Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Selection of Pollutants and Data Processing
2.2. Health Impact Assessment
2.2.1. Population Data
2.2.2. Selection of Health Endpoints
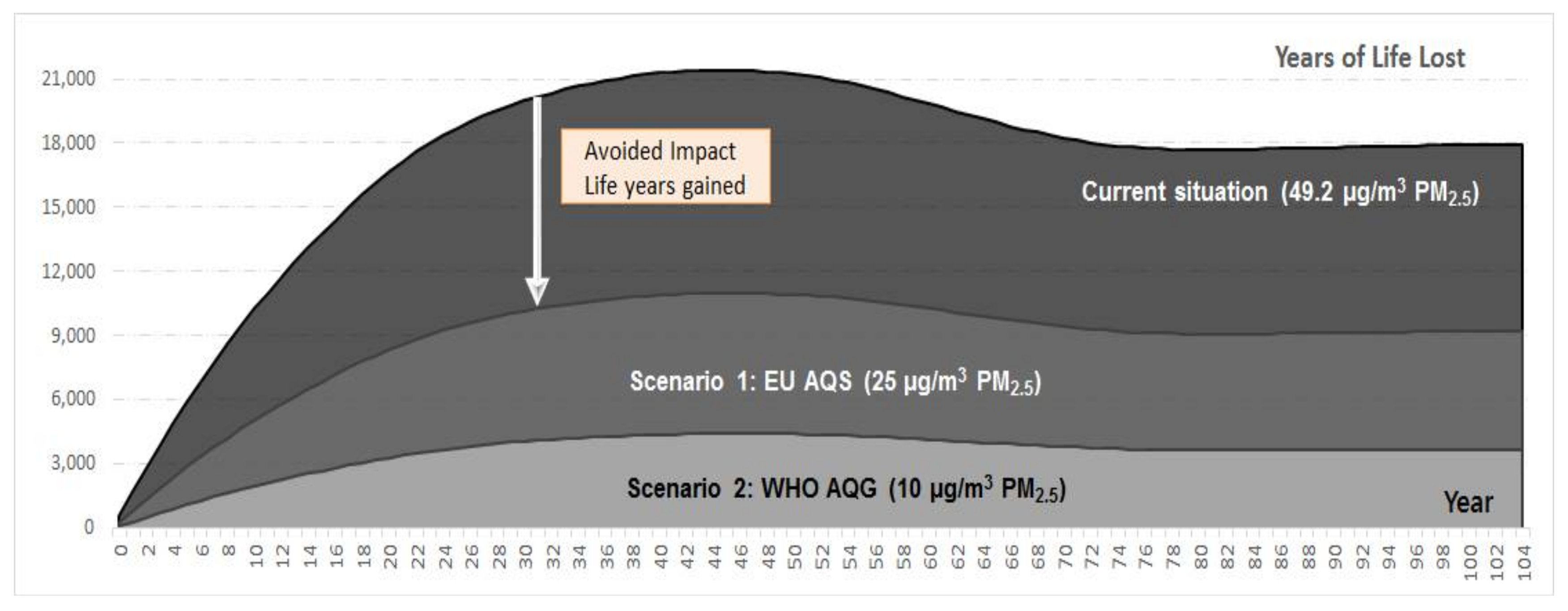
2.2.3. Pollution Mitigation Scenarios
- Current situation—Annual average concentration of PM2.5 at 49.2 μg/m3
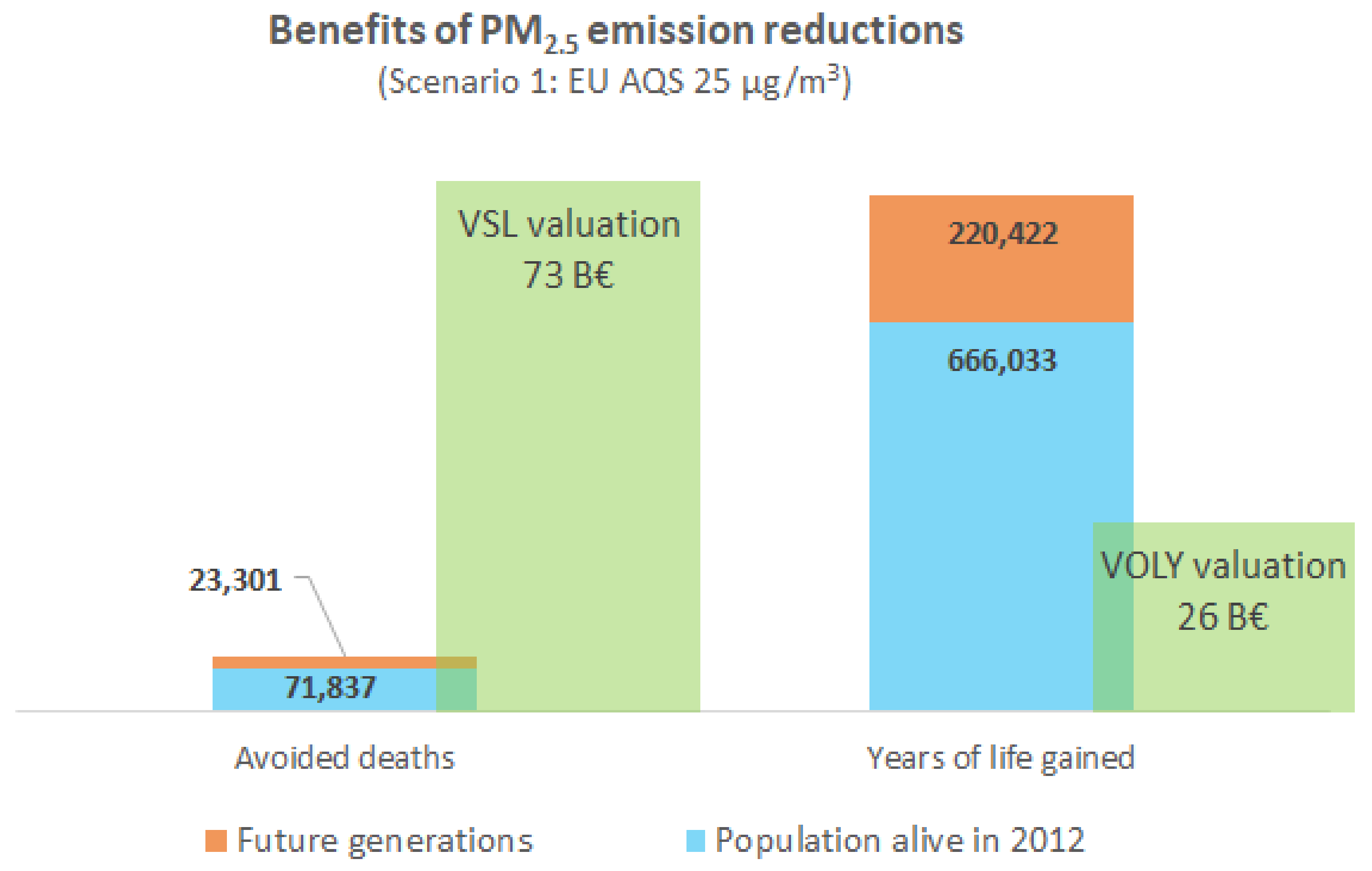
- Scenario 1: EU AQS—Annual average concentration of PM2.5 reduced to 25 μg/m3
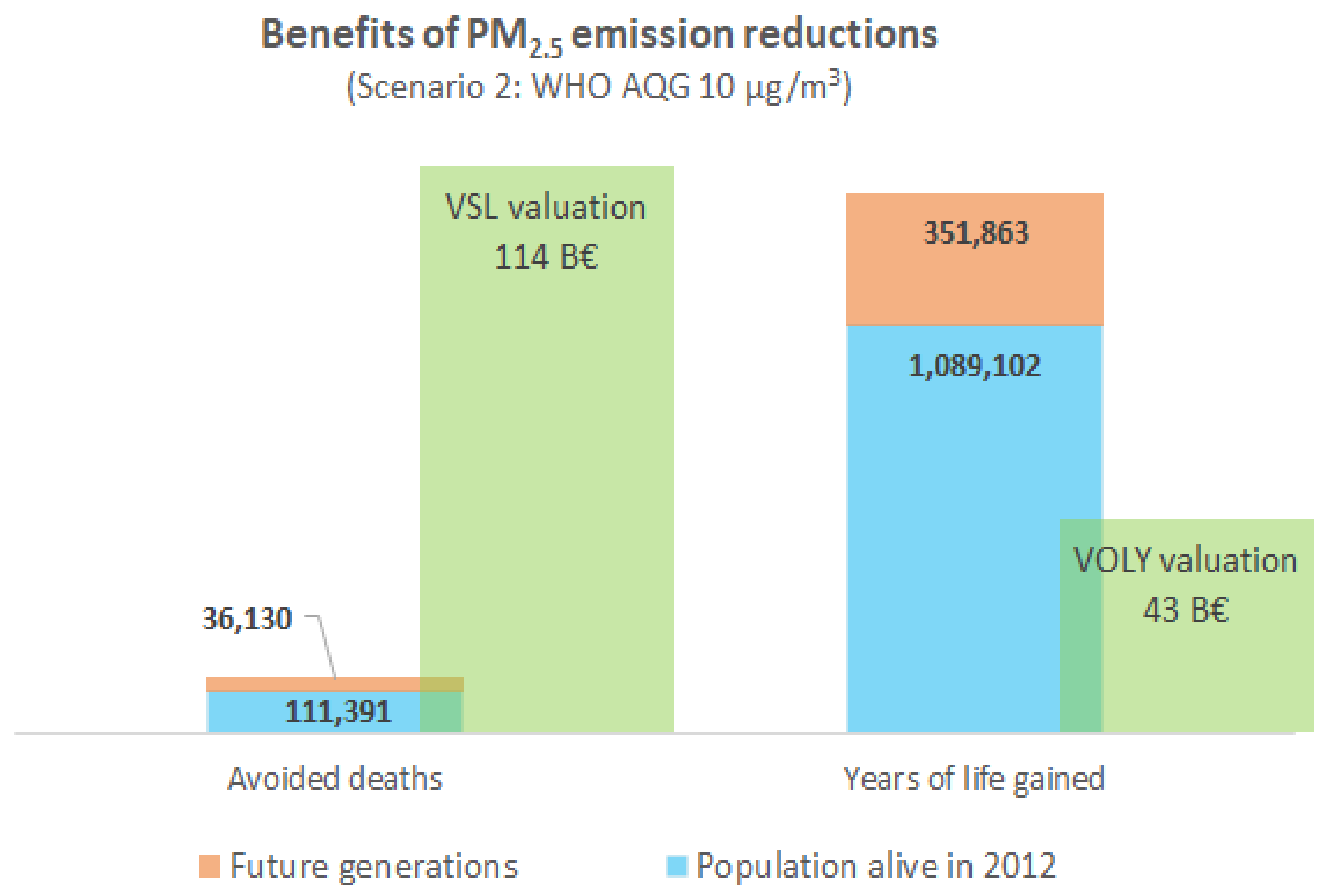
- Scenario 2: WHO AQG—Annual average concentration of PM2.5 reduced to 10 μg/m3
2.3. Economic Evaluation of Premature Mortality
3. Results
3.1. Mortality and Ylls Attributable to Air Pollution in 2012 under Different Scenarios
3.2. Morbidity Attributable to Air Pollution in Year 2012 and Avoidable Impacts under Different Mitigation Scenarios
3.3. Economic Benefits of Reduced Premature Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Brunekreef, B.; Holgate, S.T. Air pollution and health. Lancet 2002, 360, 1233–1242. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Ambient Air Pollution. A Global Assessment of Exposure and Burden of Disease; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Correia, A.W.; Pope, C.A.; Dockery, D.W.; Wang, Y.; Ezzati, M.; Dominici, F. The Effect of Air Pollution Control on Life Expectancy in the United States: An Analysis of 545 US counties for the period 2000 to 2007. Epidemiology 2013, 24, 23–31. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. Review of Evidence on Health Aspects of Air Pollution—REVIHAAP Project Technical Report; World Health Organization, Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Naumovski, K.; Krstev, B.; Basovski, G.; Todeva, T.; Krstev, A. Conditions and impacts on industrial processes and atmospheric approaches of air pollution in the Skopje and Polog region. Nat. Resour. Technol. 2017, 11, 75–82. [Google Scholar]
- Kochubovski, M.; Kendrovski, V. Monitoring of the Ambient Air Quality (PM10) in Skopje and Evaluation of the Health Effects in 2010. J. Environ. Prot. Ecol. 2012, 13, 789–796. [Google Scholar]
- Kovacevik, B.; Wagner, A.; Boman, J.; Laursen, J.; Pettersson, B. Elemental composition of fine particulate matter (PM2.5) in Skopje, FYR of Macedonia. X-ray Spectrom. 2011, 40, 280–288. [Google Scholar] [CrossRef]
- Anttila, P.; Stefanovska, A.; Nestorovska-Krsteska, A.; Grozdanovski, L.; Atanasov, I.; Golubov, N.; Walden, J. Characterisation of extreme air pollution episodes in an urban valley in the Balkan Peninsula. Air Qual. Atmos. Health 2016, 9, 129–141. [Google Scholar] [CrossRef]
- Kendrovski, V.T. The impact of ambient temperature on mortality among the urban population in Skopje, Macedonia during the period 1996–2000. BMC Public Health 2006, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Kendrovski, V.; Spasenovska, M.; Menne, B. The public health impacts of climate change in the former Yugoslav Republic of Macedonia. Int. J. Environ. Res. Public Health 2014, 11, 5975–5988. [Google Scholar] [CrossRef] [PubMed]
- Stafilov, T.; Bojkovska, T.; Hirao, M. Air pollution monitoring system in the Republic of Macedonia. J. Environ. Prot. Ecol. 2003, 4, 518–524. [Google Scholar]
- Holland, M. Cost Benefit Analysis of Final Policy Scenarios for the EU Clean Air Package; The International Institute for Applied Systems Analysis: Laxemburg, Austria, 2014. [Google Scholar]
- World Health Organization (WHO). Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide. Global Update 2005; Summary of Risk Assessment; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- World Health Organization (WHO). Health Risks of Air Pollution in Europe—HRAPIE Project Recommendations for Concentration–Response Functions for Cost–Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Martuzzi, M.; Mitis, F.; Iavarone, I.; Serinelli, M. Health Impact of Ozone in 13 Italian Cities; Europe PMC: London, UK, 2013. [Google Scholar]
- Ostro, B. Outdoor Air Pollution—Assessing the environmental burden of disease at national and local levels. In Environmental Burden of Disease Series; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Air Quality Assessment Report: Аir Quality Assessment of Sulphur Dioxide, Nitrogen Dioxide, Nitrogen Oxides, Carbon Monoxide, Particulate Matter, Ozone, Lead, Arsenic, Nickel and Cadmium Concentrations in Republic of Macedonia. Available online: http://airquality.moepp.gov.mk/airquality/wp-content/uploads/2012/03/Preliminary-assessment-report_200412_SL-FINAL.pdf (accessed on 26 January 2018).
- State Statistical Office of Macedonia. Statistical Review: Population and Social Statistics; State Statistical Office of Macedonia: Skopje, Republic of Macedonia, 2016. [Google Scholar]
- State Statistical Office of Macedonia. Statistical Review: Population and Social Statistics; State Statistical Office of Macedonia: Skopje, Republic of Macedonia, 2013. [Google Scholar]
- Hoek, G.; Krishnan, R.M.; Beelen, R.; Peters, A.; Ostro, B.; Brunekreef, B.; Kaufman, J.D. Long-term air pollution exposure and cardio-respiratory mortality: A review. Environ. Health 2013, 12, 43. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. AirQ+: Software Tool for Health Risk Assessment of Air Pollution. Available online: http://www.euro.who.int/en/health-topics/environment-and-health/air-quality/activities/airq-software-tool-for-health-risk-assessment-of-air-pollution (accessed on 26 January 2018).
- Mudu, P.; Gapp, C.; Dunbar, M. WHO AirQ+ tool: Methodologies to calculate the impacts of air pollution on health. In Proceedings of the 5th WeBIOPATR Workshop & Conference, Belgrade, Serbia, 14–16 October 2016; pp. 196–199. [Google Scholar]
- European Union (EC). Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on Ambient Air Quality and Cleaner Air for Europe; European Commission: Brussels, Belgium, 2008. [Google Scholar]
- HEATCO Developing Harmonized European Approaches for Transport Costing and Project Assessment—Deliverable 5: Proposal for Harmonized Guidelines. Available online: http://heatco.ier.uni-stuttgart.de/HEATCO_D5.pdf (accessed on 1 February 2006).
- Chanel, O.; Luchini, S. Monetary Values for Air Pollution Risk of Death: A Contingent Valuation Survey; Updated Mimeo of Working Paper # 2008-5; Working Papers Halshs-00272776; HAL: Marseille, France, 2012; Available online: https://halshs.archives-ouvertes.fr/halshs-00272776 (accessed on 26 February 2006).
- Methodology for the Cost–Benefit Analysis for CAFE: Volume 3—Uncertainty in the CAFE CBA. Available online: http://ec.europa.eu/environment/archives/cafe/ (accessed on 26 January 2018).
- The Organisation for Economic Co-operation and Development (OECD). Valuing Mortality Risk Reductions in Regulatory Analysis of Environmental, Health and Transport Policies: Policy Implications; OECD: Paris, France, 2011. [Google Scholar]
- Hammitt, J.K.; Robinson, L.A. The Income Elasticity of the Value per Statistical Life: Transferring Estimates between High and Low Income Populations. J. Benefit-Cost Anal. 2011, 2, 1–29. [Google Scholar] [CrossRef]
- Rabl, A.; Spadaro, J.; Holland, M. How Much Is Clean Air Worth?: Calculating the Benefits of Pollution Control; Cambridge Univ. Press: Cambridge, UK, 2014. [Google Scholar]
- The World Bank. FYR Macedonia: Green Growth Country Assessment; The World Bank: Washington, DC, USA, 2014. [Google Scholar]
- Meisner, C.; Gjorgjev, D.; Tozija, F. Estimating health impacts and economic costs of air pollution in the Republic of Macedonia. South East. Eur. J. Public Health 2015, 4. [Google Scholar] [CrossRef]
- European Environment Agency (EEA). Air Quality in Europe—2016 Report; EEA: Copenhagen, Denmark, 2016. [Google Scholar]
- Donevska, N. Trade-offs in sustainable urban development: The case of Skopje. J. Environ. Stud. Sci. 2017, 7, 152–159. [Google Scholar] [CrossRef]
- European Environment Agency (EEA). The Former Yugoslav Republic of Macedonia Country Briefing—The European Environment—State and Outlook 2015; EEA: Copenhagen, Denmark, 2015. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Centar (Traffic) | Gazi Baba (Background) | Karpos (Traffic) | Lisice (Industrial) | Rektorat (Traffic) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PM2.5 (mean, µg/m3) | 48.3 | n.a. | 41.6 | n.a. | n.a. | ||||||||||
| 13 December 2011 availability (% per year) | 28 | 91 | 85 | n.a. | 29 | 97 | 50 | n.a. | n.a. | ||||||
| PM10 (mean, µg/m3) | 79.2 | 84.4 | 68.3 | 108.6 | 71.7 | ||||||||||
| 13 December 2011 availability (% per year) | 28 | 91 | 90 | 3 | 58 | 58 | 29 | 97 | 91 | 86 | 92 | 98 | 21 | 96 | 99 |
| Health Endpoint (Specific Population) | ICD10 Codes | Relative Risk (RR) | Source |
|---|---|---|---|
| All-cause mortality excl. accidents (Adults 30 years and older) | A00-R99 | For 10 μg/m3 increase in PM2.5 RR = 1.062 (95% CI: 1.040–1.083) | [20] |
| Hospital admission for cardiovascular diseases (all ages) | I00-I52 | For 10 µg/m3 increases in PM2.5 RR = 1.0091 (95% CI: 1.0017–1.0166) | Air Pollution Epidemiology Database—APED [14] |
| Hospital admissions for respiratory diseases (all ages) | J00-J99 | For 10 µg/m3 increases in PM2.5 RR = 1.0190 (95% CI: 1.0190–1.0402) | Air Pollution Epidemiology Database—APED [14] |
| PM2.5 Ambient Concentrations | Life Expectancy (Years) | Loss of Life Expectancy * (Years) | Number of Deaths (Thousands) ** | Years of Life Lost (Thousands) |
|---|---|---|---|---|
| Current situation: 49.2 μg/m3 | 76.4 (at birth) | 2.8 (at birth) | 179.9 | 1813 |
| 16.3 (65 years) | 2.1 (65 years) | (123.2−227.9) | (1177−2413) | |
| Scenario 1: EU AQS (25 μg/m3) | 77.7 (at birth) | 1.4 (at birth) | 84.8 | 926.5 |
| 17.3 (65 years) | 1.1 (65 years) | (59.7−104.6) | (600.3−1235) | |
| Scenario 2: WHO AQG (10 μg/m3) | 78.6 (at birth) | 0.6 (at birth) | 32.4 | 372.0 |
| 18.0 (65 years) | 0.5 (65 years) | (23.2−39.4) | (240.7−496.6) |
| Morbidity | Current Situation | Scenario 1 EU Limits (95% CI) | Scenario 2 WHO AQG (95% CI) |
|---|---|---|---|
| Hospital admission for cardiovascular diseases | 547 (104–977) | 438 (83–784) | 272 (51–490) |
| Hospital admissions for respiratory disease | 937 (937–1869) | 753 (753–1516) | 472 (472–964) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez, G.S.; Spadaro, J.V.; Chapizanis, D.; Kendrovski, V.; Kochubovski, M.; Mudu, P. Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje. Int. J. Environ. Res. Public Health 2018, 15, 626. https://doi.org/10.3390/ijerph15040626
Martinez GS, Spadaro JV, Chapizanis D, Kendrovski V, Kochubovski M, Mudu P. Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje. International Journal of Environmental Research and Public Health. 2018; 15(4):626. https://doi.org/10.3390/ijerph15040626
Chicago/Turabian StyleMartinez, Gerardo Sanchez, Joseph V. Spadaro, Dimitris Chapizanis, Vladimir Kendrovski, Mihail Kochubovski, and Pierpaolo Mudu. 2018. "Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje" International Journal of Environmental Research and Public Health 15, no. 4: 626. https://doi.org/10.3390/ijerph15040626
APA StyleMartinez, G. S., Spadaro, J. V., Chapizanis, D., Kendrovski, V., Kochubovski, M., & Mudu, P. (2018). Health Impacts and Economic Costs of Air Pollution in the Metropolitan Area of Skopje. International Journal of Environmental Research and Public Health, 15(4), 626. https://doi.org/10.3390/ijerph15040626