Blood Lead Levels and Risk Factors for Lead Exposure in a Pediatric Population in Ho Chi Minh City, Vietnam

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Sample Selection
2.2. Questionnaire
2.3. Blood Sampling and Analysis
2.4. Reporting
2.5. Data Analysis
3. Results
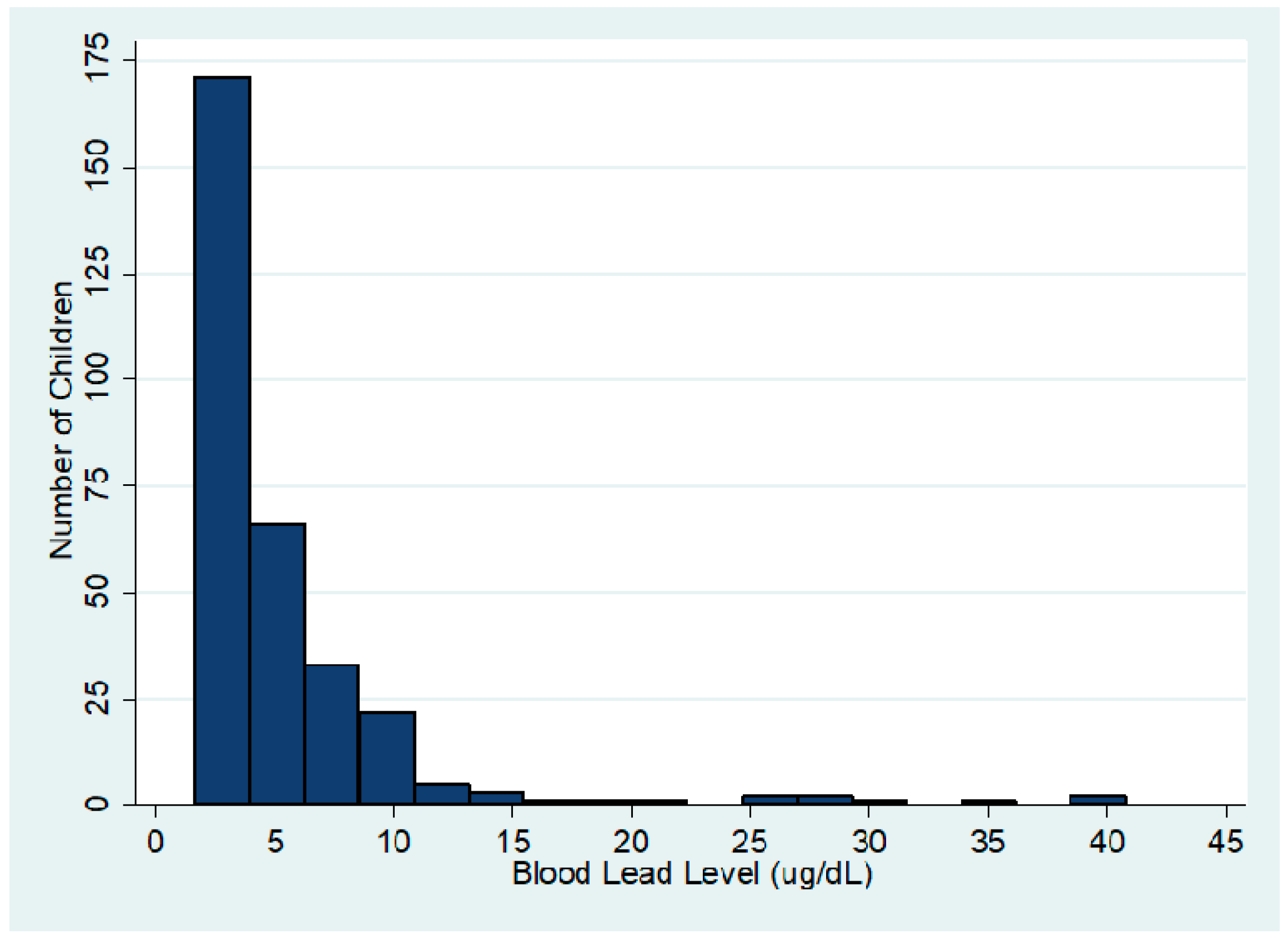
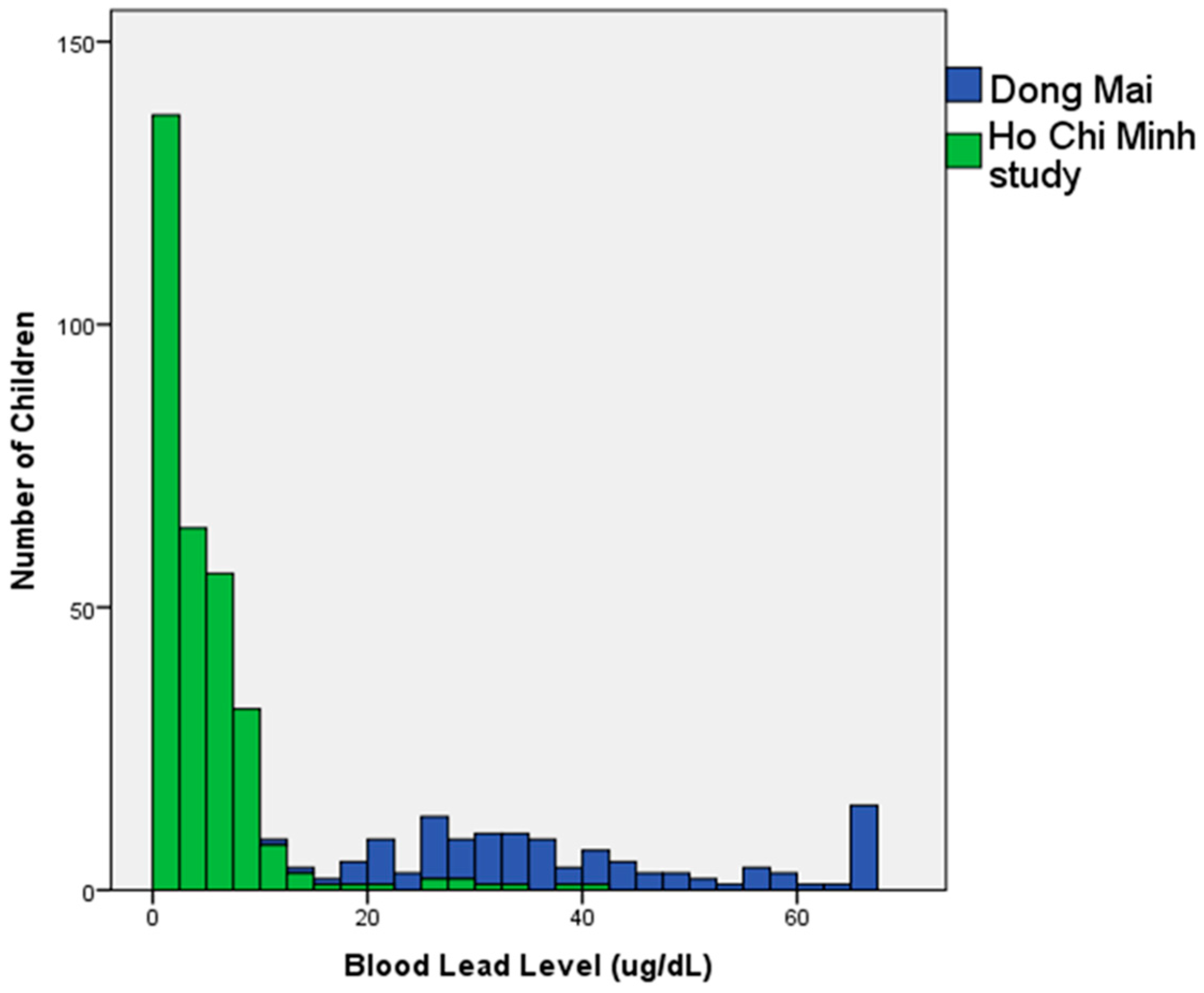
3.1. Overall Distribution of BLL
3.2. Subject Characteristics
3.3. Geographic Distribution of BLL
3.4. Child and Family Characteristics and Distribution of Blood Lead Levels
3.5. Risk Factors for High Blood Lead Levels
3.5.1. Bivariate Analysis
3.5.2. Multivariate Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Lead Poisoning and Health Fact Sheet. Available online: http://www.who.int/mediacentre/factsheets/fs379/en/ (accessed on 15 September 2017).
- World Health Organization International Programme on Chemical Safety. The Public Health Impact of Chemical: Knowns and Unknowns. Available online: http://apps.who.int/iris/bitstream/10665/206553/1/WHO_FWC_PHE_EPE_16.01_eng.pdf (accessed on 9 November 2017).
- Landrigan, P.; Fuller, R.; Acosta, N.J.; Adeyi, O.; Arnold, R.; Basu, N.; Baldé, A.; Bertollini, R.; Bose-O’Reilly, S.; Boufford, J.; et al. The lancet commission on pollution and health. Lancet 2017. [Google Scholar] [CrossRef]
- Fewtrell, L.J.; Prüss-Üstün, A.; Landrigan, P.; Ayuso-Mateos, J.L. Estimating the global burden of disease of mild mental retardation and cardiovascular diseases from environmental lead exposure. Environ. Res. 2004, 94, 120–133. [Google Scholar] [CrossRef]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef]
- Tong, S.; von Schirnding, Y.E.; Prapamontol, T. Environmental lead exposure: A public health problem of global dimensions. Bull. World Health Organ. 2000, 78, 1068–1078. [Google Scholar] [PubMed]
- Fischetti, M. Lead exposure on the rise despite decline in poisoning cases. Sci. Am. 2013. Available online: https://www.scientificamerican.com/article/lead-exposure-on-the-rise/ (accessed on 15 September 2017).
- He, K.; Wang, S.; Zhang, J. Blood lead levels of children and its trend in China. Sci. Total Environ. 2009, 407, 3986–3993. [Google Scholar] [CrossRef] [PubMed]
- Nichani, V.; Li, W.I.; Smith, M.A.; Noonan, G.; Kulkarni, M.; Kodavar, M.; Naeherer, L.P. Blood lead levels in children after phase-out of leaded gasoline in Bombay, India. Sci. Total Environ. 2006, 363, 95–106. [Google Scholar] [CrossRef] [PubMed]
- Thomas, V.M.; Socolow, R.H.; Fanelli, J.J.; Spiro, T.G. Effects of reducing lead in gasoline: An analysis of the international experience. Environ. Sci. Technol. 1999, 33, 3942–3948. [Google Scholar] [CrossRef]
- American Academy of Pediatrics, Committee on Environmental Health. Lead exposure in children: Prevention, detection, and management. Pediatrics 2005, 116, 1036–1046. [Google Scholar]
- World Bank. An Overnight Success: Vietnam’s Switch to Unleaded Gasoline; World Bank: Washington, DC, USA, 2002; Available online: https://openknowledge.worldbank.org/handle/10986/19894 (accessed on 25 December 2017).
- Gottesfeld, P.; Pokhrel, A.K. Review: Lead exposure in battery manufacturing and recycling in developing countries and among children in nearby communities. J. Occup. Environ. Hyg. 2011, 8, 520–532. [Google Scholar] [CrossRef] [PubMed]
- Ericson, B.; Landrigan, P.; Taylor, M.P.; Frostad, J.; Caravanos, J.; Keith, J.; Fuller, R. The global burden of lead toxicity attributable to informal used lead-acid battery sites. Ann. Glob. Health 2016, 82, 686–699. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Environment of Korea. Environmental Briefing Note. Environmental Management for Traditional Craft Villages in Vietnam; Korea-World Bank: Seoul, Korea, 2011; Available online: http://siteresources.worldbank.org/INTEAPREGTOPENVIRONMENT/Resources/Envi_Man_Craft_Viet.pdf (accessed on 15 September 2017).
- Daniell, W.; Tung, L.V.; Wallace, R.; Havens, D.; Karr, C.; Diep, N.B.; Croteau, G.A.; Beaudet, N.J.; Bao, N.D. Childhood lead exposure from battery recycling in Vietnam. BioMed. Res. Int. 2015, 2015, 193715. [Google Scholar] [CrossRef] [PubMed]
- Magellan Diagnostics, Inc. LeadCare II Product Support; Magellan Diagnostics, Inc.: North Billerica, MA, USA; Available online: http://www.leadcare2.com/Product-Support/FAQs (accessed on 9 November 2017).
- Magellan Diagnostics, Inc. LeadCare II Package Insert; Magellan Diagnostics, Inc.: North Billerica, MA, USA, 2016; Available online: http://www.leadcare2.com/getmedia/21d1301e-efee-480f-9586-128f1dbc568f/80-0-052-Package-Insert,-LeadCare-II-Test-Kit-v109-Rev02.pdf.aspx (accessed on 9 November 2017).
- Helsel, D. Less than obvious: Statistical treatment of data below the detection limit. Environ. Sci. Technol. 1990, 24, 1766–1774. [Google Scholar] [CrossRef]
- Chomchai, C.; Padungtod, C.; Chomchai, S. Predictors of elevated blood lead level in Thai children: A pilot study using risk assessment questionnaire. J. Med. Assoc. Thail. 2005, 88, S53–S58. [Google Scholar]
- Hashim, J.H.; Hashim, Z.; Omar, A.; Shamsudin, S.B. Blood lead levels of urban and rural Malaysian primary school children. Asia Pac. J. Public Health 2000, 12, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Riddell, T.; Solon, O.; Quimbo, S.A.; Tan, C.M.C.; Butrick, E.; Peabody, J.W. Elevated blood-lead levels among children living in the rural Philippines. Bull. World Health Organ. 2007, 85, 674–680. [Google Scholar] [CrossRef] [PubMed]
- Albalak, R.; Noonan, G.; Buchanan, S.; Flanders, W.D.; Gotway-Crawford, C.; Kim, D.; Jones, R.L.; Sulaiman, R.; Blumenthal, W.; Tan, R.; et al. Blood lead levels and risk factors for lead poisoning among children in Jakarta, Indonesia. Sci. Total Environ. 2003, 301, 75–85. [Google Scholar] [CrossRef]
- Liu, J.; Ai, Y.; McCauley, L.; Pinto-Martin, J.; Yan, C.; Shen, X.; Needleman, H. Blood lead levels and associated sociodemographic factors among preschool children in the South Eastern region of China. Paediatr. Perinat. Epidemiol. 2012, 26, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Charney, E.; Sayre, J.; Coulter, M. Increased lead absorption in inner city children: Where does the lead come from? Pediatrics 1980, 65, 226–231. [Google Scholar] [PubMed]
- Agency for Toxic Substances and Disease Registry. Lead Toxicity: What Is the Biological Fate of Lead in the Body? Agency for Toxic Substances and Disease Registry: Atlanta, GA, USA, 2017. Available online: https://www.atsdr.cdc.gov/csem/csem.asp?csem=34&po=9 (accessed on 27 December 2017).
- Dezan Shira & Associates. Vietnam Briefing. Available online: http://www.vietnam-briefing.com/regional-intelligence/binh-duong.html (accessed on 26 December 2017).



{kind=link}
{kind=link}
| Child and Family Characteristics | HCMC | Other Provinces |
|---|---|---|
| Gender | ||
| Male | 91 (63%) | 98 (59%) |
| Female | 52 (36%) | 67 (41%) |
| Age (months, mean and SD) | 19.3 (22.0) | 18.0 (19.0) |
| Height (cm, mean) | 76.9 (17.1) | 75.3 (14.6) |
| Weight (kg, mean) | 10.2 (5.1) | 9.8 (6.1) |
| Hemoglobin (g/dL, mean) | 11.7 (1.5) | 11.7 (2.6) |
| Hematocrit (%, mean) | 36.1 (3.7) | 35.6 (3.6) |
| Potential Lead Exposures | ||
| Household member recycles | 3 (2%) | 2 (1%) |
| Child participates in recycling | 0 | 1 (<1%) |
| Lead recycling in the house (in the past) | 0 | 2 (1%) |
| Lead recycling in the home (currently) | 0 | 2 (1%) |
| Using battery casings in the home for walls, furniture, or other purposes | 0 | 1 (<1%) |
| Using battery casings outside the home for driveway, fences, or other purposes | 0 | 1 (<1%) |
| Neighborhood lead recycling | 2 (1%) | 2 (1%) |
| Neighborhood burning of lead recycling waste | 1 (<1%) | 1 (<1%) |
| Metal recycling or melting | 2 (1%) | 4 (2%) |
| Occupational Exposures | ||
| Parents do automotive work | 4 (3%) | 4 (2%) |
| Parents do ceramics/glazing | 1 (<1%) | 5 (3%) |
| Parents do welding | 19 (13%) | 31 (19%) |
| Environmental Exposures | ||
| Source of Drinking Water | ||
| Piped | 65 (45%) | 37 (22%) |
| Bottled | 52 (36%) | 43 (26%) |
| Rainwater | 2 (1%) | 7 (4%) |
| Well Water | 26 (18%) | 78 (47%) |
| Peeling paint | 48 (34%) | 47 (29%) |
| Live near a busy intersection | 27 (19%) | 58 (35%) |
| Use traditional medicines | 117 (81%) | 108 (65%) |
| Age of home (mean) (years) | 10.8 (10.3) | 8.67 (6.7) |
| Home is painted-outside | 115 (80%) | 125 (76%) |
| Home is painted-inside | 124 (86%) | 131 (79%) |
| Years since home was most recently painted | 3.65 (4.3) | 3.9 (4.0) |
| Symptoms | ||
| Abdominal Pain | 10 (7%) | 12 (7%) |
| Constipation | 12 (8%) | 17 (10%) |
| Educational Factors | ||
| Highest level of education in the home | ||
| None | 2 (1%) | 2 (1%) |
| Grade School | 47 (33%) | 69 (42%) |
| High School | 53 (37%) | 71 (43%) |
| University Degree | 40 (28%) | 24 (14%) |
| University Degree +*** | 2 (1%) | 0 |
| Child has problems learning in school | 5 (3%) | 9 (5%) |
| Attends school outside the home | 35 (24%) | 42 (25%) |
| Province | Number (% of Total) | Mean BLL (μg/dL) | Median BLL (μg/dL) IQR |
|---|---|---|---|
| Binh Duong | 59 (19%) | 6.0 | 5.4 (1.65–7.9) |
| Binh Phuoc | 21 (6.8%) | 4.2 | 1.7 (1.65–3.8) |
| Dong Nai | 39 (12.5%) | 6.7 | 4.0 (1.65–7.7) |
| Dak Nong | 5 (1.6%) | 4.9 | 3.8 (1.65–4.1) |
| HCM | 145 (46.6%) | 4.5 | 1.7 (1.65–5.4) |
| Lam Dong | 8 (2.6%) | 3.3 | 3.6 (1.65–4.2) |
| Ba Ria-Vung Tau | 13 (4.2%) | 2.7 | 1.7 (1.65–3.5) |
| Other * | 21 (6.8%) | 5.3 | 4.8 (1.65–7.4) |
| Child or Family Characteristic | Mean (µg/dL) | Median (µg/dL) and IQI | p-Value * |
|---|---|---|---|
| Gender | 0.77 | ||
| Male | 5.19 | 3.70 (1.65–6.52) | |
| Female | 4.63 | 3.60 (1.65–5.80) | |
| Age (months) | <0.001 | ||
| 0–12 | 3.75 | 1.65 (1.65–3.60) | |
| 13–24 | 6.71 | 5.20 (3.63–7.60) | |
| 25–36 | 5.39 | 4.90 (1.65–7.40) | |
| 37+ | 5.70 | 5.50 (3.70–7.90) | |
| Location | 0.02 | ||
| Ho Chi Minh | 4.41 | 1.65 (1.65–5.35) | |
| All other locations | 5.43 | 3.80 (1.65–6.70) | |
| Water source | 0.12 | ||
| Piped | 4.54 | 1.65 (1.65–5.20) | |
| Bottled | 4.88 | 4.00 (1.65–6.20) | |
| Rainwater | 5.62 | 5.40 (3.28–7.95) | |
| Well water | 5.39 | 3.65 (1.65–6.68) | |
| Use traditional medicines | 5.12 | 3.80 (1.65–6.20) | 0.43 |
| Have peeling paint in the home | 4.84 | 3.50 (1.65–5.70) | 0.61 |
| Attends school outside the home | 6.54 | 5.70 (4.10–8.15) | <0.001 |
| Parents do metal recycling | 10.64 | 5.45 (4.39–14.55) | 0.12 |
| Live near a busy intersection | 5.14 | 3.60 (1.65–6.35) | 0.43 |
| Variable | Number and % of Children | Odds Ratio and 95% Confidence Interval | p-Value |
|---|---|---|---|
| Gender | |||
| Male | 67 (61%) | 1 * | |
| Female | 42 (39%) | 0.99 (0.6–1.6) | 0.99 |
| Age (months) | |||
| 0–12 | 29 (27%) | 1 | |
| 13–24 | 38 (35%) | 4.4 (2.4–8.1)) | <0.001 |
| 25–36 | 19 (17%) | 4.0 (1.9–8.4) | <0.001 |
| 37+ | 23 (21%) | 8.1 (3.6–18.1) | <0.001 |
| School outside the home | 48 (44%) | 0.2 (0.1–0.4) | <0.001 |
| Busy intersection near home | 27 (25%) | 1.3 (0.7–2.1) | 0.40 |
| Use of traditional medicine | 46 (42%) | 0.9 (0.5–1.4) | 0.54 |
| Welding | 21 (19%) | 0.8 (0.4–1.4) | 0.43 |
| Metal recycling or melting | 5 (5%) | 0.1 (0.0–0.9) | 0.04 |
| Water Source | |||
| Piped | 27 (25%) | 1 | |
| Bottled | 38 (35%) | 1.9 (1.0–3.4) | 0.05 |
| Rainwater | 6 (6%) | 5.6 (1.3–23.8) | 0.02 |
| Well | 38 (35%) | 1.6 (0.9–2.9) | 0.12 |
| Other activities ** | 6 (6%) | ** |
| Variable | Number (%) | OR (95% CI) | p-Value |
|---|---|---|---|
| Province | |||
| Ho Chi Minh | 41 (38%) | 1 * | |
| Binh Duong | 33 (30%) | 2.7 (1.4–5.6) | 0.01 |
| Binh Phuoc | 4 (4%) | 0.5 (0.1–1.8) | 0.30 |
| Dong Nai | 18 (17%) | 2.3 (1.0–5.1) | 0.05 |
| Lam Dong | 1 (1%) | 0.2 (0.0–2.3) | 0.20 |
| Ba Ria | 3 (3%) | 0.5 (0.1–2.5) | 0.39 |
| Other | 8 (7%) | 2.1 (0.7–6.2) | 0.32 |
| Water Source | |||
| Piped | 27 (25%) | 1 | |
| Bottled | 38 (35%) | 1.8 (0.9–3.3) | 0.08 |
| Rainwater | 6 (6%) | 3.6 (0.8–16.23) | 0.09 |
| Well Water | 38 (35%) | 1.5 (0.8–2.9) | 0.23 |
| Age & School | |||
| 0–12 months | 24 (22%) | 1 | |
| 13–24 months | 42 (39%) | 6.0 (3.1–11.8) | <0.001 |
| 25–36 months | |||
| Attends school | 17 (16%) | 7.5 (2.8–19.9) | <0.001 |
| Not in school | 2 (2%) | 0.9 (0.2–5.0) | 0.90 |
| >37 months | |||
| Attends school | 17 (16%) | 12.6 (4.6–34.3) | <0.001 |
| Not in school | 7 (6%) | 16.8 (3.8–74.7) | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Havens, D.; Pham, M.H.; Karr, C.J.; Daniell, W.E. Blood Lead Levels and Risk Factors for Lead Exposure in a Pediatric Population in Ho Chi Minh City, Vietnam. Int. J. Environ. Res. Public Health 2018, 15, 93. https://doi.org/10.3390/ijerph15010093
Havens D, Pham MH, Karr CJ, Daniell WE. Blood Lead Levels and Risk Factors for Lead Exposure in a Pediatric Population in Ho Chi Minh City, Vietnam. International Journal of Environmental Research and Public Health. 2018; 15(1):93. https://doi.org/10.3390/ijerph15010093
Chicago/Turabian StyleHavens, Deborah, Minh Hong Pham, Catherine J. Karr, and William E. Daniell. 2018. "Blood Lead Levels and Risk Factors for Lead Exposure in a Pediatric Population in Ho Chi Minh City, Vietnam" International Journal of Environmental Research and Public Health 15, no. 1: 93. https://doi.org/10.3390/ijerph15010093
APA StyleHavens, D., Pham, M. H., Karr, C. J., & Daniell, W. E. (2018). Blood Lead Levels and Risk Factors for Lead Exposure in a Pediatric Population in Ho Chi Minh City, Vietnam. International Journal of Environmental Research and Public Health, 15(1), 93. https://doi.org/10.3390/ijerph15010093