Barriers and Facilitators of Engaging Community Health Workers in Non-Communicable Disease (NCD) Prevention and Control in China: A Systematic Review (2006–2016)

Abstract
:1. Introduction
2. Methodology
2.1. Data Sources
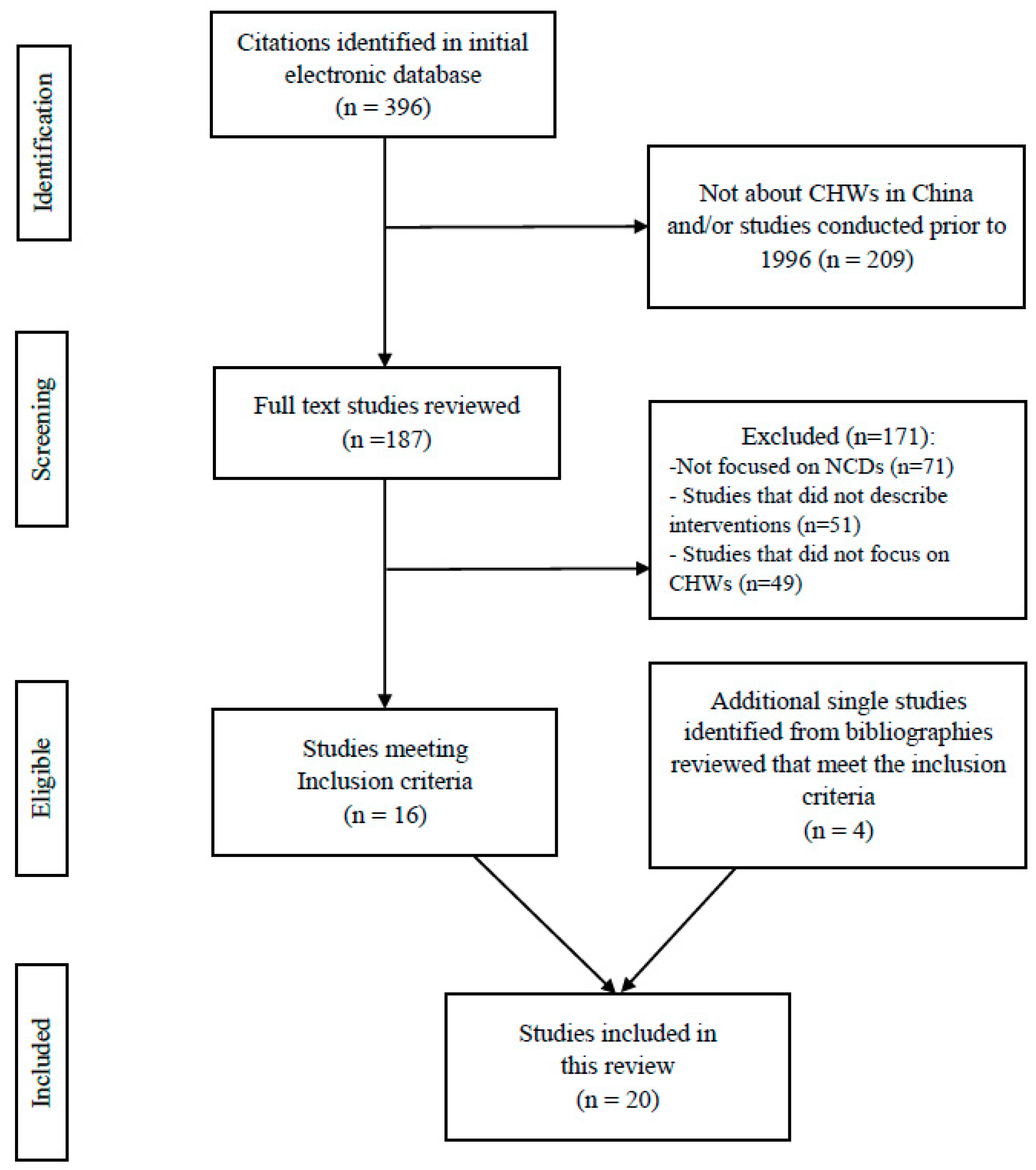
2.2. Study Selection
- Participants: Participants can be patients suffering from the aforementioned NCDs, NCD high-risk populations, or the general populations without restricting types of participants, because preventive services and interventions can reach different populations based on specific needs and settings.
- Intervention types: NCD-related preventive measures or health promotion interventions that were provided by CHWs, village doctors, lay health supporters, or those healthcare personnel who delivered community-based services but received less formal training than health professionals.
- Comparison: Not applicable.
- Outcome: Delivery of reported intervention, provider types, categories of NCD topics, and challenges and facilitators.
- Study types: Both descriptive and evaluation studies conducted in China focusing on community-based NCD-related programs (including programs focusing on the chronic diseases as well as the NCD risk factors), such as hypertension screening, physical activity promotions, early detection for cardiovascular diseases (CVDs), diabetes, and mental health illness.
- Articles that did not focus on China.
- Articles that focused on the health professionals (physicians, doctors, nurses) rather than CHWs as we have defined for this review.
- Articles that mainly discussed general primary health care (i.e., non-NCD related services), such as immunization, infectious disease case management, family planning, reproductive health, environmental health, and maternal and child health.
- Articles that did not describe structured NCD-related interventions (e.g., news, conference reports, books, reviews, health system analysis, disease prevalence).
3. Results
3.1. General Description
3.2. NCD-Related Services Provided by CHWs
3.2.1. Diabetes and Hypertension
3.3.2. Cancer
3.2.3. Mental Health
3.2.4. Cardiovascular Diseases (CVDs)
3.2.5. NCD Risk Factors
3.3. Training Received by CHWs
3.4. Barriers
3.4.1. Lack of Support from the Local Health Systems and from the Public
3.4.2. Lack of Resources
3.4.3. Heavy Workload
3.4.4. Inadequate Financial Incentives
3.4.5. Heavy Reliance on Electronic Technology
3.4.6. Lack of Knowledge and Skills
3.5. Facilitators
3.5.1. Integrated Health System
3.5.2. Community and Patient Trust
3.5.3. Incentives
3.5.4. Appropriate Training
3.5.5. Capacity of CHWs
3.5.6. Interests and Attitudes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgements
Conflicts of Interest
Abbreviations
| CHW | Community health worker |
| CVDs | Cardiovascular diseases |
| THC | Township Health lefts |
| NCMS | New Cooperative Medical Scheme |
| NCDs | Non-communicable diseases |
| RCT | Randomized control trial |
| TB | Tuberculosis |
| VDs | Village doctors |
| WHO | World Health Organization |
References
- Wang, L.; Kong, L.; Wu, F.; Bai, Y.; Burton, R. Preventing chronic diseases in China. Lancet 2005, 366, 1821–1824. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Noncommunicable Diseases. Country Profiles: China. Updated 2014. Available online: http://www.who.int/nmh/countries/chn_en.pdf (accessed on 15 June 2017).
- Wang, S.; Marquez, P.; Langenbrunner, J.; Niessen, L.; Suhrcke, M.; Song, F. Toward a healthy and harmonious life in China: Stemming the rising tide of non-communicable diseases. Available online: http://documents.worldbank.org/curated/en/618431468012000892/Toward-a-healthy-and-harmonious-life-in-China-stemming-the-rising-tide-of-non-communicable-diseases (accessed on 20 September 2018).
- Tang, S.; Ehiri, J.; Long, Q. China’s biggest, most neglected health challenge: Non-communicable diseases. Infect. Dis. Poverty 2013, 2, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qi, X.; Zhang, P.; Zhang, Y.; Wan, X.; Yang, G. China’s prevention and control strategies on non-communicable diseases: The status quo. Chin. J. Prev. Cont. Chron. Non-Commun. Dis. 2012, 20, 214–217. (In Chinese) [Google Scholar]
- Lewin, S.; Munabi-Babigumira, S.; Glenton, C.; Daniels, K.; Bosch-Capblanch, X.; van Wyk, B.E.; Odgaard-Jensen, J.; Johansen, M.; Aja, G.N.; Zwarenstein, M.; et al. Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). The World Health Report 2006: Working Together for Health. Available online: http://apps.who.int/iris/handle/10665/43432 (accessed on 15 January 2018).
- Sidel, V.W. The barefoot doctors of the People’s Republic of China. N. Engl. J. Med. 1972, 286, 1292–1300. [Google Scholar] [CrossRef] [PubMed]
- de Geyndt, W.; Zhao, X.; Liu, S. From Barefoot Doctor to Village Doctor in Rural China; World Bank Technical Paper; The World Bank: Washington, DC, USA, 1992; Available online: http://www.popline.org/node/324436 (accessed on 15 January 2018).
- Wang, J.; Kushner, K.; Frey, J.J.; Du, X.P.; Qian, N. Primary care reform in the Peoples’ Republic of China: Implications for training family physicians for the world’s largest country. Fam. Med.-Kansas City 2007, 39, 639. [Google Scholar]
- Wang, Y.; Wilkinson, M.; Ng, E.; Cheng, K.K. Primary care reform in China. Br. J. Gen. Pract. 2012, 62, 546–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cherrington, A.; Ayala, G.X.; Amick, H.; Allison, J.; Corbie-Smith, G.; Scarinci, I. Implementing the community health worker model within diabetes management: Challenges and lessons learned from programs across the United States. Diabetes Educ. 2008, 34, 824–833. [Google Scholar] [CrossRef] [PubMed]
- Browning, C.; Chapman, A.; Yang, H.; Liu, S.; Zhang, T.; Enticott, J.C.; Thomas, S.A. Management of type 2 diabetes in China: The Happy Life Club, a pragmatic cluster randomised controlled trial using health coaches. BMJ Open 2016, 6, e009319. [Google Scholar] [CrossRef] [PubMed]
- Chai, J.; Shen, X.; Feng, R.; Cheng, J.; Chen, Y.; Zha, Z.; Jia, S.; Liang, H.; Zhao, T.; Sha, R.; et al. eCROPS-CA: A systematic approach toward effective and sustainable cancer prevention in rural China. BMC Cancer 2015, 15, 233. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Ajay, V.S.; Dunzhu, D.; Hameed, S.S.; Li, X.; Liu, Z.; Li, C.; Chen, H.; Cho, K.; Li, R.; et al. A cluster-randomized controlled trial of a simplified multifaceted management program for individuals at high cardiovascular risk (SimCard Trial) in rural Tibet, China and Haryana, India. Circulation 2015, 132, 815–824. [Google Scholar] [CrossRef] [PubMed]
- Robinson, K.A.; Saldanha, J.; Mckoy, N.A. Development of a framework to identify research gaps from systematic reviews. J. Clin. Epidemiol. 2011, 64, 1325–1330. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Feng, R.; Li, K.; Cheng, J.; Xie, S.; Chai, J.; Wei, P.; Wang, D. Toward integrated and sustainable prevention against diabetes in rural China: Study rationale and protocol of eCROPS. BMC Endocr. Disord. 2013, 13, 28. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.W.; Abdullah, A.S.; Clinciu, D.L.; Scholl, J.; Jin, X.; Lu, H.; Chen, S.S.; Iqbal, U.; Heineck, M.J.; Li, Y.C. Empowering village doctors and enhancing rural healthcare using cloud computing in a rural area of mainland China. Comput. Methods Programs Biomed. 2014, 113, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Chai, J.; Cheng, J.; Li, K.; Xie, S.; Liang, H.; Shen, X.; Feng, R.; Wang, D. A smart web aid for preventing diabetes in rural China: Preliminary findings and lessons. J. Med. Internet Res. 2014, 16, e98. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Wang, Z.; Fisher, E.B.; Tanasugarn, C. Peer support for diabetes management in primary care and community settings in Anhui Province, China. Ann. Fam. Med. 2015, 13 (Suppl. 1), S50–S58. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Lei, T.; Xie, Z.; Zhang, T. Determinants of basic public health services provision by village doctors in China: Using non-communicable diseases management as an example. BMC Health Serv. Res. 2016, 16, 42. [Google Scholar] [CrossRef] [PubMed]
- Peiris, D.; Sun, L.; Patel, A.; Tian, M.; Essue, B.; Jan, S.; Zhang, P. Systematic medical assessment, referral and treatment for diabetes care in China using lay family health promoters: Protocol for the SMARTDiabetes cluster randomised controlled trial. Implement. Sci. 2016, 11, 116. [Google Scholar] [CrossRef] [PubMed]
- Belinson, J.L.; Wang, G.; Qu, X.; Du, H.; Shen, J.; Xu, J.; Zhong, L.; Yi, J.; Yi, X.; Wu, R. The development and evaluation of a community based model for cervical cancer screening based on self-sampling. Gynecol. Oncol. 2014, 132, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Prince, M.; Ferri, C.P.; Acosta, D.; Albanese, E.; Arizaga, R.; Dewey, M.; Gavrilova, S.I.; Guerra, M.; Huang, Y.; Jacob, K.S.; et al. The protocols for the 10/66 dementia research group population-based research programme. BMC Public Health 2007, 7, 165. [Google Scholar] [CrossRef] [PubMed]
- Gong, W.; Xu, D.; Zhou, L.; Brown III, H.S.; Smith, K.L.; Xiao, S. Village doctor-assisted case management of rural patients with schizophrenia: Protocol for a cluster randomized control trial. Implement. Sci. 2014, 9, 13. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Wu, G.; Wang, Z.; Yan, J.; Zhou, J.; Ding, Y.; Jiang, Y.; Rao, S.; Zhou, Q.; Ni, H.; et al. Two-year prospective case-controlled study of a case management program for community-dwelling individuals with schizophrenia. Shanghai Arch. Psychiatry 2014, 26, 119. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Gu, Y. Effect of self-management training on adherence to medications among community residents with chronic schizophrenia: A singleblind randomized controlled trial in Shanghai, China. Shanghai Arch. Psychiatry 2014, 26, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Ma, Z.; Huang, H.; Chen, Q.; Chen, F.; Abdullah, A.S.; Nie, G.; Feng, Q.; Wei, B. Mental health services in rural China: A qualitative study of primary health care providers. BioMed. Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Yang, F.; Tang, T.; Yang, X.; Zhang, W.; Wang, X.; Ji, L.; Xiao, Y.; Ma, K.; Wang, Y.; et al. Advantages and challenges of a village doctor-based cognitive behavioral therapy for late-life depression in rural China: A qualitative study. PLoS ONE 2015, 10, e0137555. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.R.; Gong, W.; Caine, E.D.; Xiao, S.; Hughes, J.P.; Ng, M.; Simoni, J.; He, H.; Smith, K.L.; Brown III, H.S.; et al. Lay health supporters aided by a mobile phone messaging system to improve care of villagers with schizophrenia in Liuyang, China: Protocol for a randomised control trial. BMJ Open 2016, 6, e010120. [Google Scholar] [CrossRef] [PubMed]
- Ajay, V.S.; Tian, M.; Chen, H.; Wu, Y.; Li, X.; Dunzhu, D.; Ali, M.K.; Tandon, N.; Krishnan, A.; Prabhakaran, D.; et al. A cluster-randomized controlled trial to evaluate the effects of a simplified cardiovascular management program in Tibet, China and Haryana, India: Study design and rationale. BMC Public Health 2014, 14, 924. [Google Scholar] [CrossRef] [PubMed]
- Yan, L.L.; Fang, W.; Delong, E.; Neal, B.; Peterson, E.D.; Huang, Y.; Sun, N.; Yao, C.; Li, X.; MacMahon, S.; et al. Population impact of a high cardiovascular risk management program delivered by village doctors in rural China: Design and rationale of a large, cluster-randomized controlled trial. BMC Public Health 2014, 14, 345. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Yan, L.L.; Niu, W.; Yao, C.; Feng, X.; Zhang, J.; Shi, J.; Zhang, Y.; Zhang, R.; Hao, Z.; et al. The effects of a community-based sodium reduction program in rural China—A cluster-randomized trial. PLoS ONE 2016, 11, e0166620. [Google Scholar] [CrossRef] [PubMed]
- Chang, A.; Patberg, E.; Cueto, V.; Li, H.; Singh, B.; Kenya, S.; Alonzo, Y.; Carrasquillo, O. Community health workers, access to care, and service utilization among Florida Latinos: A randomized controlled trial. Am. J. Public Health. 2018, 108, 1249–1251. [Google Scholar] [CrossRef] [PubMed]
- Ursua, R.A.; Aguilar, D.E.; Wyatt, L.C.; Trinh-Shevrin, C.; Gamboa, L.; Valdellon, P.; Perrella, E.G.; Dimaporo, M.Z.; Nur, P.Q.; Tandon, S.D.; et al. A community health worker intervention to improve blood pressure among Filipino Americans with hypertension: A randomized controlled trial. Prev. Med. Rep. 2018, 11, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Khetan, A.K.; Purushothaman, R.; Chami, T.; Hejjaji, V.; Madan Mohan, S.K.; Josephson, R.A.; Webel, A.R. The effectiveness of community health workers in CVD prevention in LMIC. Glob. Heart 2016, 12, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Perry, H.B.; Zulliger, R.; Rogers, M.M. Community health workers in low-, middle-, and high-income countries: An overview of their history, recent evolution, and current effectiveness. Ann. Rev. Public Health 2014, 35, 399–421. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Health Observatory Data: Risk Factors. 2017. Available online: http://www.who.int/gho/ncd/risk_factors/en/ (accessed on 15 January 2018).
- Koon, A.D.; Goudge, J.; Norris, S.A. A review of generalist and specialist community health workers for delivering adolescent health services in sub-Saharan Africa. Hum. Resour. Health 2013, 11, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reininger, B.M.; Mitchell-Bennett, L.; Lee, M.; Gowen, R.Z.; Barroso, C.S.; Gay, J.L.; Saldana, M.V. Tu Salud, ¡Si Cuenta!: Exposure to a community-wide campaign and its associations with physical activity and fruit and vegetable consumption among individuals of Mexican descent. Soc. Sci. Med. 2015, 143, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Shelley, D.; VanDevanter, N.; Cleland, C.C.; Nguyen, L.; Nguyen, N. Implementing tobacco use treatment guidelines in community health centers in Vietnam. Implement. Sci. 2015, 10, 142. [Google Scholar] [CrossRef] [PubMed]
- Wewers, M.E.; Shoben, A.; Conroy, S.; Curry, E.; Ferketich, A.K.; Murray, D.M.; Nemeth, J.; Wermert, A. Effectiveness of two community health worker models of tobacco dependence treatment among community residents of Ohio Appalachia. Nicotine Tob. Res. 2017, 19, 1499–1507. [Google Scholar] [PubMed]
- Abrahams-Gessel, S.; Denman, C.A.; Gaziano, T.A.; Levitt, N.S.; Puoane, T. Challenges facing successful scaling up of effective screening for cardiovascular disease by community health workers in Mexico and South Africa: Policy implications. Health Syst. Policy Res. 2016, 3, 26. [Google Scholar]
- Zhang, X.; Fang, P. Job satisfaction of village doctors during the new healthcare reforms in China. Aust. Health Rev. 2016, 40, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Gaziano, T.A.; Abrahams-Gessel, S.; Denman, C.A.; Montano, C.M.; Khanam, M.; Puoane, T.; Levitt, N.S. An assessment of community health workers’ ability to screen for cardiovascular disease risk with a simple, non-invasive risk assessment instrument in Bangladesh, Guatemala, Mexico, and South Africa: An observational study. Lancet Glob. Health 2015, 3, e556–563. [Google Scholar] [CrossRef]
- Han, H.R.; Kim, K.B.; Kim, M.T. Evaluation of the training of Korean community health workers for chronic disease management. Health Educ. Res. 2007, 22, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Asiimwe-Kateera, B.; Condo, J.; Ndagijimana, A.; Kumar, S.; Mukeshimana, M.; Gaju, E.; Muhire, A.; Muhimpundu, M.A.; Kim, M.J.; Kurth, A. Analysis: Mobile health approaches to non-communicable diseases in Rwanda. Rwanda J. 2015, 2, 89–92. [Google Scholar] [CrossRef]
- DiCarlo, J.M.; Gopakumar, S.; Dhillon, P.K.; Krishnan, S. Adoption of Information and communication technologies for early detection of breast and cervical cancers in low-and middle-income countries. J. Glob. Oncol. 2016, 2, 222–234. [Google Scholar] [CrossRef] [PubMed]
- Amarchand, R.; Sharma, H.; Krishnan, A. Community health workers can be trained to measure blood pressure: Experience from India. Reg. Health Forum. 2013, 17, 26–31. [Google Scholar]
- Wagstaff, A.; Lindelow, M.; Jun, G.; Ling, X.; Juncheng, Q. Extending health insurance to the rural population: An impact evaluation of China’s new cooperative medical scheme. J. Health Econ. 2009, 28, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Wang, W.; Yan, F. Compensation and welfare of village doctors under integrated management of township and village health facilities. Chin. Rural Health Serv. Adm. 2011, 31, 7–9. [Google Scholar]
- Zhang, S.; Zhang, W.; Zhou, H.; Xu, H.; Qu, Z.; Guo, M.; Wang, F.; Zhong, Y.; Gu, L.; Liang, X.; et al. How China’s new health reform influences village doctors’ income structure: Evidence from a qualitative study in six counties in China. Hum. Resour. Health 2015, 13, 26. [Google Scholar] [CrossRef] [PubMed]
- Kok, M.C.; Kane, S.S.; Tulloch, O.; Ormel, H.; Theobald, S.; Dieleman, M.; Taegtmeyer, M.; Broerse, J.E.; de Koning, K.A. How does context influence performance of community health workers in low- and middle-income countries? Evidence from the literature. Health Res. Policy Syst. 2015, 13, 13. [Google Scholar] [CrossRef] [PubMed]
- Kasteng, F.; Settumba, S.; Källander, K.; Vassall, A. Valuing the work of unpaid community health workers and exploring the incentives to volunteering in rural Africa. Health Policy Plan. 2016, 31, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Mpembeni, R.N.M.; Bhatnagar, A.; LeFevre, A.; Chitama, D.; Urassa, D.P.; Kilewo, C.; Mdee, R.M.; Semu, H.; Winch, P.J.; Killewo, J.; et al. Motivation and satisfaction among community health workers in Morogoro Region, Tanzania: Nuanced needs and varied ambitions. Hum. Resour. Health 2015, 13, 44. [Google Scholar] [CrossRef] [PubMed]
- Yip, W.C.M.; Hsiao, W.C.; Chen, W.; Hu, S.; Ma, J.; Maynard, A. Early appraisal of China’s huge and complex health-care reforms. Lancet 2012, 379, 833–842. [Google Scholar] [CrossRef]
- Zhou, X.D.; Li, L.; Hesketh, T. Health system reform in rural China: Voices of healthworkers and service-users. Soc. Sci. Med. 2014, 117, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Wang, Z.; Qian, D.; Ni, J. Effects of changes in health insurance reimbursement level on outpatient service utilization of rural diabetics: Evidence from Jiangsu Province, China. BMC Health Serv. Res. 2014, 14, 185. [Google Scholar] [CrossRef] [PubMed]
- Jafar, T.H.; Islam, M.; Hatcher, J.; Hashmi, S.; Bux, R.; Khan, A.; Poulter, N.; Badruddin, S.; Chaturvedi, N. Community based lifestyle intervention for blood pressure reduction in children and young adults in developing country: Cluster randomised controlled trial. BMJ 2010, 340, c2641. [Google Scholar] [CrossRef] [PubMed]
- Coleman, R.; Gill, G.; Wilkinson, D. Noncommunicable disease management in resource-poor settings: A primary care model from rural South Africa. Bull. World Health Organ. 1998, 76, 633. [Google Scholar] [PubMed]
- Van Rie, A.; West, N.S.; Schwartz, S.R.; Mutanga, L.; Hanrahan, C.F.; Ncayiyana, J.; Bassett, J. The unmet needs and health priorities of the urban poor: Generating the evidence base for urban community health worker programmes in South Africa. S. Afr. Med. J. 2018, 108, 734–740. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| No. | Author | Year; Location | Type of NCDs | Provider Type | Payment Mechanism/Structure (Paid/Unpaid) | Indicators | Key Findings/Lessons Learned | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Types of Services | Program Duration | Ended/Current | Types of Training | Training Duration | Challenges (−) | Facilitated Factors (+) | |||||||
| Diabetes and/or hypertension | |||||||||||||
| 1 | Feng et al. [18] | 2013; Lu’An, An’hui Province | T2DM | VDs | paid | 1. Glucose screening; 2. measured body weight and blood pressure; 3. counseling on glucose screening; 4. promoted screening participation via biannual follow-up glucose screening; 5. referral; 6. behavioral change counseling for pre-diabetics | 6 years (every 12 months for plasma glucose and ever month for body weight and blood pressure) | Current | Web-based training, with an ‘occupational toolkit’ consisting of a workbook, a manual guidance, and a set of cue-cards. For example, each cue-card enlisted critical steps or elements for delivering a specific type of counseling; the manual was a reference book including elementary protocols on common problems and solution tips for diabetes prevention | N/A | 1. Most VDs were unaware of diabetes prevention; 2. already heavy workload; 3. heavy reliance on electronic/commuter support may beyond the ability of VDs’ and elder villagers’ in rural areas | 1. Trust from patients and communities; 2. service was simple, capable for VDs (only 15 minutes); 3. well-established guidelines and manuals; 4. village clinics was appropriate setting; 5. electronic support and web-based training were cost-saving and time flexible; 6. performance-based incentives; 7. local health authorities support on resources | The study examined key success factors in a synergistic way towards integrated and sustainable diabetes prevention. It introduced a package of long-term incentives and continuous capacity building mechanism. It built up a potential operational cycle for catalyzing similar efforts in the local prefecture |
| 2 | Lin et al. [19] | 2014;Xilingol county; Inner Mongolia | Hypertension; Diabetes | VDs | paid | 1. Case management and monitoring via EHR; 2. regular followed-up check on medication compliance; 3. measured blood pressure and blood sugar levels | 2008–2011 | Ended | N/A | N/A | Lack of policy support from the health system | Close connection with higher levels of the healthcare system, if implemented in large-scale | Cloud-based EHR had the potential to improve care provision in rural China and efficiency of disease management. |
| 3 | Chen et al. [20] | 2014; Lu An; Anhui Province | T2DM | VDs | paid | 1. Identified high-risk patients; 2. case follow-up counseling and health education on diabetes risks, balanced diets, and physical activities | 6 months; 1 month/session | Ended | Instructions on the application method of the program, with standardized “step-by-step” navigation for VDs to follow in practice | N/A | 1. Lack of electricity security (facility) in remote settings; 2. communication difficulties: sometimes unable to engage patients to finish all the required interventions | 1. Easy to follow the navigation; 2. professional knowledge built in the application helps case identification and management; 3. high acceptance rate among patients | The web-based tool SWAP-DM2 can increase the effectiveness of T2DM preventive services delivered by VDs, and may increase the frontier clinicians’ participation in diabetes prevention in similar settings. |
| 4 | Zhong et al. [21] | 2015; Tonglin, Hefei, Bangbu, Anhui Province | Diabetes | Peer Leaders; CHSC Staff | N/A | Bi-weekly educational meetings co-led by PLs and CHS staffs. Topics: diets, physical activities, medications, foot care, stress management. PLs’ responsibilities: outreach, promotions, emotional support, and non-professional activities (Tai Chi, morning exercise, etc.) | 6 months/session | N/A | N/A | N/A | Lack of staff resources in sub-communities | 1. Close relationship with peer leaders; 2. knowledge; 3. high patient engagement | The PLSP was effective for subcommunity-based diabetes self-management. May be generalizable to cardiovascular prevention. |
| 5 | Li et al. [22] | 2015; three provinces in China, specific location not mentioned | Hypertension; Diabetes | village doctor | paid | 1. Hypertension and/or diabetes case management; 2. created citizen health record (no specific information provided for this category) | 2014 (cross-sectional survey among VDs) | Ended | Routine training programs including content such as health care policy; standards; BPHS quality management; and the norms, standards, and service delivery paths of BPHS. | N/A | 1. Limited compensation and low financial incentive; 2. Uneven geographic coverage of the NCMS insurance contract | 1. Education and training opportunities, 2. public health care subsidy; 3. integrated management and supervision; 4. access to NCMS insurance program contract | Increasing subsidies for VDs, availability and attendance of training opportunities, integrated management, and NCMS contracting of village clinics were important factors in increasing BPHS provision in rural areas. |
| 6 | Browning et al. [13] | 2016; Fengtai District, Beijing | T2DM | Health coach (health workers from the local CHS) | paid | Bi-weekly/monthly telephone and face-to-face motivational interviews (MIs), to provide psychosocial support and lifestyle counseling to improve the outcome of glycemic control and self-care of T2DM patients. | 1 year | Current | Key concepts in patient-centered communications, health psychology, epidemiology of targeted conditions, the framework and rationale of MIs, and the application of MIs core skills. Review workshops were arranged one month after the project initiation, and every three months after that. | Initial training: 20 hours; review workshop: half day per workshop | Not generalizable to rural settings with limited human resources | 1. Good learning and practice capacity; 2. well-organized training process including review workshops | The result of this study indicated that the coach-led psychological intervention had the potential to improve mental health status and well-being of T2DM patients. The intervention could provide evidence for the establishment of regular and free clinical health checks for people with T2DM. |
| 7 | Peiris et al. [23] | 2016; Beijing; Hebei Province | T2DM | FHPs; Healthcare staff | Healthcare Staff: Paid; FHP: unpaid | Healthcare workers: case monitoring, provided support to FHPs via communication tools built inside the mHealth application; FHPs: reported the progress and update EHR data on behalf of the patients (i.e., their family members who have diabetes) via the mHealth application. Co-determined action plan with the support from healthcare workers. Experience sharing with other FHPs in the community via application-based forum. | 2 years: 2016–2017 | N/A | Installation and the use of the technology and management of diabetes | N/A | Findings were not generalizable for other contexts without EHR infrastructure, and for the population with limited access to smart-phone technology | 1. Cost-saving; 2. time-saving; 3. strong motivation of FHPs to support families with diabetes; 4. close communication between clinical healthcare staffs and FHPs. | With FHPs’ and community healthcare staff engagement, the application-based mHealth intervention had the potential to increase the quality of treatment among diabetes patients, and to scale-up the intervention in similar settings. |
| Cancer | |||||||||||||
| 8 | Belinson et al. [24] | 2014; Henan Province | Cervical Cancer | CLs; Promoters;local health worker | paid | Joint tasks for CLs and promoters: gathering personal information and labeling specimens; following the procedures; promoting screening via video, posters, workshops. CLs: instruct sample collection. Local health workers: consultations and referrals after results generation. | 2011–2013 | Ended | Meaning of a positive test; management options and techniques; via video and workshops | 1 day | N/A | 1. Good communication skills; 2. enthusiasm for the job; 3. community, institutional, and government support | This community-based self-sampling model was capable of developing massive screenings. Improvements can be made when local doctors are trained to manage the positives. |
| 9 | Chai et al. [14] | 2015; An’hui Province | cancer | VDs | paid | 1. Health counseling regarding alerting risks and harms, discussing efficacy and benefits, and anticipating barriers; 2. risk assessment promotions; 3. support on healthy lifestyle behavioral changes (reviewing behavior changes, encouraging improvements, identifying and solving problems); 4. manage, record, and upload typical cases bi-monthly on a web forum and shared experiences with other experts and VDs | 5 years | On-going | Web-based tutorial on implementing the project prevention in both video and textual formats; typical case studies as references for practice; video and pictorial materials about cancer and its prevention | One-day orientation workshop | Heavy reliance on electronic support, so the actual practice may beyond the ability of VDs in remote rural areas to use computerized systems | 1. Performance-based incentive and awards; 2. web-based support and supervision system were time-saving; 3. user-friendly education and learning assistance; 4. self-practice, encouragement, problem inquiry, and answering in the training allowed most village doctors to become confident users of the electronic support system | This international program was to empower advocacy, raise awareness about dementia, and ensure that the health and social care needs of older people were met in low- and middle- income countries |
| Mental Health | |||||||||||||
| 10 | Prince et al. [25] | 2007; urban and rural catchment, no specific location mentioned | dementia | CHWs | paid | 1. Help researchers to detect high-risk populations; 2. being the community key informants of the research team | 2 years | Ended | N/A | N/A | N/A | N/A | Village workers with non-clinical training have the potential to manage severe psychiatric diseases and other chronic conditions. |
| 11 | Gong et al. [26] | 2014; Liuyang, Hunan Province | schizophrenia | VDs | paid | 1. Manage case files for patients; 2. store and distribute antipsychotics to family members on a weekly basis, or directly observe drug-taking at the village clinic on a daily basis; 3. accompany patients and family members on bi-monthly visits to psychiatrists for drug dispensation; 4. record patients’ medication-taking behavior weekly; 5. identify signs of relapse; 6. referral. | 1 year | Ended | Mental health knowledge, case-management skills, and DOT. | 3 days | 1. Already overload, no time for extra work; 2. no financial compensation for extra efforts; 3. inadequate engagement from patients and patients’ families | 1. Under the national “686” mental health scheme—government support; 2. consistent collaboration with local government; 3. training met local VDs’ competence and expectations | The results of this experiment provided evidence on the role of health workers with relatively limited medical training in managing severe psychiatric disease and other chronic conditions in developing countries. |
| 12 | Chen et al. [27] | 2014; Xuhui and Hongkou Districts; Shanghai | schizophrenia | CHWs | paid | Worked with community psychiatrists and nurses as a team to conduct case management: 1. Assess recovery status, employment status, and social activities of patients; 2. assist patients to develop personalized rehabilitation plan and cope with the plan, drug adherence training, daily skills training, and family psychological intervention; 3. monthly follow-up to refine the plan | 2 year | Ended | N/A | N/A | N/A | N/A | The study highlighted the need to involve family members in the management of patients’ medications, to use the minimum effective dosage of medications, and to manage all side effects. |
| 13 | Zhou et al. [28] | 2014; Shanghai | schizophrenia | CHWs | paid | Assist patients with self-management. After each patient received weekly self-management skill training, CHWs reviewed patients’ self-management checklist (recorded their daily adherence quality of sleep, occurrence of side effects, occurrence of residual symptoms and early signs of relapse, daily activities, and general mood) every month at a group meeting to supervise the adherence and collect record | 2.5 year | Ended | N/A | N/A | N/A | N/A | Self-management training could introduce a reduction in relapse and improvements in chronic schizophrenia medication adherence. Cost-benefit studies are needed to assess the feasibility of up-scaling this intervention. |
| 14 | Ma et al. [29] | 2015; Guangxi Province | mental illness | primary health care providers | paid | 1. Community education; 2. medication distribution; 3. observed compliance and life status; 4. report side effects or any abnormality; 5. referral and follow-up | 2006–present | Current | Training provided by the national ‘686 project’: mental health disease management, education and social treatment, and prevention of mental illnesses | N/A | 1. Lack of professional knowledge; 2. fear of patients’ attack; 3. extra workload; 4. no available management approach; 5. insufficient subsidies | 1. Communication skills; 2. proper attitudes (without discrimination); 3. improved knowledge; 4. increased income/subsidy | Improvements can be made regarding 1. trainings on professional mental health knowledge and attitudes; 2. management approach; 3. income/subsidy |
| 15 | Tang et al. [30] | 2015; Mianzhu, Sichuan province | late-life depression | VDs | not paid | Conducted weekly intervention with elderly depression patients using CBT techniques to 1. perform physical examinations; 2. identify emotion status and negative thoughts; 3. proceed psychological interventions; 4. provide problem solving methods | 2 months | Current | Workshops on mental disorder knowledge, counseling concepts, and techniques, with specific focus on CBT. Practice through role-play. Trainings were conducted by a qualified cognitive therapist | Six full days (three consecutive weekends) | 1. Time constraint for training; 2. under-developed training manuals and inadequate practice 3. poor patient adherence—preferred medicine over CBT; 4. no financial incentive | 1. Well designed (easy to understand the content) and organized (the use of role play) training; 2. strong learning ability and interest; 3. local community trust; 4. multi-disciplinary team | The study highlighted the feasibility and good patient acceptability of including CBT in the treatment process for the rural elderly. Remaining challenges: 1. A lack of step-by-step treatment manuals in the training; 2. a lack of support from family; 3. a need to integrate CBT intervention into public health services. |
| 16 | Xu et al. [31] | 2016; Liuyang, Hunan Province | schizophrenia | VDs; LHS: mostly family members of the patients | VD: paid; LHS: unpaid | VDs: 1. Screening, as the “686” scheme requires; 2. reported relapse signs and side effects to psychiatrists; 3. teamed up with LHSs, MHA, and psychiatrists to assist urgent care. LHSs: 1. Facilitated patient medication adherence with prompts from the e-reminders; 2. monitored for early signs of relapse and side effects using checklists from the e-monitor and report to VDs; 3. teamed up with the VDs and the township MHA to facilitate treatment adjustments and urgent care | 1 year | On-going | The built-in e-educator mHealth program sent periodic SMS messages to patients, LHSs, MHA, and VDs to educate them on schizophrenia symptoms, medication, adherence strategies, relapse, rehabilitation, and social resources | N/A | 1. Local psychiatrists with limited training may deliver inappropriate services; 2. funding for the program may not be sustainable in the future. | 1. Policy support; 2. individual and community engagement (MHAs, psychiatrists, VDs, patients and their families); VDs: No additional workload; LHSs: 1. Care and love for their families (i.e., patients) as the major job motivation; 2. non-monetary reward. | The design of the LEAN program was expected to be a cost-saving, feasible, and generalizable community-based schizophrenia management model to improve medication adherence in comparable socio-economic contexts where human and financial resources were limited. Long-term cost-effectiveness assessment is needed. |
| Cardiovascular diseases | |||||||||||||
| 17 | Ajay et al. [32] | 2014; Gongbujiang-da county, Linzhou county, Tibet Province | CVD | Community health workers(CHWs) | paid | With the smartphone-based electronic decision support, CHWs can provide 1. monthly follow-up care; 2. high-risk people identification; 3. referral; 4. therapeutic lifestyle advice (smoking cessation and salt reduction); 5. prescribe two drugs (blood pressure lowering drugs and aspirin) | 1 year | Ended | Training on the intervention protocol, including key messages on targeted CVD lifestyle risks and medications | Initial training: not mentioned; refresh training: 1–3 months after intervention began | Lack of economic and healthcare resources | Supportive national guidelines and policies on CVD prevention and control | The first study to evaluate the effects of a simplified management program delivered by CHWs with the help of electronic decision support system on improving the health of high CVD risk patients. If effective, this intervention strategy can serve as a generalized model for similar settings |
| 18 | Yan et al. [33] | 2014; Hebei, Liaoning, Ningxia, Shanxi and Shaanxi | CVD | Village Doctors | paid | 1. Identified high-risk individuals by screening all patients in the village clinics. 2. contacted patients with existing diseases or potentially at high risk to maximize screening; 3. measured blood pressure; 4. provided lifestyle modification advice; 5. monitored acute symptoms or early signs of clinical events on monthly follow-up; 4) referral | 2 years | Ended | A technical package developed to guide VDs on how to screen, identify, treat, follow-up, and refer cardiovascular high-risk individuals during their routine services. | Two 1-day sessions:1 before intervention, and again 1 month after the initiation of intervention | N/A | 1. Performance-based feedbacks and financial incentivespayment increased motivation; 2. interventions were designed to fit CVD management in resource-limited areas | This was the first cluster-randomized trial in the world to assess the population impacts of a high-risk strategy in prevention and control of CVD. The technical interventions used were all evidence-based and tailored for VDs. |
| 19 | Tian et al. [15] | 2015; Gongbu-jiangda county, Linzhou county, Tibet Province | cardiovascular disease (CVD) | Community health workers (CHWs) | paid | With the smartphone-based electronic decision support, CHWs provided 1. monthly follow-up care; 2. high-risk-patient identification; 3. referral; 4. therapeutic lifestyle advice (smoking cessation and salt reduction); prescription of two drugs (blood pressure lowering drugs and Aspirin); 5. screening for new symptoms, diseases, and side effects; 6. blood pressure measurement | 1 year | Ended | Training on the intervention protocol, including key knowledge and skill on targeted CVD lifestyle risk factors and medications. | Initial training: duration not mentioned; refresher training: 1–4 months after the intervention began | 1. The duration of the intervention was too short to observe significant health behavioral change; 2. lack of resources in remote areas | 1. Performance-based incentives. | The CHWs were capable of delivering CVD management program with smartphone-based decision support system in rural settings in China and India. |
| NCD risk factors | |||||||||||||
| 20 | Li et al. [34] | 2016; Hebei, Liaoning, Shanxi and Shaanxi provinces and the Ningxia Autonomous Region | sodium reduction | Village doctor | paid | Worked with township health educators to 1. provide health education in forms of public lectures; 2. distribute promotional materials; 3. conduct education sessions with vascular high-risk population; 4. promote salt substitute | 18 months | Ended | N/A | N/A | N/A | N/A | Population sodium intake was reduced by this intervention, through increased use of salt substitute. Larger effects could be achieved in rural China by a wholesale switch from salt to salt substitute to prevent stroke. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Long, H.; Huang, W.; Zheng, P.; Li, J.; Tao, S.; Tang, S.; Abdullah, A.S. Barriers and Facilitators of Engaging Community Health Workers in Non-Communicable Disease (NCD) Prevention and Control in China: A Systematic Review (2006–2016). Int. J. Environ. Res. Public Health 2018, 15, 2378. https://doi.org/10.3390/ijerph15112378
Long H, Huang W, Zheng P, Li J, Tao S, Tang S, Abdullah AS. Barriers and Facilitators of Engaging Community Health Workers in Non-Communicable Disease (NCD) Prevention and Control in China: A Systematic Review (2006–2016). International Journal of Environmental Research and Public Health. 2018; 15(11):2378. https://doi.org/10.3390/ijerph15112378
Chicago/Turabian StyleLong, Hongfei, Wenting Huang, Pinpin Zheng, Jiang Li, Sha Tao, Shenglan Tang, and Abu S. Abdullah. 2018. "Barriers and Facilitators of Engaging Community Health Workers in Non-Communicable Disease (NCD) Prevention and Control in China: A Systematic Review (2006–2016)" International Journal of Environmental Research and Public Health 15, no. 11: 2378. https://doi.org/10.3390/ijerph15112378
APA StyleLong, H., Huang, W., Zheng, P., Li, J., Tao, S., Tang, S., & Abdullah, A. S. (2018). Barriers and Facilitators of Engaging Community Health Workers in Non-Communicable Disease (NCD) Prevention and Control in China: A Systematic Review (2006–2016). International Journal of Environmental Research and Public Health, 15(11), 2378. https://doi.org/10.3390/ijerph15112378