Potential Diagnostic Properties of Chest Ultrasound in Thoracic Tuberculosis—A Systematic Review

 ,
, 
 , ,
, ,
Abstract
:1. Introduction
2. Methods
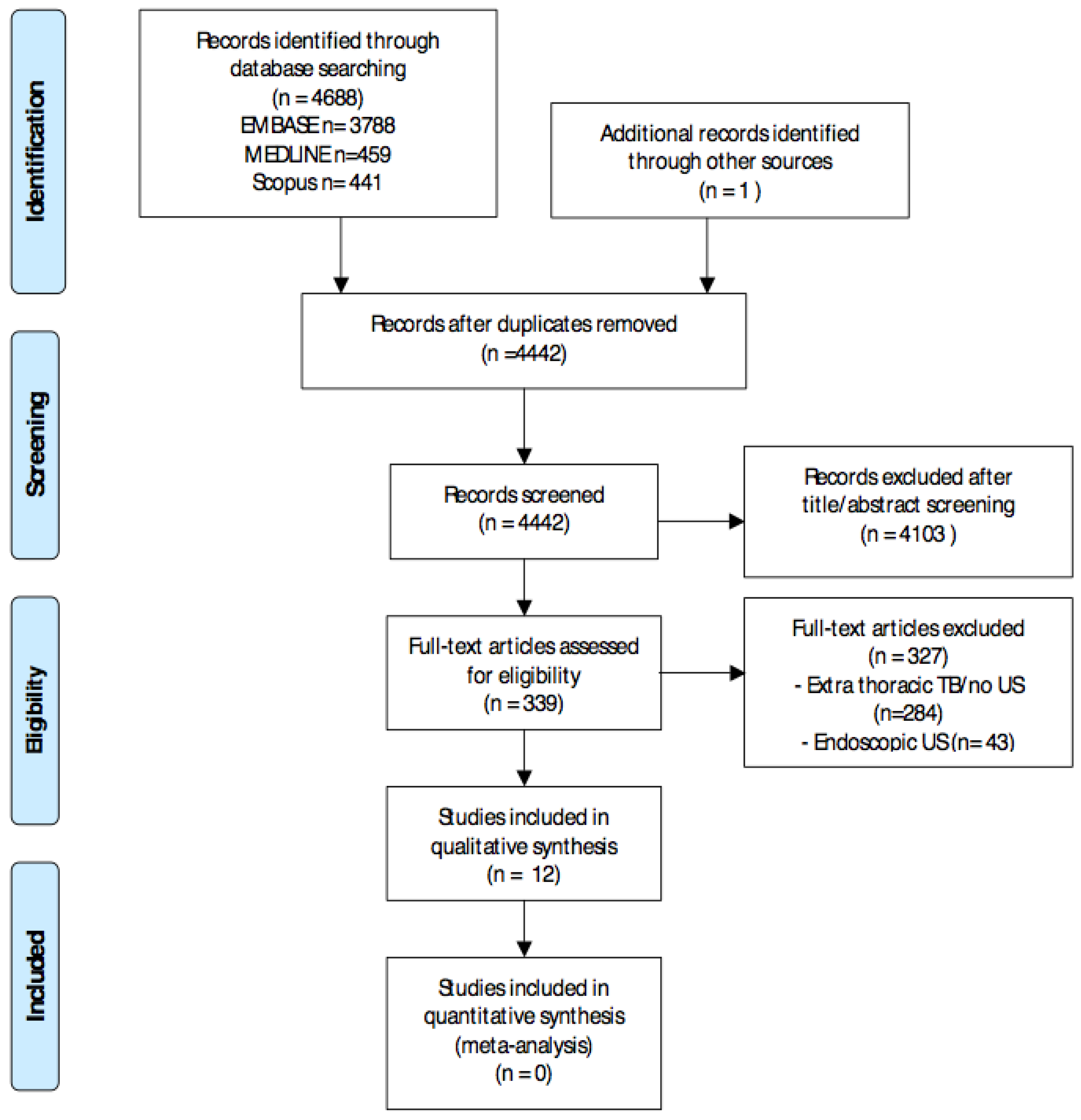
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analysis
3. Results
3.1. Study and Patient Characteristics
3.2. Main Findings
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CUS | chest ultrasound |
| TB | tuberculosis |
References
- World Health Organization. Global Tuberculosis Report 2016; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Global Strategy and Targets for Tuberculosis Prevention, Care and Control after 2015; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Sulis, G.; Centis, R.; Sotgiu, G.; D’Ambrosio, L.; Pontali, E.; Spanevello, A.; Matteelli, A.; Zumla, A.; Migliori, G.B. Recent developments in the diagnosis and management of tuberculosis. NPJ Prim. Care Respir. Med. 2016, 26, 16078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pai, M.; Behr, M.A.; Dowdy, D.; Dheda, K.; Divangahi, M.; Boehme, C.C.; Ginsberg, A.; Swaminathan, S.; Spigelman, M.; Getahun, H.; et al. Tuberculosis. Nat. Rev. Dis. Prim. 2016, 2, 16076. [Google Scholar] [CrossRef] [PubMed]
- Becker, D.M.; Tafoya, C.A.; Becker, S.L.; Kruger, G.H.; Tafoya, M.J.; Becker, T.K. The use of portable ultrasound devices in low- and middle-income countries: A systematic review of the literature. Trop. Med. Int. Health 2016, 21, 294–311. [Google Scholar] [CrossRef] [PubMed]
- Volpicelli, G.; Elbarbary, M.; Blaivas, M.; Lichtenstein, D.A.; Mathis, G.; Kirkpatrick, A.W.; Melniker, L.; Gargani, L.; Noble, V.E.; Via, G.; et al. International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012, 38, 577–591. [Google Scholar] [CrossRef] [PubMed]
- Heller, T.; Wallrauch, C.; Goblirsch, S.; Brunetti, E. Focused assessment with sonography for HIV-associated tuberculosis (FASH): A short protocol and a pictorial review. Crit. Ultrasound J. 2012, 4, 21. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Weswood, M.E.; Rutjes, A.W.S.; Reitsma, J.B.; Bossuyt, P.N.; Kleijnen, J. Evaluation of QUADAS, a tool for the quality assessment of diagnostic accuracy studies. BMC Med. Res. Methodol. 2006, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Carazo Martínez, O.; Vargas Serrano, B.; Rodríguez Romero, R. Real-time ultrasound evaluation of tuberculous pleural effusions. J. Clin. Ultrasound 1989, 17, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Akhan, O.; Demirkazik, F.B.; Ozmen, M.N.; Balkanci, F.; Ozkara, S.; Cöplü, L.; Emri, A.; Besim, A. Tuberculous pleural effusions: Ultrasonic diagnosis. J. Clin. Ultrasound 1992, 20, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Yuan, A.; Yang, P.C.; Chang, D.B.; Yu, C.J.; Lee, L.N.; Wu, H.D.; Kuo, S.H.; Luh, K.T. Ultrasound guided aspiration biopsy for pulmonary tuberculosis with unusual radiographic appearances. Thorax 1993, 48, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Gulati, M.; Venkataramu, N.; Gupta, S.; Sood, B.P.; Sheena, D.M.; Gupta, S.K.; Suri, S. Ultrasound guided fine needle aspiration biopsy in mediastinal tuberculosis. Int. J. Tuberc. Lung Dis. 2000, 4, 1164–1168. [Google Scholar] [PubMed]
- Bosch-Marcet, J.; Serres-Créixams, X.; Borrás-Pérez, V.; Coll-Sibina, M.T.; Guitet-Juliá, M.; Coll-Rosell, E. Value of sonography for follow-up of mediastinal lymphadenopathy in children with tuberculosis. J. Clin. Ultrasound 2007, 35, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Moseme, T.; Andronikou, S. Through the eye of the suprasternal notch: Point-of-care sonography for tuberculous mediastinal lymphadenopathy in children. Pediatr. Radiol. 2014, 44, 681–684. [Google Scholar] [CrossRef] [PubMed]
- Ahuja, V.; Gombar, S.; Kumar, N.; Goyal, N.; Gupta, K. Pregnancy with bilateral tubercular pleural effusion: Challenges. Trop. Doct. 2014, 44, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Bahr, H.M.; El-Shafey, M.; Hantera, M.S.; Abo-El magd, G.H.; El-Batsh, A.H. Ultrasound guided needle pleural biopsy in patients with undiagnosed pleural effusion. Egypt J. Chest Dis. Tuberc. 2014, 63, 113–118. [Google Scholar] [CrossRef]
- Hunter, L.; Bélard, S.; Janssen, S.; van Hoving, D.J.; Heller, T. Miliary tuberculosis: Sonographic pattern in chest ultrasound. Infection 2016, 44, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Heuvelings, C.C.; Bélard, S.; Janssen, S.; Wallrauch, C.; Grobusch, M.P.; Brunetti, E.; Giordani, M.T.; Heller, T. Chest ultrasonography in patients with HIV: A case series and review of the literature. Infection 2016, 44, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lai, Y.F.; Su, M.C.; Weng, H.H.; Wu, J.T.; Chiu, C.T. Sonographic septation: A predictor of sequelae of tuberculous pleurisy after treatment. Thorax 2009, 64, 806–809. [Google Scholar] [CrossRef] [PubMed]
- Bosch-Marcet, J.; Serres-Créixams, X.; Zuasnabar-Cotro, A.; Codina-Puig, X.; Català-Puigbó, M.; Simon-Riazuelo, J.L. Comparison of ultrasound with plain radiography and CT for the detection of mediastinal lymphadenopathy in children with tuberculosis. Pediatr. Radiol. 2004, 34, 895–900. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, L.; Parlatano, D.; Boccuzzi, F.; Onoscuri, M.; Volpicelli, G.; Veltri, A. The imaging spectrum of pulmonary tuberculosis. Acta Radiol. 2015, 56, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Reissig, A.; Copetti, R.; Mathis, G.; Mempel, C.; Schuler, A.; Zechner, P.; Aliberti, S.; Neumann, R.; Kroegel, C.; Hoyer, H. Lung ultrasound in the diagnosis and follow-up of community-acquired pneumonia: A prospective, multicenter, diagnostic accuracy study. Chest 2012, 142, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Berlet, T. Thoracic ultrasound for the diagnosis of pneumonia in adults: A meta-analysis. Respir. Res. 2015, 16, 89. [Google Scholar] [CrossRef] [PubMed]
- Sippel, S.; Muruganandan, K.; Levine, A.; Shah, S. Review article: Use of ultrasound in the developing world. Int J. Emerg. Med. 2011, 4, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Binkowski, A.; Riguzzi, C.; Price, D.; Fahimi, J. Evaluation of a cornstarch-based ultrasound gel alternative for low-resource settings. J. Emerg. Med. 2014, 47, e5–e9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Country | Study Design | N of Participants | Mean Age | Percentage of Females | Diagnostic Criteria for TBC | Final Diagnosis Made | Details of Ultrasound Procedure | Site of Investigation |
|---|---|---|---|---|---|---|---|---|---|
| Martinez, 1989 [10] | Spain | Case series | 21 | 22.5 | 57 | Microbiological | TB pleurisy | identification of effusion | Hemi-thoraxes |
| Akhan, 1992 [11] | Turkey | Case series | 20 | 30.5 | 35 | Pleural fluid analysis positive for MT | TB pleurisy | identification of effusion | Hemi-thoraxes and pleural line |
| Yuan, 1993 [12] | China | Case series | 13 | 53.5 | NA | Culture of MT | Pulmonary TB | percutaneous US-guided biopsy | Lung lesions |
| Gulati, 2000 [13] | India | Case series | 26 | 35.0 | 31 | Composite§ | TB-lymphoadenopathy | percutaneous US-guided FNAB | Mediastinum |
| Bosch-Marcet, 2004 [21] | Spain | Retrospective | 32 | 6 | 47 | Chest radiography/CT | TB-lymphoadenopathy | identification of lymphoadenopathy | Mediastinum |
| Bosch-Marcet, 2007 [14] | Spain | Retrospective | 57 | 6 | NA | Chest radiography | TB-lymphoadenopathy | identification of lymphoadenopathy | Mediastinum |
| Moseme, 2014 [15] | South Africa | Pilot study | 30 | 6 | NA | Not specified | TB-lymphoadenopathy | identification of lymphoadenopathy | Mediastinum |
| Ahuja, 2014 [16] | India | Case report | 1 | 27 | 100 | Culture of MT | TB pleurisy | identification of effusion | Hemi-thoraxes |
| Bahr, 2014 [17] | Egypt | Case series | 2 | NA | NA | Biopsy positive for TB | Pulmonary and TB pleurisy | percutaneous US-guided biopsy | Hemi-thoraxes and Lung lesions |
| Hunter, 2016 [18] | South Africa | Case series | 10 | 33 | 50 | Sputum positive | Pulmonary TB | Lung US | Lung |
| Heuvelings, 2016 [19] | Netherlands | Case report | 1 | 44 | 0 | Chest radiography/ Bal positive for MT | Pulmonary TB | Lung US | Lung |
| Lai, 2016 [20] | China | Prospective study | 87 | 64.2 | 32 | Pleural fluid analysis positive for MT | TB pleurisy | identification of pleural effusion and RPT | Hemi-thoraxes |
| Author, Year | Sensitivity of US Procedure * | Main Findings |
|---|---|---|
| Martinez, 1989 [10] | Not applicable | First study to propose ultrasound as a useful method for characterizing TB-related pleural effusion. US revealed winding or filiform structures in all patients associated with exudates having high fibrin and protein content. |
| Akhan, 1992 [11] | Not applicable | 90% of patients with TB-related effusion demonstrated regular pleural thickening (1–13 mm). A total of 30% had pleural nodules and 90% of the effusions presented delicate, complete septations. |
| Yuan, 1993 [12] | 90% | US-guided aspiration biopsy provided the diagnosis in 9 out of 10 patients. US findings of pulmonary TB with unusual radiographic appearances were even more diverse than the plain radiographs had depicted. While the US findings of hypo-, iso-, or hyperechoic consolidations and fluid bronchograms were not specific for pulmonary tuberculosis, US indicated the most appropriate area for aspiration. |
| Gulati, 2000 [13] | 76% | A total of 20 out of 26 patients with mediastinal tuberculosis could be diagnosed by guided FNAB. No procedure-related complications were recorded. US-guided FNAB was falsely negative in 6 patients. |
| Bosch-Marcet, 2004 [21] | 90.5% | US showed lymphoadenopathy in 67% of children with a normal chest radiograph and in 90.5% of children with chest radiographic images, compatible with TB. |
| Bosch-Marcet, 2007 [14] | Not applicable | US examination detected mediastinal lymphadenopathy in all children and a reduction in volume, after 3 months of treatment in 80.9% of children. Mediastinal sonography appears to have been a valuable tool for the diagnosis of TB and in the monitoring of response to treatment, in children. |
| Moseme, 2014 [15] | 40% | Pilot feasibility study showing how mediastinal sonography could detect mediastinal lymphadenopathy in 12 out of 30 children with suspected primary TB. Care was warranted with the deeper aorto-pulmonary zones, as they were harder to visualize. |
| Ahuja, 2014 [16] | Not applicable | A bedside lung US was the key factor in the early diagnosis of pleural effusion and subsequent patient management. |
| Bahr, 2014 [17] | Not applicable | In patients with undiagnosed pleural effusion, US-guided pleural biopsies aided in the differential diagnosis of 80% of cases, indicating a tuberculous effusion in 2 out of 30 patients (6.7%). |
| Hunter, 2016 [18] | Not applicable | Interstitial pattern with B-lines disseminated in multiple lung areas and a pattern of bilateral, diffuse sub-pleural granularity as typical changes seen in lungs of all patients with miliary TB. |
| Heuvelings, 2016 [19] | Not applicable | Lung ultrasound on a single patient revealed a subpleural consolidation with “shred signs,” compatible with infiltrative TB disease. |
| Lai, 2016 [20] | Not applicable | A complex, septated sonographic pattern was a useful sign to predict the development of residual pleural thickening, 1 year after the start of anti-TB treatment (PPV 84%, NPV 94%). |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Gennaro, F.; Pisani, L.; Veronese, N.; Pizzol, D.; Lippolis, V.; Saracino, A.; Monno, L.; Huson, M.A.M.; Copetti, R.; Putoto, G.; et al. Potential Diagnostic Properties of Chest Ultrasound in Thoracic Tuberculosis—A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 2235. https://doi.org/10.3390/ijerph15102235
Di Gennaro F, Pisani L, Veronese N, Pizzol D, Lippolis V, Saracino A, Monno L, Huson MAM, Copetti R, Putoto G, et al. Potential Diagnostic Properties of Chest Ultrasound in Thoracic Tuberculosis—A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(10):2235. https://doi.org/10.3390/ijerph15102235
Chicago/Turabian StyleDi Gennaro, Francesco, Luigi Pisani, Nicola Veronese, Damiano Pizzol, Valeria Lippolis, Annalisa Saracino, Laura Monno, Michaëla A.M. Huson, Roberto Copetti, Giovanni Putoto, and et al. 2018. "Potential Diagnostic Properties of Chest Ultrasound in Thoracic Tuberculosis—A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 10: 2235. https://doi.org/10.3390/ijerph15102235
APA StyleDi Gennaro, F., Pisani, L., Veronese, N., Pizzol, D., Lippolis, V., Saracino, A., Monno, L., Huson, M. A. M., Copetti, R., Putoto, G., & Schultz, M. J. (2018). Potential Diagnostic Properties of Chest Ultrasound in Thoracic Tuberculosis—A Systematic Review. International Journal of Environmental Research and Public Health, 15(10), 2235. https://doi.org/10.3390/ijerph15102235