Community Readiness for the Promotion of Physical Activity in Older Adults—A Cross-Sectional Comparison of Rural and Urban Communities




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Sample
2.2. Community Readiness Assessment
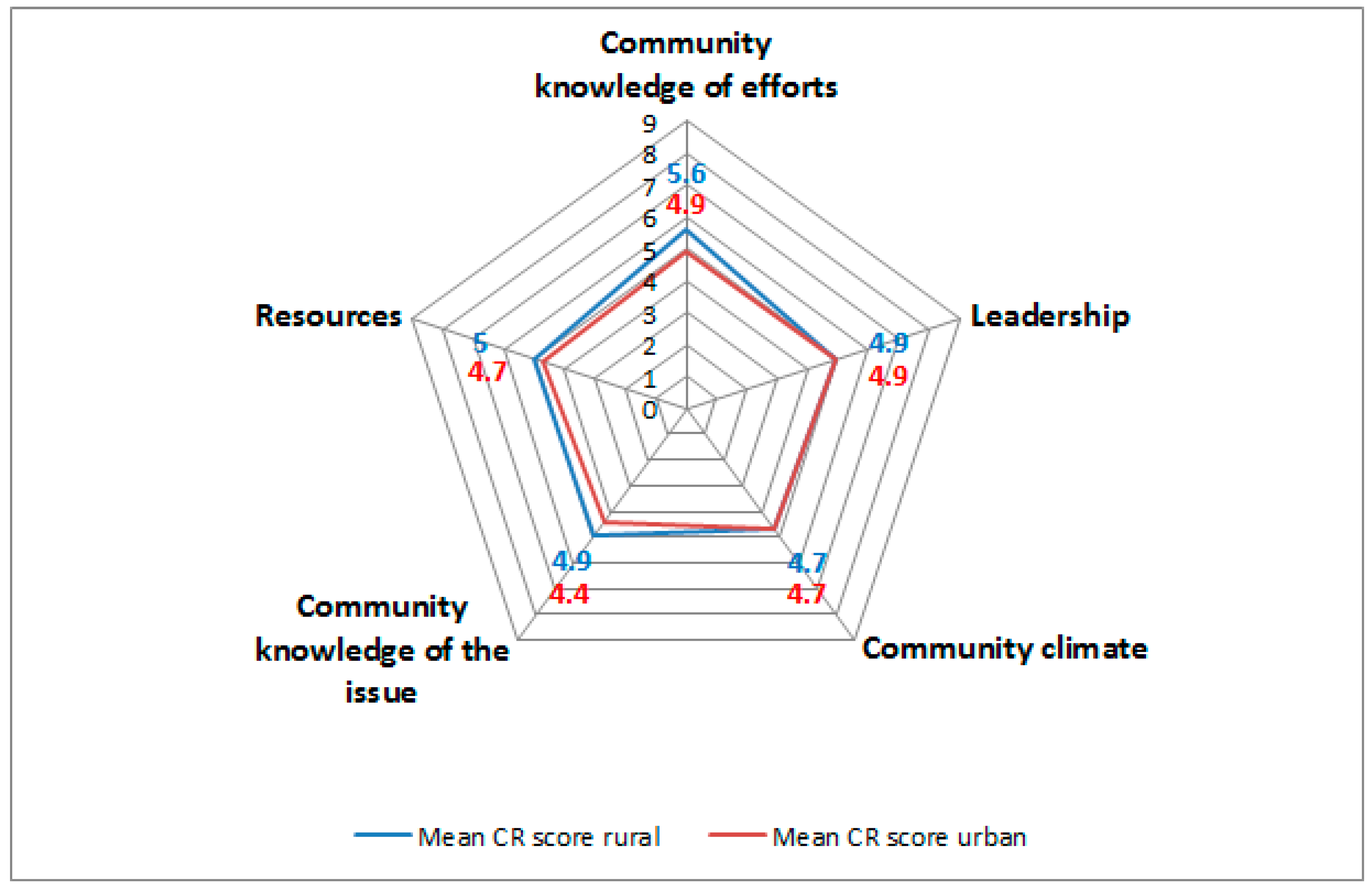
- Community efforts and knowledge of efforts,
- Leadership,
- Community climate,
- Community knowledge of the issue, and
- Resources.
2.3. Data Analysis
2.4. Ethics Statement and Consent
3. Results
3.1. Sample Characteristics
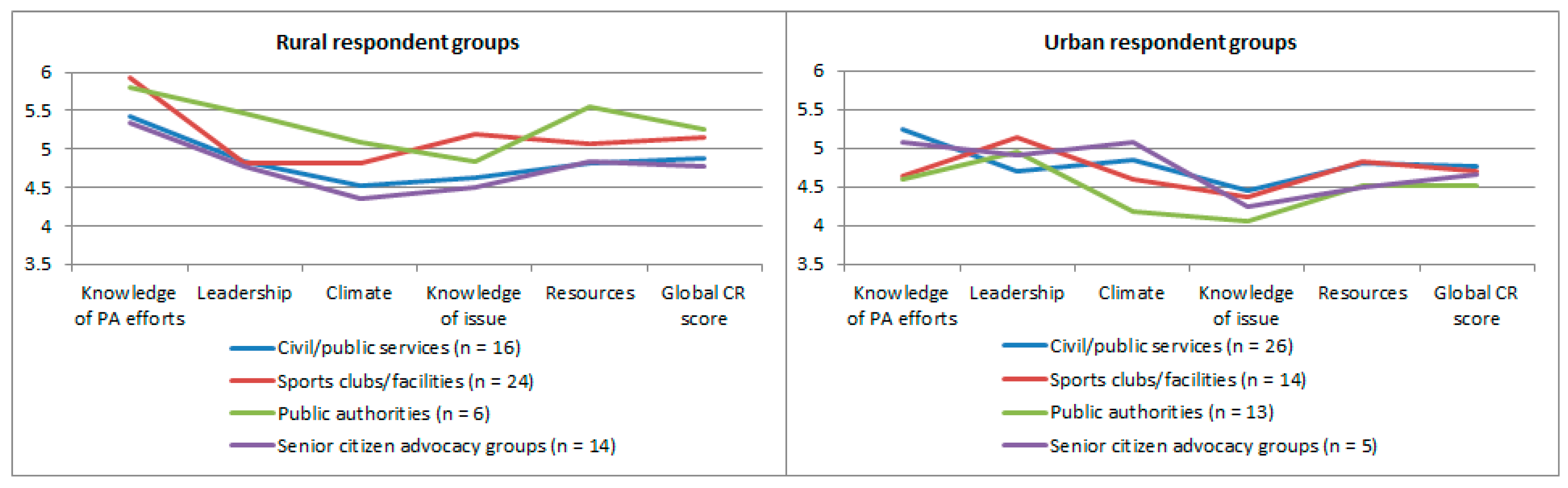
3.2. Community Readiness
3.3. Comparison or Rural and Urban Community Readiness
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Byberg, L.; Melhus, H.; Gedeborg, R.; Sundstrom, J.; Ahlbom, A.; Zethelius, B.; Berglund, L.G.; Wolk, A.; Michaelsson, K. Total mortality after changes in leisure time physical activity in 50 year old men: 35 years follow-up of population based cohort. Br. Med. J. 2009, 338. [Google Scholar] [CrossRef] [PubMed]
- Nigg, C.R.; Long, C.R. A systematic review of single health behavior change interventions vs. multiple health behavior change interventions among older adults. Transl. Behav. Med. 2012, 2, 163–179. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.H.; Hirayama, F. Physical activity and urinary incontinence in older adults: A community-based study. Curr. Aging Sci. 2012, 5, 35–40. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: A systematic analysis for the global burden of disease study 2015. Lancet 2016, 388, 1545–1602. [Google Scholar]
- Black, J.L.; Macinko, J. The changing distribution and determinants of obesity in the neighborhoods of New York city, 2003–2007. Am. J. Epidemiol. 2010, 171, 765–775. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.B.; Humphreys, J.S.; Wilson, M.G. Addressing the health disadvantage of rural populations: How does epidemiological evidence inform rural health policies and research? Aust. J. Rural Health 2008, 16, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Ross, C.E. Walking, exercising, and smoking: Does neighborhood matter? Soc. Sci. Med. 2000, 51, 265–274. [Google Scholar] [CrossRef]
- Carpiano, R.M. Neighborhood social capital and adult health: An empirical test of a bourdieu-based model. Health Place 2007, 13, 639–655. [Google Scholar] [CrossRef] [PubMed]
- Lovasi, G.S.; Hutson, M.A.; Guerra, M.; Neckerman, K.M. Built environments and obesity in disadvantaged populations. Epidemiol. Rev. 2009, 31, 7–20. [Google Scholar] [CrossRef] [PubMed]
- Meyer, M.R.U.; Perry, C.K.; Sumrall, J.C.; Patterson, M.S.; Walsh, S.M.; Clendennen, S.C.; Hooker, S.P.; Evenson, K.R.; Goins, K.V.; Heinrich, K.M.; et al. Physical activity-related policy and environmental strategies to prevent obesity in rural communities: A systematic review of the literature, 2002–2013. Prev. Chronic Dis. 2016, 13. [Google Scholar] [CrossRef]
- Sampson, R.J. Local friendship ties and community attachment in mass society: A multi-level systemic model. Am. Sociol. Rev. 1988, 53, 766–779. [Google Scholar] [CrossRef]
- Eyler, A.A.; Brownson, R.C.; Bacak, S.J.; Housemann, R.A. The epidemiology of walking for physical activity in the United States. Med. Sci. Sports Exerc. 2003, 35, 1529–1536. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, S.; Castro, C.; King, A.C.; Housemann, R.; Brownson, R.C. Determinants of leisure time physical activity in rural compared with urban older and ethnically diverse women in the United States. J. Epidemiol. Community Health 2000, 54, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Dyck, D.V.; Cardon, G.; Deforche, B.; De Bourdeaudhuij, I. Urban-rural differences in physical activity in belgian adults and the importance of psychosocial factors. J. Urban Health Bull. N. Y. Acad. Med. 2011, 88, 154–167. [Google Scholar] [CrossRef] [PubMed]
- Arnadottir, S.A.; Gunnarsdottir, E.D.; Lundin-Olsson, L. Are rural older Icelanders less physically active than those living in urban areas? A population-based study. Scand. J. Public Health 2009, 37, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Drygas, W.; Kwasniewska, M.; Kaleta, D.; Pikala, M.; Bielecki, W.; Gluszek, J.; Broda, G. Epidemiology of physical inactivity in Poland: Prevalence and determinants in a former communist country in socioeconomic transition. Public Health 2009, 123, 592–597. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, E.M.; Murphy, M.H.; Murphy, N.M.; Woods, C.; Nevill, A.M.; Lane, A. Prevalence and correlates of physical inactivity in community-dwelling older adults in Ireland. PLoS ONE 2015, 10, e0118293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oetting, E.R.; Jumper-Thurman, P.; Plested, B.; Edwards, R.W. Community readiness and health services. Subst. Use Misuse 2001, 36, 825–843. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.W.; Jumper-Thurman, P.; Plested, B.; Oetting, E.R.; Swanson, L. Community readiness: Research to practice. J. Community Psychol. 2000, 28, 291–307. [Google Scholar] [CrossRef]
- Stanley, L.R. Community Readiness for Community Change, 2nd ed.; Tri-Ethnic Center for Prevention Research: Fort Collins, CO, USA, 2014; pp. 1–70. [Google Scholar]
- Kostadinov, I.; Daniel, M.; Stanley, L.; Gancia, A.; Cargo, M. A systematic review of community readiness tool applications: Implications for reporting. Int. J. Environ. Res. Public Health 2015, 12, 3453–3468. [Google Scholar] [CrossRef] [PubMed]
- Vernon, I.S.; Jumper-Thurman, P. Prevention of HIV/aids in Native American communities: Promising interventions. Public Health Rep. 2002, 117 (Suppl. 1), S96–S103. [Google Scholar] [PubMed]
- Vernon, I.S. American Indian women, HIV/AIDS, and health disparity. Subst. Use Misuse 2007, 42, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Thurman, P.J.; Vernon, I.S.; Plested, B. Advancing HIV/aids prevention among American Indians through capacity building and the community readiness model. J. Public Health Manag. Pract. 2007, 13, S49–S54. [Google Scholar] [CrossRef]
- York, N.L.; Hahn, E.J.; Rayens, M.K.; Talbert, J. Community readiness for local smoke-free policy change. Am. J. Health Promot. 2008, 23, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Travis, D.J.; Learman, J.A.; Brooks, D.; Merrill, T.; Spence, R.T. The faith community, substance abuse, and readiness for change: A national study. J. Soc. Ser. Res. 2012, 38, 231–247. [Google Scholar] [CrossRef]
- Sliwa, S.; Goldberg, J.P.; Clark, V.; Collins, J.; Edwards, R.; Hyatt, R.R.; Junot, B.; Nahar, E.; Nelson, M.E.; Tovar, A.; et al. Using the community readiness model to select communities for a community-wide obesity prevention intervention. Prev. Chronic Dis. 2011, 8, A150. [Google Scholar] [PubMed]
- Pradeilles, R.; Rousham, E.K.; Norris, S.A.; Kesten, J.M.; Griffiths, P.L. Community readiness for adolescents’ overweight and obesity prevention is low in Urban South Africa: A case study. BMC Public Health 2016, 16, 763. [Google Scholar] [CrossRef] [PubMed]
- The Scottish Government. Community Capacity Building—A Review of Current Issues for Community Learning and Development; Communities Scotland: Edinburgh, UK, 2008. [Google Scholar]
- Forberger, S.; Bammann, K.; Bauer, J.; Boll, S.; Bolte, G.; Brand, T.; Hein, A.; Koppelin, F.; Lippke, S.; Meyer, J.; et al. How to tackle key challenges in the promotion of physical activity among older adults (65+): The Aequipa network approach. Int. J. Environ. Res. Public Health 2017, 14, 379. [Google Scholar] [CrossRef] [PubMed]
- Statistisches Bundesamt. Zensus 2011; Version 1; Statistisches Bundesamt: Wiebaden, Germany, 2011. [Google Scholar]
- Brand, T.; Gansefort, D.; Rothgang, H.; Roseler, S.; Meyer, J.; Zeeb, H. Promoting community readiness for physical activity among older adults in Germany-protocol of the ready to change intervention trial. BMC Public Health 2016, 16, 99. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.V. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol. Assess. 1994, 6, 284–290. [Google Scholar] [CrossRef]
- Jones, D.L.; Settipalli, S.; Goins, R.T.; Goodman, J.M.; Hootman, J.M. Community readiness for adopting a physical activity program for people with arthritis in West Virginia. Prev. Chronic Dis. 2012, 9, E70. [Google Scholar] [CrossRef] [PubMed]
- Turcotte, M. Social Engagement and Civic Participation: Are Rural and Small Town Populations Really at an Advantage? Statistics Canada: Ottawa, ON, Canada, 2005; Volume 6. [Google Scholar]
- Barnett, D.W.; Barnett, A.; Nathan, A.; Van Cauwenberg, J.; Cerin, E.; Council on Environment & Physical Activity—Older Adults Working Group. Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 103. [Google Scholar] [CrossRef] [PubMed]
- Muellmann, S.; Bragina, I.; Voelcker-Rehage, C.; Rost, E.; Lippke, S.; Meyer, J.; Schnauber, J.; Wasmann, M.; Toborg, M.; Koppelin, F.; et al. Development and evaluation of two web-based interventions for the promotion of physical activity in older adults: Study protocol for a community-based controlled intervention trial. BMC Public Health 2017, 17. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Stage | Title | Description |
|---|---|---|
| 1 | No awareness | Issue is not generally recognized by the community or leaders as a problem (or it may truly not be an issue). |
| 2 | Denial/resistance | At least some community members recognize that it is a concern, but there is little recognition that it might be occurring locally. |
| 3 | Vague awareness | Most feel that there is a local concern, but there is no immediate motivation to do anything about it. |
| 4 | Preplanning | There is clear recognition that something must be done, and there may even be a group addressing it. However, efforts are not focused or detailed. |
| 5 | Preparation | Active leaders begin planning in earnest. Community offers modest support of efforts. |
| 6 | Initiation | Enough information is available to justify efforts. Activities are underway. |
| 7 | Stabilization | Activities are supported by administrators or community decision makers. Staff are trained and experienced. |
| 8 | Confirmation/expansion | Efforts are in place. Community members feel comfortable using services, and they support expansions. Local data are regularly obtained. |
| 9 | Community ownership/Professionalization | Detailed and sophisticated knowledge exists about prevalence, causes, and consequences. Effective evaluation guides new directions. Model is applied to other issues. |
| Key Respondents | Overall (n = 118) | Rural Communities (n = 60) | Urban Communities (n = 58) | p-Value * |
|---|---|---|---|---|
| Self-reported sex (% male/female) | 44.9/55.1 | 45.0/55.0 | 44.8/55.2 | n.s. |
| Age in years (mean (±)) | 57.0 (±12.6) | 60.7 (±11.1) | 53.1 (±12.9) | 0.002 |
| Living in respective community (% Yes (n)) | 67.8 (117) | 88.3 (53) | 46.6 (27) | 0.000 |
| Representative from: | ||||
| Civil and public services % (n) | 35.6 (42) | 26.7 (16) | 44.8 (26) | 0.008 |
| Sports clubs/facilities % (n) | 32.2 (38) | 40.0 (24) | 24.1 (14) | |
| Public authorities % (n) | 16.1 (19) | 10.0 (6) | 22.4 (13) | |
| Senior citizen advocacy groups % (n) | 16.1 (19) | 23.3 (14) | 8.6 (5) |
| Global Community Readiness Score | Community Knowledge of Efforts | Community Leadership | Community Climate | Community Knowledge of the Issue | Community Resources | |
|---|---|---|---|---|---|---|
| RC (95% CI) | RC (95% CI) | RC (95% CI) | RC (95% CI) | RC (95% CI) | RC (95% CI) | |
| Geographical Area | ||||||
| Urban | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Rural | 0.29 (−0.02, 0.59) | 0.70 (0.26, 1.14) * | 0.11 (−0.35, 0.58) | −0.09 (−0.47, 0.29) | 0.37 (0.04, 0.70) * | 0.35 (−0.11, 0.82) |
| Key Respondent Groups | ||||||
| Civil and public services | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Sports clubs/facilities | −0.04 (−0.32, 0.24) | −0.04 (−0.42, 0.23) | −0.05 (−0.53, 0.42) | 0.09 (−0.32, 0.50) | −0.16 (−0.60, 0.28) | −0.05 (−0.40, 0.29) |
| Public authorities | −0.31 (−0.65, 0.03) | −0.23 (−0.79, 0.32) | −0.15 (−0.48, 0.18) | −0.30 (−0.85, 0.25) | −0.57 (−1.05, −0.08) * | −0.27 (−0.67, 0.13) |
| Senior citizen advocacy groups | −0.11 (−0.32, 0.10) | −0.14 (−0.53, 0.26) | −0.10 (−0.52, 0.72) | −0.24 (−0.83, 0.34) | −0.47 (−0.80, −0.16) * | −0.07 (−0.55, 0.40) |
| Respondent’s Age | 0.00 (−0.01, 0.01) | 0.01 (−0.01, 0.02) | 0.00 (−0.01, 0.01) | 0.00 (−0.01, 0.01) | 0.01 (−0.01, 0.02) | 0.00 (−0.02, 0.01) |
| Self-Reported Sex | ||||||
| Male | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| Female | 0.00 (−0.01, 0.01) | 0.47 (0.11, 0.83) * | −0.35 (−0.68, −0.02) * | −0.12 (−0.44, 0.20) | −0.19 (−0.50, 0.11) | −0.27 (−0.55, 0.01) |
| Living in Respective Community | ||||||
| Yes | Ref. | Ref. | Ref. | Ref. | Ref. | Ref. |
| No | −0.03 (−0.28, 0.23) | 0.10 (−0.40, 0.59) | 0.17 (−0.14, 0.49) | −0.36 (−0.89, 0.17) | −0.17 (−0.47, −0.14) | 0.08 (−0.45, 0.61) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gansefort, D.; Brand, T.; Princk, C.; Zeeb, H. Community Readiness for the Promotion of Physical Activity in Older Adults—A Cross-Sectional Comparison of Rural and Urban Communities. Int. J. Environ. Res. Public Health 2018, 15, 453. https://doi.org/10.3390/ijerph15030453
Gansefort D, Brand T, Princk C, Zeeb H. Community Readiness for the Promotion of Physical Activity in Older Adults—A Cross-Sectional Comparison of Rural and Urban Communities. International Journal of Environmental Research and Public Health. 2018; 15(3):453. https://doi.org/10.3390/ijerph15030453
Chicago/Turabian StyleGansefort, Dirk, Tilman Brand, Christina Princk, and Hajo Zeeb. 2018. "Community Readiness for the Promotion of Physical Activity in Older Adults—A Cross-Sectional Comparison of Rural and Urban Communities" International Journal of Environmental Research and Public Health 15, no. 3: 453. https://doi.org/10.3390/ijerph15030453
APA StyleGansefort, D., Brand, T., Princk, C., & Zeeb, H. (2018). Community Readiness for the Promotion of Physical Activity in Older Adults—A Cross-Sectional Comparison of Rural and Urban Communities. International Journal of Environmental Research and Public Health, 15(3), 453. https://doi.org/10.3390/ijerph15030453