Maeda, M., Ohira, T., Itagaki, S., Harigane, M., Suzuki, Y., Yabe, H., Yasumura, S., Kamiya, K., & Ohto, H. (2018). Trajectories of Emotional Symptoms and Peer Relationship Problems in Children after Nuclear Disaster: Evidence from the Fukushima Health Management Survey. International Journal of Environmental Research and Public Health, 15(1), 82. https://doi.org/10.3390/ijerph15010082