Spatio-Temporal Epidemiology of Viral Hepatitis in China (2003–2015): Implications for Prevention and Control Policies




Abstract
:1. Introduction
2. Data and Methods
2.1. Study Setting and Data Resources
2.2. Time-Series Analysis
2.3. Spatial Clustering Analysis
2.3.1. Spatial Autocorrelation Analysis
2.3.2. Space-Time Scan Statistics
2.4. Software Tools
3. Results
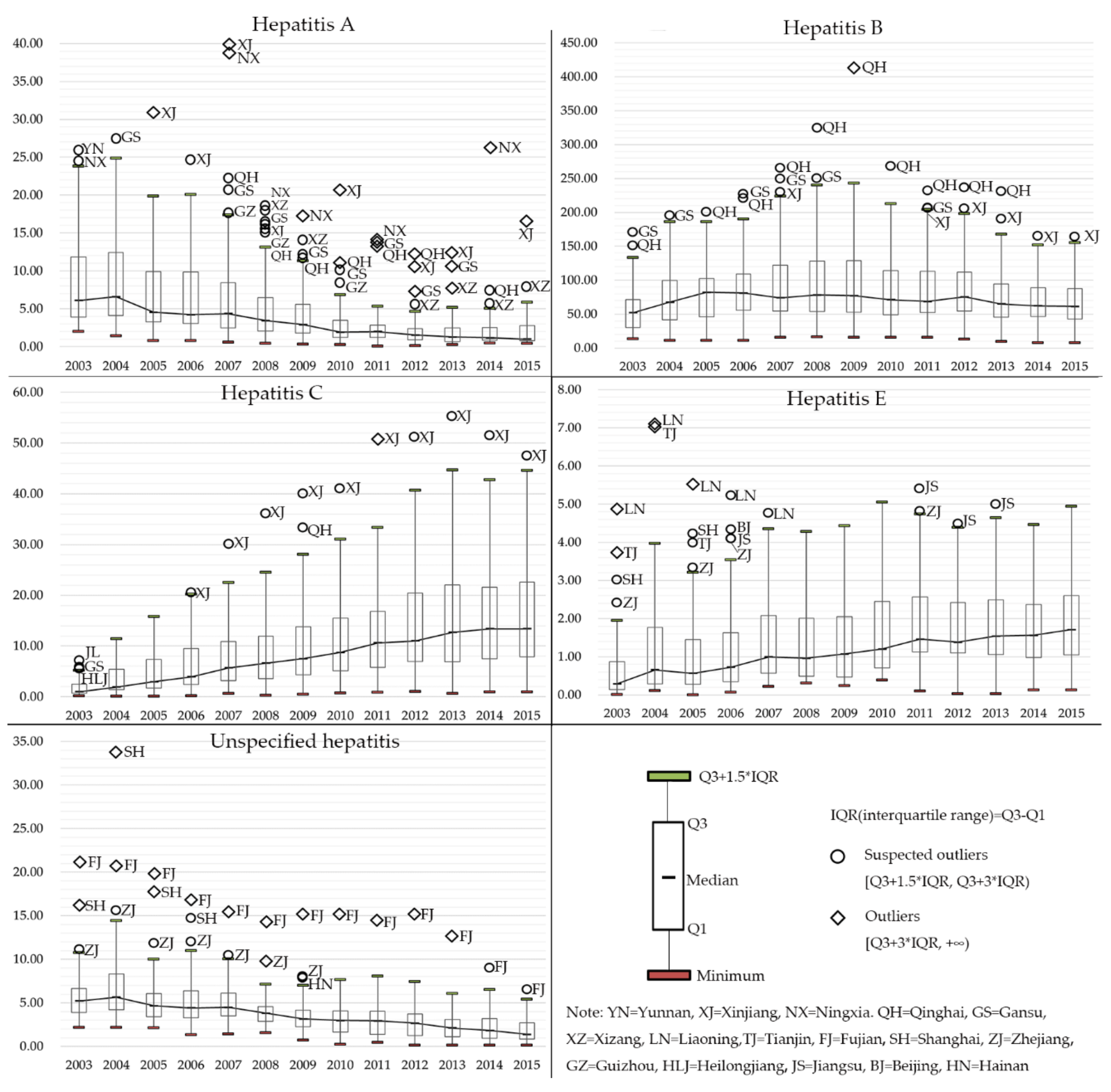
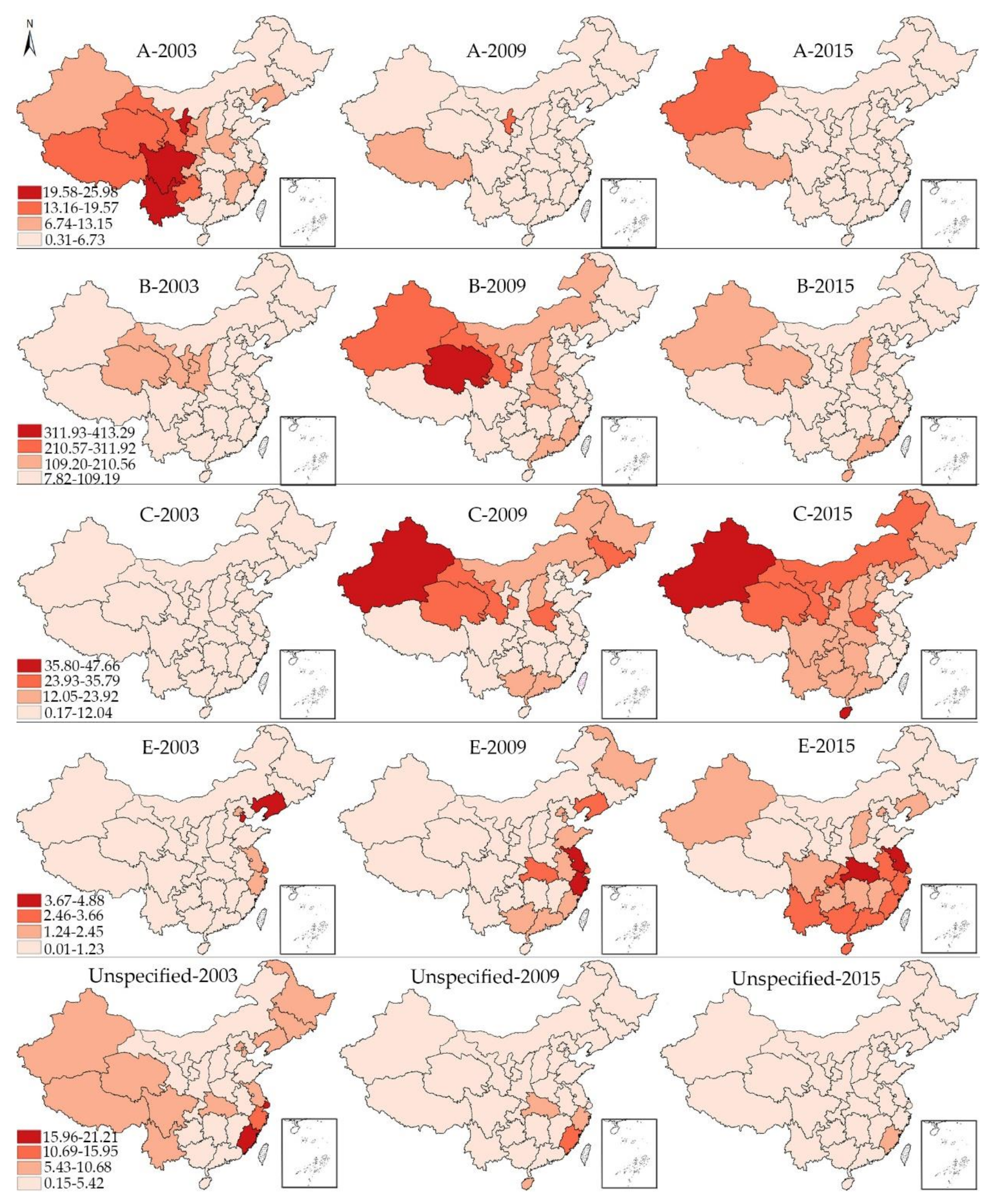
3.1. Epidemiologic Trends
3.2. Global Spatial Autocorrelation
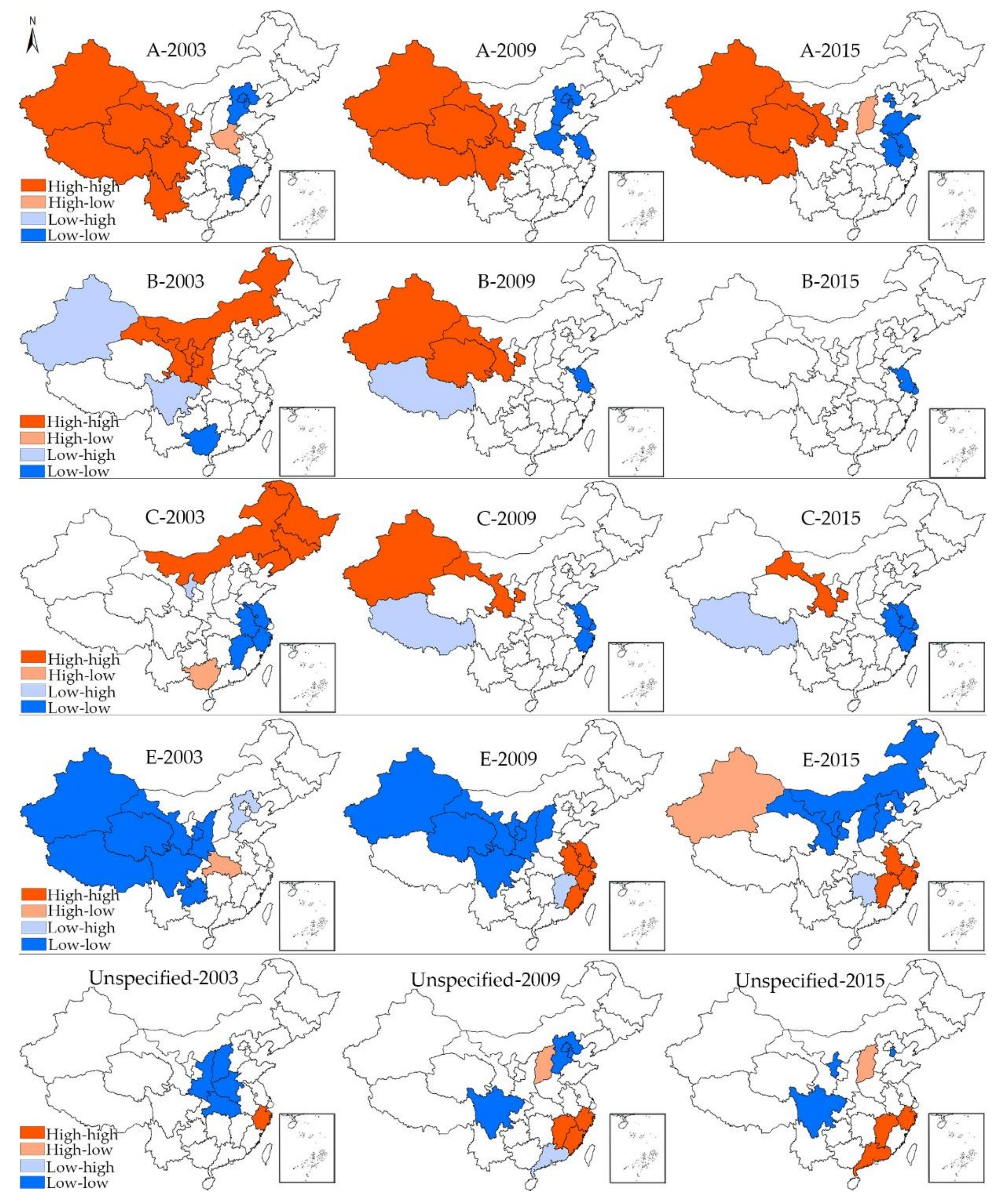
3.3. Local Spatial Autocorrelation
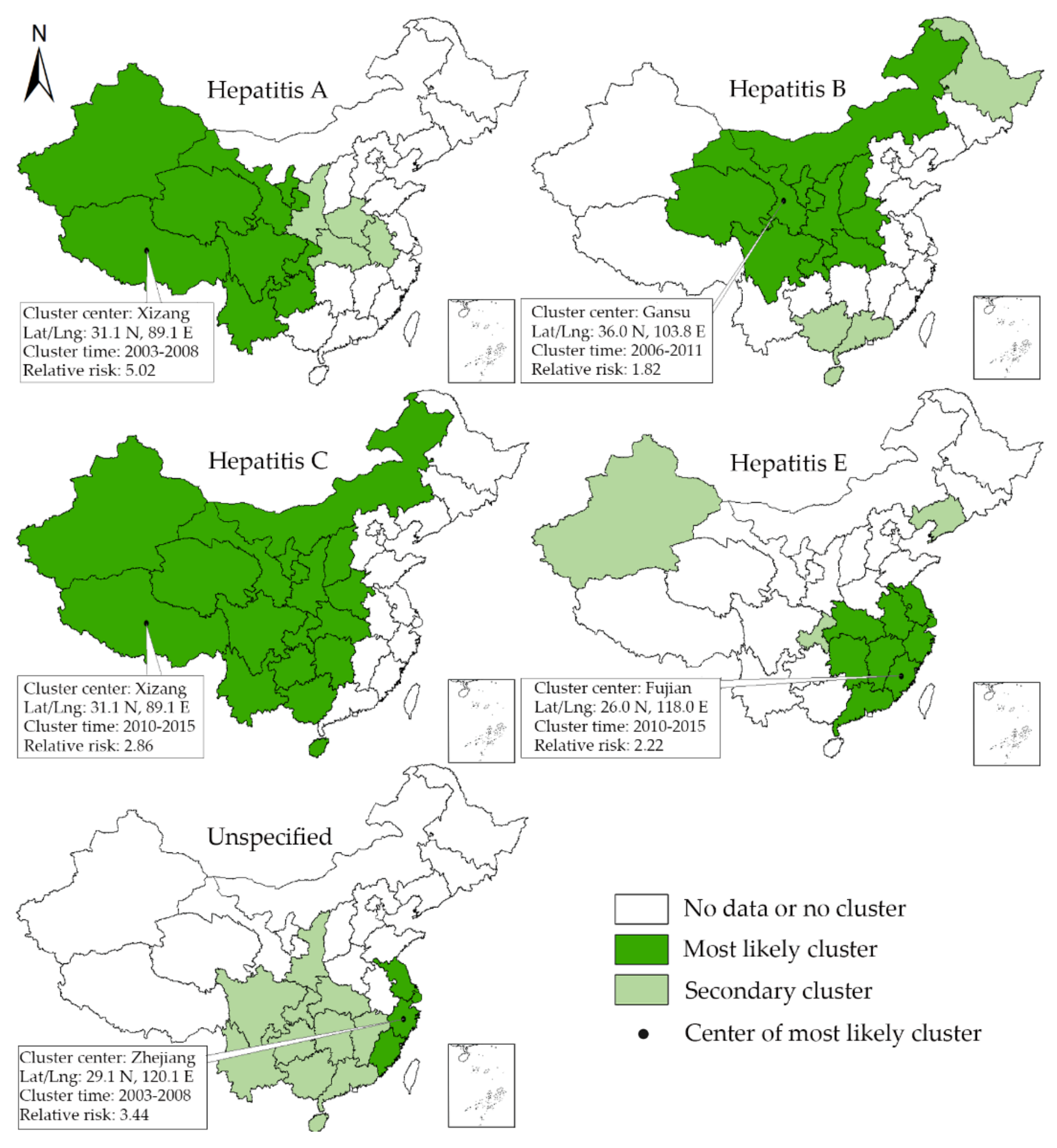
3.4. Space-Time Scan Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Conflicts of Interest
References
- World Health Organization. Health in 2015: From MDGs to SDGs; World Health Organization: Genova, Switherland, 2015. [Google Scholar]
- World Health Organization. Global Health Sector Steategy on Sexually Transmitted Infections 2016–2021: Towards Ending STIs; World Health Organization: Genova, Switherland, 2016. [Google Scholar]
- World Health Organization. Global Health Sector Strategy on Viral Hepatitis 2016–2021; World Health Organization: Genova, Switherland, 2016. [Google Scholar]
- Wu, W.; Chen, J.; Haiyan, H.; Zhao, Y.; Li, C. Analysis on the characteristics and revision of reported non-type viral hepatitis in Tianjin (2004–2013). Chin. J. Public Health Prev. Med. 2015, 26, 7–9. [Google Scholar]
- Zhang, L.; Wilson, D.P. Trends in notifiable infectious diseases in Vhina: Implications for surveillance and population health policy. PLoS ONE 2012, 7. [Google Scholar] [CrossRef]
- Fung, I.C.H.; Hao, Y.; Cai, J.; Ying, Y.; Schaible, B.J.; Yu, C.M.; Tse, Z.T.H.; Fu, K.W. Chinese social media reaction to information about 42 notifiable infectious diseases. PLoS ONE 2015, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Xiang, R.; Wu, P.; Liping, W.; Geng, M.; Zeng, L.; Zhang, J.; Xia, N.; Lai, S.; Dalton, H.R.; Cowling, B.J.; et al. Changing Epidemiology of Hepatitis A and Hepatitis E Viruses in China, 1990–2014. Emerg. Infect. Dis. 2017, 23, 1–4. [Google Scholar]
- Sumi, A.; Luo, T.; Zhou, D.; Yu, B.; Kong, D.; Kobayashi, N. Time-series analysis of hepatitis A, B, C and E infections in a large Chinese city: Application to prediction analysis. Epidemiol. Infect. 2013, 141, 905–915. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zhou, Y.; Lin, X.; Jiang, Y.; Tian, R.; Zhang, Y.; Wu, J.; Zhang, F.; Zhang, Y.; Wang, Y.; et al. General Epidemiological Parameters of Viral Hepatitis A, B, C, and E in Six Regions of China: A Cross-Sectional Study in 2007. PLoS ONE 2009, 4, 14–16. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Qi, W.; Wang, X.; Zhang, Y.; Xu, Y.; Qin, S.; Zhao, P.; Guo, H.; Jiao, J.; Zhou, C.; et al. Epidemiology of Hepatitis B and Hepatitis C Infections and Bene fi ts of Programs for Hepatitis Prevention in Northeastern China: A Cross-Sectional Study. Clin. Infect. Dis. 2017, 62, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Jia, Z.; Yi, Y.; Liu, J.; Cao, J.; Zhang, Y.; Tian, R.; Yu, T.; Wang, H.; Wang, X.; Su, Q.; et al. Epidemiology of hepatitis e virus in China: Results from the Third National Viral Hepatitis Prevalence Survey, 2005–2006. PLoS ONE 2014, 9, 2005–2006. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Xing, J.; Chen, F.; Yan, R.; Ge, L.; Qin, Q.; Wang, L.; Ding, Z.; Guo, W.; Wang, N. Spatial Analysis on Hepatitis C Virus Infection in Mainland China: From 2005 to 2011. PLoS ONE 2014, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Fu, Y.; Liu, J.; Mao, Y. Notifiable sexually transmitted infections in China: Epidemiologic trends and spatial changing patterns. Sustainability 2017, 9, 1784. [Google Scholar] [CrossRef]
- Hu, Y.; Xiong, C.; Zhang, Z.; Luo, C.; Cohen, T.; Gao, J.; Zhang, L.; Jiang, Q. Changing patterns of spatial clustering of schistosomiasis in southwest China between 1999–2001 and 2007–2008: Assessing progress toward eradication after the World bank loan project. Int. J. Environ. Res. Public Health 2014, 11, 701–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, M.M.; Griffith, D.A. Modeling spatial autocorrelation in spatial interaction data: An application to patent citation data in the european union. J. Reg. Sci. 2008, 48, 969–989. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, X.; Liu, Y.; Sun, D.; Ding, S.; Zhang, B.; Du, Z.; Xue, F. Detecting Spatial-Temporal Clusters of HFMD from 2007 to 2011 in Shandong Province, China. PLoS ONE 2013, 8, e63447. [Google Scholar] [CrossRef] [PubMed]
- Xia, J.; Cai, S.; Zhang, H.; Lin, W.; Fan, Y.; Qiu, J.; Sun, L.; Chang, B.; Zhang, Z.; Nie, S. Spatial, temporal, and spatiotemporal analysis of malaria in Hubei Province, China from 2004–2011. Malar. J. 2015, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ge, E.; Zhang, X.; Wang, X.; Wei, X. Spatial and temporal analysis of tuberculosis in Zhejiang Province, China, 2009-2012. Infect. Dis. Poverty 2016, 5, 11. [Google Scholar] [CrossRef] [PubMed]
- Varga, C.; Pearl, D.L.; McEwen, S.A.; Sargeant, J.M.; Pollari, F.; Guerin, M.T. Area-level global and local clustering of human Salmonella Enteritidis infection rates in the city of Toronto, Canada, 2007–2009. BMC Infect. Dis. 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Abbas, T.; Younus, M.; Muhammad, S.A. Spatial cluster analysis of human cases of Crimean Congo hemorrhagic fever reported in Pakistan. Infect. Dis. Poverty 2015, 4, 9. [Google Scholar] [CrossRef] [PubMed]
- Martins-Melo, F.R.; Cristhiany, M.; Pinheiro, C.; Ramos, N.A., Jr.; Alencar, C.H.; Schemelzer, F.; Bezerra, D.M. Spatiotemporal Patterns of Schistosomiasis- Related Deaths, Brazil, 2000–2011. Emerg. Infect. Dis. 2015, 21, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Anselin, L. Local Indicators of Spatial Association—Lisa. Geogr. Anal. 1995, 27, 93–115. [Google Scholar] [CrossRef]
- Anselin, L.; Syabri, I.; Kho, Y. An Introduction to Spatial Data Analysis. Geogr. Anal. 2006, 38, 5–22. [Google Scholar] [CrossRef]
- Qi, L.; Tang, W.; Zhao, H.; Ling, H.; Su, K.; Zhao, H.; Li, Q.; Shen, T. Epidemiological characteristics and spatial-temporal distribution of hand, foot, and mouth disease in Chongqing, China, 2009–2016. Int. J. Environ. Res. Public Health 2018, 15. [Google Scholar] [CrossRef] [PubMed]
- Deng, T.; Huang, Y.; Yu, S.; Gu, J.; Huang, C.; Xiao, G.; Hao, Y. Spatial-Temporal Clusters and Risk Factors of Hand, Foot, and Mouth Disease at the District Level in Guangdong Province, China. PLoS ONE 2013, 8, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Jia, J.D.; Yao, G.B. Achieving ultimate control of hepatitis B infection in China: Progress and challenges. J. Viral Hepat. 2010, 17, 2–3. [Google Scholar] [CrossRef] [PubMed]
- Cui, F.; Liang, X.; Gong, X.; Chen, Y.; Wang, F.; Zheng, H.; Wu, Z.; Miao, N.; Hadler, S.C.; Hutin, Y.J.; et al. Preventing hepatitis B though universal vaccination: Reduction of inequalities through the GAVI China project. Vaccine 2013, 31, J29–J35. [Google Scholar] [CrossRef] [PubMed]
- Vellozzi, C.; Averhoff, F. An opportunity for further control of hepatitis B in China? Lancet Infect. Dis. 2016, 16, 10–11. [Google Scholar] [CrossRef]
- Qiu, Y.; Ren, J.; Yao, J. Healthy adult vaccination: An urgent need to prevent hepatitis B in China. Hum. Vaccines Immunother. 2016, 12, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.-L.; Qiao, Y.-P.; Wang, L.-H.; Fang, L.-W.; Wang, F.; Jin, X.; Qiu, J.; Wang, X.-Y.; Wang, Q.; Wu, J.-L.; et al. Integrated prevention of mother-to-child transmission for human immunodeficiency virus, syphilis and hepatitis B virus in China. Bull. World Health Org. 2015, 93, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zeng, T.; Liu, J.-Y.; Lei, Y.; Zhong, S.; Sheng, Y.-J.; Zhou, Z.; Ren, H. Measures to Reduce Mother-to-Child Transmission of Hepatitis B Virus in China: A Meta-Analysis. Dig. Dis. Sci. 2014, 59, 242–258. [Google Scholar] [CrossRef] [PubMed]
- Zou, X.; Chow, E.P.; Zhao, P.; Xu, Y.; Ling, L.; Zhang, L. Rural-to-urban migrants are at high risk of sexually transmitted and viral hepatitis infections in China: A systematic review and meta-analysis. BMC Infect. Dis. 2014, 14, 490. [Google Scholar] [CrossRef] [PubMed]
- Su, S.; Chow, E.P.F.; Muessig, K.E.; Yuan, L.; Tucker, J.D.; Zhang, X.; Ren, J. Sustained high prevalence of viral hepatitis and sexually transmissible infections among female sex workers in China: A systematic review and meta-analysis. BMC Infect. Dis. 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Murray, J.M. Roadmap to control HBV and HDV epidemics in China. J. Theor. Biol. 2017, 423, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Long, Y.; Wang, T.; Xiao, D.; Zhang, J.; Guo, Z.; Wang, B.; Yan, Y. Epidemiology of Hepatitis C Virus Infection in Highly Endemic HBV Areas in China. PLoS ONE 2013, 8, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Jia, J. Update on epidemiology of hepatitis B and C in China. J. Gastroenterol. Hepatol. 2013, 28, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Provinces, Y. Global health lessons from HIV and hepatitis co-infection in China. Hepatol. Res. 2010, 40, 248–250. [Google Scholar] [CrossRef]
- Zhao, R.; Peng, J.; Tang, L.; Huang, H.; Liu, M.; Kong, W.; Pang, B. Epidemiological Distribution and Genotype Characterization of Hepatitis C Virus and HIV Co-Infection in Wuhan, China, Where the Prevalence of HIV is Low. J. Med. Virol. 2013, 85, 1712–1723. [Google Scholar] [CrossRef] [PubMed]
- Zhang, F.; Zhu, H.; Wu, Y.; Dou, Z.; Zhang, Y.; Kleinman, N.; Bulterys, M.; Wu, Z.; Ma, Y.; Zhao, D.; et al. HIV, hepatitis B virus, and hepatitis C virus co-infection in patients in the China national free antiretroviral treatment program, 2010–2012: A retrospective observational cohort study. Lancet Infect. Dis. 2014, 14, 1065. [Google Scholar] [CrossRef]
- Zhang, C.; Li, X.; Liu, Y.; Qiao, S.; Chen, Y.; Zhou, Y.; Shen, Z. Co-infections of tuberculosis, hepatitis B or C viruses in a cohort of people living with HIV/AIDS in China: Predictors and sequelae. AIDS Care 2017, 29, 974–977. [Google Scholar] [CrossRef] [PubMed]
- Zhibin, Q.; Jun, L.; Yang, Y.; Meilan, L.; Jianguang, W. Prevelance of hepatitis A, C, E and unclassified hepatitis, Weihai City, 2011–2013. Prev. Med. Trib. 2015, 21, 937–942. (In Chinese) [Google Scholar] [CrossRef]
- Gibney, K.B.; Cheng, A.C.; Hall, R.; Leder, K. An overview of the epidemiology of notifiable infectious diseases in Australia, 1991–2011. Epidemiol. Infect. 2016, 144, 3263–3277. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Region | Hepatitis A | Hepatitis B | Hepatitis C | Hepatitis E | Unspecificied Hepatitis | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 03growth09 | 09growth15 | 03growth09 | 09growth15 | 03growth09 | 09growth15 | 03growth09 | 09growth15 | 03growth09 | 09growth15 | |
| Beijing | 3.69(−75%)**0.92 | 0.92(−46%)0.50 | 16.48(37%)22.54 | 22.54(−65%)**7.82 | 1.79(393%)*8.83 | 8.83(−54%)**4.07 | 1.56(49%)2.32 | 2.32(−45%)**1.28 | 7.59(−86%)**1.10 | 1.10(−86%)**0.15 |
| Tianjin | 2.11(−85%)**0.31 | 0.31(39%)0.43 | 23.05(−11%)20.59 | 20.59(−39%)**12.51 | 1.42(138%)3.38 | 3.38(19%)4.02 | 3.76(−62%)*1.42 | 1.42(−54%)**0.66 | 8.66(−80%)**1.75 | 1.75(−71%)**0.50 |
| Hebei | 3.12(−64%)**1.13 | 1.13(−37%)*0.71 | 57.57(42%)**82.00 | 82.00(−10%)73.94 | 0.73(649%)**5.47 | 5.47(133%)**12.74 | 0.56(107%)1.16 | 1.16(−10%)1.04 | 3.53(−54%)**1.62 | 1.62(−43%)**0.93 |
| Shanxi | 3.82(−44%)**2.14 | 2.14(43%)**3.05 | 30.95(305%)**125.34 | 125.34(−1%)124.54 | 1.62(753%)**13.82 | 13.82(69%)**23.31 | 0.20(90%)0.38 | 0.38(334%)**1.65 | 2.85(32%)3.76 | 3.76(−39%)*2.31 |
| Neimenggu | 5.90(−66%)**2.00 | 2.00(−61%)0.79 | 73.06(81%)**132.48 | 132.48(−34%)**87.94 | 3.33(472%)**19.04 | 19.04(45%)**27.52 | 0.23(35%)0.31 | 0.31(142%)**0.75 | 2.47(−40%)1.47 | 1.47(−76%)**0.36 |
| Liaoning | 11.46(−71%)**3.36 | 3.36(32%)4.44 | 36.72(76%)**64.52 | 64.52(−30%)**44.87 | 4.95(161%)**12.92 | 12.92(55%)**20.05 | 4.88(−41%)*2.88 | 2.88(−23%)*2.21 | 7.63(−30%)**5.36 | 5.36(−32%)**3.62 |
| Jilin | 6.33(−74%)**1.64 | 1.64(−51%)**0.81 | 46.03(42%)**65.18 | 65.18(−37%)40.86 | 7.65(250%)**26.74 | 26.74(−13%)23.17 | 0.79(33%)1.05 | 1.05(0%)1.05 | 6.95(−39%)**4.24 | 4.24(−78%)**0.94 |
| Heilongjiang | 4.74(−78%)**1.03 | 1.03(−38%)**0.64 | 57.27(−8%)52.92 | 52.92(−50%)**26.69 | 5.49(152%)**13.84 | 13.84(−8%)12.77 | 0.85(64%)1.39 | 1.39(−21%)**1.10 | 5.74(−35%)**3.74 | 3.74(−48%)**1.93 |
| Shanghai | 3.83(−66%)**1.29 | 1.29(−37%)0.81 | 16.87(79%)30.20 | 30.20(15%)34.74 | 0.96(88%)**1.80 | 1.80(310%)**7.38 | 3.04(−12%)2.69 | 2.69(6%)2.84 | 16.25(−86%)**2.29 | 2.29(−68%)**0.73 |
| Jiangsu | 3.99(−54%)**1.83 | 1.83(−54%)**0.84 | 18.40(1%)18.60 | 18.60(−3%)17.95 | 0.81(190%)**2.35 | 2.35(69%)**3.97 | 1.49(183%)**4.22 | 4.22(−10%)3.81 | 10.37(−51%)**5.12 | 5.12(−42%)**2.98 |
| Zhejiang | 7.40(−71%)**2.11 | 2.11(−60%)**0.84 | 66.17(−2%)64.83 | 64.83(−64%)**23.57 | 0.86(340%)**3.78 | 3.78(28%)4.82 | 2.41(55%)3.73 | 3.73(−15%)3.16 | 12.79(−38%)**7.96 | 7.96(−68%)**2.56 |
| Anhui | 5.75(−70%)**1.74 | 1.74(−43%)**0.99 | 44.72(18%)**52.58 | 52.58(17%)*61.28 | 0.57(509%)**3.47 | 3.47(200%)**10.40 | 0.33(588%)**2.27 | 2.27(15%)2.61 | 3.98(−4%)3.82 | 3.82(1%)3.87 |
| Fujian | 6.12(−51%)**2.99 | 2.99(−53%)**1.42 | 76.61(89%)**144.92 | 144.92(−11%)*129.41 | 0.38(1192%)**4.91 | 4.91(53%)**7.50 | 0.30(510%)**1.83 | 1.83(37%)2.50 | 21.21(−29%)**15.02 | 15.02(−55%)**6.76 |
| Jiangxi | 8.84(−66%)**3.03 | 3.03(−80%)**0.61 | 59.54(37%)81.33 | 81.33(5%)85.23 | 0.50(528%)**3.14 | 3.14(165%)**8.32 | 0.22(386%)**1.07 | 1.07(70%)1.82 | 4.96(−18%)4.09 | 4.09(−44%)**2.29 |
| Shandong | 2.45(−78%)**0.55 | 0.55(−4%)0.53 | 31.89(12%)35.65 | 35.65(37%)**48.75 | 0.30(423%)**1.57 | 1.57(169%)**4.22 | 0.91(40%)1.27 | 1.27(−3%)1.23 | 3.57(−37%)**2.26 | 2.26(−44%)**1.26 |
| Henan | 11.34(−62%)**4.28 | 4.28(−90%)**0.41 | 69.84(141%)**168.34 | 168.34(−62%)**63.62 | 2.05(1081%)**24.21 | 24.21(8%)26.22 | 0.08(425%)**0.42 | 0.42(52%)0.64 | 2.18(−33%)1.47 | 1.47(−69%)**0.45 |
| Hubei | 6.01(−45%)**3.29 | 3.29(−55%)**1.47 | 81.49(71%)**139.63 | 139.63(−24%)**106.43 | 1.01(732%)**8.40 | 8.40(79%)**15.02 | 0.88(220%)**2.82 | 2.82(42%)**4.00 | 5.79(4%)6.03 | 6.03(−44%)**3.38 |
| Hunan | 3.29(−40%)1.96 | 1.96(−53%)**0.92 | 29.67(115%)**63.72 | 63.72(27%)**80.70 | 0.74(857%)**7.08 | 7.08(175%)**19.45 | 0.10(610%)**0.71 | 0.71(141%)**1.71 | 2.23(41%)**3.15 | 3.15(−26%)2.33 |
| Guangdong | 2.00(−8%)1.85 | 1.85(−16%)1.55 | 29.72(361%)**137.10 | 137.10(−2%)134.56 | 0.89(1382%)**13.19 | 13.19(49%)**19.64 | 0.49(388%)**2.39 | 2.39(7%)2.55 | 3.81(−10%)3.43 | 3.43(−37%)**2.15 |
| Guangxi | 4.27(−32%)*2.92 | 2.92(−48%)**1.53 | 55.76(53%)**85.21 | 85.21(2%)87.13 | 2.51(573%)**16.89 | 16.89(14%)19.18 | 0.29(338%)**1.27 | 1.27(155%)**3.24 | 4.48(−3%)4.33 | 4.33(−21%)3.44 |
| Hainan | 5.88(−49%)2.99 | 2.99(−70%)**0.91 | 52.09(41%)73.35 | 73.35(74%)**127.63 | 0.64(1075%)**7.52 | 7.52(393%)**37.09 | 0.01(4200%)**0.43 | 0.43(519%)**2.66 | 4.55(74%)**7.92 | 7.92(−62%)**3.02 |
| Chongqing | 12.29(−56%)**5.35 | 5.35(−45%)**2.93 | 81.55(−9%)74.10 | 74.10(−11%)66.03 | 0.81(616%)**5.80 | 5.80(126%)**13.08 | 0.13(354%)**0.59 | 0.59(410%)**3.01 | 4.95(−29%)**3.49 | 3.49(−64%)**1.24 |
| Sichuan | 20.09(−71%)**5.84 | 5.84(−50%)**2.93 | 44.78(72%)77.10 | 77.10(−39%)**47.39 | 0.56(923%)**5.73 | 5.73(113%)**12.23 | 0.12(442%)**0.65 | 0.65(123%)*1.45 | 6.32(−41%)**3.70 | 3.70(−63%)**1.38 |
| Guizhou | 17.71(−46%)9.62 | 9.62(−88%)**1.11 | 24.57(286%)**94.88 | 94.88(−38%)**58.71 | 0.98(556%)**6.43 | 6.43(109%)**13.42 | 0.60(−42%)0.35 | 0.35(394%)**1.73 | 4.02(−27%)2.94 | 2.94(−67%)**0.96 |
| Yunnan | 25.98(−67%)*8.65 | 8.65(−68%)**2.74 | 13.53(238%)*45.75 | 45.75(−1%)45.25 | 0.17(5541%)**9.59 | 9.59(129%)**22.00 | 0.03(3733%)**1.15 | 1.15(126%)**2.60 | 6.17(−81%)**1.18 | 1.18(−75%)**0.29 |
| Xizang | 14.15(−1%)14.04 | 14.04(−43%)7.97 | 64.42(−76%)15.64 | 15.64(403%)**78.73 | 1.21(−60%)0.49 | 0.49(100%)0.98 | 0.15(60%)0.24 | 0.24 (−46%)0.13 | 5.90(−88%)**0.73 | 0.73(90%)1.39 |
| Shaanxi | 9.60(−73%)**2.62 | 2.62(−62%)**1.00 | 127.35(−33%)**85.68 | 85.68(−28%)**61.38 | 2.82(259%)**10.12 | 10.12(88%)**19.05 | 0.18(128%)*0.41 | 0.41(78%)0.73 | 5.21(−51%)**2.53 | 2.53(−69%)**0.79 |
| Gansu | 18.61(−35%)12.15 | 12.15(−76%)**2.89 | 172.46(37%)**237.04 | 237.04(−84%)**38.78 | 5.95(323%**)25.17 | 25.17(4%)26.21 | 0.08(263%)**0.29 | 0.29(66%)*0.48 | 3.49(−18%)2.86 | 2.86(−62%)**1.08 |
| Qinghai | 18.64(−37%)11.71 | 11.71(−51%)*5.79 | 153.14(170%)**413.29 | 413.29(−65%)**146.31 | 3.57(838%)**33.47 | 33.47(2%)34.14 | 0.11(536%)**0.70 | 0.70(76%)*1.23 | 6.00(−56%)**2.63 | 2.63(−49%)*1.35 |
| Ningxia | 24.36(−30%)17.17 | 17.17(−87%)*2.24 | 130.09(−14%)112.19 | 112.19(−61%)**44.02 | 1.25(334%)**5.42 | 5.42(124%)**12.15 | 0.18(178%)**0.50 | 0.50(−52%)0.24 | 5.19(−45%)2.84 | 2.84(−80%)**0.56 |
| Xinjiang | 11.24(−21%)8.88 | 8.88(86%)16.52 | 50.62(319%)**211.91 | 211.91(−22%)*164.31 | 2.49(1507%)**40.02 | 40.02(19%)47.66 | 0.18(467%)**1.02 | 1.02(123%)**2.27 | 5.73(−47%)3.06 | 3.06(−8%)*2.81 |
| SUM | 7.37(−55%)**3.30 | 3.30(−50%)**1.66 | 53.32(67%)**88.82 | 88.82(−23%)**68.57 | 1.57(532%)**9.93 | 9.93(54%)**15.26 | 0.72(113%)**1.53 | 1.53(30%)1.99 | 5.57(−33%)**3.72 | 3.72(−47%)**1.98 |
| Year | Hepatitis A | Hepatitis B | Hepatitis C | Hepatitis E | Unclassified Hepatitis | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Moran’s I | Z-Value | p-Value | Moran’s I | Z-Value | p-Value | Moran’s I | Z-Value | p-Value | Moran’s I | Z-Value | p-Value | Moran’s I | Z-Value | p-Value | |
| 2003 | 0.4605 | 4.3622 | 0.0002 | 0.3486 | 3.4146 | 0.0029 | 0.5125 | 5.0126 | 0.0003 | 0.2093 | 2.3184 | 0.0256 | 0.3084 | 3.3259 | 0.0054 |
| 2004 | 0.5586 | 5.1435 | 0.0002 | 0.3801 | 3.6752 | 0.0013 | 0.4496 | 4.2313 | 0.0005 | 0.2941 | 3.0198 | 0.0083 | 0.3298 | 3.8927 | 0.0020 |
| 2005 | 0.5082 | 5.2675 | 0.0001 | 0.3446 | 3.3712 | 0.0017 | 0.3965 | 3.7419 | 0.0008 | 0.3620 | 3.5710 | 0.0024 | 0.3279 | 3.5401 | 0.0041 |
| 2006 | 0.5262 | 5.1908 | 0.0001 | 0.3172 | 3.1546 | 0.0046 | 0.2800 | 2.7817 | 0.0069 | 0.3868 | 3.7780 | 0.0011 | 0.3369 | 3.5350 | 0.0035 |
| 2007 | 0.3813 | 3.8694 | 0.0022 | 0.3317 | 3.2922 | 0.0027 | 0.2709 | 2.7911 | 0.0072 | 0.3577 | 3.3243 | 0.0029 | 0.2346 | 2.6270 | 0.0108 |
| 2008 | 0.5486 | 5.1385 | 0.0001 | 0.3186 | 3.2575 | 0.0029 | 0.2585 | 2.7350 | 0.0085 | 0.3990 | 3.7677 | 0.0009 | 0.2724 | 3.1474 | 0.0049 |
| 2009 | 0.4961 | 4.7851 | 0.0002 | 0.2510 | 2.8569 | 0.0066 | 0.2835 | 2.8584 | 0.0072 | 0.4314 | 4.1267 | 0.0005 | 0.1994 | 2.4228 | 0.0160 |
| 2010 | 0.4449 | 5.0161 | 0.0005 | 0.2881 | 2.9339 | 0.0060 | 0.2670 | 2.6532 | 0.0104 | 0.4378 | 4.0594 | 0.0003 | 0.1668 | 2.1739 | 0.0245 |
| 2011 | 0.5467 | 5.5616 | 0.0006 | 0.3382 | 3.3336 | 0.0028 | 0.2438 | 2.5212 | 0.0133 | 0.4265 | 4.1490 | 0.0004 | 0.1880 | 2.3237 | 0.0175 |
| 2012 | 0.6636 | 6.8015 | 0.0001 | 0.2644 | 2.6571 | 0.0101 | 0.2317 | 2.4156 | 0.0164 | 0.3042 | 2.9360 | 0.0044 | 0.1463 | 2.1520 | 0.0208 |
| 2013 | 0.6226 | 6.4308 | 0.0002 | 0.1740 | 1.8903 | 0.0420 | 0.2293 | 2.4237 | 0.0146 | 0.2898 | 2.8619 | 0.0055 | 0.0943 | 1.3990 | 0.0812 |
| 2014 | 0.2434 | 4.7610 | 0.0006 | 0.2247 | 2.2409 | 0.0209 | 0.2245 | 2.3661 | 0.0151 | 0.2885 | 2.8319 | 0.0064 | 0.1152 | 1.4535 | 0.0821 |
| 2015 | 0.4039 | 5.1859 | 0.0005 | 0.2565 | 2.5737 | 0.0097 | 0.2209** | 2.2592 | 0.0199 | 0.3572 | 3.4000 | 0.0013 | 0.1402 | 1.5063 | 0.0648 |
| Type of Viral Hepatitis | Cluster Type | Location | Location IDs Included | Coordinates | Radius (Km) | Time (Year) | Number of Cases | Expected Cases | Annual Cases/100,000 | RELATIVE RISK | LLR | p-Value |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | Most likely cluster | Xizang | Xizang, Qinghai, Xinjiang, Sichuan, Yunnan, Gansu, Ningxia, Guizhou, Chongqing | 31.1 N, 89.1 E | 1790.28 | 2003–2008 | 225,471 | 61,027.91 | 14.7 | 5.02 | 154,163.66 | <0.001 |
| A | Secondary cluster | Henan | Henan, Hubei, Anhui, Shaanxi | 33.8 N, 113.6 E | 445.66 | 2003–2004 | 40,424 | 20,496.61 | 7.8 | 2.03 | 7829.79 | <0.001 |
| B | Most likely cluster | Gansu | Gansu, Ningxia, Shaanxi, Sichuan, Qinghai, Chongqing, Shanxi, Neimenggu, Henan, Hubei | 36.0 N, 103.8 E | 1023.00 | 2006–2011 | 3,010,858 | 1,839,009.52 | 127.0 | 1.82 | 374,337.42 | <0.001 |
| B | Secondary cluster | Hainan | Hainan, Guangxi, Guangdong | 19.2 N, 109.8 E | 583.68 | 2010–2015 | 1,160,486 | 754,743.36 | 119.3 | 1.59 | 100,129.46 | <0.001 |
| B | Secondary cluster | Heilongjiang | Heilongjiang | 46.8 N, 127.9 E | — | 2004–2005 | 63,354 | 59,295.19 | 82.9 | 1.07 | 136.47 | <0.001 |
| C | Most likely cluster | Xizang | Xizang, Qinghai, Xinjiang, Sichuan, Yunnan, Gansu, Ningxia, Guizhou, Chongqing, Shaanxi, Guangxi, Hunan, Shanxi, Neimenggu, Hubei, Henan, Hainan | 31.1 N, 89.1 E | 2454.71 | 2010–2015 | 743,192 | 366,284.22 | 19.7 | 2.86 | 209,702.96 | <0.001 |
| E | Most likely cluster | Fujian | Fujian, Jiangxi, Zhejiang, Guangdong, Anhui, Hunan, Shanghai, Hubei, Jiangsu | 26.0 N, 118.0 E | 742.95 | 2010–2015 | 95,534 | 52769.84 | 3.0 | 2.22 | 18,154.26 | <0.001 |
| E | Secondary cluster | Liaoning | Liaoning | 41.5 N, 123.5 E | — | 2003–2008 | 13,013 | 4225.54 | 5.1 | 3.18 | 5988.83 | <0.001 |
| E | Secondary cluster | Chongqing | Chongqing | 29.8 N, 107.8 E | — | 2013–2015 | 2759 | 1483.82 | 3.1 | 1.87 | 438.96 | <0.001 |
| E | Secondary cluster | Xinjiang | Xinjiang | 42.0 N, 85.7 E | — | 2015 | 535 | 388.91 | 2.3 | 1.38 | 24.57 | <0.001 |
| Unspeficied | Most likely cluster | Zhejiang | Zhejiang, Shanghai, Jiangsu, Fujian | 29.1 N, 120.1 E | 400.88 | 2003–2008 | 129,643 | 43,380.75 | 12.1 | 3.44 | 61,614.92 | <0.001 |
| Unspeficied | Secondary cluster | Guizhou | Guizhou, Chongqing, Guangxi, Hunan, Sichuan, Yunnan, Guangdong, Hubei, Shaanxi, Hainan, Jiangxi | 26. 7 N, 106.6 E | 899.36 | 2003–2007 | 127,014 | 110,380.63 | 4.7 | 1.18 | 1432.19 | <0.001 |
| Unspeficied | Secondary cluster | Xinjiang | Xinjiang | 42.0 N, 85.7 E | — | 2004–2007 | 6704 | 3297.72 | 8.3 | 2.04 | 1358.39 | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, B.; Liu, J.; Fu, Y.; Zhang, B.; Mao, Y. Spatio-Temporal Epidemiology of Viral Hepatitis in China (2003–2015): Implications for Prevention and Control Policies. Int. J. Environ. Res. Public Health 2018, 15, 661. https://doi.org/10.3390/ijerph15040661
Zhu B, Liu J, Fu Y, Zhang B, Mao Y. Spatio-Temporal Epidemiology of Viral Hepatitis in China (2003–2015): Implications for Prevention and Control Policies. International Journal of Environmental Research and Public Health. 2018; 15(4):661. https://doi.org/10.3390/ijerph15040661
Chicago/Turabian StyleZhu, Bin, Jinlin Liu, Yang Fu, Bo Zhang, and Ying Mao. 2018. "Spatio-Temporal Epidemiology of Viral Hepatitis in China (2003–2015): Implications for Prevention and Control Policies" International Journal of Environmental Research and Public Health 15, no. 4: 661. https://doi.org/10.3390/ijerph15040661
APA StyleZhu, B., Liu, J., Fu, Y., Zhang, B., & Mao, Y. (2018). Spatio-Temporal Epidemiology of Viral Hepatitis in China (2003–2015): Implications for Prevention and Control Policies. International Journal of Environmental Research and Public Health, 15(4), 661. https://doi.org/10.3390/ijerph15040661