Estimating the Causal Impact of Proximity to Gold and Copper Mines on Respiratory Diseases in Chilean Children: An Application of Targeted Maximum Likelihood Estimation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Questionnaire
2.2. Respiratory Outcomes
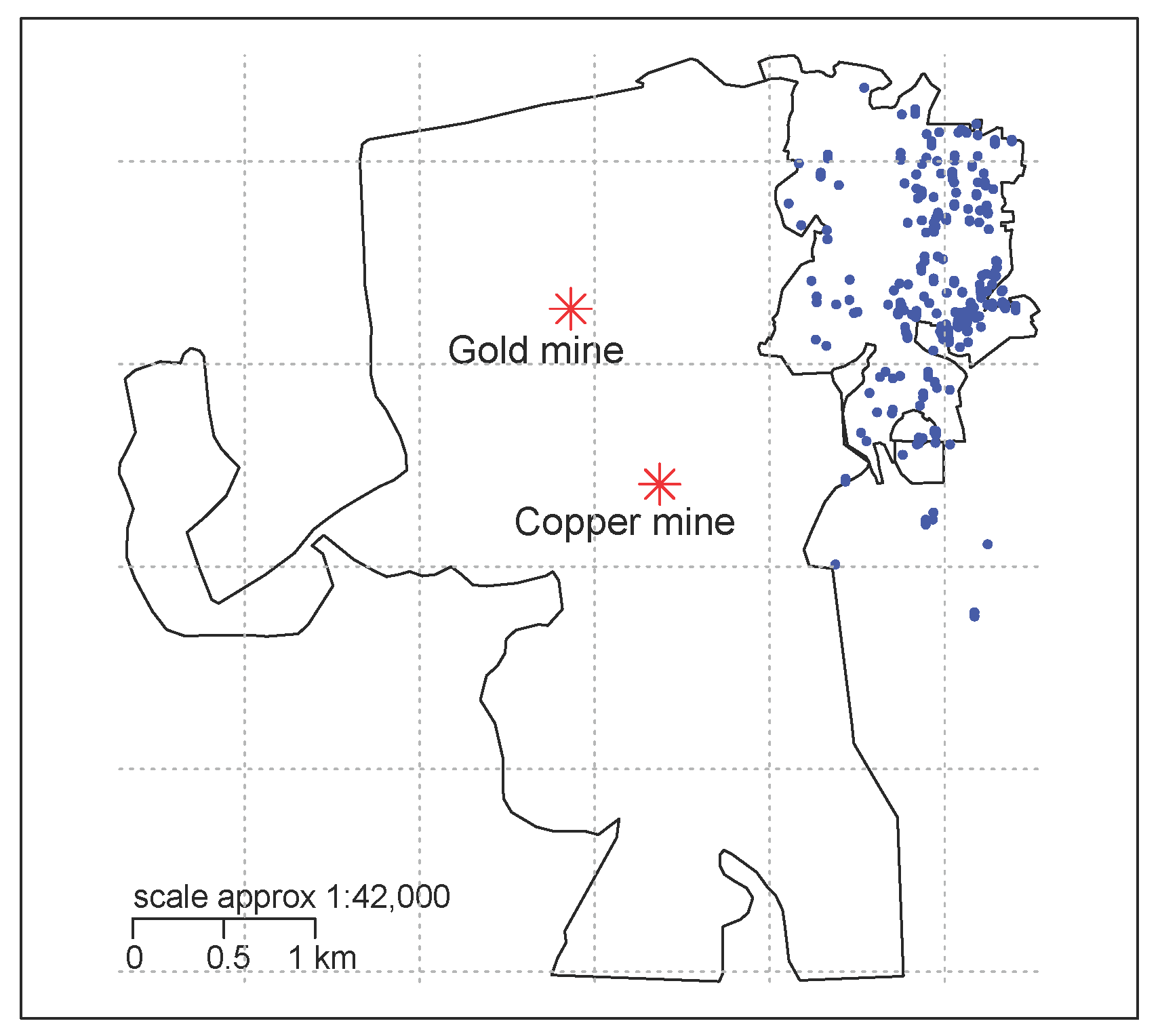
2.3. Exposure to Mines
2.4. Potential Confounders
2.5. Statistical Analysis
2.5.1. Parameters of Interest
2.5.2. Identification of the Causal Parameter
2.5.3. Estimation of Parameters of Interest
2.5.4. Missing Values
3. Results
3.1. Descriptive Results
3.2. Causal Attributable Risk
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CAR | Causal attributable risk |
| CI | Confidence interval |
| ETA | Experimental treatment assumption |
| GPS | Global positioning system |
| GP | General practitioners |
| ISAAC | International Study on Asthma and Allergies in Childhood |
| SES | Socioeconomic status |
| TMLE | Targeted maximum likelihood estimation |
Appendix A.
Tables

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Asthma a | Rhinoconjunctivitis a | Asthma or Rhinoconjunctivitis a | |||||
|---|---|---|---|---|---|---|---|
| CAR | CI | CAR | CI | CAR | CI | ||
| Gold mine | Quartile 1 (1.9 km) | −2.8% | (−6.0%; 0.3%) | −2.4% | (−5.4%; 0.6%) | −3.0% | (−6.8%; 0.2%) |
| Quartile 2 (2.3 km) | −0.4% | (−4.5%; 3.6%) | −1.2% | (−5.4%; 2.9%) | −0.3% | (−4.7%; 4.1%) | |
| Copper mine | Quartile 1 (1.6 km) | −1.3% | (−4.3%; 1.2%) | −3.6% | (−6.7%; −0.4%) | −3.2% | (−6.5%; −0.01%) |
| Quartile 2 (2.0 km) | −1.6% | (−5.7%; 2.4%) | −3.7% | (−8.0%; 0.6%) | −3.2% | (−7.6%; 1.2%) | |
| Either mine | Quartile 1 | −1.2% | (−3.7%; 1.3%) | −1.6% | (−4.0%; 0.9%) | −2.0% | (−4.5%; 0.5%) |
| Quartile 2 | 0.9% | (−3.6%; 5.4%) | −1.7% | (−6.4%; 3.0%) | 1.6% | (−3.3%; 6.6%) | |
Figures
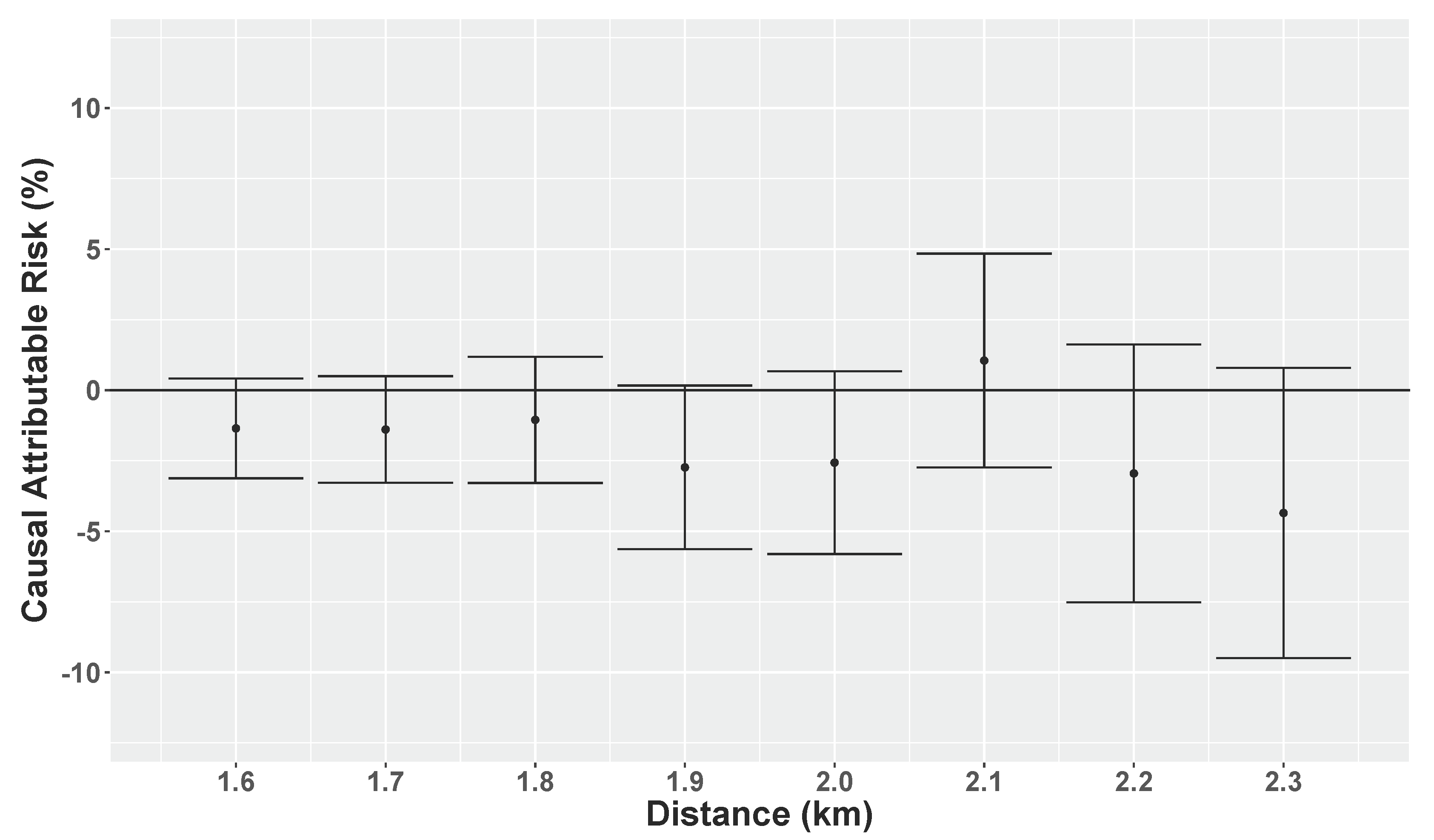
Appendix A.1. Causal Attributable Risks at Different Distances to the Gold Mine



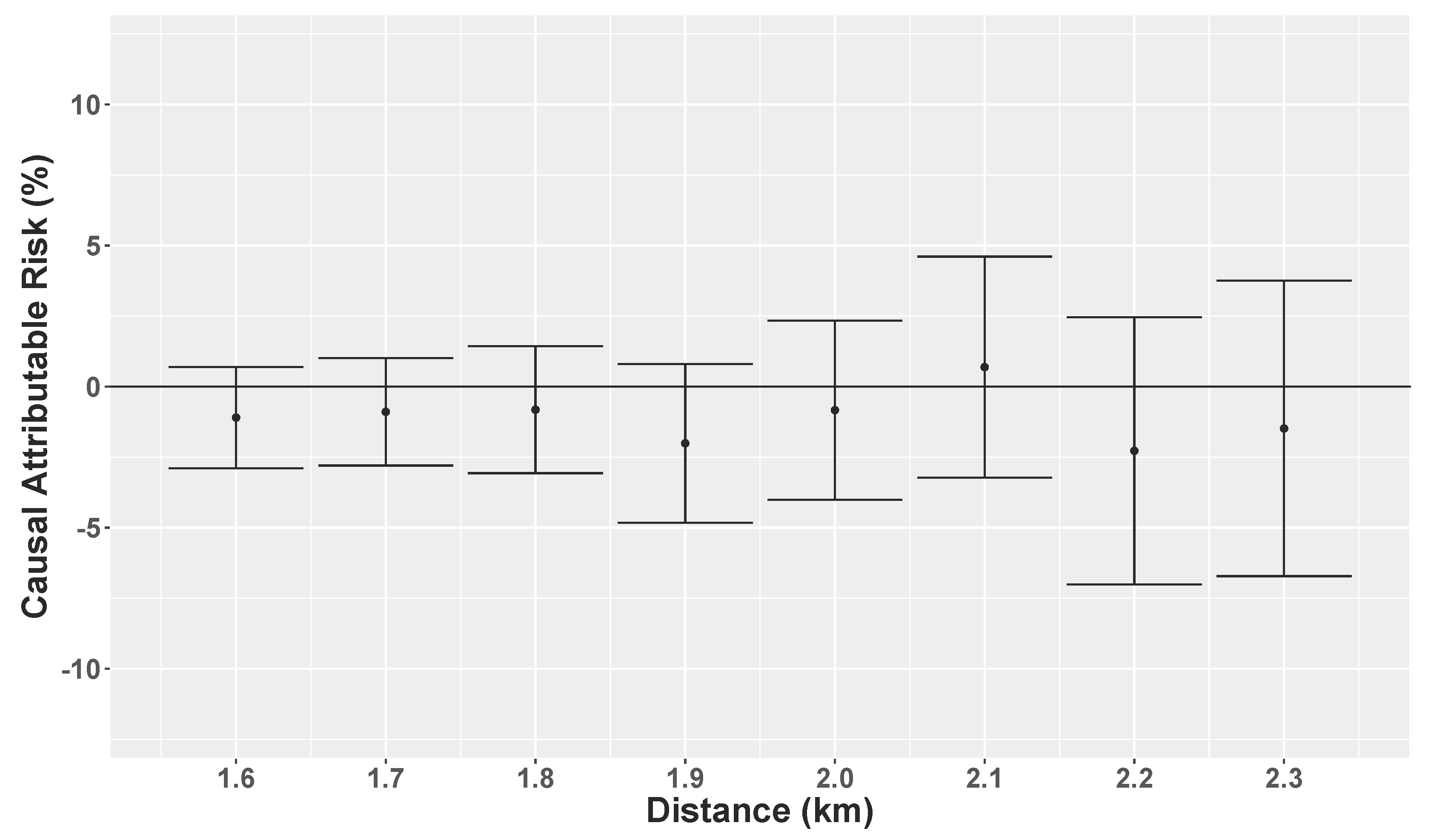
Appendix A.2. Causal Attributable Risk at Different Distances to the Copper Mine



References
- Consejo Minero Chile. Minería en Cifras. Consejo Minero: Minería en Cifras Web Report. 2015. Available online: http://www.consejominero.cl/wp-content/uploads/2015/03/Miner%C3%ADa-en-Cifras-0315.pdf (accessed on 4 February 2016).
- Eisler, R. Health Risk of Gold Miners: A Synoptic Review. Environ. Geochem. Health 2003, 25, 325–345. [Google Scholar] [CrossRef] [PubMed]
- Monjezi, M.; Shahriar, K.; Dehghani, H.; Samimi, F. Environmental Impact Assessment of Open Pit Mining in Iran. Environ. Geol. 2009, 58, 205–216. [Google Scholar] [CrossRef]
- Schwartz, J. Air pollution in Children’s Health. Pediatrics 2004, 113, 1037–1043. [Google Scholar] [PubMed]
- Vanos, J.K. Children’s Health and Vulnerability in Outdoor Microclimates: A Comprehensive Review. Environ. Int. 2015, 76, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Howel, D.; Pless-Mulloli, T.; Darnell, R. Consultations of Children Living Near Open-Cast Coal Mines. Environ. Health Perspect. 2001, 109, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Quiroz-Arcentales, L.; Hernández, L.; Agudelo, C.; Medina, K.; Robledo, R.; Osorio-García, S. Enfermedad y síntomas Respiratorios en Niños de Cinco Municipios Carboníferos del Cesar, Colombia. Rev. Salud Pública 2013, 15, 66–79. [Google Scholar] [PubMed]
- Rava, M.; Marcon, A.; Girardi, P.; Pironi, V.; Silocchi, C.; Ricci, P.; de Marco, R. Proximity to Wood Factories and Hospitalizations for Respiratory Diseases in Children. Sci. Total Environ. 2011, 410–411, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Rava, M.; Crainicianu, C.; Marcon, A.; Cazzoletti, L.; Pironi, V.; Silocchi, C.; Ricci, P.; de Marco, R. Proximity to Wood Industries and Respiratory Symptoms in Children: A Sensitivity Analysis. Environ. Int. 2012, 38, 37–44. [Google Scholar] [CrossRef] [PubMed]
- Arbex, M.A.; Martins, L.C.; de Oliveira, R.C.; Amador Pereira, L.A.; Arbex, F.F.; Cançado, J.E.D.; Saldiva, P.H.N.; Braga, A.L.F. Air Pollution from Biomass Burning and Asthma Hospital Admissions in a Sugar Cane Plantation Area in Brazil. J. Epidemiol. Community Health 2007, 61, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Milligan, P.; Brabin, B.; Kelly, Y.; Pearson, M.; Mahoney, G.; Dunne, E.; Heaf, D.; Reid, J. Association of Spatial Distribution of Childhood Respiratory Morbidity with Environmental Dust Pollution. J. Toxicol. Environ. Health Part A 1998, 55, 169–184. [Google Scholar] [PubMed]
- De Marco, R.; Marcon, A.; Rava, M.; Cazzoletti, L.; Pironi, V.; Silocchi, C.; Ricci, P. Proximity to Chipboard Industries Increases the Risk of Respiratory and Irritation Symptoms in Children: The Viadana Study. Sci. Total Environ. 2010, 408, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Loyo-Berríos, N.; Irizarry, R.; Hennessey, J.; Tao, X.; Matanoski, G. Air Pollution Sources and Childhood Asthma Attacks in Cataño, Puerto Rico. Am. J. Epidemiol. 2007, 165, 927–935. [Google Scholar] [CrossRef] [PubMed]
- Herrera, R.; Radon, K.; von Ehrenstein, O.S.; Cifuentes, S.; Muñoz, D.M.; Berger, U. Proximity to Mining Industry and Respiratory Diseases in Children in a Community in Northern Chile: A Cross-sectional Study. Environ. Health 2016, 15, 66. [Google Scholar] [CrossRef] [PubMed]
- Crawford, B.; Krayenhoff, E.S.; Cordy, P. The Urban Energy Balance of a Lightweight Low-rise Neighborhood in Andacollo, Chile. In Theoretical and Applied Climatology; Springer: Vienna, Austria, 2016; pp. 1–14. [Google Scholar]
- Clima Andacollo, 2017. Web Report. Available online: https://www.meteoblue.com/es/tiempo/pronostico/modelclimate/andacollo_chile_3899680 (accessed on 18 December 2017).
- Westreich, D. From Exposures to Population Interventions: Pregnancy and Response to HIV Therapy. Am. J. Epidemiol. 2014, 179, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Westreich, D.; Edwards, J.K.; Rogawski, E.T.; Hudgens, M.G.; Stuart, E.A.; Cole, S.R. Causal impact: Epidemiological Approaches for a Public Health of Consequence. Am. J. Public Health 2016, 106, 1011. [Google Scholar] [CrossRef] [PubMed]
- Ohlander, J.; Huber, S.M.; Schomaker, M.; Heumann, C.; Schierl, R.; Michalke, B.; Jenni, O.G.; Caflisch, J.; Muñoz, D.M.; von Ehrenstein, O.S.; et al. Risk Factors for Mercury Exposure of Children in a Rural Mining Town in Northern Chile. PLoS ONE 2013, 8, e79756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernández, C.M.; Fernández-Benítez, M.; Miranda, M.P.; Grima, F.G. Validation of the Spanish Version of the Phase III ISAAC Questionnaire on Asthma. J. Investig. Allergol. Clin. Immunol. 2005, 15, 201–210. [Google Scholar]
- Hernán, M.; Robins, J. Estimating Causal Effects from Epidemiological Data. J. Epidemiol. Community Health 2006, 60, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Van der Laan, M.; Rose, S. Targeted Learning: Causal Inference for Observational and Experimental Data; Springer: New York, NY, USA, 2011. [Google Scholar]
- Hubbard, A.; van der Laan, M. Population Intervention Models in Causal Inference. Biometrika 2008, 95, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Balzer, L.; Galea, S. The roles of Outlet Density and Norms in Alcohol Use Disorder. Drug Alcohol Depend. 2015, 151, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Carrillo, B.; Iglesias, W.; Trujillo, J. Attainments and Limitations of an Early Childhood Programme in Colombia. Health Policy Plan. 2015, 30, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, N.; Tiesman, H.; Sumitani, J.; Mize, T.; Amarnath, K.; Bayakly, A.; Murphy, M. Public Health Impact of Heat-Related Illness among Migrant Farmworkers. Am. J. Prev. Med. 2013, 44, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, N.; Fernald, L.; Hubbard, A. Estimating the Potential Impact of Intervention from Observational Data: Methods for Estimating Causal Attributable Risk in a Cross-sectional Analysis of Depressive Symptoms in Latin America. J. Epidemiol. Community Health 2010, 64, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Clasen, T.; Pruss-Ustun, A.; Mathers, C.; Cairncross, O.C.S.; Colford, J.M., Jr. Estimating the Impact of Unsafe Water, Sanitation and Hygiene on the Global Burden of Disease: Evolving and Alternative Methods. Trop. Med. Int. Health 2013, 19, 884–893. [Google Scholar] [CrossRef] [PubMed]
- Fleischer, N.; Fernald, L.; Hubbard, A. Depressive Symptoms in Low-Income Women in Rural Mexico. Epidemiology 2007, 18, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Van der Laan, M.; Polley, E.; Hubbard, A. Super Learner. Stat. Appl. Genet. Mol. Biol. 2007, 6, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Snowden, J.; Mortimer, K.; Dufour, M.; Tager, I. Population Intervention Models to Estimate Ambient NO2 Health Effects in Children with Asthma. J. Expo. Sci. Environ. Epidemiol. 2015, 25, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Hubbard, A.; Galea, S. Estimating the Effects of Potential Public Health Interventions on Population Disease Burden: A Step-by-Step Illustration of Causal Inference Methods. Am. J. Epidemiol. 2008, 169, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Schuler, M.S.; Rose, S. Targeted Maximum Likelihood Estimation for Causal Inference in Observational Studies. Am. J. Epidemiol. 2017, 185, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.J.; Rose, S.; Khan, J.A.; Ahmed, S.; Peters, D.H.; Niessen, L.W.; Trujillo, A.J. The Relationship Between Non-communicable Disease Occurrence and Poverty—Evidence from Demographic Surveillance in Matlab, Bangladesh. Health Policy Plan. 2016, 31, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Van Buuren, S.; Groothuis-Oudshoorn, K. mice: Multivariate Imputation by Chained Equations in R. J. Stat. Softw. 2011, 45, 1–67. [Google Scholar] [CrossRef]
- Rubin, D. Multiple Imputation for Nonresponse in Surveys; John Wiley & Sons: Hoboken, NJ, USA, 1987. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2017. [Google Scholar]
- Gruber, S.; van der Laan, M.J. tmle: An R Package for Targeted Maximum Likelihood Estimation. J. Stat. Softw. 2012, 51, 1–35. [Google Scholar] [CrossRef]
- Polley, E.; van der Laan, M. SuperLearner: Super Learner Prediction; R Package Version 2.0-15; CRAN: Viena, Austria, 2014. [Google Scholar]
- Ahern, J.; Margerison-Zilko, C.; Hubbard, A.; Galea, S. Alcohol Outlets and Binge Drinking in Urban Neighborhoods: The Implications of Nonlinearity for Intervention and Policy. Am. J. Public Health 2013, 103, e81–e87. [Google Scholar] [CrossRef] [PubMed]
- Salvi, S. Health effects of ambient air pollution in children. Paediatr. Respir. Rev. 2007, 8, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Westreich, D. From Patients to Policy: Population Intervention Effects in Epidemiology. Epidemiology 2017, 28, 525. [Google Scholar] [CrossRef] [PubMed]
- Ahern, J.; Hubbard, A. A Roadmap for Estimating and Interpreting Population Intervention Parameters. In Methods in Social Epidemiology; John Wiley & Sons: San Francisco, CA, USA, 2017; pp. 432–457. [Google Scholar]
- Roberts, E. Does Your Child Have Asthma? Parent Reports and Medication Use for Pediatric Asthma. Arch. Pediatr. Adolesc. Med. 2003, 157, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Porter, K.; Gruber, S.; van der Laan, M.; Sekhon, J.S. The Relative Performance of Targeted Maximum Likelihood Estimators. Int. J. Biostat. 2011, 7, 31. [Google Scholar] [CrossRef] [PubMed]
- Petersen, M.; Porter, K.; Gruber, S.; Wang, Y.; van der Laan MJ, M. Diagnosing and Responding to Violations in the Positivity Assumption. Stat. Methods Med. Res. 2012, 21, 31–54. [Google Scholar] [CrossRef] [PubMed]

| Distance to | Gold Mine > Quartile 1 | Copper Mine > Quartile 1 | Either Mine > Quartile 1 | ||||
|---|---|---|---|---|---|---|---|
| Total n per Category | % | (n) | % | (n) | % | (n) | |
| Sex | |||||||
| Female | (126) | 75 | (94) | 75 | (94) | 75 | (94) |
| Male | (149) | 75 | (112) | 75 | (112) | 74 | (111) |
| Age | |||||||
| 6–7 years | (74) | 77 | (57) | 76 | (56) | 77 | (57) |
| 8–9 years | (86) | 74 | (64) | 76 | (65) | 76 | (65) |
| 10–11 years | (82) | 70 | (57) | 72 | (59) | 70 | (57) |
| ≥12 years | (33) | 85 | (28) | 79 | (26) | 79 | (26) |
| Living with both parents (NA = 9) | |||||||
| No | (81) | 72 | (58) | 68 | (55) | 70 | (57) |
| Yes | (185) | 76 | (140) | 78 | (144) | 76 | (141) |
| Parental atopic disease (NA = 30) | |||||||
| No | (160) | 77 | (123) | 77 | (123) | 76 | (122) |
| Yes | (85) | 73 | (62) | 76 | (65) | 76 | (65) |
| Mother working (NA = 15) | |||||||
| No | (191) | 76 | (146) | 74 | (142) | 74 | (142) |
| Yes | (69) | 70 | (48) | 78 | (54) | 75 | (52) |
| Father working (NA = 22) | |||||||
| No | (22) | 68 | (15) | 64 | (14) | 54 | (12) |
| Yes | (231) | 78 | (181) | 78 | (181) | 79 | (182) |
| Hours child stay at home (NA = 61) | |||||||
| Less 3 h | (20) | 95 | (19) | 85 | (17) | 85 | (17) |
| 3–6 h | (46) | 74 | (34) | 72 | (33) | 74 | (34) |
| More than 6 h | (148) | 71 | (105) | 76 | (112) | 73 | (108) |
| Place child play most of the time (NA = 9) | |||||||
| Inside | (105) | 77 | (81) | 75 | (79) | 78 | (82) |
| Outside | (161) | 73 | (118) | 75 | (120) | 72 | (116) |
| Smoking in child’s presence (NA = 28) | |||||||
| No | (180) | 77 | (139) | 73 | (132) | 74 | (134) |
| Yes | (67) | 69 | (46) | 81 | (54) | 76 | (51) |
| Nearest road (NA = 10) | |||||||
| Dirt | (57) | 67 | (38) | 60 | (34) | 58 | (33) |
| Paved | (208) | 77 | (160) | 79 | (164) | 79 | (164) |
| Type of heater (NA = 69) | |||||||
| Other | (80) | 78 | (62) | 78 | (62) | 76 | (61) |
| Coal and Gas | (126) | 73 | (92) | 72 | (91) | 73 | (92) |
| Distance to | Asthma | Rhinoconjunctivitis | Asthma or Rhinoconjunctivitis | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall Prevalence | () | () | () | ||||||||
| Missing Data | (NA = 35) | (NA = 17) | (NA = 26) | ||||||||
| Total n per Category | % | (n) | OR (95% CI) | % | (n) | OR (95% CI) | % | (n) | OR (95% CI) | ||
| Gold mine | |||||||||||
| Quartile 1 (1.9 km) | ≤ | (69) | 32 | (22) | 1.67 (0.89; 3.11) | 41 | (28) | 1.54 (0.86; 2.75) | 52 | (36) | 1.58 (0.89; 2.84) |
| > | (206) | 21 | (44) | 1 | 32 | (65) | 1 | 41 | (85) | 1 | |
| Quartile 2 (2.3 km) | ≤ | (138) | 24 | (34) | 1.01 (0.58; 1.79) | 35 | (48) | 1.08 (0.65; 1.80) | 44 | (61) | 0.99 (0.60; 1.62) |
| > | (137) | 23 | (32) | 1 | 33 | (45) | 1 | 44 | (60) | 1 | |
| Copper mine | |||||||||||
| Quartile 1 (1.6 km) | ≤ | (69) | 30 | (21) | 1.47 (0.78; 2.72) | 45 | (31) | 1.79 (1.01; 3.16) | 57 | (39) | 1.70 (0.97; 3.01) |
| > | (206) | 22 | (45) | 1 | 30 | (62) | 1 | 39 | (82) | 1 | |
| Quartile 2 (2.0 km) | ≤ | (138) | 25 | (35) | 1.18 (0.67; 2.09) | 38 | (52) | 1.38 (0.83; 2.31) | 47 | (65) | 1.27 (0.78; 2.10) |
| > | (137) | 23 | (31) | 1 | 30 | (41) | 1 | 41 | (56) | 1 | |
| Both mines | |||||||||||
| Quartile 1 | ≤ | (96) | 30 | (29) | 1.61 (0.90; 2.87) | 43 | (41) | 1.81 (1.07; 3.08) | 53 | (51) | 1.66 (0.99; 2.81) |
| ≥ | (179) | 20 | (37) | 1 | 30 | (52) | 1 | 40 | (70) | 1 | |
| Quartile 2 | ≤ | (101) | 24 | (41) | 0.79 (0.44; 1.41) | 35 | (61) | 0.75 (0.45; 1.27) | 44 | (76) | 0.74 (0.44; 1.24) |
| > | (174) | 25 | (25) | 1 | 32 | (32) | 1 | 45 | (45) | 1 | |
| Asthma a | Rhinoconjunctivitis a | Asthma or Rhinoconjunctivitis a | |||||
|---|---|---|---|---|---|---|---|
| CAR | CI | CAR | CI | CAR | CI | ||
| Gold mine | Quartile 1 (1.9 km) | % | (%; 0.3%) | % | (%; 0.8%) | 2.7% | (%; 0.2%) |
| Quartile 2 (2.3 km) | % | (%; 0.8%) | % | (%; 3.4%) | 3.7% | (%; 1.9%) | |
| Copper mine | Quartile 1 (1.6 km) | % | (%; 1.6%) | % | (%; %) | % | (%;%) |
| Quartile 2 (2.0 km) | % | (%; 2.9%) | % | (%; 2.9%) | % | (%; 3.1%) | |
| Either mine | Quartile 1 | % | (%; 0.1%) | % | (%; %) | % | (%; %) |
| Quartile 2 | 0.5% | (%; 5.0%) | % | (%; 2.7%) | 0.7% | (C%; 5.6%) | |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herrera, R.; Berger, U.; Von Ehrenstein, O.S.; Díaz, I.; Huber, S.; Moraga Muñoz, D.; Radon, K. Estimating the Causal Impact of Proximity to Gold and Copper Mines on Respiratory Diseases in Chilean Children: An Application of Targeted Maximum Likelihood Estimation. Int. J. Environ. Res. Public Health 2018, 15, 39. https://doi.org/10.3390/ijerph15010039
Herrera R, Berger U, Von Ehrenstein OS, Díaz I, Huber S, Moraga Muñoz D, Radon K. Estimating the Causal Impact of Proximity to Gold and Copper Mines on Respiratory Diseases in Chilean Children: An Application of Targeted Maximum Likelihood Estimation. International Journal of Environmental Research and Public Health. 2018; 15(1):39. https://doi.org/10.3390/ijerph15010039
Chicago/Turabian StyleHerrera, Ronald, Ursula Berger, Ondine S. Von Ehrenstein, Iván Díaz, Stella Huber, Daniel Moraga Muñoz, and Katja Radon. 2018. "Estimating the Causal Impact of Proximity to Gold and Copper Mines on Respiratory Diseases in Chilean Children: An Application of Targeted Maximum Likelihood Estimation" International Journal of Environmental Research and Public Health 15, no. 1: 39. https://doi.org/10.3390/ijerph15010039
APA StyleHerrera, R., Berger, U., Von Ehrenstein, O. S., Díaz, I., Huber, S., Moraga Muñoz, D., & Radon, K. (2018). Estimating the Causal Impact of Proximity to Gold and Copper Mines on Respiratory Diseases in Chilean Children: An Application of Targeted Maximum Likelihood Estimation. International Journal of Environmental Research and Public Health, 15(1), 39. https://doi.org/10.3390/ijerph15010039