Changing the Paradigm in Public Health and Disability through a Knowledge Translation Center

 , ,
, ,
Abstract
:1. Introduction
People with Disabilities Face Health Inequities
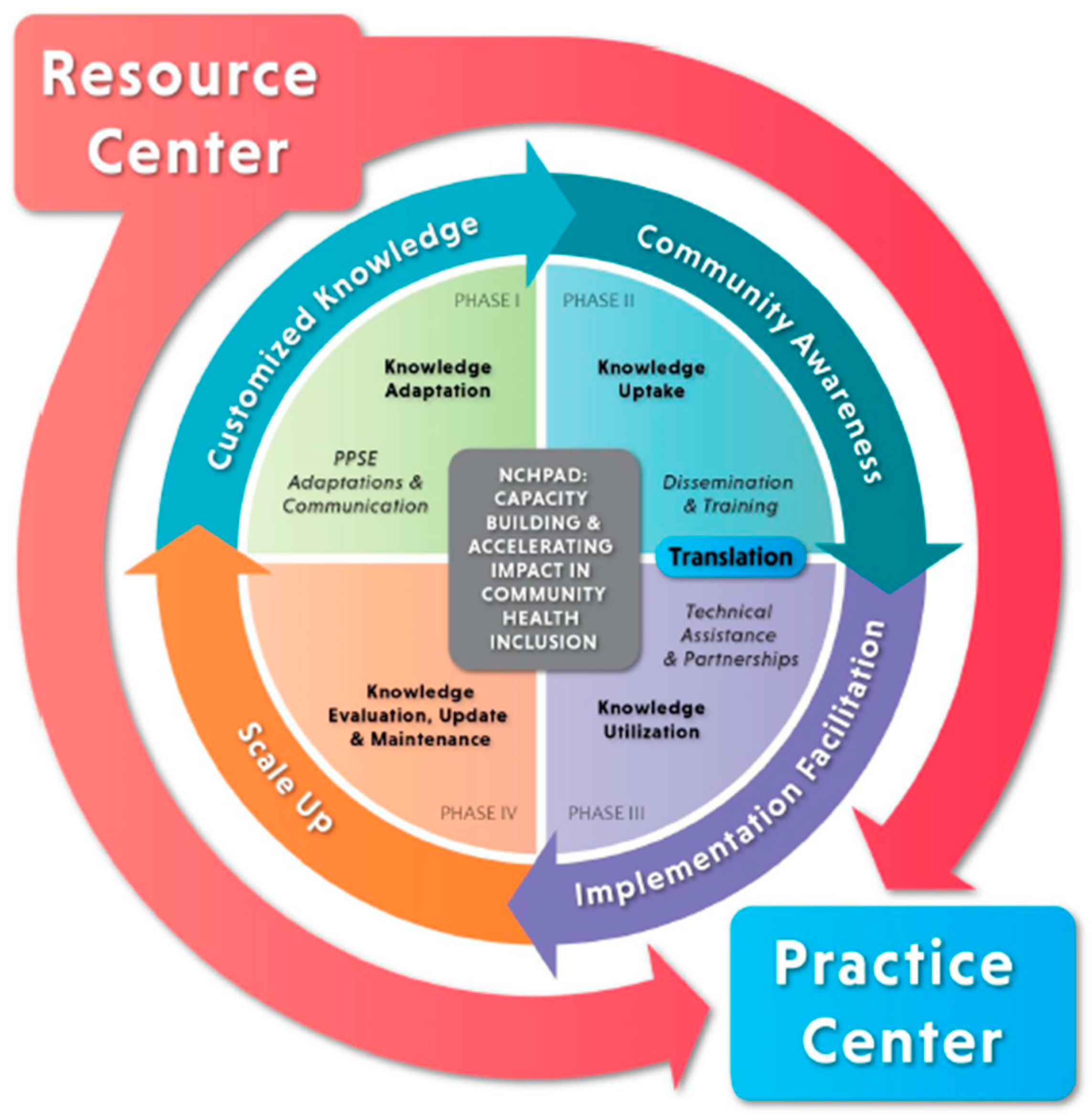
2. Methods
2.1. Phase 1: Knowledge Adaptation: PPSE Adaptation and Communication
2.2. Phase 2: Knowledge Uptake: Dissemination and Training
2.3. Phase 3—Knowledge Utilization: Technical Assistance and Partnerships
2.3.1. Facilitating Top-Down Implementation
2.3.2. Facilitating Bottom-Up Implementation
2.4. Phase 4—Knowledge Evaluation, Update, and Maintenance
3. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Krahn, G.L.; Walker, D.K.; Correa-De-Araujo, R. Persons with disabilities as an unrecognized health disparity population. Am. J. Public Health 2015, 105, S198–S206. [Google Scholar] [CrossRef] [PubMed]
- Braveman, P.A.; Kumanyika, S.; Fielding, J.; LaVeist, T.; Borrell, L.N.; Manderscheid, R.; Troutman, A. Health disparities and health equity: The issue is justice. Am. J. Public Health 2011, 101, S149–S155. [Google Scholar] [CrossRef] [PubMed]
- Americans with Disabilities Act of 1990 Pub. L. 110–325, §4(a), Sept. 25, 2008, 122 Stat. 3555. Available online: https://www.gpo.gov/fdsys/pkg/PLAW-110publ325/pdf/PLAW-110publ325.pdf (accessed on 18 January 2018).
- Drum, C.; McClain, M.R.; Horner-Johnson, W.; Taitan, G. Health Disparities Chart Book on Disability and Racial and Ethnic Status in the United States; University of New Hampshire, Institute on Disability: Concord, NH, USA, 2011. [Google Scholar]
- Kraus, L. Disability Statistics Annual Report; University of New Hampshire: Durham, NH, USA, 2015. [Google Scholar]
- Anderson, W.L.; Armour, B.S.; Finkelstein, E.A.; Wiener, J.M. Estimates of state-level health-care expenditures associated with disability. Public Health Rep. 2010, 125, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Policy, Systems, and Environmental Change. 2011. Available online: http://www.cdc.gov/communitiesputtingpreventiontowork/policy/index.htm#strategies (accessed on 6 December 2017).
- Commission on Social Determinants of Health, Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. 2008. Available online: http://www.who.int/iris/handle/10665/43943 (accessed on 1 November 2017).
- Rimmer, J.H.; Hsieh, K.; Graham, B.C.; Gerber, B.S.; Gray-Stanley, J.A. Barrier removal in increasing physical activity levels in obese African American women with disabilities. J. Women’s Health 2010, 19, 1869–1876. [Google Scholar] [CrossRef] [PubMed]
- Vasudevan, V. An exploration of how people with mobility disabilities rate community barriers to physical activity. Calif. J. Health Promot. 2016, 14, 37–43. [Google Scholar]
- Lindsay, S. Discrimination and other barriers to employment for teens and young adults with disabilities. Disabil. Rehabilit. 2011, 33, 1340–1350. [Google Scholar] [CrossRef] [PubMed]
- Lennox, N.; Diggens, J.; Ugoni, A. The general practice care of people with intellectual disability: Barriers and solutions. J. Intellect. Disabil. Res. 1997, 41, 380–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kroll, T.; Jones, G.C.; Kehn, M.; Neri, M.T. Barriers and strategies affecting the utilisation of primary preventive services for people with physical disabilities: A qualitative inquiry. Health Soc. Care Commun. 2006, 14, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Neri, M.T.; Kroll, T. Understanding the consequences of access barriers to health care: Experiences of adults with disabilities. Disabil. Rehabilit. 2003, 25, 85–96. [Google Scholar] [CrossRef]
- Rimmer, J.H.; Riley, B.; Wang, E.; Rauworth, A.; Jurkowski, J. Physical activity participation among persons with disabilities: Barriers and facilitators. Am. J. Prev. Med. 2004, 26, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Abbott, S.; McConkey, R. The barriers to social inclusion as perceived by people with intellectual disabilities. J. Intellect. Disabil. 2006, 10, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Law, M.; Petrenchik, T.; King, G.; Hurley, P. Perceived environmental barriers to recreational, community, and school participation for children and youth with physical disabilities. Arch. Phys. Med. Rehabil. 2007, 88, 1636–1642. [Google Scholar] [CrossRef] [PubMed]
- Benz, M.R.; Lindstrom, L.; Yovanoff, P. Improving graduation and employment outcomes of students with disabilities: Predictive factors and student perspectives. Except. Child. 2000, 66, 509–529. [Google Scholar] [CrossRef]
- Pivik, J.; McComas, J.; Laflamme, M. Barriers and facilitators to inclusive education. Except. Child. 2002, 69, 97–107. [Google Scholar] [CrossRef]
- Hernandez, B.; Keys, C.; Balcazar, F. Employer attitudes toward workers with disabilities and their ADA employment rights: A literature review. J. Rehabil. 2000, 66, 4. [Google Scholar]
- Fiedler, I.; Indermuehle, D.; Drobac, W.; Laud, P. Perceived barriers to employment in individuals with spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2002, 7, 73–82. [Google Scholar] [CrossRef]
- Ottomanelli, L.; Lind, L. Review of critical factors related to employment after spinal cord injury: Implications for research and vocational services. J. Spinal Cord Med. 2009, 32, 503. [Google Scholar] [CrossRef] [PubMed]
- National Center on Health Physical Activity and Disability, Definition of Inclusion. 2018. Available online: https://www.nchpad.org/1456/6380/Definition~of~Inclusion (accessed on 18 January 2018).
- Rimmer, J.H.; Vanderbom, K.A.; Graham, I.D. A new framework and practice center for adapting, translating, and scaling evidence-based health/wellness programs for people with disabilities. J. Neurol. Phys. Ther. 2016, 40, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Williams, A.S.; Moore, S.M. Universal design of research: Inclusion of persons with disabilities in mainstream biomedical studies. Sci. Trans. Med. 2011, 3. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, M.; Swartz, L.; Officer, A.; Chan, K.Y.; Rudan, I.; Saxena, S. Research priorities for health of people with disabilities: An expert opinion exercise. Lancet 2009, 374, 1857–1862. [Google Scholar] [CrossRef]
- Rimmer, J.H.; Vanderbom, K.A.; Bandini, L.G.; Drum, C.E.; Luken, K.; Suarez-Balcazar, Y.; Graham, I.D. GRAIDs: A framework for closing the gap in the availability of health promotion programs and interventions for people with disabilities. Implement. Sci. 2014, 9, 100. [Google Scholar] [CrossRef] [PubMed]
- UNC Center for Health Promotion and Disease Prevention, Center TRT, Intervention Review Process, Research Dissemination Categories Definitions. 2013. Available online: http://www.centertrt.org/?p=about_how_interventions_review (accessed on 19 January 2018).
- The ADAPTE Collaboration. The ADAPTE Process: Resource Toolkit for Guideline Adaptation. Version 2.0. Available online: http://www.g-i-n.net/document-store/working-groups-documents/adaptation/adapte-resource-toolkit-guideline-adaptation-2-0.pdf/view (accessed on 4 December 2017).
- Girls on the Run. About Us. 2017. Available online: https://www.girlsontherun.org (accessed on 19 January 2018).
- McCormack, L.; Sheridan, S.; Lewis, M.; Boudewyns, V.; Melvin, C.L.; Kistler, C.; Lohr, K.N. Communication and Dissemination Strategies to Facilitate the Use of Health-Related Evidence; RTI International–University of North Carolina Evidence-based Practice Center: Rockville, MD, USA, 2013. [Google Scholar]
- Sofaer, S.; Hibbard, J. Best Practices in Public Reporting No. 3: How to Maximize Public Awareness and Use of Comparative Quality Reports through Effective Promotion and Dissemination Strategies; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2010.
- Roussos, S.T.; Fawcett, S.B. A review of collaborative partnerships as a strategy for improving community health. Ann. Rev. Public Health 2000, 21, 369–402. [Google Scholar] [CrossRef] [PubMed]
- Provan, K.G.; Nakama, L.; Veazie, M.A.; Teufel-Shone, N.I.; Huddleston, C. Building community capacity around chronic disease services through a collaborative interorganizational network. Health Educ. Behav. 2003, 30, 646–662. [Google Scholar] [CrossRef] [PubMed]
- National Recreation and Parks Association, Parks for Inclusion. 2017. Available online: http://www.nrpa.org/our-work/partnerships/initiatives/parks-for-inclusion/parks-for-inclusion-about/ (accessed on 4 December 2017).
- Harrison, M.; van den Hoek, J. CAN-IMPLEMENT©: A Guideline Adaptation and Implementation Planning Resource; Queen’s University School of Nursing and Canadian Partnership against Cancer: Kingston, ON, Canada, 2012. [Google Scholar]
- Eisenberg, Y.; Rimmer, J.H.; Mehta, T.; Fox, M.H. Development of a community health inclusion index: An evaluation tool for improving inclusion of people with disabilities in community health initiatives. BMC Public Health 2015, 15, 1050. [Google Scholar] [CrossRef] [PubMed]
- McMenamin, T.; Hipple, S. The development of questions on disability for the Current Population Survey. Mon. Labor Rev. 2014, 137. [Google Scholar] [CrossRef]
- Robert Wood Johnson Foundation. Building a Culture of Health. 2017. Available online: https://www.cultureofhealth.org/ (accessed on 28 November 2017).



{kind=link}
{kind=link}
| 1. Plan from the outset for promotion and dissemination of inclusion materials and information created and adapted |
| 2. Identify the target audience as early as possible |
| 3. Engage those who can help learn about and reach the target audiences |
| 4. Use the insights of social marketing to help craft messages about the inclusion materials or information, as well as the dissemination activities |
| 5. Be strategic about the timing of the release of the inclusion materials |
| 6. Be strategic about the positioning of important information within the inclusion materials disseminated |
| 7. Actively work with the media, locally and nationally, to promote inclusion materials and information |
| 8. Use advertising to promote the inclusion materials and information |
| 9. Use outreach to promote the inclusion materials and information and facilitate their use |
| 10. Gather and analyze feedback on the dissemination efforts |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanderbom, K.A.; Eisenberg, Y.; Tubbs, A.H.; Washington, T.; Martínez, A.X.; Rauworth, A. Changing the Paradigm in Public Health and Disability through a Knowledge Translation Center. Int. J. Environ. Res. Public Health 2018, 15, 328. https://doi.org/10.3390/ijerph15020328
Vanderbom KA, Eisenberg Y, Tubbs AH, Washington T, Martínez AX, Rauworth A. Changing the Paradigm in Public Health and Disability through a Knowledge Translation Center. International Journal of Environmental Research and Public Health. 2018; 15(2):328. https://doi.org/10.3390/ijerph15020328
Chicago/Turabian StyleVanderbom, Kerri A., Yochai Eisenberg, Allison H. Tubbs, Teneasha Washington, Alex X. Martínez, and Amy Rauworth. 2018. "Changing the Paradigm in Public Health and Disability through a Knowledge Translation Center" International Journal of Environmental Research and Public Health 15, no. 2: 328. https://doi.org/10.3390/ijerph15020328
APA StyleVanderbom, K. A., Eisenberg, Y., Tubbs, A. H., Washington, T., Martínez, A. X., & Rauworth, A. (2018). Changing the Paradigm in Public Health and Disability through a Knowledge Translation Center. International Journal of Environmental Research and Public Health, 15(2), 328. https://doi.org/10.3390/ijerph15020328