Spatiotemporal Characteristics and Health Risk Assessment of Heavy Metals in PM2.5 in Zhejiang Province

Abstract
:1. Introduction
2. Materials and Methods
2.1. Investigation Fields
2.2. Sample Collection
2.3. Sample Analysis
2.4. Exposure Assessment
2.5. Risk Characterization
3. Results and Discussion
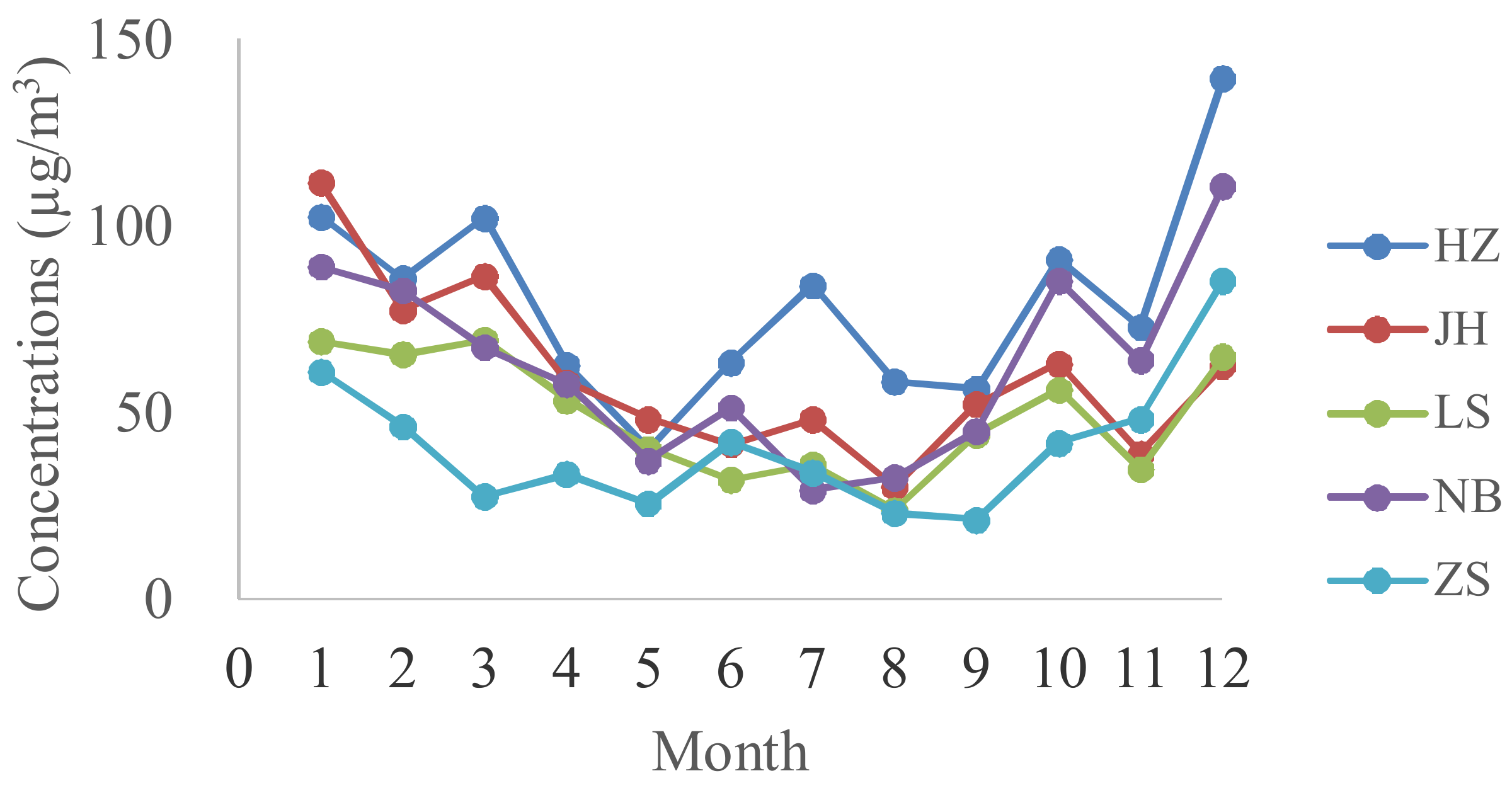
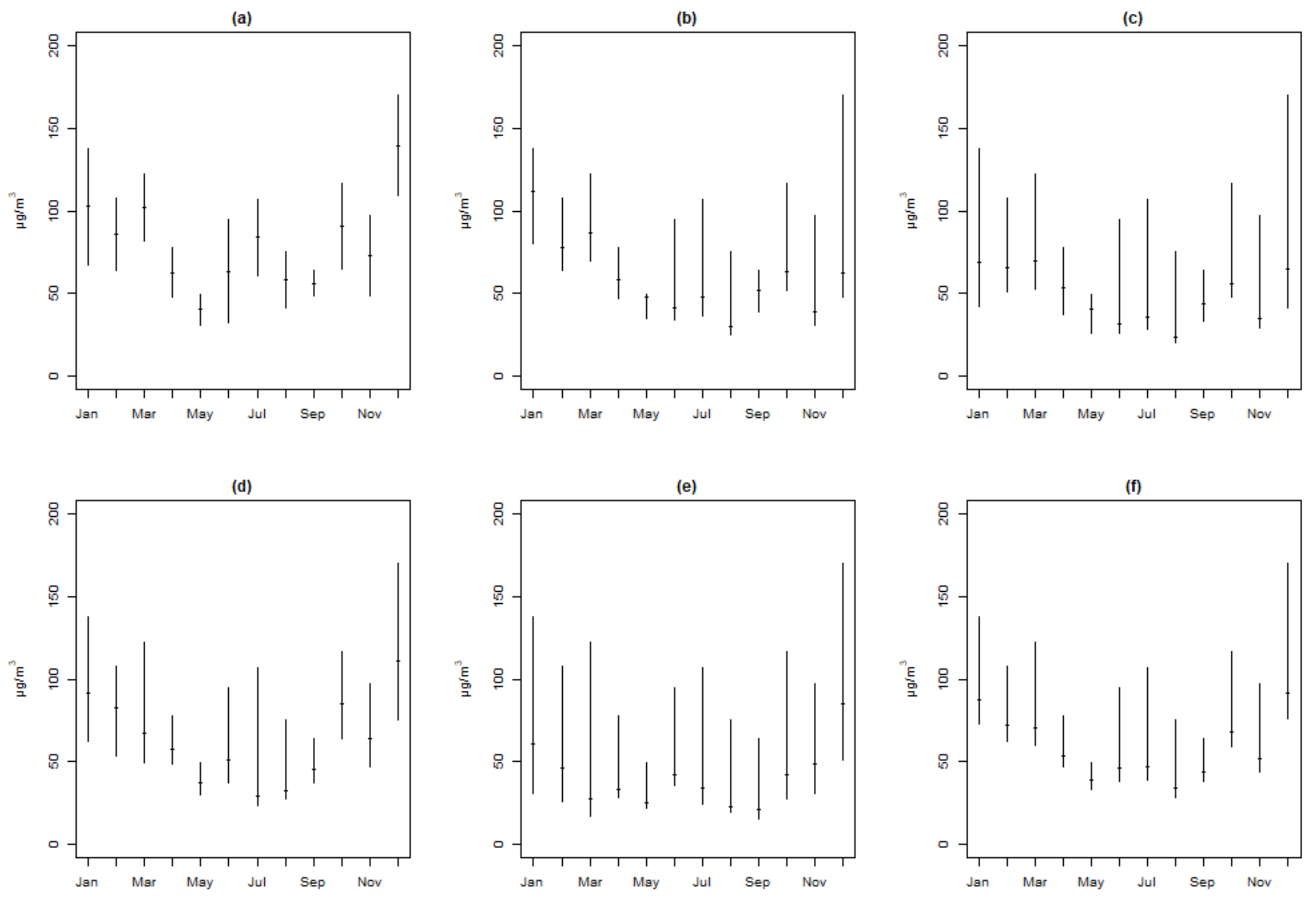
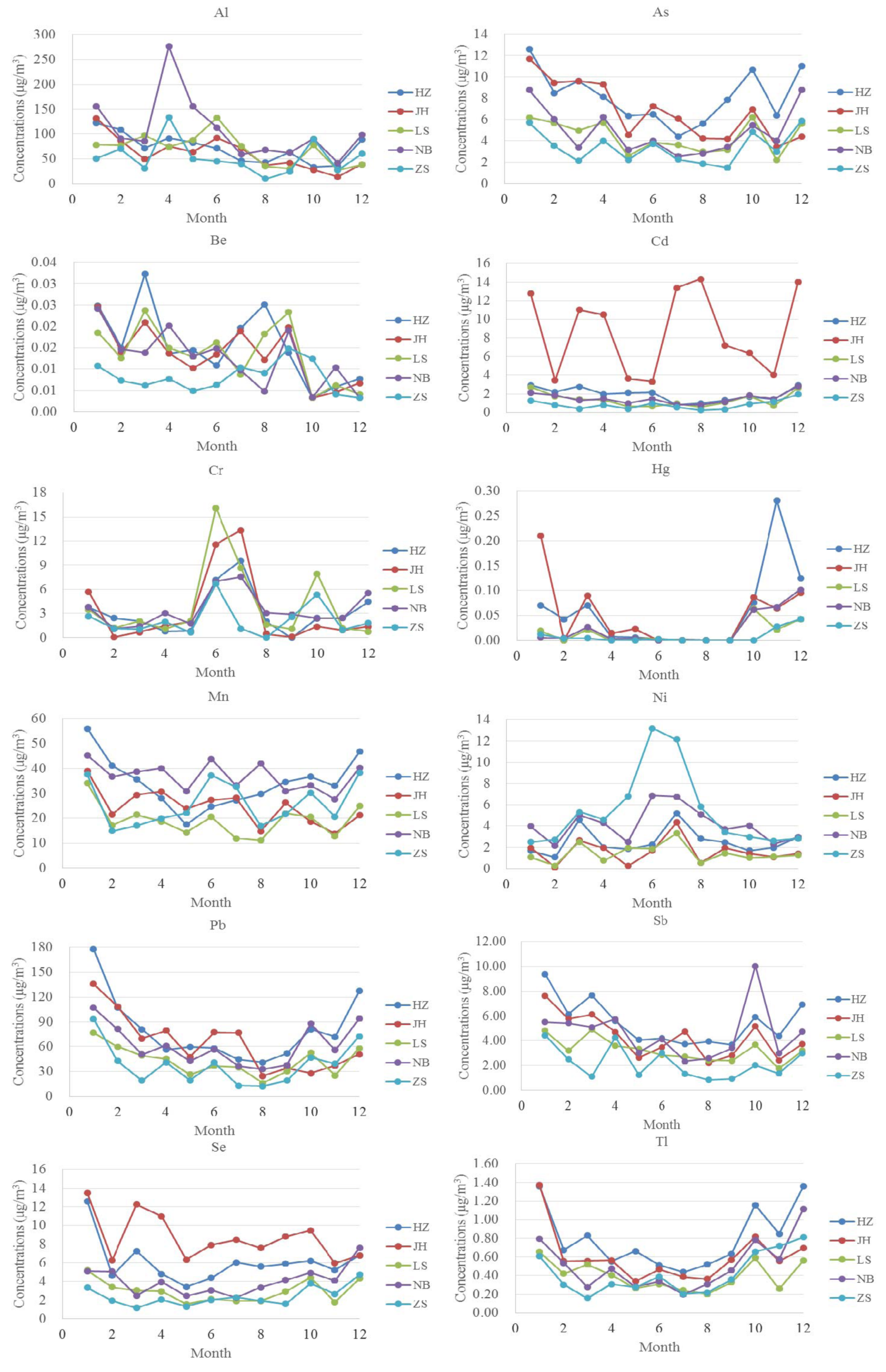
3.1. Spatiotemporal Distributions of PM2.5 and Heavy Metals
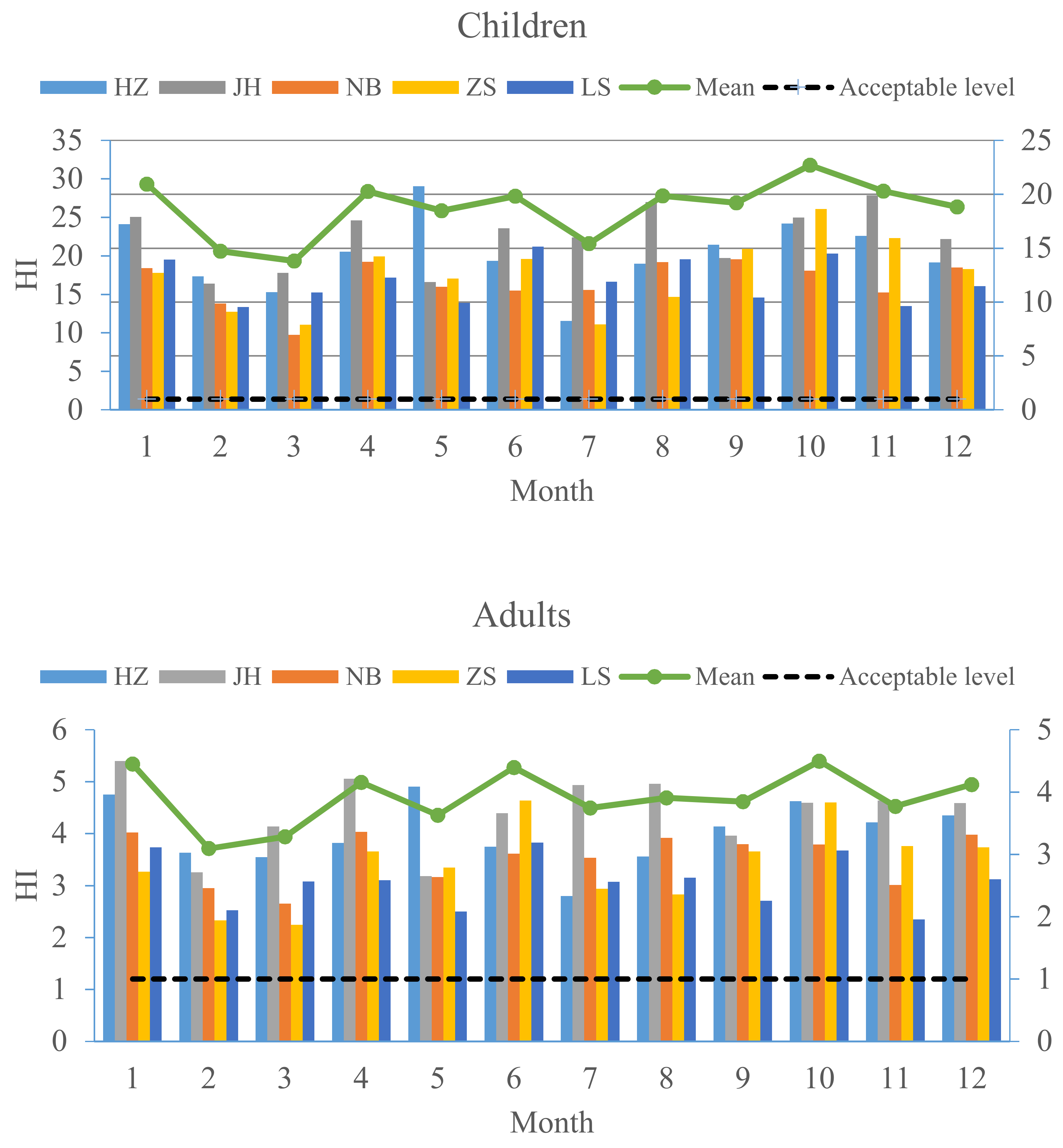
3.2. Non-Carcinogenic Risk Assessment of Toxic Elements in PM2.5
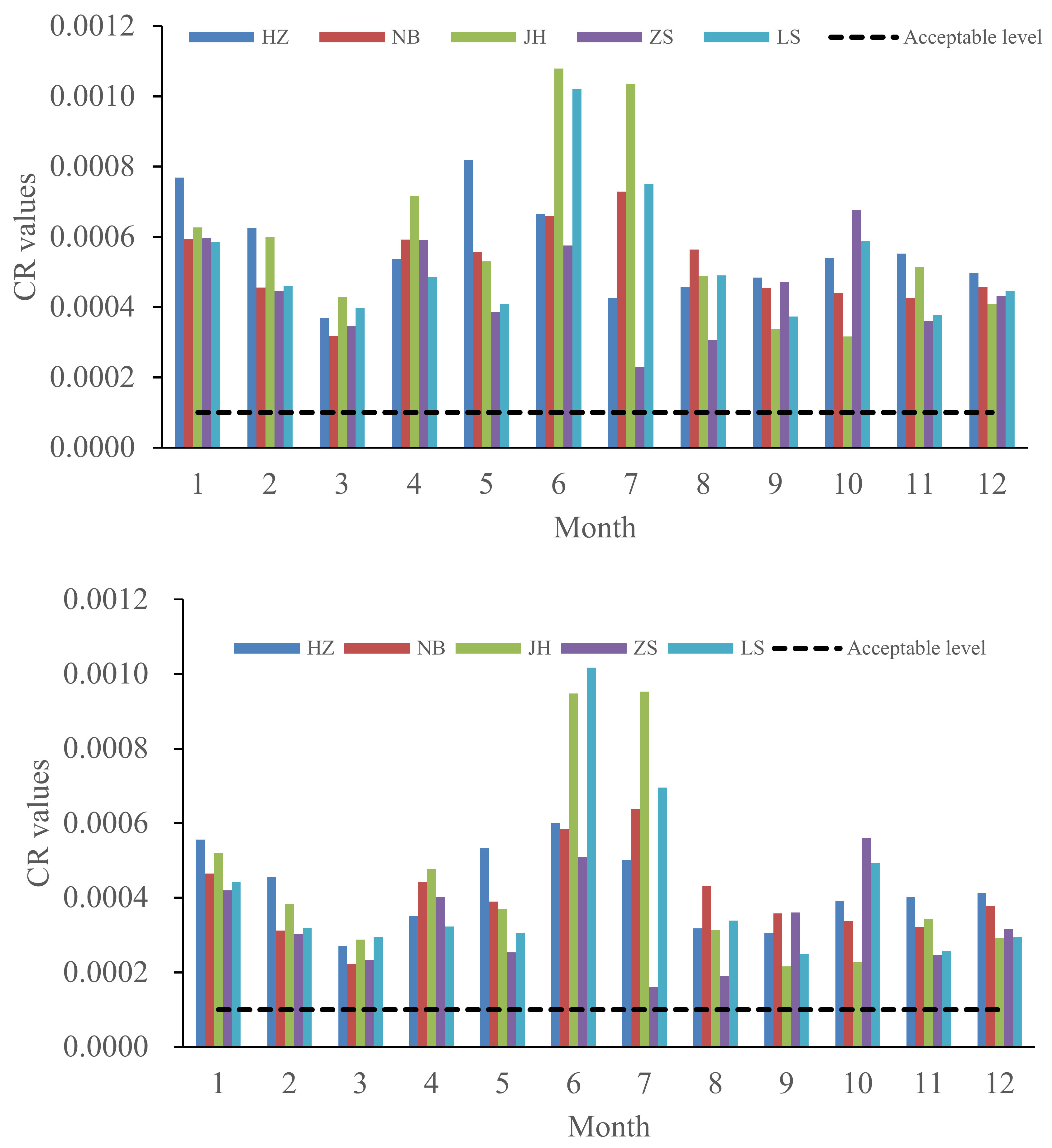
3.3. Carcinogenic Risk Assessment of Toxic Elements in PM2.5
3.4. Uncertainty and Limitation of Health Risk Assessment
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- IARC (International Agency for Research on Cancer). Agents Classified by the IARC Monographs, vol. 1-116. 2016. Available online: http://monographs.iarc.fr/ENG/Classification/latest_classif.php (accessed on 3 August 2016).
- World Health Organization. Ambient (Outdoor) Air Quality and Health (Updated September 2016). 2016. Available online: http://www.who.int/mediacentre/factsheets/fs313/en/ (accessed on 3 August 2016).
- Cheng, Z.; Wang, S.X.; Jiang, J.K.; Fu, Q.Y.; Chen, C.H.; Xu, B.Y.; Yu, J.Q.; Fu, X.; Hao, J.M. Long-term trend of haze pollution and impact of particulate matter in the Yangtze River Delta, China. Environ. Pollut. 2013, 182, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.Y.; Wang, Y.Q.; Niu, T.; Zhang, X.C.; Gong, S.L.; Zhang, Y.M.; Sun, J.Y. Atmospheric aerosol compositions in China: Spatial/temporal variability, chemical signature, regional haze distribution and comparisons with global aerosols. Atmos. Chem. Phys. 2012, 12, 779–799. [Google Scholar] [CrossRef] [Green Version]
- Xiao, Z.M.; Zhang, Y.F.; Hong, S.M.; Bi, X.H.; Jiao, L.; Feng, Y.C.; Wang, Y.Q. Estimation of the Main Factors Influencing Haze, Based on a Long-term Monitoring Campaign in Hangzhou, China. Aerosol. Air Qual. Res. 2011, 11, 873–882. [Google Scholar] [CrossRef]
- Zheng, X.X.; Hong, Z.F.; Chen, H.; Cao, X.F.; Dai, Z.; Zhu, C.; Xiang, Y.; Wang, W.F.; Zhang, T. Study on Distribution Characteristics of PM2.5 Concentration in Zhejiang Province. Environ. Sustain. Dev. 2015, 3, 166–168. [Google Scholar]
- Mishra, B.K.; Gupta, S.K.; Sinha, A. Human health risk analysis from disinfection by-products (DBPs) in drinking and bathing water of some Indian cities. J. Environ. Health Sci. Eng. 2014, 12, 73. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.J.; Cai, Z.Q.; Xiang, X.M.; Chen, W.; Zhu, L.F. Air Quality in Zhejiang Province and the Impact of Main Meteorological Elements (in Chinese). Environ. Sci. Technol. 2014, 37, 372–377. [Google Scholar]
- Sharma, A.K.; Baliyan, P.; Kumar, P. Air pollution and public health: The challenges for Delhi, India. Rev. Environ. Health. 2018, 33, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Rinehart, L.R.; Fujita, E.M.; Chow, J.C.; Magliano, K.; Zielinska, B. Spatial distribution of PM2.5 associated organic compounds in central California. Atmos. Environ. 2006, 40, 290–303. [Google Scholar] [CrossRef]
- Bari, A.; Dutkiewicz, V.; Judd, C.; Wislon, L.; Luttinger, D.; Husain, L. Regional sources of particulate sulfate, SO2, PM2.5, HCl, and HNO3, in New York, NY. Atmos. Environ. 2003, 37, 2837–2844. [Google Scholar] [CrossRef]
- Karl-Espen, Y.; Wenche, A.; Leonor, T.; Vigdis, V.; Svetlana, T.; David, S.; David, H.; Svetlana, T.; Robert, W.; Zbigniew, K.; et al. Transboundary particulate matter in Europe. Status Rep. 2007, 4, 12. [Google Scholar]
- Chen, K.; Glonek, G.; Hansen, A.; Williams, S.; Tuke, J.; Salter, A.; Bi, P. The effects of air pollution on asthma hospital admissions in Adelaide, South Australia, 2003–2013: Time-series and case-crossover analyses. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2016, 46, 1416–1430. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Sass-Kortsak, A.; Purdham, J.T.; Dales, R.E.; Brook, J.R. Associations between personal exposures and fixed-site ambient measurements of fine particulate matter, nitrogen dioxide, and carbon monoxide in Toronto, Canada. J. Expo. Sci. Environ. Epidemiol. 2006, 16, 172–183. [Google Scholar] [CrossRef] [PubMed]
- Esworthy, R. Air Quality: EPA’s 2013 Changes to the Particulate Matter (PM) Standard; Congressional Research Service: Washington, DC, USA, 2015; p. 6.
- Hu, X.; Zhang, Y.; Ding, Z.H.; Wang, T.J.; Lian, H.Z.; Sun, Y.Y.; Wu, J.C. Bioaccessibility and health risk of arsenic and heavy metals (Cd, Co., Cr, Cu, Ni, Pb, Zn and Mn) in TSP and PM2.5 in Nanjing, China. Atmos. Environ. 2012, 57, 146–152. [Google Scholar] [CrossRef]
- Chen, P.; Bi, X.; Zhang, J.; Wu, J.; Feng, Y. Assessment of heavy metal pollution characteristics and human health risk of exposure to ambient PM2.5 in Tianjin, China. Particuology 2015, 20, 104–109. [Google Scholar] [CrossRef]
- Juda-Rezler, K.; Reizer, M.; Oudinet, J.-P. Determination and analysis of PM10 source apportionment during episodes of air pollution in Central Eastern European urban areas: The case of wintertime 2006. Atmos. Environ. 2011, 45, 6557–6566. [Google Scholar] [CrossRef]
- Srimuruganandam, B.; Nagendra, S.M.S. Source characterization of PM10 and PM2.5 mass using a chemical mass balance model at urban roadside. Sci. Total Environ. 2012, 433, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Bateson, T.F.; Schwartz, J. Children’s response to air pollutants. J. Toxicol. Environ. Health (Part A) 2008, 71, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Brauer, M.; Amann, M.; Burnett, R.T.; Cohen, A.; Dentener, F.; Ezzati, M.; et al. Exposure assessment for estimation of the global burden of disease attributable to outdoor air pollution. Environ. Sci. Technol. 2012, 46, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Kampa, M.; Castanas, E. Human health effects of air pollution. Environ. Pollut. 2008, 151, 362–367. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kabir, E.; Kabir, S. A review on the human health impact of airborne particulate matter. Environ. Int. 2015, 74, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Sacks, J.D.; Stanek, L.W.; Luben, T.J.; Johns, D.O.; Buckley, B.J.; Brown, J.S.; Ross, M. Particulate matter-induced health effects: Who is susceptible? Environ. Health Perspect. 2011, 119, 446. [Google Scholar] [CrossRef] [PubMed]
- Li, K.; Liang, T.; Wang, L. Risk assessment of atmospheric heavy metals exposure in Baotou, a typical industrial city in northern China. Environ. Geochem. Health 2015, 38, 843–853. [Google Scholar] [CrossRef] [PubMed]
- US EPA. Risk Assessment Guidance for Superfund Volume I—Human Health Evaluation Manual (Part A); EPA/540/1-89/002; Office of Emergency and Remedial Response: Washington, DC, USA, 1989.
- US EPA. Risk Assessment Guidance for Superfund Volume I—Human Health Evaluation Manual (Part E, Supplemental Guidance for Dermal Risk Assessment); EPA/540/R/99/005; Office of Superfund Remediation and Technology Innovation: Washington, DC, USA, 2004.
- US EPA. Risk Assessment Guidance for Superfund Volume I—Human Health Evaluation Manual (Part F, Supplemental Guidance for Inhalation Risk Assessment); EPA-540-R-070-002; Office of Superfund Remediation and Technology Innovation: Washington, DC, USA, 2009.
- US EPA. Baseline Human Health Risk Assessment; Vasquez Boulevard and I-70 Superfund Site Denver: Denver, CO, USA, 2001.
- MEPPRC (Ministry of Environmental Protection of the People’s Republic of China). Technical Guidelines for Risk Assessment of Contaminated Sites (HJ 25.3-2014). Available online: http://kjs.mep.gov.cn/hjbhbz/bzwb/trhj/trjcgfffbz/201402/t20140226_268358.htm (accessed on 11 March 2016).
- Environmental Site Assessment Guideline. Available online: http://www.adelaideairport.com.au/corporate/wp-content/uploads/2015/03/EMGDLAALPALEnvironmentalSiteAssessment.pdf (accessed on 23 March 2018).
- US EPA. Supplemental Guidance for Developing Soil Screening Levels for Superfund Sites. Available online: https://nepis.epa.gov/Exe/ZyNET.exe/91003IJK.txt?ZyActionD=ZyDocument&Client=EPA&Index=2000%20Thru%202005&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&UseQField=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery=&File=D%3A%5CZYFILES%5CINDEX%20DATA%5C00THRU05%5CTXT%5C00000023%5C91003IJK.txt&User=ANONYMOUS&Password=anonymous&SortMethod=h%7C-&MaximumDocuments=1&FuzzyDegree=0&ImageQuality=r75g8/r75g8/x150y150g16/i425&Display=hpfr&DefSeekPage=x&SearchBack=ZyActionL&Back=ZyActionS&BackDesc=Results%20page&MaximumPages=20&ZyEntry=1&slide (accessed on 23 March 2018).
- RAIS. The Risk Assessment Information System. 2013. Available online: http://rais.ornl.gov/ (accessed on 3 August 2016).
- US EPA. Risk Assessment Guidance for Superfund: Volume III-Part A, Process for Conducting Probabilistic Risk Assessment; EPA 540-R-02-002; US Environmental Protection Agency: Washington, DC, USA, 2001.
- US EPA. Regional Screening Levels (RSLs). 2016. Available online: https://www.epa.gov/risk/regional-screening-levels-rsls (accessed on 11 March 2016).
- Geng, N.B.; Wang, J.; Xu, Y.F.; Zhang, W.D.; Chen, C.; Zhang, R.Q. PM2.5 in an industrial district of Zhengzhou, China: Chemical composition and source apportionment. Particuology 2013, 11, 99–109. [Google Scholar] [CrossRef]
- Kulshrestha, A.; Satsangi, P.G.; Masih, J.; Taneja, A. Metal concentration of PM2.5 and PM10 particles and seasonal variations in urban and rural environment of Agra, India. Sci. Total Environ. 2009, 407, 6196–6204. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Zhang, L.M.; Engling, G.; Zhang, R.J.; Yang, Y.H.; Cao, J.J.; Zhu, C.S.; Wang, K.Y. Chemical composition of PM2.5 in an urban environment in Chengdu, China: Importance of springtime dust storms and biomass burning. Atmos. Res. 2013, 122, 270–283. [Google Scholar] [CrossRef]
- Liu, R.C.; Zeng, J.; Jiang, X.Y.; Chen, J.Y.; Gao, X.F.; Zhang, L.; Li, T.T. The relationship between airborne fine particle matter and emergency ambulance dispatches in a southwestern city in Chengdu, China. Environ. Pollut. 2017, 229, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Hu, Z.M.; Chen, Y.Y.; Chen, Z.L.; Xu, S.Y. Contamination characteristics and possible sources of PM10 and PM2.5 in different functional areas of Shanghai, China. Atmos. Environ. 2013, 68, 221–229. [Google Scholar] [CrossRef]
- Sun, Y.Y.; Hu, X.; Wu, J.C.; Lian, H.Z.; Chen, Y.J. Fractionation and health risks of atmospheric particle-bound As and heavy metals in summer and winter. Sci. Total Environ. 2015, 493, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Jiao, L.; Ma, W. Variation of PM2.5 concentration in Hangzhou, China. Particuology 2013, 11, 55–62. [Google Scholar] [CrossRef]
- Kang, H.Q.; Zhu, B.; Su, J.F.; Wang, H.L.; Zhang, Q.C.; Wang, F. Analysis of a longlasting haze episode in Nanjing, China. Atmos. Res. 2013, 120, 78–87. [Google Scholar] [CrossRef]
- Li, H.; Wang, Q.; Shao, M.; Wang, J.; Wang, C.; Sun, Y.; et al. Fractionation of airborne particulate-bound elements in haze-fog episode and associated health risks in a megacity of southeast China. Environ. Pollut. 2016, 208, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Qing, X.; Yutong, Z.; Shenggao, L. Assessment of heavy metal pollution and human health risk in urban soils of steel industrial city (Anshan), Liaoning, Northeast China. Ecotoxicol. Environ. Saf. 2015, 120, 377–385. [Google Scholar] [CrossRef] [PubMed]
- US EPA. Toxicological Review of Trivalent Chromium. In Support of Summary Information on the Integrated Risk Information System (IRIS); U.S. Environmental Protection Agency: Washington, DC, USA, 1998. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Notation | Unit | Value | References | |
|---|---|---|---|---|---|
| Children | Adults | ||||
| Metal concentrations in PM2.5 | C | µg/m3 | Table 2 | This study | |
| Average lifetime | ATn | hours | ED × 365 × 24 (for non-carcinogens) 70 × 365 × 24 (for carcinogens) | ED × 365 × 24 (for non-carcinogens) 70 × 365 × 24 (for carcinogens) | [29] |
| Averaging lifetime | AT | days | ED × 365 (for non-carcinogens) 70 × 365 (for carcinogens) | ED × 365 (for non-carcinogens) 70 × 365 (for carcinogens) | [29] |
| Body weight | BW | kg | 15.9 | 56.8 | [30] |
| Conversion factor | CF | mg/kg | 10−6 | 10−6 | [29] |
| Exposure duration | ED | year | 6 | 24 | [29] |
| Exposure frequency | EF | days/year | 350 | 350 | [31] |
| Exposure time | ET | h/day | 24 | 24 | [29] |
| Ingestion rate | IR | mg/day | 200 | 100 | [29] |
| Skin surface area adherence that contacts the airborne particulates | SA | cm2 | 1600 | 4350 | [31] |
| Skin adherence factor for the airborne particulates | AF | mg/cm2 | 0.2 | 0.07 | [32] |
| Dermal absorption factor | ABS | / | 0.03 (As), 0.1 (Pb), 0.001 (Cd), 0.01 (other metals) | [33] | |
| City | PM2.5 | Al | As | Be | Cd | Cr | Hg | Mn | Ni | Pb | Sb | Se | Tl |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HZ | 78.73 ± 39.85 | 71.16 ± 45.47 | 8.08 ± 4.19 | 0.02 ± 0.01 | 1.91 ± 1.42 | 3.14 ± 3.05 | 0.06 ± 0.12 | 34.01 ± 18.65 | 2.55 ± 1.91 | 78.79 ± 53.77 | 5.44 ± 3.11 | 6.06 ± 3.47 | 0.78 ± 0.47 |
| JH | 61.72 ± 32.43 | 63.52 ± 44.96 | 7.02 ± 5.45 | 001 ± 0.01 | 8.81 ± 11.98 | 3.57 ± 5.13 | 0.05 ± 0.08 | 25.37 ± 12.38 | 1.70 ± 1.86 | 66.48 ± 50.50 | 4.45 ± 2.33 | 8.96 ± 4.53 | 0.62 ± 0.40 |
| NB | 62.89 ± 35.86 | 108.15 ± 85.92 | 4.88 ± 3.30 | 0.01 ± 0.01 | 1.50 ± 0.91 | 3.42 ± 3.52 | 0.02 ± 0.04 | 36.80 ± 15.18 | 4.09 ± 2.78 | 61.88 ± 38.46 | 4.61 ± 3.90 | 4.06 ± 2.92 | 0.51 ± 0.37 |
| ZS | 41.88 ± 31.62 | 52.88 ± 44.90 | 3.48 ± 2.76 | 0.01 ± 0.01 | 0.83 ± 0.85 | 2.14 ± 2.25 | 0.01 ± 0.02 | 26.29 ± 22.03 | 5.30 ± 4.39 | 40.28 ± 49.54 | 2.25 ± 2.59 | 2.44 ± 1.93 | 0.42 ± 0.35 |
| LS | 48.99 ± 24.44 | 69.32 ± 56.64 | 4.39 ± 2.58 | 0.01 ± 0.01 | 1.34 ± 1.01 | 3.95 ± 6.08 | 0.01 ± 0.02 | 18.99 ± 10.32 | 1.44 ± 1.25 | 42.33 ± 25.08 | 3.22 ± 1.76 | 2.93 ± 1.65 | 0.39 ± 0.24 |
| Mean | 58.83 ± 35.36 | 72.61 ± 60.05 | 5.60 ± 4.20 | 0.01 ± 0.01 | 3.02 ± 6.45 | 3.25 ± 4.29 | 0.03 ± 0.07 | 28.18 ± 17.33 | 2.99 ± 3.03 | 58.05 ± 47.03 | 4.00 ± 3.02 | 4.98 ± 3.95 | 0.55 ± 0.40 |
| Toxic Elements | 95%UCL | CDI (mg/kg-Day) | EC (μg/m3) | DAD (mg/kg) | Non-Carcinogenic Risks (HQ) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ng/mg) | (ng/m3) | Child | Adult | Child | Adult | Child | Adult | Child-Ing | Adult-Ing | Child-Inh | Adult-Inh | Child-Der | Adult-Der | Child | Adult | |
| Al | 1.59 × 103 | 7.80 × 101 | 1.18 × 10−2 | 1.66 × 10−3 | 4.54 × 10−2 | 4.54 × 10-2 | 1.90 × 10−4 | 5.05 × 10−5 | 1.18 × 10−2 | 1.66 × 10−3 | 9.09 × 10−3 | 9.09 × 10−3 | 1.39 × 10−6 | 5.94 × 10−6 | 2.09 × 10−2 | 1.08 × 10−2 |
| As | 1.07 × 102 | 5.97 × 100 | 1.07 × 10−3 | 1.50 × 10−4 | 4.24 × 10−3 | 4.24 × 10−3 | 5.13 × 10−5 | 1.37 × 10−5 | 3.56 × 100 | 4.99 × 10−1 | 2.12 × 10−1 | 2.12 × 10−1 | 1.26 × 10−3 | 5.36 × 10−3 | 3.78 × 100 | 7.16 × 10−1 |
| Be | 2.78 × 10−1 | 1.37 × 10−2 | 2.16 × 10−6 | 3.02 × 10−7 | 8.55 × 10−6 | 8.55 × 10−6 | 3.46 × 10−8 | 9.21 × 10−9 | 1.08 × 10−3 | 1.51 × 10−4 | 4.27 × 10−4 | 4.27 × 10−4 | 1.81 × 10−5 | 7.73 × 10−5 | 1.53 × 10−3 | 6.56 × 10−4 |
| Cd | 6.31 × 101 | 3.59 × 100 | 3.58 × 10−4 | 5.01 × 10−5 | 1.42 × 10−3 | 1.42 × 10−3 | 5.73 × 10−7 | 1.53 × 10−7 | 3.58 × 10−1 | 5.01 × 10−2 | 1.42 × 10−1 | 1.42 × 10−1 | 1.68 × 10−4 | 7.17 × 10−4 | 5.00 × 10−1 | 1.92 × 10−1 |
| Cr | 7.92 × 101 | 3.63 × 100 | 1.95 × 10−4 | 2.72 × 10−5 | 7.53 × 10−4 | 7.53 × 10−4 | 3.11 × 10−6 | 8.30 × 10−7 | 6.49 × 10−2 | 9.08 × 10−3 | 7.53 × 10−3 | 7.53 × 10−3 | 3.05 × 10−4 | 1.30 × 10−3 | 7.27 × 10−2 | 1.79 × 10−2 |
| Hg | 4.92 × 10−1 | 3.79 × 10−2 | 1.02 × 10−6 | 1.43 × 10−7 | 5.86 × 10−6 | 5.86 × 10−6 | 1.64 × 10−8 | 4.36 × 10−9 | 6.40 × 10−3 | 8.96 × 10−4 | 1.95 × 10−5 | 1.95 × 10−5 | 7.52 × 10−7 | 3.21 × 10−6 | 6.42 × 10−3 | 9.19 × 10−4 |
| Pb | 1.05 × 103 | 6.22 × 101 | 1.07 × 10−2 | 1.50 × 10−3 | 4.24 × 10−2 | 4.24 × 10−2 | 1.72 × 10−3 | 4.57 × 10−4 | - | - | - | - | - | - | - | - |
| Mn | 5.67 × 102 | 2.97 × 101 | 5.75 × 10−3 | 8.05 × 10−4 | 2.28 × 10−2 | 2.28 × 10−2 | 9.20 × 10−5 | 2.45 × 10−5 | 4.11 × 10−2 | 5.75 × 10−3 | 4.55 × 10−1 | 4.55 × 10−1 | 4.83 × 10−6 | 2.06 × 10−5 | 4.96 × 10−1 | 4.61 × 10−1 |
| Ni | 7.68 × 101 | 3.26 × 100 | 3.24 × 10−4 | 4.53 × 10−5 | 1.29 × 10−3 | 1.29 × 10−3 | 5.18 × 10−6 | 1.38 × 10−6 | 2.94 × 10−2 | 4.12 × 10−3 | 1.29 × 10−1 | 1.29 × 10−1 | 8.64 × 10−5 | 3.68 × 10−4 | 1.59 × 10−1 | 1.34 × 10−1 |
| Sb | 7.46 × 101 | 4.26 × 100 | 7.33 × 10−4 | 1.03 × 10−4 | 2.89 × 10−3 | 2.89 × 10−3 | 1.17 × 10−5 | 3.12 × 10−6 | 1.83 × 100 | 2.56 × 10−1 | 1.45 × 10−2 | 1.45 × 10−2 | 1.44 × 10−3 | 6.12 × 10−3 | 1.85 × 100 | 2.77 × 10−1 |
| Se | 9.39 × 101 | 5.33 × 100 | 9.06 × 10−4 | 1.27 × 10−4 | 3.59 × 10−3 | 3.59 × 10−3 | 1.45 × 10−5 | 3.86 × 10−6 | 1.81 × 10−1 | 2.54 × 10−2 | 1.79 × 10−4 | 1.79 × 10−4 | 2.13 × 10−5 | 9.07 × 10−5 | 1.81 × 10−1 | 2.56 × 10−2 |
| Tl | 1.00 × 101 | 5.83 × 10−1 | 1.03 × 10−4 | 1.44 × 10−5 | 4.05 × 10−4 | 4.05 × 10−4 | 1.65 × 10−6 | 4.40 × 10−7 | 1.031 × 101 | 1.44 × 100 | - | - | 1.21 × 10−3 | 5.17 × 10−3 | 1.03 × 101 | 1.45 × 100 |
| Sum | 3.20 × 10−2 | 4.48 × 10−3 | 1.25 × 10−1 | 1.25 × 10−1 | 2.09 × 10−3 | 5.55 × 10−4 | 1.640 × 101 | 2.30 × 100 | 9.70 × 10−1 | 9.70 × 10−1 | 4.51 × 10−3 | 1.92 × 10−2 | 1.738 × 101 | 3.28 × 100 | ||
| Toxic Elements | 95%UCL | CDI (mg/kg-Day) | EC (μg/m3) | DAD (mg/kg) | Carcinogenic Risk (CR) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (ng/mg) | (ng/m3) | Child | Adult | Child | Adult | Child | Adult | Child-Ing | Adult-Ing | Child-Inh | Adult-Inh | Child-Der | Adult-Der | Child | Adult | |
| Al | 1.59 × 103 | 7.80 × 101 | 1.02 × 10−3 | 5.69 × 10−4 | 3.90 × 10−3 | 1.56 × 10−2 | 1.63 × 10−5 | 1.73 × 10−5 | - | - | - | - | ||||
| As | 1.07 × 102 | 5.97 × 100 | 9.17 × 10−5 | 5.13 × 10−5 | 3.63 × 10−4 | 1.45 × 10−-3 | 4.40 × 10−6 | 4.69 × 10−6 | 1.37 × 10−4 | 7.70 × 10−5 | 1.56 × 10−6 | 6.25 × 10−6 | 6.60 × 10−6 | 7.03 × 10−6 | 1.46 × 10−4 | 9.03 × 10−5 |
| Be | 2.78 × 10−1 | 1.37 × 10−2 | 1.85 × 10−7 | 1.04 × 10−7 | 7.32 × 10−7 | 2.93 × 10−6 | 2.96 × 10−9 | 3.16 × 10−9 | - | - | 1.76 × 10−9 | 7.03 × 10−9 | - | - | 1.76 × 10−9 | 7.03 × 10−9 |
| Cd | 6.31 × 101 | 3.59 × 100 | 3.07 × 10−5 | 1.72 × 10−5 | 1.21 × 10−4 | 4.85 × 10−4 | 4.91 × 10−8 | 5.23 × 10−8 | - | - | 2.18 × 10−7 | 8.73 × 10−7 | - | - | 2.18 × 10−7 | 8.73 × 10−7 |
| Cr | 7.92 × 101 | 3.63 × 100 | 1.67 × 10−5 | 9.34 × 10−6 | 6.45 × 10−5 | 2.58 × 10−4 | 2.67 × 10−7 | 2.84 × 10−7 | 8.34 × 10−6 | 4.67 × 10−6 | 5.42 × 10−6 | 2.17 × 10−5 | 5.34 × 10−6 | 5.69 × 10−6 | 1.91 × 10−5 | 3.20 × 10−5 |
| Hg | 4.92 × 10−1 | 3.79 × 10−2 | 8.78 × 10−8 | 4.91 × 10−8 | 5.02 × 10−7 | 2.01 × 10−6 | 1.40 × 10−9 | 1.50 × 10−9 | - | - | - | - | - | - | - | - |
| Pb | 1.05 × 103 | 6.22 × 101 | 9.19 × 10−4 | 5.14 × 10−4 | 3.64 × 10−3 | 1.45 × 10−2 | 1.47 × 10−4 | 1.57 × 10−4 | 2.57 × 10−4 | 1.44 × 10−4 | 2.91 × 10−7 | 1.16 × 10−6 | 4.12 × 10−5 | 4.39 × 10−5 | 2.99 × 10−4 | 1.89 × 10−4 |
| Mn | 5.67 × 102 | 2.97 × 101 | 4.93 × 10−4 | 2.76 × 10−4 | 1.95 × 10−3 | 7.80 × 10−3 | 7.88 × 10−6 | 8.40 × 10−6 | - | - | - | - | - | - | - | - |
| Ni | 7.68 × 101 | 3.26 × 100 | 2.77 × 10−5 | 1.55 × 10−5 | 1.11 × 10−4 | 4.43 × 10−4 | 4.44 × 10−7 | 4.73 × 10−7 | - | - | 2.66 × 10−8 | 1.06 × 10−7 | - | - | 2.66 × 10−8 | 1.06 × 10−7 |
| Sb | 7.46 × 101 | 4.26 × 100 | 6.28 × 10−5 | 3.52 × 10−5 | 2.48 × 10−4 | 9.92 × 10−4 | 1.00 × 10−6 | 1.07 × 10−6 | - | - | - | - | - | - | - | - |
| Se | 9.39 × 101 | 5.33 × 100 | 7.76 × 10−5 | 4.35 × 10−5 | 3.08 × 10−4 | 1.23 × 10−3 | 1.24 × 10−6 | 1.32 × 10−6 | - | - | - | - | - | - | - | - |
| Tl | 1.00 × 101 | 5.83 × 10−1 | 8.84 × 10−6 | 4.95 × 10−6 | 3.47 × 10−5 | 1.39 × 10−4 | 1.41 × 10−7 | 1.51 × 10−7 | - | - | - | - | - | - | - | - |
| Sum | 4.03 × 10−4 | 2.26 × 10−4 | 7.52 × 10−6 | 3.01 × 10−5 | 5.31×10−5 | 5.66 × 10−5 | 4.64 × 10−4 | 3.12 × 10−4 | ||||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; He, S.; Chen, S.; Zhang, Y.; Wang, A.; Luo, J.; Ye, X.; Mo, Z.; Wu, L.; Xu, P.; et al. Spatiotemporal Characteristics and Health Risk Assessment of Heavy Metals in PM2.5 in Zhejiang Province. Int. J. Environ. Res. Public Health 2018, 15, 583. https://doi.org/10.3390/ijerph15040583
Wang X, He S, Chen S, Zhang Y, Wang A, Luo J, Ye X, Mo Z, Wu L, Xu P, et al. Spatiotemporal Characteristics and Health Risk Assessment of Heavy Metals in PM2.5 in Zhejiang Province. International Journal of Environmental Research and Public Health. 2018; 15(4):583. https://doi.org/10.3390/ijerph15040583
Chicago/Turabian StyleWang, Xiaofeng, Shengliang He, Shuchang Chen, Yongli Zhang, Aihong Wang, Jinbin Luo, Xialiang Ye, Zhe Mo, Lizhi Wu, Peiwei Xu, and et al. 2018. "Spatiotemporal Characteristics and Health Risk Assessment of Heavy Metals in PM2.5 in Zhejiang Province" International Journal of Environmental Research and Public Health 15, no. 4: 583. https://doi.org/10.3390/ijerph15040583
APA StyleWang, X., He, S., Chen, S., Zhang, Y., Wang, A., Luo, J., Ye, X., Mo, Z., Wu, L., Xu, P., Cai, G., Chen, Z., & Lou, X. (2018). Spatiotemporal Characteristics and Health Risk Assessment of Heavy Metals in PM2.5 in Zhejiang Province. International Journal of Environmental Research and Public Health, 15(4), 583. https://doi.org/10.3390/ijerph15040583