Personal Network Analysis in the Study of Social Support: The Case of Chronic Pain


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Sample Description
2.3. Variables
- (a)
- Personal network structure: unlike sociocentric or complete networks, in which each member is considered to contribute equally to shaping the network structure, personal networks examine the influence on the informant (ego) of each member of a network, based on the principle that not all network members contribute equally to the phenomenon under study [35], be that behaviour, personality or social support. Personal network data were obtained regarding:Density: the percentage of ties that exist in a network out of all possible ties.Degree centrality (two measures: mean of a personal network and at node level): number of vertices adjacent to a given vertex in an asymmetric graph or the number of relations of a given person. It is a measure of network activity. An alter is highly degree central to the extent that he or she is directly connected to many other alters.Betweenness centrality (two measures: mean of a personal network and at node level): number of times a vertex occurs on a geodesic (e.g., the shortest path) connecting every other pairs in a graph. A single alter is highly between central to the extent that they lie on many geodesics (shortest paths) between alters. In this sense, they act as a bridge between alters and thus, potentially, control information, for example.Components: set of alters who are connected to one another directly or indirectly.Isolates: actors who are not connected to any other actors.
- (b)
- Personal network composition (alter characteristics): age, sex, type of tie with ego, place of residence and proximity.
- (c)
- Social support (function): type, satisfaction, reciprocity, variation over time, frequency and channel of transmission. In this specific context of chronic pain, support was considered generally: emotional support, such as the interpersonal transactions that make a person feel understood and accompanied in his or her pain; instrumental support, such as the help of other people in activities that the individual either cannot perform or for which others are required as a result of pain (e.g., help in mobility, hygiene, clothing or personal care); and informational support, such as advice or information about chronic pain that helps the subject deal with the pain (e.g., formal support resources or self-help groups and associations).
2.4. Data Collection Instruments
- (a)
- Uses a name generator able to elicit a large number of alters that distinguishes between the global personal network and the specific social support network. It allows to identify non-providers and their characteristics in terms of attributes and their position in the network structure.
- (b)
- Facilitates an analysis of different social support dimensions:
- (c)
- Facilitates the simultaneous study of micro phenomena (interactions) and meso phenomena (local structures surrounding informants, including institutions) [42], which in the specific case of social support can reveal the existence of formal social support structures such as support groups, voluntary organisations or social resources in the community, besides the support provided mainly by family, friends, neighbours and other personal contacts.
- (d)
- Determines personal network structure and composition and the characteristics of the social support contained in relationships, enabling simultaneous study of other health outcomes (e.g., quality of life, stress).
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Sociodemographic and Pain Descriptors
3.2. Experience of Pain
The pain has stopped me from living, from having a social life, from working, from being with my family, from being with my friends, because the pain stops me from getting out of the house. I don’t have a life, I go from bed to the sofa and from the sofa to bed. And being at home so much drives you crazy. Because days go by, and they’re days of your life that serve no purpose. Man, 47 years old.
I never go out, not to eat with friends, not to go for a walk, not … not even to go for a walk with my child … this last year I haven’t been out at all. Woman, 31 years old.
[…] You can’t plan or do anything, it’s … it tortures you, you get depressed, you … well I was begging them to amputate my leg as soon as I knew nothing could be done […], it’s devastating to be in so much pain, not knowing what to do, not knowing how to act … it destroys you: as a person, as a woman, as a worker, as a mother, as a wife … it completely annihilates you. Woman, 46 years old.
When I have one of my very bad days I, I … how can I say it? I don’t want to be with them. I don’t, because I feel so unwell, nothing feels good, everything looks black, and I need to be alone […]. I’m very moody. It makes me feel so powerless, I can’t do anything and nobody can do anything for me. Woman, 66 years old.
I used to go out, go walking with my friends, I looked after my daughter [cries] … it’s looking after my daughter that’s the worst thing because … I can’t give her a bath because I’d have to bend over and I can’t, fetch her from school … that’s the worst thing for me. Woman, 34 years old.
I used to have a very wide circle but not now, not for some years now, there’s no circle. Only the very closest ones are left, the people at home. Things happen to you, as they did to me, and you lock yourself away with your pain and misery, because you can’t get around like you did before […]. It’s made me distance myself in the sense of not wanting to go out. Man, 60 years old.
It affects everything around me, everything, absolutely everything. In general, friends … I don’t do much because I’m not up to it, because actually I have 8 brothers and sisters [cries], and I realise that I can’t spend an hour sitting down, I can’t lead a life like … I’d love to spend time with them. Woman, 52 years old.
The people around me, mainly. I didn’t realise until I saw that they were suffering as much as I was when they saw the state I was in (…). Yes, those around me, I understand because somehow I get … I snap and don’t realise until later … I not as patient as I ought to be, sometimes I get aggressive and say things I wouldn’t normally say given my education and my way of being … (…) and then I feel like I’m someone else, I’m not myself, and that really upsets me. Man, 65 years old.
[…] sometimes very bad, sometimes I realise that I’ve been taking it out on the first person to cross my path. And feeling ill, sometimes anything they said to me would set me off. Because I wasn’t well … you know? Yes, of course it changed me, of course it did. Woman, 66 years old.
[…] Sometimes you have to say no to certain things, because I can’t, or I can but I don’t want to because I’ll suffer for it later, so of course you limit yourself a bit … you have less social life at times, and not just you but those closest to you as well because they’re not always going to say “Well you stay at home and we’ll go”, but … Man, 46 years old.
For the two months I was in bed, I was completely helpless because they had to pick me up, carry me to the shower, wash me and then dress me and put me back to bed. Once they gave me injections I could do it for myself, but they had to sit me on a seat in the shower in order for me to be able to wash myself. I couldn’t stand. Man, 47 years old.
Housework: my husband has to help me make the bed or sometimes he has to do it himself because I can’t. Sometimes it’s the same for getting dressed, I have to tell him: help me tie this because I can’t, or get me that because I can’t, or do this because my hands aren’t strong enough. Woman, 66 years old.
When I got ill they were the ones who really helped me. They helped me a lot because sometimes I couldn’t get out of bed, I couldn’t cook […], I couldn’t even dress myself, I couldn’t do anything because the pain was so strong, I wouldn’t wish this on anyone, honestly, it was so horrible that … Man, 30 years old.
3.3. Descriptive Analysis
3.3.1. Personal Network Composition Variables
3.3.2. Personal Network Structure Variables
3.3.3. Functional Variables of Social Support
3.3.4. Relationships not Providing Social Support
- Sex: more men (N = 115, 57.79%) than women (N = 84, 42.21%) were non-providers.
- Age: non-providers presented a mean age of 46.46 years old, but encompassed both ends of the life cycle (range 1–92 years).
- Type of tie: non-providers included friends (N = 64, 32.16%), family (N = 48, 24.12%), other relatives (N = 35, 17.59%) and close family (N = 28, 14.07%), including 3 spouses, 15 siblings and 10 children. Parents formed the only social tie not represented among non-providers. To a lesser extent, neighbours (N = 13, 6.53%) and co-workers (N = 11, 5.53%) appeared among the non-providers.
- Reciprocity: the non-provider group included a higher percentage of relationships in which the ego had provided support (N = 118, 59.3%) than those in which the ego had not done so (N = 81, 40.7%).
- Variation in support over time: the absence of support was maintained over time in almost all non-provider relationships (N = 183, 91.96%), and support decreased in a small percentage of cases (N = 16, 8.04%).
- Tie strength: non-providers of support presented a weak tie with the ego (N = 101, 50.75%), although notably, the ego presented a strong tie with a similar percentage of these contacts (N = 98, 49.25%).
- Place of residence of the alter: most non-providers of support resided in the same town as the ego (N = 86, 43.22%) or in the same province (N = 80, 40.20%). A smaller percentage resided in another province (N = 25, 12.56%) or in another country (N = 8, 4.02%).
I’m a househusband and nurse because my wife is bedridden, she’s ill. […]. No, the children are only concerned with work, enjoying themselves, asking for something, but everything else? At least with me. […]. Man, 66 years old.
Let’s see, he does help me a lot [her husband], because he’s there but in my heart I don’t think he understands either… I mean, he understands that I’m in pain but at the same time he’s also very like…: well, you’ll have to cope, there’s no alternative. […] I’d like more [referring to support], I’d like much more but I can’t force people … Women, 34 years old.
[…] I’d have expected more support from her [her daughter]. She doesn’t understood me enough, either (…) I expected more support from her and more help. I think it might be because she doesn’t really believe me, because she’s also going through a bad patch […]. I’d like to think that she’s upset for me, I mean, that she doesn’t know how to help me but she does know how I am from the doctors, who’ve told her “your mother is very ill and so on”, but she doesn’t give me that impression. Maybe it’s because I don’t say anything and I need people to say it to me. Woman, 56 years old.
Yes, there’s a relationship but it’s not support … it’s different, no. We’re family but… there isn’t a relationship of, of, of … you often have more contact, more support, with a neighbour than with a family member. […] We’re sisters and we see each other almost every day but it’s not to say: you’re ill and I’m going to support you … no, no, no. I’ve had several operations and she’s never been to visit and so on, no, no. Woman, 66 years old.
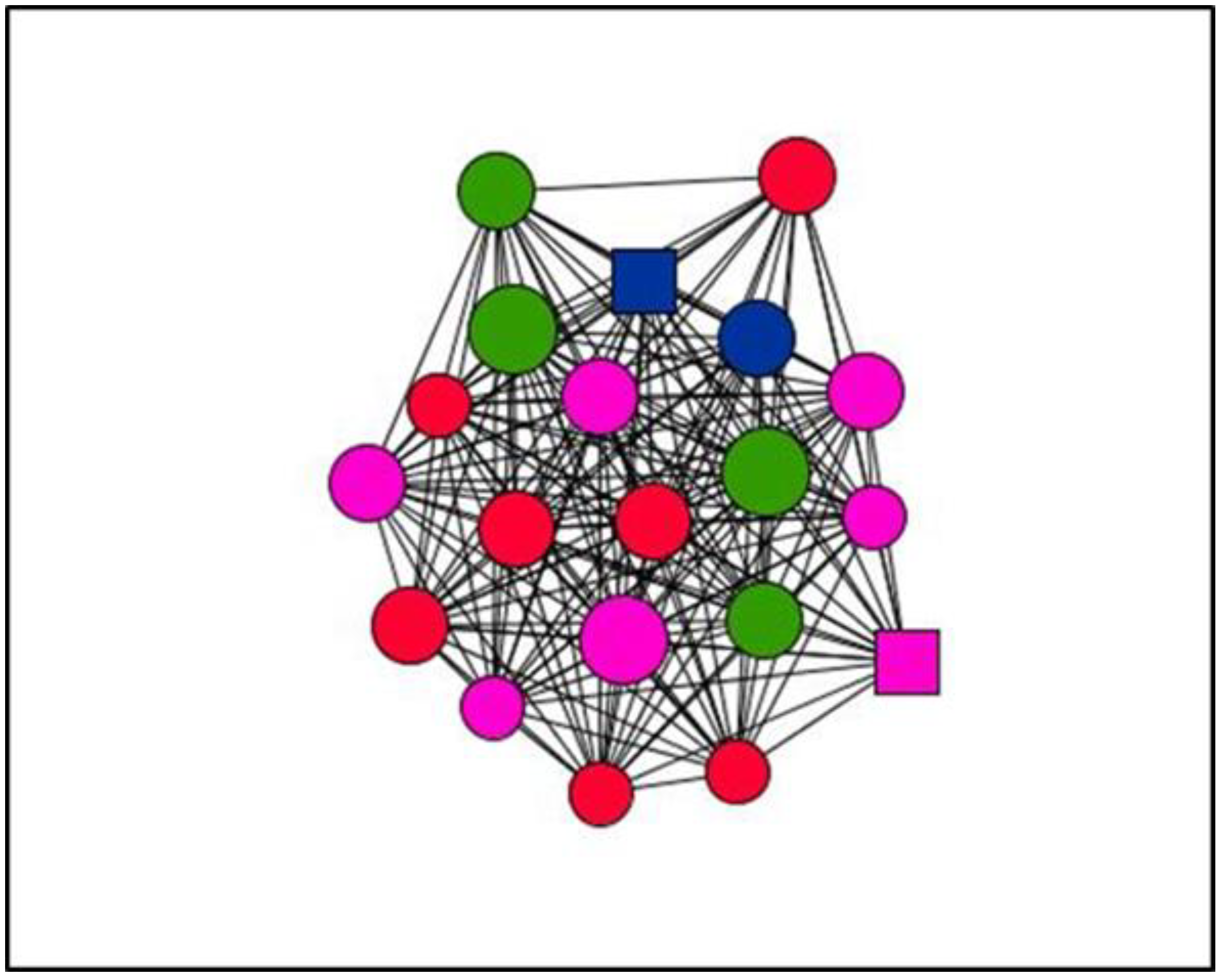
3.4. Visualisation of Personal Support Networks
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dueñas, M.; Ojeda, B.; Salazar, A.; Mico, J.A.; Failde, I. A review of chronic pain impact on patients, their social environment and the health care system. J. Pain Res. 2016, 9, 457–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannes, C.B.; Le, T.K.; Zhou, X.; Johnston, J.A.; Dworkin, R.H. The Prevalence of Chronic Pain in United States Adults: Results of an Internet-Based Survey. J. Pain 2010, 11, 1230–1239. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Collett, B.; Ventafridda, V.; Cohen, R.; Gallacher, D. Survey of chronic pain in Europe: Prevalence, impact on daily life, and treatment. Eur. J. Pain 2006, 10, 287–333. [Google Scholar] [CrossRef] [PubMed]
- Dueñas, M.; Salazar, A.; Ojeda, B.; Fernández-Palacín, F.; Micó, J.; Torres, L.; Failde, I. A Nationwide Study of Chronic Pain Prevalence in the General Spanish Population: Identifying Clinical Subgroups through Cluster Analysis. Pain Med. 2015, 16, 811–822. [Google Scholar] [CrossRef] [PubMed]
- International Association for the Study of Pain. Available online: http://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698#Pain (accessed on 16 November 2018).
- Cobb, S. Social support as a moderator of life stress. Psychosom. Med. 1976, 38, 300–314. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Barclay, L.; Schmied, V. Defining social support in context: A necessary step in improving research, intervention, and practice. Qual. Health Res. 2004, 14, 942–960. [Google Scholar] [CrossRef] [PubMed]
- Cassel, J. The contribution of the social environment to host resistance. Am. J. Epidemiol. 1976, 104, 107–123. [Google Scholar] [CrossRef] [PubMed]
- Berkman, L.F.; Glass, T.; Brissette, I.; Seeman, T.E. From social integration to health: Durkheim in the new millennium. Soc. Sci. Med. 2000, 51, 843–857. [Google Scholar] [CrossRef]
- Lin, N.; Dean, A.; Ensel, W.M. Social support scales: A methodological note. Schizophr. Bull. 1981, 7, 73–89. [Google Scholar] [CrossRef] [PubMed]
- House, J.S.; Umberson, D.; Landis, K.R. Structures and processes of social support. Annu. Rev. Sociol. 1988, 14, 293–318. [Google Scholar] [CrossRef]
- Langford, C.; Bowsher, J.; Maloney, J.; Lillis, P. Social support: A conceptual analysis. J. Adv. Nurs. 1997, 25, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, D.E. Types and timing of social support. J. Health Soc. Behav. 1986, 27, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Wills, T.A. Supportive Functions of Interpersonal Relationships. In Social Support and Health; Cohen, S., Syme, S.L., Eds.; Academic Press: San Diego, CA, USA, 1985; pp. 61–81. [Google Scholar]
- Barrera, M. Distinctions between Social Support Concepets, Measures, and Models. Am. J. Community Psychol. 1986, 14, 413–445. [Google Scholar] [CrossRef]
- Wills, T.A.; Shinar, O. Measuring Perceived and Received Social Support. In Social Support Measurement and Intervention: A Guide for Health and Social Scientists; Cohen, S., Underwood, L.G., Gottlieb, B.H., Eds.; Oxford University Press: New York, NY, USA, 2000; pp. 86–135. [Google Scholar]
- Jacobson, D. The Cultural Context of Social Support and Support Networks. Med. Anthropol. Q. 1987, 1, 42–67. [Google Scholar] [CrossRef]
- Gottlieb, B.H.; Bergen, A.E. Social support concepts and measures. J. Psychosom. Res. 2010, 69, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Luke, D.A.; Harris, J.K. Network analysis in public health: History, methods, and applications. Annu. Rev. Public Health 2007, 28, 69–93. [Google Scholar] [CrossRef] [PubMed]
- Schoen, W.; Moreland-Russell, S.; Prewitt, K.; Carothers, B.J. Social network analysis of public health programs to measure partnership. Soc. Sci. Med. 2014, 123, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Perkins, J.M.; Subramanian, S.V.; Christakis, N.A. Social networks and health: A systematic review of sociocentric network studies in low- and middle-income countries. Soc. Sci. Med. 2015, 125, 60–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, S.; de la Haye, K.; Ji, M.; An, R. Applications of social network analysis to obesity: A systematic review. Obes. Rev. 2018, 19, 976–988. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, D.R.; Simpkins, S.D. Using social network analysis to clarify the role of obesity in selection of adolescent friends. Am. J. Public Health 2014, 104, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Valente, T. Network interventions. Science 2012, 337, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Latkin, C.A.; Knowlton, A.R. Social Network Assessments and Interventions for Health Behavior Change: A Critical Review. Behav. Med. 2015, 41, 90–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinto, R.M. Using social network interventions to improve mentally ill clients’ well-being. Clin. Soc. Work J. 2006, 34, 83–100. [Google Scholar] [CrossRef] [PubMed]
- Ashida, S.; Heaney, C.A. Differential associations of social support and social connectedness with structural features of social networks and the health status of older adults. J. Aging Health 2008, 20, 872–893. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P.; Webster, C.; Shiell, A. A glossary of terms for navigating the field of social network analysis. J. Epidemiol. Community Health 2004, 58, 971–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassilev, I.; Rogers, A.; Kennedy, A.; Wensing, M.; Koetsenruijter, J.; Orlando, R.; Portillo, M.C.; Culliford, D. Social network type and long-term condition management support: A cross-sectional study in six European countries. PLoS ONE 2016, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Shiovitz-Ezra, S.; Litwin, H. Social network type and health-related behaviors: Evidence from an American national survey. Soc. Sci. Med. 2012, 75, 901–904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harasemiw, O.; Newall, N.; Shooshtari, S.; Mackenzie, C.; Menec, V. From Social Integration to Social Isolation: The Relationship Between Social Network types and perceived availability of social support in a national sample of older canadians. Res. Aging 2018, 40, 715–739. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Kang, J.Y.; Chadiha, L.A. Social Network Types, Health, and Health-Care Use among South Korean Older Adults. Res. Aging 2018, 40, 131–154. [Google Scholar] [CrossRef] [PubMed]
- Christakis, N.A.; Fowler, J.H. Social contagion theory: Examining dynamic social networks and human behavior. Stat. Med. 2013, 32, 556–577. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.P.; Christakis, N.A. Social networks and health. Annu. Rev. Sociol. 2008, 34, 405–418. [Google Scholar] [CrossRef]
- McCarty, C. Structure in Personal Networks. J. Soc. Struct. 2002, 3, 1–29. [Google Scholar]
- Hâncean, M.; Molina, J.L.; Lubbers, M.J. Recent Advancements, Developments and Applications of Personal Network Analysis. Int. Rev. Soc. Res. 2016, 6, 137–145. [Google Scholar] [CrossRef] [Green Version]
- Tardy, C. Social support Measurement. Am. J. Community Psychol. 1985, 13, 187–202. [Google Scholar] [CrossRef]
- O’Reilly, P. Methodological issues in social support and social network research. Soc. Sci. Med. 1988, 26, 863–873. [Google Scholar] [CrossRef]
- Borgatti, S.P.; Everett, M.G. Analyzing Social Networks; Sage Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- McCarty, C.; Molina, J.L.; Aguilar, C.; Rota, L. A Comparison of Social Network Mapping and Personal Network Visualization. Field Methods 2007, 19, 145–162. [Google Scholar] [CrossRef]
- Kennedy, D.P.; Green, H.D.; McCarty, C.; Tucker, J.S. Nonexperts’ Recognition of Structure in Personal Network Data. Field Methods 2011, 23, 287–306. [Google Scholar] [CrossRef] [PubMed]
- Molina, J.L. El estudio de las redes personales: Contribuciones, métodos y perspectivas. Emp. Rev. Metodol. Cienc. Soc. 2005, 10, 71–105. [Google Scholar]
- Miller, R.J.; Darlington, Y. Who supports? The providers of social support to dual-parent families caring for young children. J. Community Psychol. 2002, 30, 461–473. [Google Scholar] [CrossRef]
- Li, H.; Ji, Y.; Chen, T. The roles of different sources of social support on emotional well-being among Chinese elderly. PLoS ONE 2014, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Hough, E.S.; Magnan, M.A.; Templin, T.; Gadelrab, H.F. Social network structure and social support in HIV-positive inner city mothers. J. Assoc. Nurses AIDS Care 2005, 16, 14–24. [Google Scholar] [CrossRef] [PubMed]
- Feld, S.L.; Suitor, J.J.; Gartner, J. Describing Changes in Personal Networks over Time. Field Methods 2007, 19, 218–236. [Google Scholar] [CrossRef]
- Herz, A. Relational constitution of social support in migrants’ transnational personal communities. Soc. Netw. 2015, 40, 64–74. [Google Scholar] [CrossRef]
- Fernández, M. Social support networks in Spain: The factors that determine models of choice. Int. Sociol. 2012, 27, 384–402. [Google Scholar] [CrossRef]
- Mok, D.; Wellman, B. Did distance matter before the Internet? Interpersonal contact and support in the 1970s. Soc. Netw. 2007, 29, 430–461. [Google Scholar] [CrossRef]
- Weiner, A.S.B.; Hannum, J.W. Differences in the quantity of social support between geographically close and long-distance friendships. J. Soc. Pers. Relat. 2012, 30, 662–672. [Google Scholar] [CrossRef]
- Seeman, T.E.; Berkman, L.F. Structural characteristics of social networks and their relationship with social support in the elderly: Who provides support. Soc. Sci. Med. 1988, 26, 737–749. [Google Scholar] [CrossRef]
- Pearlin, L.I. Social structure and processes of social support. In Social Support and Health; Cohen, S.L., Syme, S.L., Eds.; Academic Press: San Diego, CA, USA, 1985; pp. 43–63. [Google Scholar]
- Agneessens, F.; Waege, H.; Lievens, J. Diversity in social support by role relations: A typology. Soc. Netw. 2006, 28, 427–441. [Google Scholar] [CrossRef]
- Strunin, L.; Boden, L.I. Family consequences of chronic back pain. Soc. Sci. Med. 2004, 58, 1385–1393. [Google Scholar] [CrossRef]
- DeLongis, A.; Capreol, M.; Holtzman, S.; O’Brien, T.; Campbell, J. Social Support and Social Strain Among Husbands and Wives: A Multilevel Analysis. J. Fam. Psychol. 2004, 18, 470–479. [Google Scholar] [CrossRef] [PubMed]
- Rook, K.S. The negative side of social interaction: Impact on psychological well-being. J. Pers. Soc. Psychol. 1984, 46, 1097–1108. [Google Scholar] [CrossRef] [PubMed]
- Rook, K.S. Exposure and reactivity to negative social exchanges: A preliminary investigation using daily diary data. J. Gerontol. 2003, 58, P100–P111. [Google Scholar] [CrossRef]
- Sapin, M.; Widmer, E.; Iglesias, K. From support to overload: Patterns of positive and negative family relationships of adults with mental illness over time. Soc. Netw. 2016, 47, 59–72. [Google Scholar] [CrossRef]
- Newsom, J.T.; Rook, K.S.; Nishishiba, M.; Sorkin, D.H.; Mahan, T.L. Understanding the relative importance of positive and negative social exchanges: Examining specific domains and appraisals. J. Gerontol. 2005, 60, 304–312. [Google Scholar] [CrossRef]
- Baruch-Feldman, C.; Brondolo, E.; Ben-Dayan, D.; Schwartz, J. Sources of social support and burnout, job satisfaction, and productivity. J. Occup. Health Psychol. 2002, 7, 84–93. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Stoner, M. Burnout and turnover intention among social workers: Effects of role stress, job autonomy and social support. Adm. Soc. Work 2008, 32, 5–25. [Google Scholar] [CrossRef]
- Nissly, J.; Barak, M.M.; Levin, A. Stress, Social Support, and Workers’ Intentions to Leave Their Jobs in Public Child Welfare. Adm. Soc. Work 2004, 29, 79–100. [Google Scholar] [CrossRef]
- House, J.S. Social Support and Social Structure. Sociol. Forum 1987, 2, 135–146. [Google Scholar] [CrossRef]
- Robertson, S.M.; Zarit, S.H.; Duncan, L.G.; Rovine, M.J.; Femia, E.E. Family caregivers’ patterns of positive and negative affect. Fam. Relat. 2007, 56, 12–23. [Google Scholar] [CrossRef]
- Adelman, R.D.; Tmanova, L.; Delgado, D.; Dion, S.; Lachs, M.S. Caregiver Burden: A Clinical Review. J. Am. Med. Assoc. 2014, 311, 1052–1060. [Google Scholar] [CrossRef] [PubMed]
- Rodakowski, J.; Skidmore, E.R.; Rogers, J.C.; Schulz, R. Role of social support in predicting caregiver burden. Arch. Phys. Med. Rehabil. 2012, 93, 2229–2236. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | Median | SD | Min. | Max. | ||
|---|---|---|---|---|---|---|
| Density | Men | 0.4 | 0.4 | 0.2 | 0.1 | 0.7 |
| Women | 0.5 | 0.4 | 0.2 | 0.2 | 1 | |
| Total | 0.6 | 0.4 | 0.2 | 0.1 | 1 | |
| Degree centrality | Men | 8.2 | 8.0 | 3.3 | 2.6 | 13.5 |
| Women | 9.0 | 7.6 | 4.3 | 3.10 | 18.1 | |
| Total | 8.6 | 8 | 3.8 | 2.6 | 18.1 | |
| Betweenness centrality | Men | 3.7 | 3.5 | 2.8 | 0.1 | 10.8 |
| Women | 4.3 | 4.3 | 2.0 | 0.5 | 8.8 | |
| Total | 4 | 3.9 | 2.4 | 0.1 | 10.8 | |
| Components | Men | 2.9 | 2.0 | 2.6 | 1.0 | 11.0 |
| Women | 2.2 | 2.0 | 1.6 | 1.0 | 6.0 | |
| Total | 2.5 | 2.0 | 2.2 | 1.0 | 11.0 | |
| Isolates | Men | 1.3 | 0.00 | 2.5 | 0.0 | 9.0 |
| Women | 0.9 | 0.0 | 1.4 | 0.0 | 5.0 | |
| Total | 1.1 | 0.0 | 2 | 0 | 9 |
| Variable | Category | N (%) |
|---|---|---|
| Characteristics of personal relationships in terms of social support (N = 600) | ||
| Satisfaction | Very satisfactory | 74 (12.3) |
| Quite satisfactory | 132 (22) | |
| Satisfactory | 156 (26) | |
| Quite unsatisfactory | 39 (6.5) | |
| Very unsatisfactory | 199 (33.2) | |
| Variation | No change | 450 (75) |
| Has increased | 82 (13.7) | |
| Has decreased | 68 (11.3) | |
| Reciprocity | Yes | 458 (76.3) |
| No | 142 (23.7) | |
| Characteristics of social support in provider relationships (N = 401) | ||
| Type | Emotional | 255 (63.6) |
| Instrumental | 16 (4.0) | |
| Informational | 5 (1.2) | |
| All three types of support | 22 (5.5) | |
| Emotional and instrumental | 84 (21) | |
| Emotional and informational | 14 (3.5) | |
| Instrumental and informational | 1 (0.2) | |
| Health professionals | 4 (1) | |
| Frequency | Daily | 122 (30.4) |
| Weekly | 145 (36.2) | |
| Fortnightly | 47 (11.7) | |
| Monthly | 57 (14.2) | |
| Every 2–3 months | 16 (4.0) | |
| Every 3 months or so | 14 (3.5) | |
| Channel of transmission | In person | 192 (47.9) |
| Telephone | 63 (15.7) | |
| Internet | 8 (2) | |
| In person and telephone | 134 (33.4) | |
| Telephone and internet | 4 (1) | |
| Mean | Median | SD | Min. | Max. | |
|---|---|---|---|---|---|
| Non-providers: degree centrality | 7.3 | 8 | 4.8 | 0 | 18 |
| Degree centrality (total) | 8.6 | 9 | 5.4 | 0 | 19 |
| Non-providers: betweenness centrality | 2.1 | 0.2 | 5.3 | 0 | 38.7 |
| Betweenness centrality (total) | 4 | 0.33 | 10.1 | 0 | 114.3 |
| Node Shape: Sex | Node Size: Satisfaction | Node Colour: Type of Social Support | |
|---|---|---|---|
| Circle: woman Square: man | Large: more satisfaction Small: less satisfaction | Emotional: red Instrumental: blue Informational: yellow All types: green | Non-providers: black Emotional and instrumental: pink Emotional and informational: orange Instrumental and informational: grey |
| Variables | Categories | Case 2 N (%) | Case 24 N (%) | Case 7 N (%) | Case 26 N (%) |
|---|---|---|---|---|---|
| Satisfaction | Very satisfactory | 3 (15) | 3 (15) | 4 (20) | 2 (10) |
| Quite satisfactory | - | 10 (50) | 1 (5) | 6 (30) | |
| Satisfactory | 7 (35) | 7 35) | 2 (10) | 5 (25) | |
| Quite unsatisfactory | 5 (25) | - | - | 1 (5) | |
| Very unsatisfactory | 5 (25) | - | 13 (65) | 6 (30) | |
| Variation | No change | 7 (35) | 18 (90) | 17 (85) | 12(60) |
| Has increased | 10 (50) | 1 (5) | 1(5) | 8 (40) | |
| Has decreased | 3 (15) | 1 (5) | 2(10) | - | |
| Reciprocity | Yes | 18 (90) | 18 (90) | 10 (50) | 11 (55) |
| No | 2 (10) | 2 (10) | 10 (50) | 9 (45) | |
| Types of support | Emotional | 13 (65) | 7 (35) | 6 (30) | 6 (30) |
| Instrumental | - | 2 (10) | - | 1 (5) | |
| Informational | - | - | - | 1(5) | |
| All three types of support | - | 4 (20) | - | 2 (10) | |
| Emotional and instrumental | 2 (10) | 7 (35) | 1 (5) | 2 (10) | |
| Emotional and informational | - | - | - | 1(5) | |
| Instrumental and informational | - | - | - | 1(5) | |
| Health professionals | - | - | - | - | |
| Non-Providers | 5 (25) | - | 13 (65) | 6 (30) | |
| Frequency | Daily | 3 (15) | 10 (50) | 5 (25) | 4 (20) |
| Weekly | 5 (25) | 10 (50) | 2 (10) | 6 (30) | |
| Fortnightly | 2 (10) | - | - | 1 (5) | |
| Monthly | 5 (25) | - | - | 1 (5) | |
| Every 2–3 months | - | - | - | 1 (5) | |
| Every 3 months or so | - | - | - | 1 (5) | |
| Non-providers | 5 (25) | - | 13 (65) | 6 (30) | |
| Channel of transmission | In person | 2 (10) | 13 (65) | 1 (5) | 10 (50) |
| Telephone | 12 (60) | 1 (5) | 1 (5) | 1 (5) | |
| Internet | 1 (5) | - | - | - | |
| In person and telephone | - | 6 (30) | 5 (25) | 1(5) | |
| Telephone and internet | - | - | - | 2 (10) | |
| Non-providers | 5 (25) | - | 13 (65) | 6 (30) |
| Case 2 | Case 24 | Case 07 | Case 26 | |
|---|---|---|---|---|
| Density | 0.6 | 1 | 0.4 | 0.2 |
| Degree centrality (mean) | 10.4 | 18.1 | 8.2 | 3.6 |
| Betweenness centrality (mean) | 4.3 | 0.5 | 1.9 | 8 |
| Components | 1 | 1 | 5 | 4 |
| Isolates | 0 | 0 | 4 | 3 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fernández-Peña, R.; Molina, J.L.; Valero, O. Personal Network Analysis in the Study of Social Support: The Case of Chronic Pain. Int. J. Environ. Res. Public Health 2018, 15, 2695. https://doi.org/10.3390/ijerph15122695
Fernández-Peña R, Molina JL, Valero O. Personal Network Analysis in the Study of Social Support: The Case of Chronic Pain. International Journal of Environmental Research and Public Health. 2018; 15(12):2695. https://doi.org/10.3390/ijerph15122695
Chicago/Turabian StyleFernández-Peña, Rosario, José Luis Molina, and Oliver Valero. 2018. "Personal Network Analysis in the Study of Social Support: The Case of Chronic Pain" International Journal of Environmental Research and Public Health 15, no. 12: 2695. https://doi.org/10.3390/ijerph15122695
APA StyleFernández-Peña, R., Molina, J. L., & Valero, O. (2018). Personal Network Analysis in the Study of Social Support: The Case of Chronic Pain. International Journal of Environmental Research and Public Health, 15(12), 2695. https://doi.org/10.3390/ijerph15122695