Factors Affecting the Retention of Indigenous Australians in the Health Workforce: A Systematic Review


Abstract
:1. Introduction
2. Methods
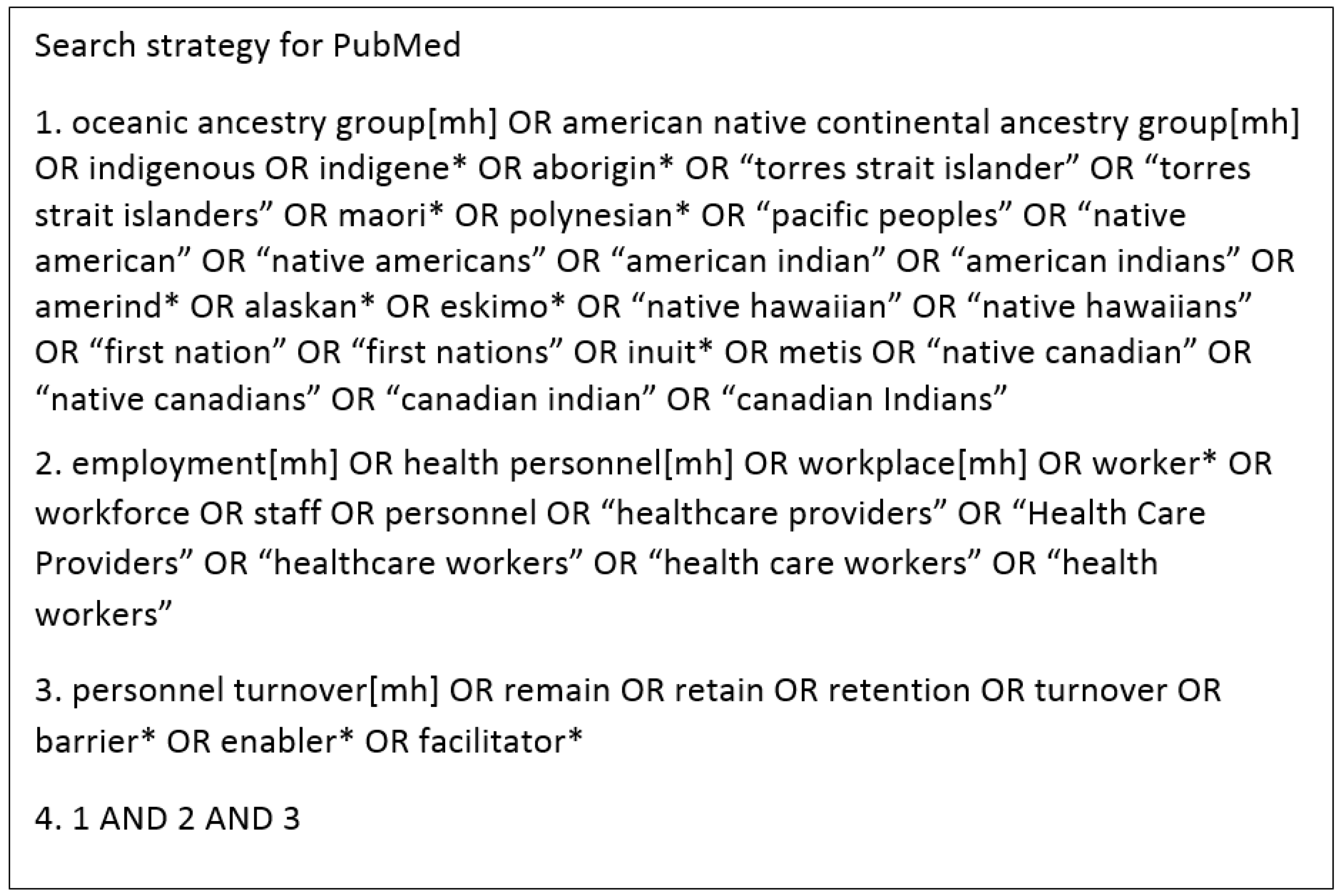
2.1. Search Strategy
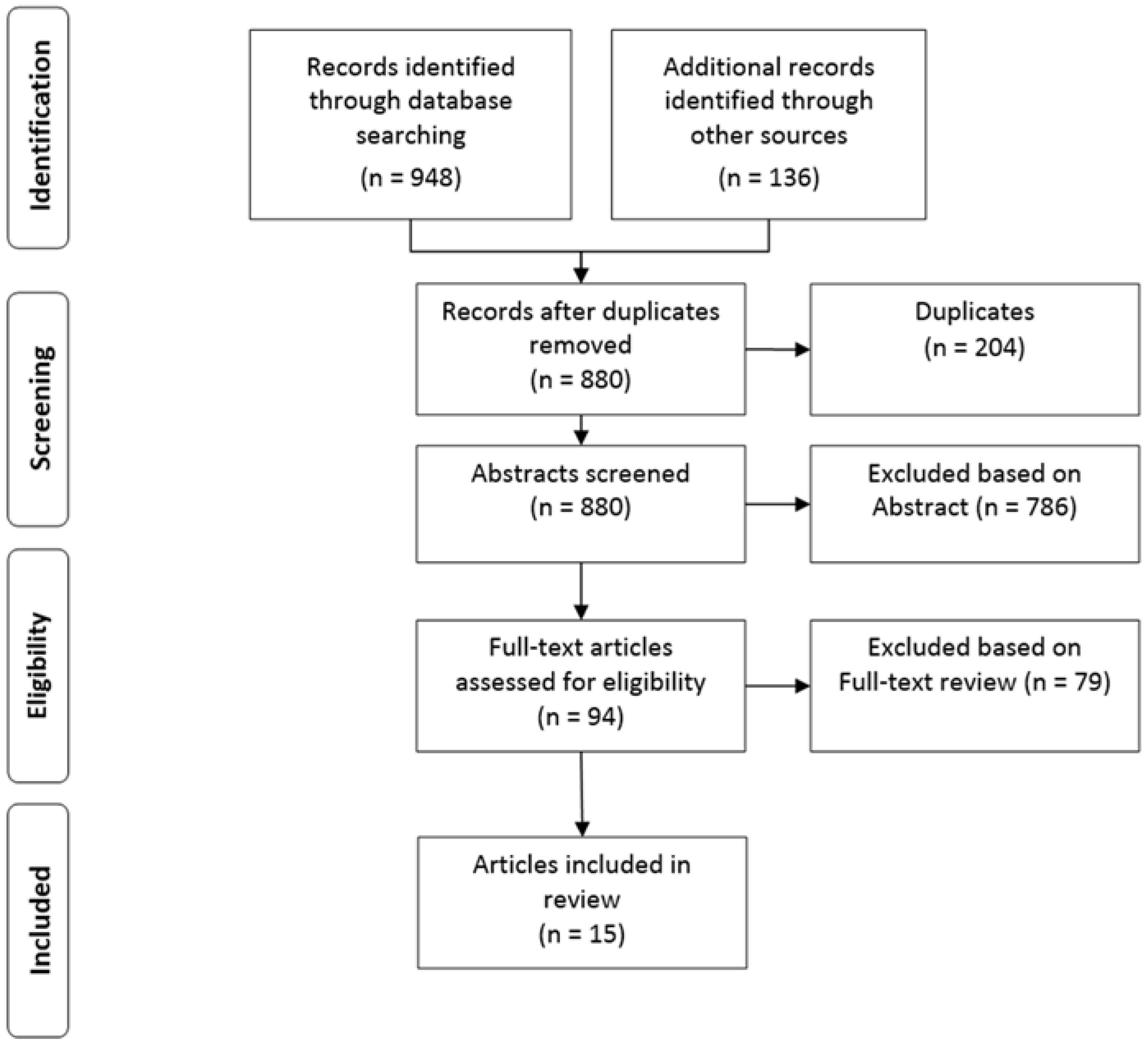
2.2. Screening Process: Inclusion and Exclusion Criteria
2.3. Quality Appraisal and Analysis
3. Results
3.1. Description of Studies
3.2. Enablers
3.2.1. Organisational-Level Factors
3.2.2. Individual Level Factors
3.3. Barriers
3.3.1. Structural-Level Factors
3.3.2. System-Level Factors
3.3.3. Organisational-Level Factors
3.3.4. Individual-Level Factors
3.4. Recommendations
3.4.1. System-Level Recommendations
3.4.2. Organisational-Level Recommendations
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Vos, T.; Barker, B.; Begg, S.; Stanley, L.; Lopez, A.D. Burden of disease and injury in aboriginal and torres strait islander peoples: The indigenous health gap. Int. J. Epidemiol. 2009, 38, 470–477. [Google Scholar] [CrossRef] [PubMed]
- McLennan, W.; Madden, R. The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples. Available online: http://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/4704.01997?OpenDocument (accessed on 5 December 2017).
- Department of the Prime Minister and Cabinet. Closing the Gap Prime Minister’s Report 2018. Available online: https://closingthegap.pmc.gov.au/sites/default/files/ctg-report-2018.pdf (accessed on 10 April 2018).
- Australian Department of Health and Ageing. National Aboriginal and Torres Strait Islander Health Plan 2013–2023; Australian Department of Health and Ageing: Canberra, Australia, 2013.
- Thompson, S.C.; Shahid, S.; Bessarab, D.; Durey, A.; Davidson, P.M. Not just bricks and mortar: Planning hospital cancer services for aboriginal people. BMC Res. Notes 2011, 4, 62. [Google Scholar] [CrossRef] [PubMed]
- Shahid, S.; Finn, L.D.; Thompson, S.C. Barriers to participation of aboriginal people in cancer care: Communication in the hospital setting. Med. J. Aust. 2009, 190, 574–579. [Google Scholar] [PubMed]
- Australian Medical Association. Healing Hands: Aboriginal and Torres Strait Islander Workforce Requirements. Available online: https://ama.com.au/article/2004-ama-indigenous-health-report-card-healing-hands-aboriginal-and-torres-strait-islander (accessed on 5 December 2017).
- Anderson, I.P.S.; Ewen, S.C.; Knoche, D.A. Indigenous medical workforce development: Current status and future directions. Med. J. Aust. 2009, 190, 580–581. [Google Scholar] [PubMed]
- Taylor, K.P.; Thompson, S.C.; Smith, J.S.; Dimer, L.; Ali, M.; Wood, M.M. Exploring the impact of an aboriginal health worker on hospitalised aboriginal experiences: Lessons from cardiology. Aust. Health Rev. 2009, 33, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Hayman, N. Strategies to improve indigenous access for urban and regional populations to health services. Heart Lung Circul. 2010, 19, 367–371. [Google Scholar] [CrossRef] [PubMed]
- McGrath, P.D.; Patton, M.A.; Ogilvie, K.F.; Rayner, R.D.; McGrath, Z.M.; Holewa, H.A. The case for aboriginal health workers in palliative care. Aust. Health Rev. 2007, 31, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Davidson, P.M.; MacIsaac, A.; Cameron, J.; Jeremy, R.; Mahar, L.; Anderson, I. Problems, solutions and actions: Addressing barriers in acute hospital care for indigenous Australians and New Zealanders. Heart Lung Circul. 2012, 21, 639–643. [Google Scholar] [CrossRef] [PubMed]
- Abbott, P.; Gordon, E.; Davison, J. Expanding roles of aboriginal health workers in the primary care setting: Seeking recognition. Contemp. Nurse 2008, 27, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. The Health and Welfare of Australia’s Aboriginal and Torres Strait Islander Peoples: 2015. Available online: https://www.aihw.gov.au/reports/indigenous-health-welfare/indigenous-health-welfare-2015/contents/indigenous-population-key-points (accessed on 10 April 2018).
- Australian Health Ministers’ Advisory Council. Aboriginal and Torres Strait Islander Health Performance Framework 2014 Report. Available online: https://www.pmc.gov.au/sites/default/files/publications/indigenous/Health-Performance-Framework-2014/home/tier-3-health-system-performance.html (accessed on 5 December 2017).
- Australian Institute of Health and Welfare. Nursing and Midwifery Workforce 2015. Available online: https://www.aihw.gov.au/reports/workforce/nursing-and-midwifery-workforce-2015/contents/who-are-nurses-and-midwives (accessed on 5 December 2017).
- Australian Institute of Health and Welfare. Medical Practitioners Workforce 2015. Available online: https://www.aihw.gov.au/reports/workforce/medical-practitioners-workforce-2015/contents/who-are-medical-practitioners (accessed on 5 December 2017).
- Australian Institute of Health and Welfare. Aboriginal and Torres Strait Islander Health Performance Framework. Available online: https://www.aihw.gov.au/reports/indigenous-health-welfare/health-performance-framework/contents/tier-3/aboriginal-and-torres-strait-islander-people-in-the-health-workforce-measure-3-12 (accessed on 10 April 2018).
- Health Workforce Australia. Growing Our Future: The Aboriginal and Torres Strait Islander Health Worker Project Final Report; Health Workforce Australia: Adelaide, Australia, 2011.
- Health Workforce Australia. Environmental Scan: Aboriginal and Torres Strait Islander Health Worker Project; Version 7.0: Final; Health Workforce Australia: Adelaide, Australia, 2011.
- Roche, A.; Tovell, A.; Weetra, D.; Freeman, T.; Bates, N.; Trifonoff, A.; Steenson, T. Stories of Resilience: Indigenous Alcohol and Other Drug Workers’ Wellbeing, Stress, and Burnout; Centre for Education and Training on Addiction (NCETA), Flinders University: Adelaide, Australia, 2010. [Google Scholar]
- Department of the Prime Minister and Cabinet. Closing the Gap Prime Minister’s Report 2017. Available online: https://www.pmc.gov.au/sites/default/files/publications/ctg-report-2017.pdf (accessed on 5 December 2017).
- Russell, D.J.; Wakerman, J.; Humphreys, J.S. What is a reasonable length of employment for health workers in Australian rural and remote primary healthcare services? Aust. Health Rev. 2013, 37, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.J.; Zhao, Y.; Guthridge, S.; Ramjan, M.; Jones, M.P.; Humphreys, J.S.; Wakerman, J. Patterns of resident health workforce turnover and retention in remote communities of the Northern Territory of Australia, 2013–2015. Hum. Resour. Health 2017, 15, 52. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, J.; Wakerman, J.; Pashen, D.; Buykx, P. Retention Strategies & Incentives for Health Workers in Rural & Remote Areas: What Works? Available online: http://files.aphcri.anu.edu.au/research/international_retention_strategies_research_pdf_10642.pdf (accessed on 15 February 2018).
- Shields, M.A.; Ward, M. Improving nurse retention in the national health service in England: The impact of job satisfaction on intentions to quit. J Health Econ. 2001, 20, 677–701. [Google Scholar] [CrossRef]
- Ratima, M.; Brown, R.; Garrett, N.; Wikaire, E.; Ngawati, R.; Aspin, C.; Potaka, U. Rauringa Raupa: Recruitment and Retention of Maori in the Health and Disability Workforce. Available online: https://www.health.govt.nz/system/files/documents/publications/maori_health_workforce_110708low_with_cover.pdf (accessed on 4 August 2017).
- Katz, J.R.; O’Neal, G.; Strickland, C.J.; Doutrich, D. Retention of native American nurses working in their communities. J. Transcult. Nurs. 2010, 21, 393–401. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Robert, E.; Cargo, M.; Bartlett, G.; O’Cathain, A.; Griffiths, F.; Boardman, F.; Gagnon, M.P.; Rousseau, M.C. Proposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies Reviews. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com (accessed on 13 February 2018).
- Pace, R.; Pluye, P.; Bartlett, G.; Macaulay, A.C.; Salsberg, J.; Jagosh, J.; Seller, R. Testing the reliability and efficiency of the pilot mixed methods appraisal tool (mmat) for systematic mixed studies review. Int. J. Nurs. Stud. 2012, 49, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Gagnon, M.-P.; Griffiths, F.; Johnson-Lafleur, J. A scoring system for appraising mixed methods research, and concomitantly appraising qualitative, quantitative and mixed methods primary studies in mixed studies reviews. Int. J. Nurs. Stud. 2009, 46, 529–546. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Department of Family Medicine, McGill University, Montreal, QC, Canada. Personal communication, 2018.
- Browne, J.; Thorpe, S.; Tunny, N.; Adams, K.; Palermo, C. A qualitative evaluation of a mentoring program for aboriginal health workers and allied health professionals. Aust. N. Z. J. Public Health 2013, 37, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.; Tsourtos, G.; Lawn, S. The barriers and facilitators that indigenous health workers experience in their workplace and communities in providing self-management support: A multiple case study. BMC Health Serv. Res. 2017, 17, 319. [Google Scholar] [CrossRef] [PubMed]
- Cosgrave, C.; Maple, M.; Hussain, R. Factors affecting job satisfaction of aboriginal mental health workers working in community mental health in rural and remote New South Wales. Aust. Health Rev. 2017, 41, 707–711. [Google Scholar] [CrossRef] [PubMed]
- Ella, S.; Lee, K.K.; Childs, S.; Conigrave, K.M. Who are the New South Wales aboriginal drug and alcohol workforce? A first description. Drug Alcohol Rev. 2015, 34, 312–322. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Robinson, G. The aboriginal mental health worker program: The challenge of supporting aboriginal involvement in mental health care in the remote community context. Aust. e-J. Adv. Ment. Health 2007, 6, 1–11. [Google Scholar] [CrossRef]
- King, L.; King, M.; Willis, E.; Munt, R.; Semmens, F. The experiences of remote and rural aboriginal health workers and registered nurses who undertook a postgraduate diabetes course to improve the health of indigenous Australians. Contemp. Nurse 2012, 42, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.M.; Duraisingam, V.; Trifonoff, A.; Tovell, A. The health and well-being of indigenous drug and alcohol workers: Results from a national Australian survey. J. Subst. Abuse Treat. 2013, 44, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Roche, A.M.; Duraisingam, V.; Trifonoff, A.; Battams, S.; Freeman, T.; Tovell, A.; Weetra, D.; Bates, N. Sharing stories: Indigenous alcohol and other drug workers’ well-being, stress and burnout. Drug Alcohol Rev. 2013, 32, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Watson, K.; Young, J.; Barnes, M. What constitutes ‘support’ for the role of the aboriginal and torres strait islander child health workforce? Aust. Health Rev. 2013, 37, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Robinson, G.; Harris, A. Aboriginal Mental Health Worker Program: Final Evaluation Report. Available online: http://nceta.flinders.edu.au/files/6813/5787/2431/Abor_mh_worker_program_final.pdf (accessed on 6 February 2018).
- Duraisingam, V.; Roche, A.M.; Trifonoff, A.; Tovell, A. Indigenous aod Workers’ Wellbeing, Stress and Burnout: Findings from an Online Survey; National Centre for Education and Training on Addiction (NCETA), Flinders University: Adelaide, Australia, 2010. [Google Scholar]
- Aboriginal and Torres Strait Islander Health Workforce Working Group. National Aboriginal and Torres Strait Islander Health Workforce Strategic Framework: 2016–2023; Department of Health, Australia: Canberra, Australia, 2017.
- Congress of Aboriginal and Torres Strait Islander Nurses and Midwives. Catsinam Mentoring Program Review Report. Available online: http://catsinam.org.au/static/uploads/files/mentoring-program-review-report-final-may-16-2014-wfvpiqvtkbhj.pdf (accessed on 3 August 2017).
- Health Workforce Australia. Leadership for the Sustainability of the Health System: Part 4: Aboriginal and Torres Strait Islander Health Leadership, a Key Informant Interview Report. Available online: http://www.healthinfonet.ecu.edu.au/key-resources/bibliography/?lid=27685 (accessed on 4 August 2017).
- Health Workforce Australia. Aboriginal & Torres Strait Islander Health Worker Project Interim Report. Available online: https://www.natsihwa.org.au/sites/default/files/atsihw-project-interim-report-20111017.pdf (accessed on 4 August 2017).
- Mercer, C.A. The Experiences of Aboriginal Health Workers and Non-Aboriginal Health Professionals Working Collaboratively in the Delivery of Health Care to Aboriginal Australians: A Systematic Review of Qualitative Evidence. Available online: https://digital.library.adelaide.edu.au/dspace/bitstream/2440/100425/2/02whole.pdf (accessed on 17 January 2018).
- Biddle, N.; Lahn, J.; Australian National University Centre for Aboriginal Economic Policy Research. Understanding Aboriginal and Torres Strait Islander Employee Decisions to Exit the Australian Public Service. Available online: http://caepr.cass.anu.edu.au/sites/default/files/docs/CAEPR-WP110_2016pdf_0.pdf (accessed on 16 January 2018).
- Day, A.; Giles, G.; Marshall, B.; Sanderson, V. The recruitment and retention of indigenous criminal justice agency staff in an Australian state. Int. J. Offender Ther. Comp. Criminol. 2004, 48, 347–359. [Google Scholar] [CrossRef] [PubMed]
- Duffield, C.M.; Roche, M.A.; Blay, N.; Stasa, H. Nursing unit managers, staff retention and the work environment. J. Clin. Nurs. 2011, 20, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Hayes, L.J.; O’Brien-Pallas, L.; Duffield, C.; Shamian, J.; Buchan, J.; Hughes, F.; Spence Laschinger, H.K.; North, N.; Stone, P.W. Nurse turnover: A literature review. Int. J. Nurs. Stud. 2006, 43, 237–263. [Google Scholar] [CrossRef] [PubMed]
- Thackrah, R.D.; Thompson, S.C. Refining the concept of cultural competence: Building on decades of progress. Med. J. Aust. 2013, 199, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Durey, A.; Thompson, S.C. Reducing the health disparities of indigenous Australians: Time to change focus. BMC Health Serv. Res. 2012, 12, 151. [Google Scholar] [CrossRef] [PubMed]
- Rickard, G.; Lenthall, S.; Dollard, M.; Opie, T.; Knight, S.; Dunn, S.; Wakerman, J.; MacLeod, M.; Seiler, J.; Brewster-Webb, D. Organisational intervention to reduce occupational stress and turnover in hospital nurses in the northern territory, Australia. Collegian 2012, 19, 211–221. [Google Scholar] [CrossRef] [PubMed]
- National Aboriginal and Torres Strait Islander Health Worker Association. National Framework for Determining Scope of Practice for the Aboriginal and/or Torres Strait Islander Health Worker/Health Practitioner Workforce; National Aboriginal and Torres Strait Islander Health Worker Association: Canberra, Australia, 2016.
- Roche, A.; Pidd, K. National Centre for Education and Training on Addiction (Australia). Setting the Scene: Alcohol and Other Drugs Workforce Development Issues and Imperatives. Available online: http://nceta.flinders.edu.au/files/4912/7200/2031/EN422%20Roche%20%20Pidd%202010.pdf (accessed on 16 January 2018).
- Dwyer, J.M.; Lavoie, J.; O’Donnell, K.; Marlina, U.; Sullivan, P. Contracting for indigenous health care: Towards mutual accountability. Aust. J. Public Adm. 2011, 70, 34–46. [Google Scholar] [CrossRef]
- Gray, D.; Stearne, A.; Wilson, M.; Doyle, M. Indigenous-Specific Alcohol and Other Drug Interventions: Continuities, Changes and Areas of Greatest Need. Available online: http://www.healthinfonet.ecu.edu.au/uploads/resources/18131_18131.pdf (accessed on 17 January 2018).
- Perkins, D.; Larsen, K.; Lyle, D.; Burns, P. Securing and retaining a mental health workforce in far western New South Wales. Aust. J. Rural Health 2007, 15, 94–98. [Google Scholar] [CrossRef] [PubMed]
- O’Toole, K.; Schoo, A.; Hernan, A. Why did they leave and what can they tell us? Allied health professionals leaving rural settings. Aust. Health Rev. 2010, 34, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Buykx, P.; Humphreys, J.; Wakerman, J.; Pashen, D. Systematic review of effective retention incentives for health workers in rural and remote areas: Towards evidence-based policy. Aust. J. Rural Health 2010, 18, 102–109. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author (Year) Location | Methods | Study Population and Response Rate | Focus | Relevant Findings | MMAT Score |
|---|---|---|---|---|---|
| Browne et al. (2013) [34] Victoria Rurality not Specified | Qualitative Interviews | 30 mentoring program participants (17 IHWs (Indigenous Health Workers), 13 AHPs (allied health professionals)). Response rate: 86% of mentoring program participants. | Evaluate peer mentoring between IHWs and non-Indigenous allied health professionals. | Peer mentoring between Indigenous and non-Indigenous health workforce found to facilitate two-way learning, meet learning needs, and promote practice improvement. Helps address the challenging nature of the work of IHWs, which currently results in high turnover. | 75% |
| Conway et al. (2017) [35] Australia Rural and Urban | Qualitative Interviews | 5 IHWs (from five different states) Case study methodology. Mass recruitment via e-mail to 201 IHWs, followed by purposive sampling selected by key informants, due to low response rate. | Barriers and facilitators for IHWs in the workplace in providing self-management support. | Causes of stress for IHWs included: time pressures, work/life imbalance and cultural expectations, lack of mentorship, high staff turnover and culturally insensitive non-Indigenous colleagues. Stress contributed to burn out and attrition, and was more prevalent in rural and remote environments. IHWs have limited support and are excluded from decision-making by other staff, also leading to burnout and attrition. Adequate staffing and support structures are required to reverse these barriers. | 75% |
| Cosgrave et al. (2017) [36] New South Wales Rural and Remote | Qualitative Interviews | 5 IMHWs (Indigenous Mental Health Workers). Criterion sampling: participants had to meet qualifications conditions to work as CMH (community mental health) professionals and had to be currently/recently working in a rural/remote local health district in NSW. Participants recruited through group presentations. Response rate: unspecified. | Factors affecting job satisfaction and retention of IMHWs (Indigenous mental health workers). | Three main factors affecting job satisfaction were: difficulties being accepted into the team and workplace caused by lack of understanding of role, challenges with setting culturally-appropriate personal and professional boundaries and perceived salary inequalities and low salary. Inadequate remuneration was linked to turnover intention. Lack of career opportunities a motivator for leaving the health sector. | 50% |
| Ella et al. (2015) [37] New South Wales Metro 22%, Regional 59% Rural 14%, Remote 6% | Quantitative Survey | 51 Indigenous AOD (alcohol and other drug) workers. Response rate: 85% of study population. No workers declined to participate. No contact data was available for the nine workers not identified for interview. | Description of Indigenous AOD workers employed in NSW and strategies to improve retention. | Improvement of retention among Indigenous AOD workers requires implementation of professional development opportunities, improved pay and job security, greater role clarity, access to formal supervision and clinical and cultural mentoring. | 100% |
| Harris & Robinson (2007) [38] Northern Territory Remote | Mixed methods Audit, participant observation and interviews | Audit: 30 client records across five health centres. Interviews: 52 personnel and stakeholders involved in the IMHW program (all employed IMHWs, mental health clients, non-Indigenous health professionals, key stakeholders). Response rate: unspecified. Purposive sampling. | Evaluate the “Aboriginal Mental Health Worker Program” in the NT. | Role ambiguity and unclear cultural legitimacy of IMHW practice causes stress and can lead to burnout. Geographical isolation, limited mentoring, lack of support and difficulty accessing training were linked to attrition. Greater role clarity, culturally informed mental health practices and local managerial support are essential for IMHWs to be effective members of the primary health team. Support at the supra-local level with departmental strategies, resources and partnerships are required for long term improvements and systematic change. | 75% 1 |
| King et al. (2012) [39] New South Wales Rural and Remote | Qualitative Interviews | 17 participants, educators and managers regarding the diabetes course. (5 AHW (Aboriginal Health Worker) DEs (Diabetes Educators), 1 AHW student DE, 8 RN (registered nurse) DNEs (Diabetes Nurse Educators), 1 RN student DNE, 2 Nurse Mangers. Response rate: 86% of IHWs who attended the course, unclear for other participants. Purposive sampling. | Experiences of IHWs and RNs during and after completion of specialist diabetes training, and managerial strategies to support workers during and after training. | Completing specialist training was empowering, encouraged retention, improved service delivery for clients and was a good investment for the health service. Managers can support completion of training by allocating work time for study, providing formal support, and by making changes to role, duties and/or remuneration to reflect additional qualifications. | 50% |
| Roche et al. (2013) [40] Australia Metropolitan Rural and Remote | Quantitative Survey | 294 AOD workers (184 Indigenous, 108 non-Indigenous, 2 unknown). Response rate: unknown. Convenience sampling. | Factors that contribute to the stress levels, well-being and turnover intention of Indigenous AOD workers. | Emotional exhaustion is a key predictor of turnover intention and is caused by work/family life imbalance and lack of co-worker support. Ensuring adequate and equitable salaries, providing career development opportunities and reducing stress levels may reduce turnover intention. | 75% 2 |
| Roche et al. (2013) [41] Australia Metropolitan Rural and Remote | Qualitative Focus Groups | 121 AOD Workers (70 Indigenous, 20 non-Indigenous, 31 unspecified). Response rate: unspecified. Purposive, maximum-variation sampling. | Indigenous AOD workers experiences and perspectives on well-being, stress and burnout and strategies to improve well-being. | Heavy workloads, lack of career opportunities, poor job security and low salaries contribute to turnover intention among IAOD workers. Other sources of workplace stress included: proximity to and expectations of communities and experiences of racism and discrimination. Workforce development strategies included: adequate remuneration, supervision and mentorship, cultural sensitivity training for non-Indigenous workers, and training in boundary setting. | 75% 3 |
| Taylor et al. (2009) [9] Western Australia Metropolitan | Qualitative Interviews | 2 IHWs, 12 non-Indigenous health professionals, 12 Indigenous patients. Response rate: Unspecified. Purposive sampling. | Impact of and challenges faced by an IHW working in cardiac rehabilitation in a tertiary hospital. | Job dissatisfaction was caused by limitations in the IHW training for hospital settings, role ambiguity and poor role definition, poor remuneration and limited career pathways. Recommendations to improve the IHW role and retention in a hospital setting included: providing additional training in the hospital setting, supporting collaborations with other Indigenous staff, documenting clear role responsibilities, and ensuring appropriate remuneration. | 50% |
| Watson et al. (2013) [42] Queensland | Qualitative Focus Groups | 47 CHWs (child health workers) (33 Indigenous, 11 non-Indigenous, 3 mixed cultural background). Response rate: 96% of program participants. | Areas of support that are important to Indigenous and non-Indigenous CHWs working within Indigenous communities. | ICHWs (Indigenous child health workers) require support in relation to the cultural safety of the workplace, educational opportunities, collaboration with colleagues and peers, and professional mentorship, improvement of which can increase job satisfaction. | 50% |
| Author (Year) | Methods | Study Population and Response Rate | Focus | Relevant Findings | MMAT Score |
|---|---|---|---|---|---|
| Aboriginal and Torres Strait Islander Health Workforce Working Group (2017) [45] Australia | Qualitative Consensus | None. Working party consensus with input from Indigenous health stakeholders. | Framework to guide IHW workforce policy and planning. | Six strategies (with suggested actions) for a stronger workforce: improve recruitment and retention, improve skills and capacity, provide culturally-safe workplaces, increase number of health students, improve completion rates for health students, improve health workforce planning and policy. | N/A |
| Congress of Aboriginal and Torres Strait Islander Nurses and Midwives (2014) [46] Australia | Mixed methods Survey, yarning circles and forums | 67 participants (57 CATSINaM Members (nurses or student nurses, approx. 28% of total membership) and 11 non-Members). Yarning Circles: unspecified. Forums: unspecified. | Proposed solutions for a revised mentoring program for Indigenous nurses. | Mentoring was identified as a priority strategy to improve retention among Indigenous nurses through the provision of cultural support and preceptoring relationships. | 25% |
| Health Workforce Australia (2014) [47] Australia | Qualitative Interviews | 13 Indigenous health leaders (3 CEOs, 3 middle management, 2 clinical management, 5 academics; 9 participants also current or former clinicians). Response rate: 65% of identified key informants. | Challenges faced by Indigenous health leaders and recommendations to support and develop current and future leaders. | Shortage of Indigenous health leaders causes high workloads and stress. Covert and systemic racism in the health system contributes to stress. Need for cultural competency for all health leaders. Need to improve overall legitimacy, credibility and support for Indigenous health workforce. Need for succession planning and mentoring to develop future Indigenous health leaders. | 75% |
| Health Workforce Australia (2011) [48] Australia | Mixed methods Interviews, survey and focus groups | 923 health professionals. Survey: 351 IHWs (response rate of 22–35%), 100 managers. Focus Groups: 264 IHWs, 100 managers, 25 health professionals. Interviews: 138 key informants. | How the IHW workforce can be strengthened. | Barriers that affect retention of IHWs include: low salary and salary inequities, lack of job security, burn-out, lack of respect and support, and limited career progression opportunities. Other challenges for IHWs include limited professional development opportunities, racism and lack of cultural security in the workplace and inadequate supervision. Enablers to retention: high job satisfaction, strong ties to the community and wanting to make a difference for the community. Effective retention strategies included: supportive management structure, respect from colleagues, Indigenous leadership in the health workforce, culturally safe workplace, flexible working conditions, and access to professional development. | 75% |
| Health Workforce Australia (2011) [19] Australia | Mixed methods Interviews, survey and focus groups | 1052 health professionals. Survey: 351 IHWs (response rate of 22–35%), 100 managers. Focus Groups: 264 IHWs, 100 managers, 25 health professionals. Interviews: 212 key informants (138 individuals in Phase 1 and 74 individuals in Phase 2). | Policies and strategies that aim to strengthen and sustain the IHW workforce. | Makes 27 recommendations to support and strengthen the IHW workforce including recommendations to improve retention (such as addressing salary inequities). Includes the HWA Health Service Toolkit (Appendix F) which provides actions that health services can undertake to support IHWs and address retention challenges. | 75% |
| Study Criterion | Structural | System | Organisational | Individual |
|---|---|---|---|---|
| Enablers | None | None | Co-worker support and peer mentorship (8) [19,34,38,39,40,42,46,48]. Culturally safe workplace (4) [41,42,47,48]. Access to clinical and cultural supervision (4) [37,40,42,48]. Professional development opportunities (4) [39,40,42,48]. Job security and adequate remuneration (2) [37,40]. | Making a difference for Indigenous health (5) [39,41,42,47,48]. |
| Barriers | Racism (5) [35,40,41,47,48] | Limited organisational funding and inadequate remuneration (8) [9,36,37,40,41,42,47,48]. Limited career pathways (2) [36,48]. | Heavy workloads and demands (10) [9,35,36,37,38,40,41,42,47,48]. Lack of support from management and lack of mentoring (8) [34,35,37,38,41,46,47,48]. Lack of professional development opportunities (5) [9,36,37,38,41]. | Proximity to community (8) [35,36,37,40,41,42,47,48]. |
| Recommendations | None | Recognition of the Indigenous health professional role (8) [9,19,37,38,40,41,45,47]. Increased remuneration and salary parity (7) [9,19,37,39,40,41,48]. Work with educational systems to improve curriculum structure and facilitate career progression (4) [19,36,39,45]. | Implement mentoring, clinical supervision and support systems (10) [9,19,34,35,37,39,41,42,45,46]. Embed cultural respect in the workplace (7) [19,34,36,37,41,45,47]. Professional development opportunities (7) [19,39,40,41,42,45,47]. Flexible working arrangements (3) [19,40,41]. | None. |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, G.C.; Taylor, E.V.; Haigh, M.M.; Thompson, S.C. Factors Affecting the Retention of Indigenous Australians in the Health Workforce: A Systematic Review. Int. J. Environ. Res. Public Health 2018, 15, 914. https://doi.org/10.3390/ijerph15050914
Lai GC, Taylor EV, Haigh MM, Thompson SC. Factors Affecting the Retention of Indigenous Australians in the Health Workforce: A Systematic Review. International Journal of Environmental Research and Public Health. 2018; 15(5):914. https://doi.org/10.3390/ijerph15050914
Chicago/Turabian StyleLai, Genevieve C., Emma V. Taylor, Margaret M. Haigh, and Sandra C. Thompson. 2018. "Factors Affecting the Retention of Indigenous Australians in the Health Workforce: A Systematic Review" International Journal of Environmental Research and Public Health 15, no. 5: 914. https://doi.org/10.3390/ijerph15050914
APA StyleLai, G. C., Taylor, E. V., Haigh, M. M., & Thompson, S. C. (2018). Factors Affecting the Retention of Indigenous Australians in the Health Workforce: A Systematic Review. International Journal of Environmental Research and Public Health, 15(5), 914. https://doi.org/10.3390/ijerph15050914