Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks



Abstract
:1. Introduction
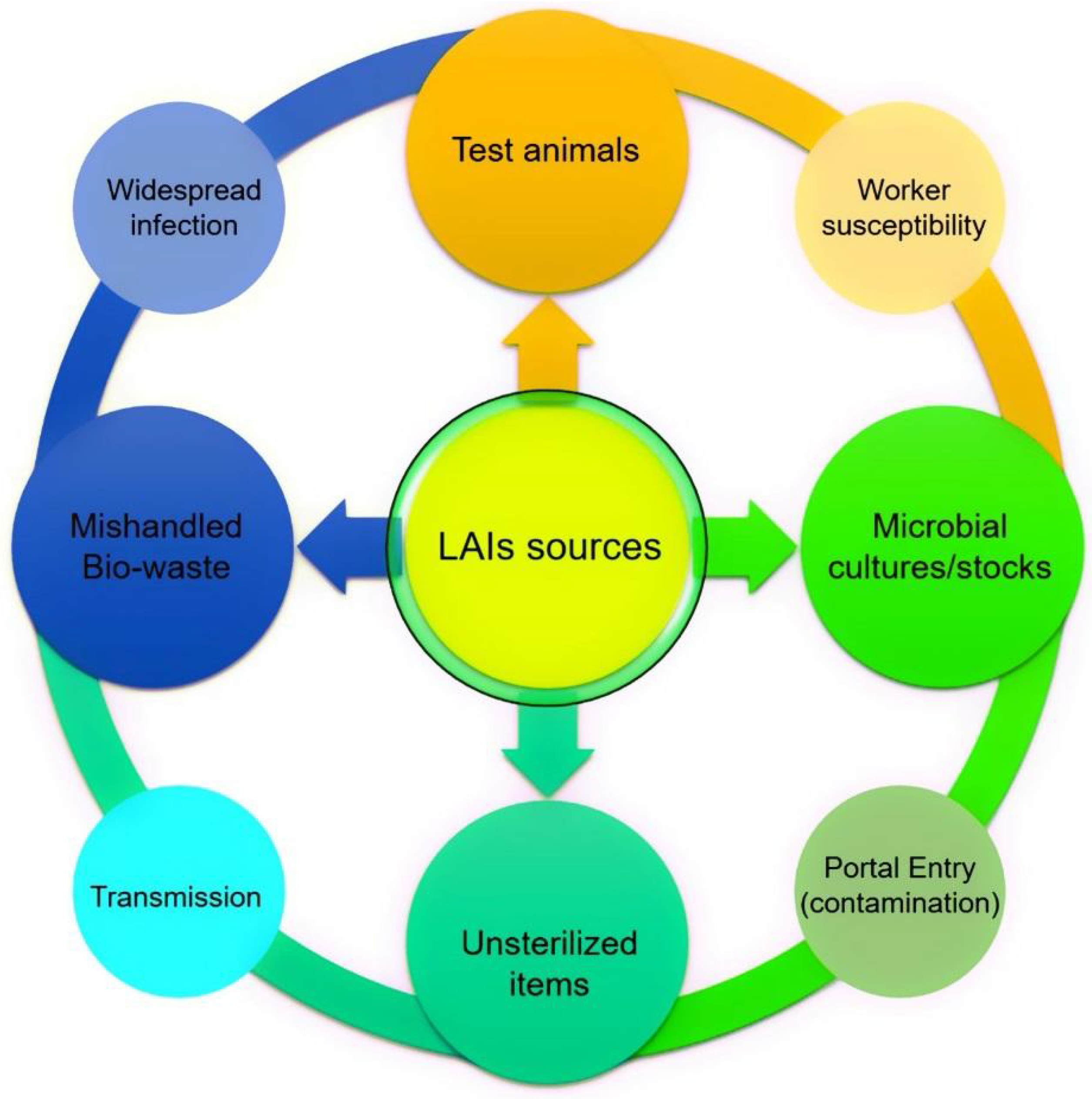
2. LAIs and Associated Risks
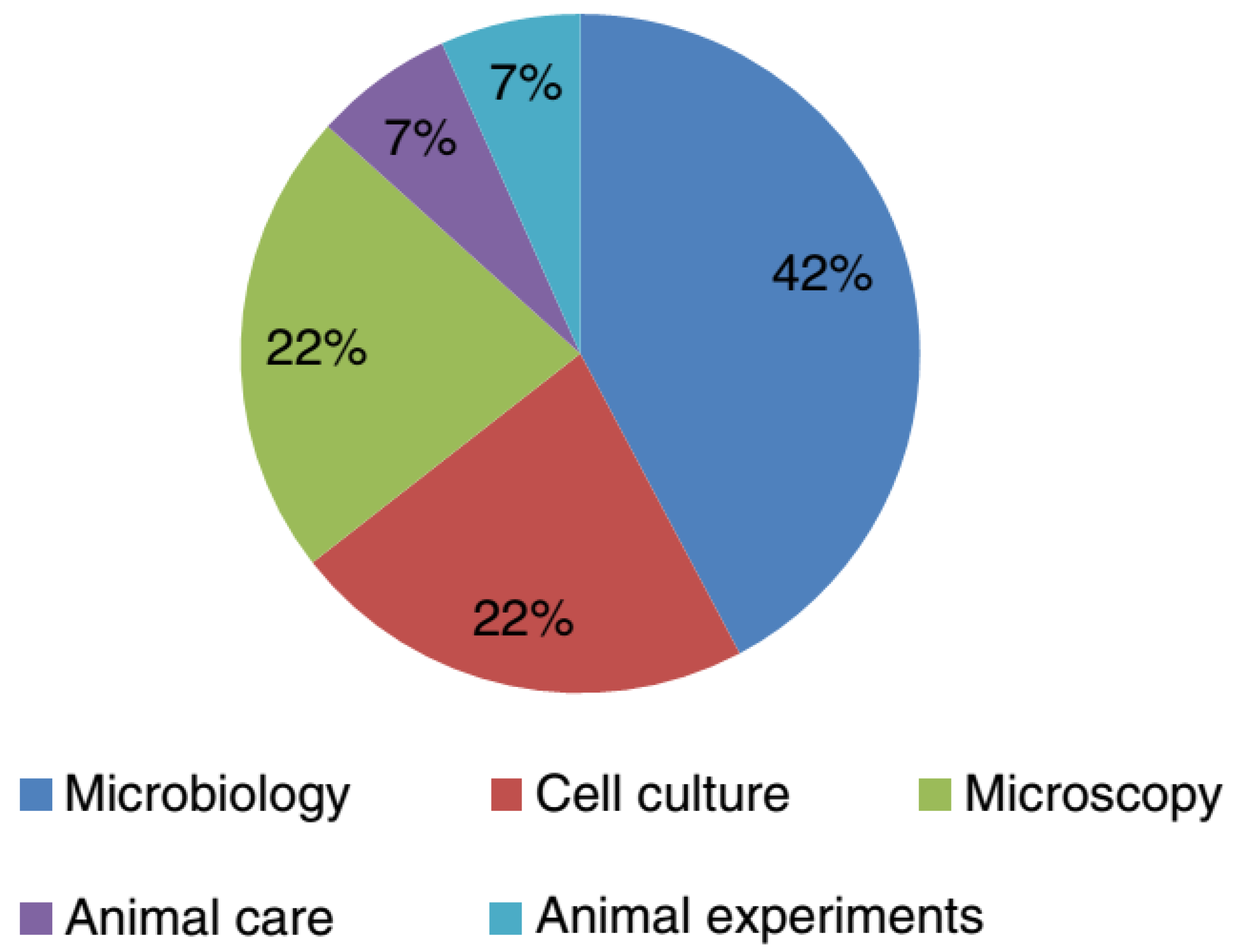
3. Studies of Laboratory-Acquired Infections (LAIs)
4. Specific Laboratory-Acquired Infections and Prevention
4.1. Laboratory-Acquired Brucellosis and Prevention Strategies
4.2. Laboratory-Acquired Tuberculosis and Prevention Strategies
4.3. Other Bacterial-Associated LAIs and Prevention Strategies
4.4. Viral-Associated LAIs and Prevention Strategies
4.5. Parasites Associated LAIs and Prevention Strategies
4.6. Fungal-Associated LAIs and Prevention Strategies
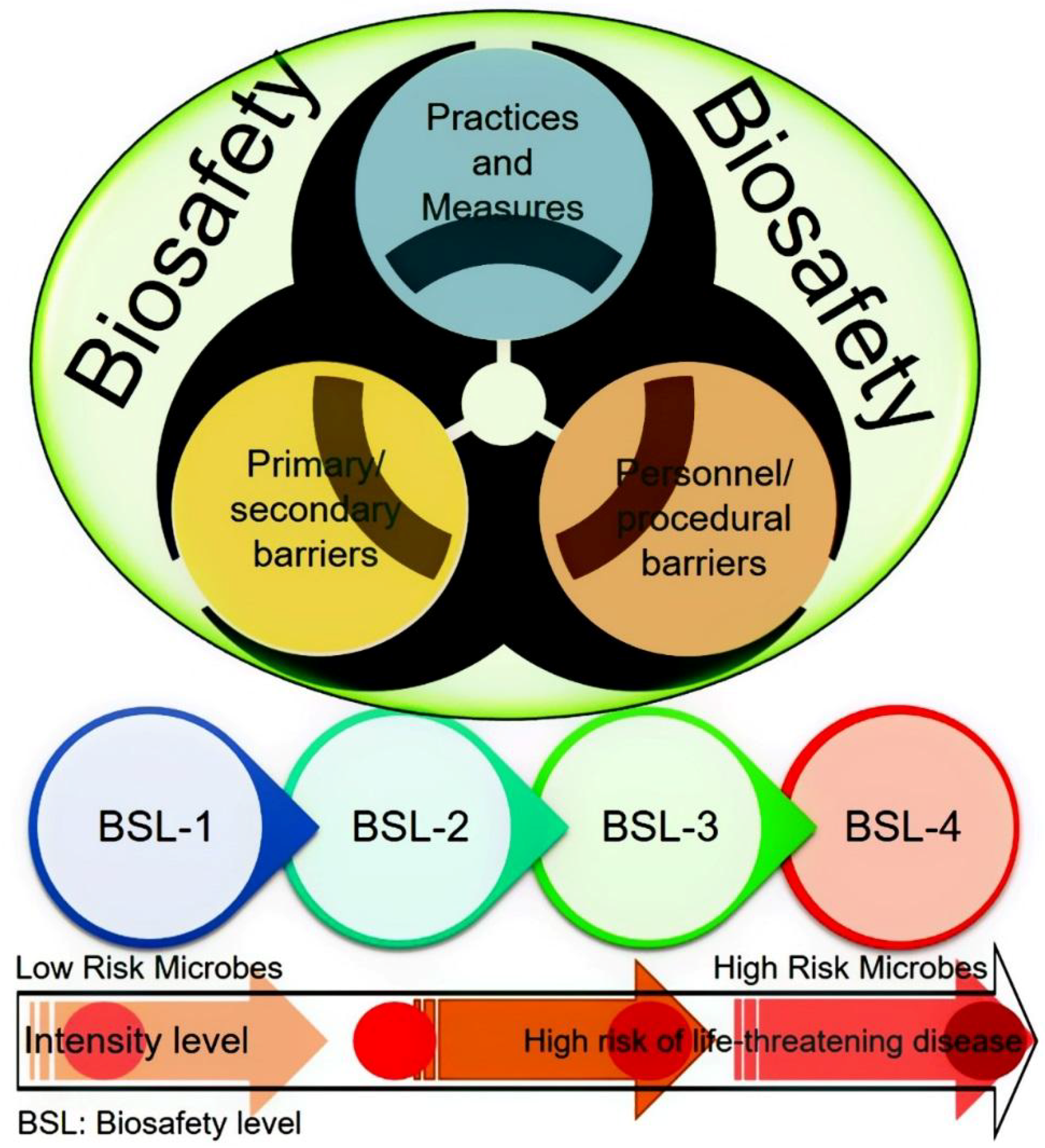
5. Biological Risk Classification and Prevention Strategies
6. Lessons Learned and Future Perspectives
7. Concluding Remarks and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kimman, T.G.; Smit, E.; Klein, M.R. Evidence-based biosafety: Are view of the principles and effectiveness of microbiological containment measures. Clin. Microbiol. Rev. 2008, 21, 403–425. [Google Scholar] [CrossRef] [PubMed]
- Lacroix, G. Literature Review of Laboratory-Acquired Infections in Canada and the United States between 2000 and 2009 (PowerPoint presentation). Available online: http://biosafety.icid.com/en/files/presentations/Literature-Review-%20Laboratory-Acquired-Infections-Canada-US-2000-2009.pdf (accessed on 24 September 2017).
- Coelho, A.C.; García Díez, J. Biological risks and laboratory-acquired infections: A reality that cannot be ignored in health biotechnology. Front. Bioeng. Biotechnol. 2015, 3, 56. [Google Scholar] [CrossRef] [PubMed]
- Blacksell, S.D.; Robinson, M.T.; Newton, P.N.; Day, N.P. Laboratory-acquired Scrub Typhus and Murine Typhus Infections: The Argument for a Risk-based Approach to Biosafety Requirements for Orientia tsutsugamushi and Rickettsia typhi Laboratory Activities. Clin. Infect. Dis. 2018. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.F.; Eddie, B. Laboratory infections due to Brucella. J. Infect. Dis. 1897, 68, 24–32. [Google Scholar]
- Zaki, A.N. Biosafety and biosecurity measures: Management of biosafety level 3 facilities. Int. J. Antimicrob. Agents 2010, 36, S70–S74. [Google Scholar] [CrossRef] [PubMed]
- Herfst, S.; Osterhaus, A.D.M.E.; Fouchier, R.A.M. The future of research and publication on altered H5N1 viruses. J. Infect. Dis. 2012, 205, 1628–1631. [Google Scholar] [CrossRef] [PubMed]
- Casadevall, A.; Imperiale, M.J. Risks, and benefits of gain-of function experiments with pathogens of pandemic potential, such as influenza virus: A call for a science-based discussion. mBio 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Lipsitch, M.; Inglesby, T.V. Reply to ‘studies on influenza virus transmission between ferrets: The public health risks revisited’. mBio 2015, 6. [Google Scholar] [CrossRef] [PubMed]
- Doherty, P.C.; Thomas, P.G. Dangerous for ferrets: Lethal for humans? BMC Biol. 2012, 10, 10. [Google Scholar] [CrossRef] [PubMed]
- Bakanidze, L.; Imnadze, P.; Perkins, D. Biosafety and biosecurity as essential pillars of international health security and cross-cutting elements of biological nonproliferation. BMC Public Health 2010, 10 (Suppl. 1), S12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baltz, R.H.; Davies, J.E.; Demain, A.L. Manual of Industrial Microbiology and Biotechnology; ASM Press: Washington, DC, USA, 2010. [Google Scholar]
- Wei, Q.; Li, X.Y.; Wang, L.; Lu, X.C.; Jiang, M.N.; Wu, G.Z.; Hou, P.S. Preliminary studies on pathogenic microorganisms laboratory-acquired infections cases in recent years and its control strategies. Chin. J. Exp. Clin. Virol. 2011, 25, 390–392. [Google Scholar]
- Nisii, C.; Castilletti, C.; Raoul, H.; Hewson, R.; Brown, D.; Gopal, R.; Eickmann, M.; Gunther, S.; Mirazimi, A.; Koivula, T.; et al. Biosafety Level-4 laboratories in Europe: Opportunities for public health, diagnostics, and research. PLoS Pathog. 2013, 9, e1003105. [Google Scholar] [CrossRef] [PubMed]
- Traxler, R.M.; Lehman, M.W.; Bosserman, E.A.; Guerra, M.A.; Smith, T.L. A literature review of laboratory-acquired brucellosis. J. Clin. Microbiol. 2013, 51, 3055–3062. [Google Scholar] [CrossRef] [PubMed]
- Riyesh, T.; Karuppusamy, S.; Bera, B.C.; Barua, S.; Virmani, N.; Yadav, S.; Vaid, R.K.; Anand, T.; Bansal, M.; Malik, P.; et al. Laboratory-acquired buffalo pox virus infection, India. Emerg. Infect. Dis. 2014, 20, 325–327. [Google Scholar] [CrossRef] [PubMed]
- Siengsanan-Lamont, J.; Blacksell, S.D. A Review of Laboratory-Acquired Infections in the Asia-Pacific: Understanding Risk and the Need for Improved Biosafety for Veterinary and Zoonotic Diseases. Trop. Med. Infect. Dis. 2018, 3, 36. [Google Scholar] [CrossRef] [PubMed]
- American Biological Safety Association. Laboratory-Acquired Infection (LAI) Database. 2017. Available online: https://my.absa.org/LAI (accessed on 23 January 2018).
- Johnson, B. OSHA infectious dose white paper. Appl. Biosaf. 2003, 8, 160–165. [Google Scholar] [CrossRef]
- Singh, K. It’s time for a centralized registry of laboratory-acquired infections. Nat. Med. 2011, 17, 919. [Google Scholar] [CrossRef] [PubMed]
- Pike, R.M. Laboratory-associated infections: Summary and analysis of 3921 cases. Health Lab. Sci. 1976, 13, 105–114. [Google Scholar] [PubMed]
- Pike, R.M. Past and present hazards of working with infectious agents. Arch. Pathol. Lab. Med. 1978, 102, 333–336. [Google Scholar] [PubMed]
- Pike, R.M. Laboratory-associated infections: Incidence, fatalities, causes, and prevention. Annu. Rev. Microbiol. 1979, 33, 41–66. [Google Scholar] [CrossRef] [PubMed]
- Walker, D.; Campbell, D. A survey of infections in United Kingdom laboratories, 1994–1995. J. Clin. Pathol. 1999, 52, 415–418. [Google Scholar] [CrossRef] [PubMed]
- Jacobson, J.T.; Orlob, R.B.; Clayton, J.L. Infections acquired in clinical laboratories in Utah. J. Clin. Microbiol. 1985, 21, 486–489. [Google Scholar] [PubMed]
- Baron, E.J.; Miller, J.M. Bacterial and fungal infections among diagnostic laboratory workers: Evaluating the risks. Diagn. Microbiol. Infect. Dis. 2008, 60, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Grist, N.R.; Emslie, J.A.N. Infections in British clinical laboratories, 1988–1989. J. Clin. Pathol. 1991, 44, 667–669. [Google Scholar] [CrossRef] [PubMed]
- Harding, A.L.; Byers, K.B. Laboratory-associated infections: Summary and analysis of 3921 cases. In Biological Safety: Principles and Practices, 4th ed.; Fleming, D.O., Hunt, D.L., Eds.; ASM Press: Washington, DC, USA, 2006; pp. 53–77. [Google Scholar]
- Knudsen, A.; Kronborg, G.; Dahl Knudsen, J.; Lebech, A.M. Laboratory exposure to Brucella melitensis in Denmark: A prospective study. J. Hosp. Infect. 2013, 85, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Dentinger, C.M.; Jacob, K.; Lee, L.V.; Mendez, H.A.; Chotikanatis, K.; McDonough, P.L.; Campagnolo, E.R. Human Brucella canis infection and subsequent laboratory exposures associated with a puppy, New York City, 2012. Zoonoses Public Health 2015, 62, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Byers, K.B. Laboratory-acquired infections (PowerPoint presentation). In Proceedings of the 60th Annual Biological Safety Conference, Albuquerque, NM, USA, 13–18 October 2017. [Google Scholar]
- Ergönül, O.; Celikbas, A.; Tezeren, D.; Güvener, E.; Dokuzoguz, B. Analysis of risk factors for laboratory-acquired Brucella infections. J. Hosp. Infect. 2004, 56, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Sam, I.C.; Karunakaran, R.; Kamarulzaman, A.; Ponnampalavanar, S.; Syed Omar, S.F.; Ng, K.P.; Yusof, M.M.; Hooi, P.S.; Jafar, F.L.; Abubakar, S. A large exposure to Brucella melitensis in a diagnostic laboratory. J. Hosp. Infect. 2012, 80, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, R.A.; Singh, K. Laboratory-acquired infections. Clin. Infect. Dis. 2009, 49, 142–147. [Google Scholar]
- Collins, C.H.; Grange, J.M. Tuberculosis acquired in laboratories and necropsy rooms. Commun. Dis. Public Health 1999, 2, 161–167. [Google Scholar] [PubMed]
- Wurtz, N.; Papa, A.; Hukic, M.; Di Caro, A.; Leparc-Goffart, I.; Leroy, E.; Busquets, N. Survey of laboratory-acquired infections around the world in biosafety level 3 and 4 laboratories. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 1247–1258. [Google Scholar] [CrossRef] [PubMed]
- Pfyffer, GE. Mycobacterium: General characteristics. In Manual of Clinical Microbiology, 9th ed.; Murray, P.R., Baron, E.J., Jorgensen, J.H., Landry, M.L., Pfaller, M.A., Eds.; American Society of Microbiology: Washington, DC, USA, 2007. [Google Scholar]
- Lam, S.T.; Sammons-Jackson, W.; Sherwood, J.; Ressner, R. Laboratory- acquired tularemia successfully treated with ciprofloxacin: A case report. Infect. Dis. Clin. Pract. 2012, 20, 204–207. [Google Scholar] [CrossRef]
- Bouza, E.; Sánchez-Carrillo, C.; Hernan-Gómez, S.; González, M.J. Spanish co-operative group for the study of laboratory-acquired brucellosis. Laboratory-acquired brucellosis: A Spanish national survey. J. Hosp. Infect. 2005, 61, 80–83. [Google Scholar] [CrossRef] [PubMed]
- Gaidamovich, S.Y.; Butenko, A.M.; Leschinskaya, H.V. Human laboratory acquired arbo-, arena-, and Hantavirus infections. Appl. Biosaf. 2000, 5, 5–11. [Google Scholar] [CrossRef]
- Britton, S.; van den Hurk, A.F.; Simmons, R.J.; Pyke, A.T.; Northill, J.A.; McCarthy, J.; McCormack, J. Laboratory-acquired dengue virus infection—A case report. PLoS Negl. Trop. Dis. 2011, 5, e1324. [Google Scholar] [CrossRef] [PubMed]
- Wei, Q.; Jiang, M.N.; Han, J.; Wang, Z.J. Immune control strategies for vaccinia virus-related laboratory-acquired infections. Biomed. Environ. Sci. 2014, 27, 142–146. [Google Scholar] [PubMed]
- Sewell, D.L. Laboratory associated infections and biosafety. Clin. Microbiol. Rev. 1995, 8, 389–405. [Google Scholar] [CrossRef] [PubMed]
- West, DL. The risk of hepatitis B infection among health care professionals in the United States: A. review. Am. J. Med. Sci. 1984, 287, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Wasley, A.; Grytdal, S.; Gallagher, K. Surveillance for acute viral hepatitis—United States, 2006. Morb. Mortal. Wkly. Rep. 2008, 57, 1–24. [Google Scholar]
- Centers for Disease Control and Prevention. Surveillance for occupationally acquired HIV infection—United States, 1981–1992. Morb. Mortal. Wkly. Rep. 1992, 41, 823–825. [Google Scholar]
- Lipsitch, M.; Bloom, B.R. Rethinking biosafety in research on potential pandemic pathogens. mBio 2012, 3. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita-Yanaga, A.T.; Toledo, M.J.D.O.; Araújo, S.M.D.; Vier, B.P.; Gomes, M.L. Accidental infection by Trypanosoma cruzi follow-up by the polymerase chain reaction: Case report. Rev. Inst. Med. Trop. São Paulo 2009, 51, 295–298. [Google Scholar] [CrossRef]
- Felintode Brito, M.E.; Andrade, M.S.; deAlmeida, É.L.; Medeiros, Â.C.R.; Werkhäuser, R.P.; Araújo, A.I.F.D.; Brandão-Filho, S.P.; Paiva de Almeida, A.M.; Gomes Rodrigues, E.H. Occupationally acquired American cutaneous leishmaniasis. Case Rep. Dermatol. Med. 2012, 2012, 279517. [Google Scholar] [CrossRef] [PubMed]
- Herwaldt, B.L. Laboratory-acquired parasitic infections form accidental exposures. Clin. Microbiol. Rev. 2001, 14, 659–688. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.P.; Dubey, J.P.; Moutinho, O.; Gargaté, M.J.; Vilares, A.; Rodrigues, M.; Cardoso, L. Seroepidemiology of Toxoplasma gondii infection in women from the North of Portugal in their child bearing years. Epidemiol. Infect. 2012, 140, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Bosia, A. Health risks and benefits from biotechnology. In Women in Biotechnology; Molfino, F., Zucco, F., Eds.; Springer: Basel, Switzerland, 2008; pp. 303–314. [Google Scholar]
- Corrao, C.R.N.; Mazzotta, A.; Torre, G.L.; Giusti, M.D. Biological risk and occupational health. Ind. Health 2012, 50, 326–337. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Additional laboratory hazards–Noise. In Laboratory Biosafety Manual, 3rd ed.; WHO Library Cataloguing-in-Publication Data: Geneva, Switzerland, 2004. [Google Scholar]
- Shinnick, T.M.; Gilpin, C. A risk assessment-based approach to defining minimum biosafety precautions for tuberculosis laboratories in resource-limited settings. App. Biosaf. 2012, 17, 6. [Google Scholar] [CrossRef]
- Sture, J.; Whitby, S.; Perkins, D. Biosafety, biosecurity and internationally mandated regulatory regimes: Compliance mechanisms for education and global health security. Med. Conf. Surviv. 2013, 29, 289–321. [Google Scholar] [CrossRef] [PubMed]
- Hackney, R.W.; Myatt, T.A.; Gilbert, K.M.; Caruso, R.R.; Simon, S.L. Current trends in institutional biosafety committee practices. Appl. Biosaf. 2012, 17, 11–18. [Google Scholar] [CrossRef]
- Rusnak, J.M.; Kortepeter, M.G.; Hawley, R.J.; Anderson, A.O.; Boudreau, E.; Eitzen, E. Rick of occupationally acquired illness from biologi- cal threat agents in unvaccinated laboratory workers. Biosecur. Bioterror. 2004, 2, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Mourya, D.T.; Yadav, P.D.; Majumdar, T.D.; Chauhan, D.S.; Katoch, V.M. Establishment of biosafety level-3 (BSL-3) laboratory: Important criteria to consider while designing, constructing, commissioning & operating the facility in Indian setting. Indian J. Med. Res. 2014, 140, 171. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Year | Country | Microorganism | Affected Worker | Laboratory Type/Level |
|---|---|---|---|---|
| 2016 | Taiwan | Ralstonia pickettii | - | - |
| 2014 | South Korea | Dengue | Laboratory staff | Research/BSL2 |
| 2011 | Australia | Dengue | Scientist | Research/BSL2 |
| 2010 | India | Buffalopox virus (BPXV) (Z) | Researcher | - |
| 2009 | Malaysia | Brucella melitensis | Laboratory staff | Clinical |
| 2006 | Taiwan | Shigella spp. (Z) | Graduate student | Research |
| 2006 | PR China | Seoul virus and hantavirus (Z) | 8 postgraduate students | Research |
| 2004 | Taiwan | Dengue type 1 | Graduate student | Research |
| 2004 | Taiwan | SARS-CoV (Z) | Researcher | Research |
| 2004 | PR China | SARS-CoV (Z) | 8 human cases, 1 died | Research |
| 2003 | Singapore | SARS-CoV (Z) | Graduate student | Research/BSL3 |
| 2002 | Taiwan | Arthroderma benhamiae (Z) | Scientist | Research |
| 2002 | Australia | S. aureus, MRSA, EMRSA (Z) | Laboratory staff | Clinical |
| 2001 | Japan | Arthroderma benhamiae (Z) | Researcher | Research |
| 2000 | South Korea | Orientia tsutsugamushi (Z) | Worker | - |
| 1999 | Taiwan | Vibrio parahaemolyticus (Z) | Laboratory staff | - |
| 1998 | Japan | Helicobacter pylori (Z) | Bacteriologist | - |
| 1996–2000 | Australia | Brucella suis (Z) | Various | Clinical |
| 1996 | Malaysia | Salmonella typhi | Laboratory staff | - |
| 1992 | Australia | Pseudomonas pseudomallei (Z) | 3 Laboratory staff | Diagnostic |
| 1990 | South Korea | Rickettsia typhi (Z) | Laboratory staff | Clinical |
| 1990 | India | Mycobacterium leprae (Z) | Worker | Clinical |
| 1989 | South Korea | Rickettsia typhi (Z) | Laboratory staff | Research |
| 1987 | Australia | Newcastle disease virus (Z) | Laboratory staff | Research/BSL3 |
| 1986 | Australia | Brucella melitensis (Z) | Researcher | Research |
| 1985 | Japan | Mycobacterium tuberculosis (Z) | Pathologist | Research |
| 1982 | Australia | Shigella flexneri (Z) | Laboratory staff | Clinical |
| Risk Group | Individual Risk | Community Risk | Description |
|---|---|---|---|
| 1 | Low | Low | A microorganism that is unlikely to cause human or animal disease. |
| 2 | Moderate | Low | A pathogen that can cause human or animal disease but is unlikely to be a serious hazard to laboratory workers, the community, livestock or the environment. Laboratory exposure may cause serious infection, but effective treatment and preventive measures are available, and the risk of spread of infection is limited. |
| 3 | High | Low/moderate | A pathogen that usually causes serious human or animal disease but does not ordinarily spread from one infected individual to another. Effective treatment and preventive measures are available. |
| 4 | High | High | A pathogen that usually causes serious human or animal disease and can be readily transmitted from one individual to another, directly or indirectly. Effective treatment and preventive measures are not usually available. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, H.; Bilal, M.; Iqbal, H.M.N. Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks. Int. J. Environ. Res. Public Health 2018, 15, 2697. https://doi.org/10.3390/ijerph15122697
Peng H, Bilal M, Iqbal HMN. Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks. International Journal of Environmental Research and Public Health. 2018; 15(12):2697. https://doi.org/10.3390/ijerph15122697
Chicago/Turabian StylePeng, Huasong, Muhammad Bilal, and Hafiz M. N. Iqbal. 2018. "Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks" International Journal of Environmental Research and Public Health 15, no. 12: 2697. https://doi.org/10.3390/ijerph15122697
APA StylePeng, H., Bilal, M., & Iqbal, H. M. N. (2018). Improved Biosafety and Biosecurity Measures and/or Strategies to Tackle Laboratory-Acquired Infections and Related Risks. International Journal of Environmental Research and Public Health, 15(12), 2697. https://doi.org/10.3390/ijerph15122697