Risk, Severity, and Predictors of Obstructive Sleep Apnea in Hemodialysis and Peritoneal Dialysis Patients

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Database, Validation, and Ethics Statement
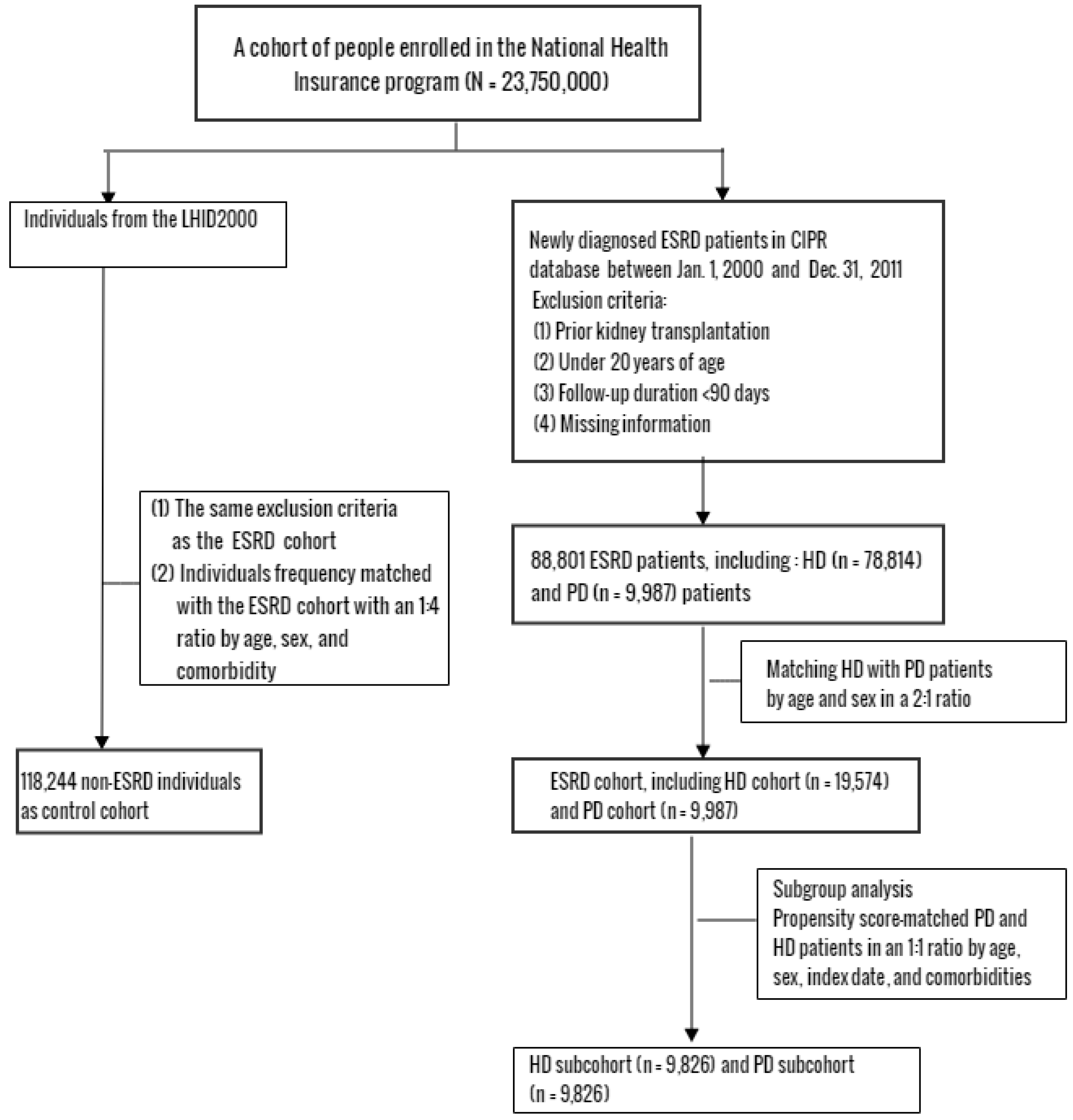
2.2. Study Design and Participants
2.3. Outcome Measurement
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Pathogenesis of OSA in Dialysis Patients
4.2. Dialysis Modalities: PD versus HD
4.3. OSA Treatment and Impact on Survival in Dialysis Patients
4.4. Study Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Bradley, T.D.; Floras, J.S. Obstructive sleep apnoea and its cardiovascular consequences. Lancet 2009, 373, 82–93. [Google Scholar] [CrossRef]
- Gottlieb, D.J.; Yenokyan, G.; Newman, A.B.; O’connor, G.T.; Punjabi, N.M.; Quan, S.F.; Redline, S.; Resnick, H.E.; Tong, E.K.; Diener-West, M.; et al. Prospective study of obstructive sleep apnea and incident coronary heart disease and heart failure: The sleep heart health study. Circulation 2010, 122, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Redline, S.; Yenokyan, G.; Gottlieb, D.J.; Shahar, E.; O’connor, G.T.; Resnick, H.E.; Diener-West, M.; Sanders, M.H.; Wolf, P.A.; Geraghty, E.M.; et al. Obstructive sleep apnea-hypopnea and incident stroke: The sleep heart health study. Am. J. Respir. Crit. Care Med. 2010, 182, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Walia, H.K.; Li, H.; Rueschman, M.; Bhatt, D.L.; Patel, S.R.; Quan, S.F.; Gottlieb, D.J.; Punjabi, N.M.; Redline, S.; Mehra, R. Association of severe obstructive sleep apnea and elevated blood pressure despite antihypertensive medication use. J. Clin. Sleep Med. 2014, 10, 835–843. [Google Scholar] [CrossRef] [PubMed]
- Marrone, O.; Battaglia, S.; Steiropoulos, P.; Basoglu, O.K.; Kvamme, J.A.; Ryan, S.; Pepin, J.L.; Verbraecken, J.; Grote, L.; Hedner, J.; et al. Chronic kidney disease in European patients with obstructive sleep apnea: The ESADA cohort study. J. Sleep Res. 2016, 25, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Forni Ogna, V.; Ogna, A.; Pruijm, M.; Bassi, I.; Zuercher, E.; Halabi, G.; Phan, O.; Bullani, R.; Teta, D.; Gauthier, T.; et al. Prevalence and diagnostic approach to sleep apnea in hemodialysis patients: A population study. Biomed. Res. Int. 2015, 2015, 103686. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.C.; Lai, K.N. Sleep disturbances and sleep apnea in patients on chronic peritoneal dialysis. J. Nephrol. 2009, 22, 318–325. [Google Scholar] [PubMed]
- Lin, Y.S.; Liu, P.H.; Lin, S.W.; Chuang, L.P.; Ho, W.J.; Chou, Y.T.; Juan, K.C.; Lo, M.T.; Chu, P.H.; Chen, N.H. Simple obstructive sleep apnea patients without hypertension or diabetes accelerate kidney dysfunction: A population follow-up cohort study from Taiwan. Sleep Breath. 2017, 21, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Lanis, A.; Kerns, E.; Hu, S.L.; Bublitz, M.H.; Risica, P.; Martin, S.; Parker, J.; Millman, R.; Dworkin, L.D.; Bourjeily, G. Residual renal function affects severity of sleep apnea in peritoneal dialysis: A pilot study. Lung 2018, 196, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Abuyassin, B.; Sharma, K.; Ayas, N.T.; Laher, I. Obstructive Sleep Apnea and Kidney Disease: A Potential Bidirectional Relationship? J. Clin. Sleep Med. 2015, 11, 915–924. [Google Scholar] [CrossRef] [PubMed]
- Sakaguchi, Y.; Shoji, T.; Kawabata, H.; Niihata, K.; Suzuki, A.; Kaneko, T.; Okada, N.; Isaka, Y.; Rakugi, H.; Tsubakihara, Y. High prevalence of obstructive sleep apnea and its association with renal function among nondialysis chronic kidney disease patients in Japan: A cross-sectional study. Clin. J. Am. Soc. Nephrol. 2011, 6, 995–1000. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.M.; Chan, C.T.; Paul, N.; Motwani, S.S.; Kasai, T.; Gabriel, J.M.; Spiller, N.; Bradley, T.D. Relationship of pharyngeal water content and jugular volume with severity of obstructive sleep apnea in renal failure. Nephrol. Dial. Transplant. 2013, 28, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.C.; Lai, K.N. Tired but can’t sleep. Perit. Dial. Int. 2007, 27, 647–650. [Google Scholar] [PubMed]
- Yang, J.Y.; Huang, J.W.; Peng, Y.S.; Chiang, S.S.; Yang, C.S.; Yang, C.C.; Chen, H.W.; Wu, M.S.; Wu, K.D.; Tsai, T.J.; et al. Quality of sleep and psychosocial factors for patients undergoing peritoneal dialysis. Perit. Dial. Int. 2007, 27, 675–680. [Google Scholar] [PubMed]
- dos Reis Santos, I.; Danaga, A.R.; de Carvalho Aguiar, I.; Oliveira, E.F.; Dias, I.S.; Urbano, J.J.; Martins, A.A.; Ferraz, L.M.; Fonsêca, N.T.; Fernandes, V.; et al. Cardiovascular risk and mortality in end-stage renal disease patients undergoing dialysis: Sleep study, pulmonary function, respiratory mechanics, upper airway collapsibility, autonomic nervous activity, depression, anxiety, stress and quality of life: A prospective, double blind, randomized controlled clinical trial. BMC Nephrol. 2013, 14, 215. [Google Scholar]
- Cheng, C.L.; Kao, Y.H.; Lin, S.J.; Lee, C.H.; Lai, M.L. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol. Drug Saf. 2011, 20, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Wu, V.C.; Wang, C.Y.; Shiao, C.C.; Chang, C.H.; Huang, H.Y. National Taiwan University Study Group on Acute Renal Failure; Taiwan Anti-Mycobacteria Investigation Group. Increased risk of active tuberculosis following acute kidney injury: A nationwide, population-based study. PLoS ONE 2013, 25, e69556. [Google Scholar]
- Su, V.Y.; Liu, C.J.; Wang, H.K.; Wu, L.A.; Chang, S.C.; Perng, D.W.; Wu, L.A.; Chang, S.C.; Perng, D.W.; Su, W.J.; et al. Sleep apnea and risk of pneumonia: A nationwide population-based study. CMAJ 2014, 186, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Fine, J.P.; Gray, R.J. A proportional hazards model for the subdistribution of a competing risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Redolfi, S.; Yumino, D.; Ruttanaumpawan, P.; Yau, B.; Su, M.C.; Lam, J.; Bradley, T.D. Relationship between overnight rostral fluid shift and Obstructive Sleep Apnea in nonobese men. Am. J. Respir. Crit. Care Med. 2009, 179, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Elias, R.M.; Bradley, T.D.; Kasai, T.; Motwani, S.S.; Chan, C.T. Rostral overnight fluid shift in end-stage renal disease: Relationship with obstructive sleep apnea. Nephrol. Dial. Transplant. 2012, 27, 1569–1573. [Google Scholar] [CrossRef] [PubMed]
- Roumelioti, M.E.; Brown, L.K.; Unruh, M.L. The relationship between volume overload in end-stage renal disease and obstructive sleep apnea. Semin. Dial. 2015, 28, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Ogna, A.; Forni Ogna, V.; Mihalache, A.; Pruijm, M.; Halabi, G.; Phan, O.; Cornette, F.; Bassi, I.; Rubio, J.H.; Burnier, M.; et al. Obstructive sleep apnea severity and overnight body fluid shift before and after hemodialysis. Clin. J. Am. Soc. Nephrol. 2015, 10, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Lyons, O.D.; Chan, C.T.; Yadollahi, A.; Bradley, T.D. Effect of ultrafiltration on sleep apnea and sleep structure in patients with end-stage renal disease. Am. J. Respir. Crit. Care Med. 2015, 191, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Sivalingam, M.; Chakravorty, I.; Mouatt, S.; Farrington, K. Obstructive sleep apnea in incremental hemodialysis: Determinants, consequences, and impact on survival. Hemodial. Int. 2013, 17, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Beecroft, J.M.; Hoffstein, V.; Pierratos, A.; Chan, C.T.; McFarlane, P.A.; Hanly, P.J. Pharyngeal narrowing in end-stage renal disease: Implications for obstructive sleep apnoea. Eur. Respir. J. 2007, 30, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Tripepi, R.; Torino, C.; Bellantoni, M.; Tripepi, G.; Mallamaci, F. Lung congestion as a risk factor in end-stage renal disease. Blood Purif. 2013, 36, 184–191. [Google Scholar] [CrossRef] [PubMed]
- Hanly, P.J.; Pierratos, A. Improvement of sleep apnea in patients with chronic renal failure who undergo nocturnal hemodialysis. N. Engl. J. Med. 2001, 344, 102–107. [Google Scholar] [CrossRef] [PubMed]
- Beecroft, J.M.; Hoffstein, V.; Pierratos, A.; Chan, C.T.; McFarlane, P.; Hanly, P.J. Nocturnal haemodialysis increases pharyngeal size in patients with sleep apnoea and end-stage renal disease. Nephrol. Dial. Transplant. 2008, 23, 673–679. [Google Scholar] [CrossRef] [PubMed]
- Wanic-Kossowska, M. Ventilation and gas exchange in patients with chronic renal failure treated with hemodialysis (HD) and intermittent peritoneal dialysis (IPD). Pol. Arch. Med. Wewn. 1996, 96, 442–450. [Google Scholar] [PubMed]
- Skatrud, J.B.; Dempsey, J.A.; Badr, S.; Begle, R.L. Effect of airway impedance on CO2 retention and respiratory muscle activity during NREM sleep. J. Appl. Physiol. (1985) 1988, 65, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.C.; Lam, B.; Yao, T.J.; Leung, W.S.; Chu, C.M.; Ho, Y.W.; Ip, M.S.; Lai, K.N. Sleep apnea is a novel risk predictor of cardiovascular morbidity and death in patients receiving peritoneal dialysis. Kidney Int. 2010, 77, 1031–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, T.; Peppard, P.E.; Gottlieb, D.J. Epidemiology of obstructive sleep apnea: A population health perspective. Am. J. Respir. Crit. Care Med. 2002, 165, 1217–1239. [Google Scholar] [CrossRef] [PubMed]
- Prezant, D.J. Effect of uremia and its treatment on pulmonary function. Lung 1990, 168, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Bunchman, T.E.; Meldrum, M.K.; Meliones, J.E.; Sedman, A.B.; Walters, M.B.; Kershaw, D.B. Pulmonary function variation in ventilator dependent critically ill infants on peritoneal dialysis. Adv. Perit. Dial. 1992, 8, 75–78. [Google Scholar] [PubMed]
- Stanchina, M.L.; Malhotra, A.; Fogel, R.B.; Trinder, J.; Edwards, J.K.; Schory, K.; White, D.P. The influence of lung volume on pharyngeal mechanics, collapsibility, and genioglossus muscle activation during sleep. Sleep 2003, 26, 851–856. [Google Scholar] [CrossRef] [PubMed]
- van Biesen, W.; Claes, K.; Covic, A.; Fan, S.; Lichodziejewska-Niemierko, M.; Schoder, V.; Verger, C.; Wabel, P. A multicentric, international matched pair analysis of body composition in peritoneal dialysis versus haemodialysis patients. Nephrol. Dial. Transplant. 2013, 28, 2620–2628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Díaz, V.; Pérez-Escudero, A.; Sanz-Ballesteros, S.; Rodríguez-Portela, G.; Valenciano-Martínez, S.; Palomo-Aparicio, S.; Hernández-García, E.; Sánchez-García, L.; Gordillo-Martín, R.; Marcos-Sánchez, H. A New Method to Increase Ultrafiltration in Peritoneal Dialysis: Steady Concentration Peritoneal Dialysis. Perit. Dial. Int. 2016, 36, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Choi, E.W.; Park, J.W.; Cho, K.H.; Do, J.Y. Clinical Significance of the Edema Index in Incident Peritoneal Dialysis Patients. PLoS ONE 2016, 11, e0147070. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.E.; Kwon, Y.J.; Song, H.C.; Kim, J.K.; Song, Y.R.; Shin, S.J.; Kim, H.W.; Lee, C.H.; Lee, T.W.; Kim, Y.O.; et al. Overhydration Negatively Affects Quality of Life in Peritoneal Dialysis Patients: Evidence from a Prospective Observational Study. Int. J. Med. Sci. 2016, 13, 686–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Young, T.; Skatrud, J.; Peppard, P.E. Risk factors for obstructive sleep apnea in adults. JAMA 2004, 291, 2013–2016. [Google Scholar] [CrossRef] [PubMed]
- Lo, W.K. Metabolic syndrome and obesity in peritoneal dialysis. Kidney Res. Clin. Pract. 2016, 35, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Schwab, R.J. Properties of tissues surrounding the upper airway. Sleep 1996, 19 (Suppl. S10), S170–S174. [Google Scholar] [CrossRef] [PubMed]
- Losso, R.L.; Minhoto, G.R.; Riella, M.C. Sleep disorders in patients with end-stage renal disease undergoing dialysis: Comparison between hemodialysis, continuous ambulatory peritoneal dialysis and automated peritoneal dialysis. Int. Urol. Nephrol. 2015, 47, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Punjabi, N.M.; Caffo, B.S.; Goodwin, J.L.; Gottlieb, D.J.; Newman, A.B.; O’Connor, G.T.; Rapoport, D.M.; Redline, S.; Resnick, H.E.; Robbins, J.A.; et al. Sleep-disordered breathing and mortality: A prospective cohort study. PLoS Med. 2009, 6, e1000132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowdhuri, S.; Quan, S.F.; Almeida, F.; Ayappa, I.; Batool-Anwar, S.; Budhiraja, R.; Cruse, P.E.; Drager, L.F.; Griss, B.; Marshall, N.; et al. An Official American Thoracic Society Research Statement: Impact of Mild Obstructive Sleep Apnea in Adults. Am. J. Respir. Crit. Care Med. 2016, 193, e37–e54. [Google Scholar] [CrossRef] [PubMed]
- Campos-Rodriguez, F.; Martinez-Garcia, M.A.; de la Cruz-Moron, I.; Almeida-Gonzalez, C.; Catalan-Serra, P.; Montserrat, J.M. Cardiovascular mortality in women with obstructive sleep apnea with or without continuous positive airway pressure treatment: A cohort study. Ann. Intern. Med. 2012, 156, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Marin, J.M.; Carrizo, S.J.; Vicente, E.; Agusti, A.G. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: An observational study. Lancet 2005, 365, 1046–1053. [Google Scholar] [CrossRef]
- Barbé, F.; Durán-Cantolla, J.; Sánchez-de-la-Torre, M.; Martínez-Alonso, M.; Carmona, C.; Barceló, A.; Chiner, E.; Masa, J.F.; Gonzalez, M.; Marín, J.M.; et al. Effect of continuous positive airway pressure on the incidence of hypertension and cardiovascular events in nonsleepy patients with obstructive sleep apnea: A randomized controlled trial. JAMA 2012, 307, 2161–2168. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, R.D.; Antic, N.A.; Heeley, E.; Luo, Y.; Ou, Q.; Zhang, X.; Mediano, O.; Chen, R.; Drager, L.F.; Liu, Z.; et al. CPAP for Prevention of Cardiovascular Events in Obstructive Sleep Apnea. N. Engl. J. Med. 2016, 375, 919–931. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Age, Sex, and Index-Year Frequency Matched | Propensity Score Matched Subgroup analysis | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Controls N = 118244 | Total ESRD N = 29561 | HD N = 19574 | PD N = 9987 | ESRD vs. Control | HD vs. PD | HD N = 9826 | PD N = 9826 | HD vs. PD | |||||||
| n | % | n | % | n | % | n | % | p-value | n | % | n | % | p-Value | ||
| Age, years | 0.99 | 0.13 | 0.10 | ||||||||||||
| <50 | 47,300 | 40.0 | 11,825 | 40.0 | 7750 | 39.6 | 4075 | 40.8 | 4145 | 42.2 | 4006 | 40.8 | |||
| 50–64 | 41,712 | 35.3 | 10,428 | 35.3 | 6952 | 35.5 | 3476 | 34.8 | 3295 | 33.5 | 3416 | 34.8 | |||
| 65+ | 29,232 | 24.7 | 7308 | 24.7 | 4872 | 24.9 | 2436 | 24.4 | 2386 | 24.3 | 2404 | 24.5 | |||
| Mean ± SD a | 54.0 | 14.9 | 54.1 | 14.8 | 54.3 | 14.7 | 53.7 | 15.1 | 0.18 a | <0.001 a | 53.7 | 15.1 | 53.7 | 15.1 | 0.89 a |
| Gender | 0.99 | 0.27 | 0.77 | ||||||||||||
| Women | 63,152 | 53.4 | 15,788 | 53.4 | 10,409 | 53.2 | 5379 | 53.9 | 5260 | 53.5 | 5280 | 53.7 | |||
| Men | 55,092 | 46.6 | 13,773 | 46.6 | 9165 | 46.8 | 4608 | 46.1 | 4566 | 46.5 | 4546 | 46.3 | |||
| Comorbidity | |||||||||||||||
| CAD | 17,217 | 14.6 | 10,153 | 34.4 | 7090 | 36.2 | 3063 | 30.7 | <0.001 | <0.001 | 3073 | 31.3 | 3043 | 31.0 | 0.64 |
| Diabetes | 10,287 | 8.70 | 12,974 | 43.9 | 9354 | 47.8 | 3620 | 36.3 | <0.001 | <0.001 | 3600 | 36.6 | 3620 | 36.8 | 0.77 |
| Stroke | 17,360 | 14.7 | 3902 | 13.2 | 2885 | 14.7 | 1017 | 10.2 | <0.001 | <0.001 | 1034 | 10.5 | 1017 | 10.4 | 0.69 |
| Hyperlipidemia | 23,203 | 19.6 | 13,234 | 44.8 | 8698 | 44.4 | 4536 | 45.4 | <0.001 | 0.11 | 4362 | 44.4 | 4437 | 45.2 | 0.28 |
| COPD | 11,636 | 9.84 | 3839 | 13.0 | 2645 | 13.5 | 1194 | 12.0 | <0.001 | <0.001 | 1212 | 12.3 | 1179 | 12.0 | 0.47 |
| Hypertension | 36,888 | 31.2 | 26,275 | 88.9 | 17,317 | 88.5 | 8958 | 89.7 | <0.001 | 0.002 | 8773 | 89.3 | 8799 | 89.6 | 0.55 |
| CHF | 2807 | 2.37 | 6677 | 22.6 | 4875 | 24.9 | 1802 | 18.0 | <0.001 | <0.001 | 1854 | 18.9 | 1801 | 18.3 | 0.33 |
| Obesity | 1346 | 1.14 | 481 | 1.63 | 331 | 1.69 | 150 | 1.50 | <0.001 | 0.22 | 151 | 1.54 | 149 | 1.52 | 0.91 |
| Variable | Event | PY | Rate † | cSHR ‡ (95% CI) | aSHR # (95% CI) |
|---|---|---|---|---|---|
| ESRD | |||||
| None | 365 | 661,456 | 5.52 | 1.00 | 1.00 |
| HD | 60 | 85,402 | 7.03 | 1.31( 1.00, 1.72) * | 0.89 (0.65, 1.21) |
| PD | 70 | 37,095 | 18.9 | 3.50 (2.71, 4.50) *** | 2.34 (1.75, 3.12) *** |
| All ESRD | 130 | 122,497 | 10.6 | 1.98 (1.63, 2.41) *** | 1.36 (1.06, 1.73) * |
| Age, year | |||||
| <50 | 210 | 346,743 | 6.06 | 1.11 (0.91, 1.36) | 1.57 (1.26,1.97) *** |
| 50–64 | 194 | 271,513 | 7.15 | 1.31 (1.05, 1.62) * | 1.50 (1.19, 1.88) *** |
| 65+ | 91 | 165,697 | 5.49 | 1.00 | 1.00 |
| Gender | |||||
| Women | 181 | 424,070 | 4.27 | 1.00 | 1.00 |
| Men | 314 | 359,883 | 8.73 | 1.92 (1.62, 2.28) *** | 2.10 (1.75, 2.52) *** |
| Comorbidity | |||||
| CAD | |||||
| No | 351 | 661,699 | 5.30 | 1.00 | 1.00 |
| Yes | 144 | 122,254 | 11.8 | 2.50 (2.03, 3.08) *** | 1.68 (1.33, 2.13) *** |
| Diabetes | |||||
| No | 421 | 693,230 | 6.07 | 1.00 | 1.00 |
| Yes | 74 | 90,723 | 8.16 | 1.31 (1.02, 1.68) * | 0.65 (0.49, 0.86) ** |
| Stroke | |||||
| No | 416 | 687,372 | 6.05 | 1.00 | 1.00 |
| Yes | 79 | 96,581 | 8.18 | 1.40 (1.09, 1.80) ** | 1.08 (0.83, 1.40) |
| Hyperlipidemia | |||||
| No | 315 | 619,785 | 5.08 | 1.00 | 1.00 |
| Yes | 180 | 164,168 | 11.0 | 2.22 (1.83, 2.69) *** | 1.67(1.35, 2.06) *** |
| COPD | |||||
| No | 422 | 715,044 | 5.90 | 1.00 | 1.00 |
| Yes | 73 | 68,909 | 10.6 | 1.87 (1.44, 2.41) *** | 1.44 (1.10, 1.87) ** |
| Hypertension | |||||
| No | 216 | 490,374 | 4.40 | 1.00 | 1.00 |
| Yes | 279 | 293,579 | 9.50 | 2.43 (2.01, 2.94) *** | 1.73 (1.36, 2.20) *** |
| CHF | |||||
| No | 454 | 749,156 | 6.06 | 1.00 | 1.00 |
| Yes | 41 | 34,796 | 11.8 | 1.93 (1.40, 3.67) *** | 1.06 (0.75, 1.51) |
| Obesity | |||||
| No | 484 | 776,328 | 6.23 | 1.00 | 1.00 |
| Yes | 11 | 7625 | 14.4 | 2.15 (1.18, 3.91) * | 1.71 (0.94, 3.13) |
| Outcome | Propensity Score Matched | |
| HD | PD | |
| (N = 9826) | (N = 9826) | |
| Person-years | 38,989 | 36,804 |
| OSA | ||
| Overall | ||
| No. of event | 26 | 70 |
| Incidence rate | 6.67 | 19.0 |
| cSHR (95% CI) | 1.00 (Reference) | 2.14 (1.46, 3.14) *** |
| aSHR a (95% CI) | 1.00 (Reference) | 2.17 (1.47, 3.21) ** |
| Outcome | Age and Sex Frequency Matched | Propensity Score Matched | |||
| Control | HD | PD | HD | PD | |
| n/N | n/N | n/N | n/N | n/N | |
| MOSA/OSA | 141/365 | 30/60 | 48/70 | 14/26 | 48/70 |
| Rate, % | 38.6% | 50.0% | 68.6% | 53.9% | 68.6% |
| cOR (95% CI) | 1.00 (Reference) | 1.59 (0.92, 2.75) | 3.47 (2.01, 5.99) *** | 1.00 (Reference) | 1.87 (0.74,4.70) |
| aORs (95% CI) a | 1.00 (Reference) | 1.31 (0.70, 2.45) | 3.05 (1.64, 5.71) ** | 1.00 (Reference) | 2.18 (0.77,6.15) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, S.-T.; Lin, C.-L.; Yu, T.-M.; Kao, C.-H.; Liang, W.-M.; Chou, T.-C. Risk, Severity, and Predictors of Obstructive Sleep Apnea in Hemodialysis and Peritoneal Dialysis Patients. Int. J. Environ. Res. Public Health 2018, 15, 2377. https://doi.org/10.3390/ijerph15112377
Huang S-T, Lin C-L, Yu T-M, Kao C-H, Liang W-M, Chou T-C. Risk, Severity, and Predictors of Obstructive Sleep Apnea in Hemodialysis and Peritoneal Dialysis Patients. International Journal of Environmental Research and Public Health. 2018; 15(11):2377. https://doi.org/10.3390/ijerph15112377
Chicago/Turabian StyleHuang, Shih-Ting, Chen-Li Lin, Tung-Min Yu, Chia-Hung Kao, Wen-Miin Liang, and Tzu-Chieh Chou. 2018. "Risk, Severity, and Predictors of Obstructive Sleep Apnea in Hemodialysis and Peritoneal Dialysis Patients" International Journal of Environmental Research and Public Health 15, no. 11: 2377. https://doi.org/10.3390/ijerph15112377
APA StyleHuang, S. -T., Lin, C. -L., Yu, T. -M., Kao, C. -H., Liang, W. -M., & Chou, T. -C. (2018). Risk, Severity, and Predictors of Obstructive Sleep Apnea in Hemodialysis and Peritoneal Dialysis Patients. International Journal of Environmental Research and Public Health, 15(11), 2377. https://doi.org/10.3390/ijerph15112377