A Cross-Disciplinary Successful Aging Intervention and Evaluation: Comparison of Person-to-Person and Digital-Assisted Approaches

 ,
, 
Abstract
:1. Introduction
1.1. Intervention on Successful Aging
1.2. Intervention Approach
1.3. Aims
2. Materials and Methods
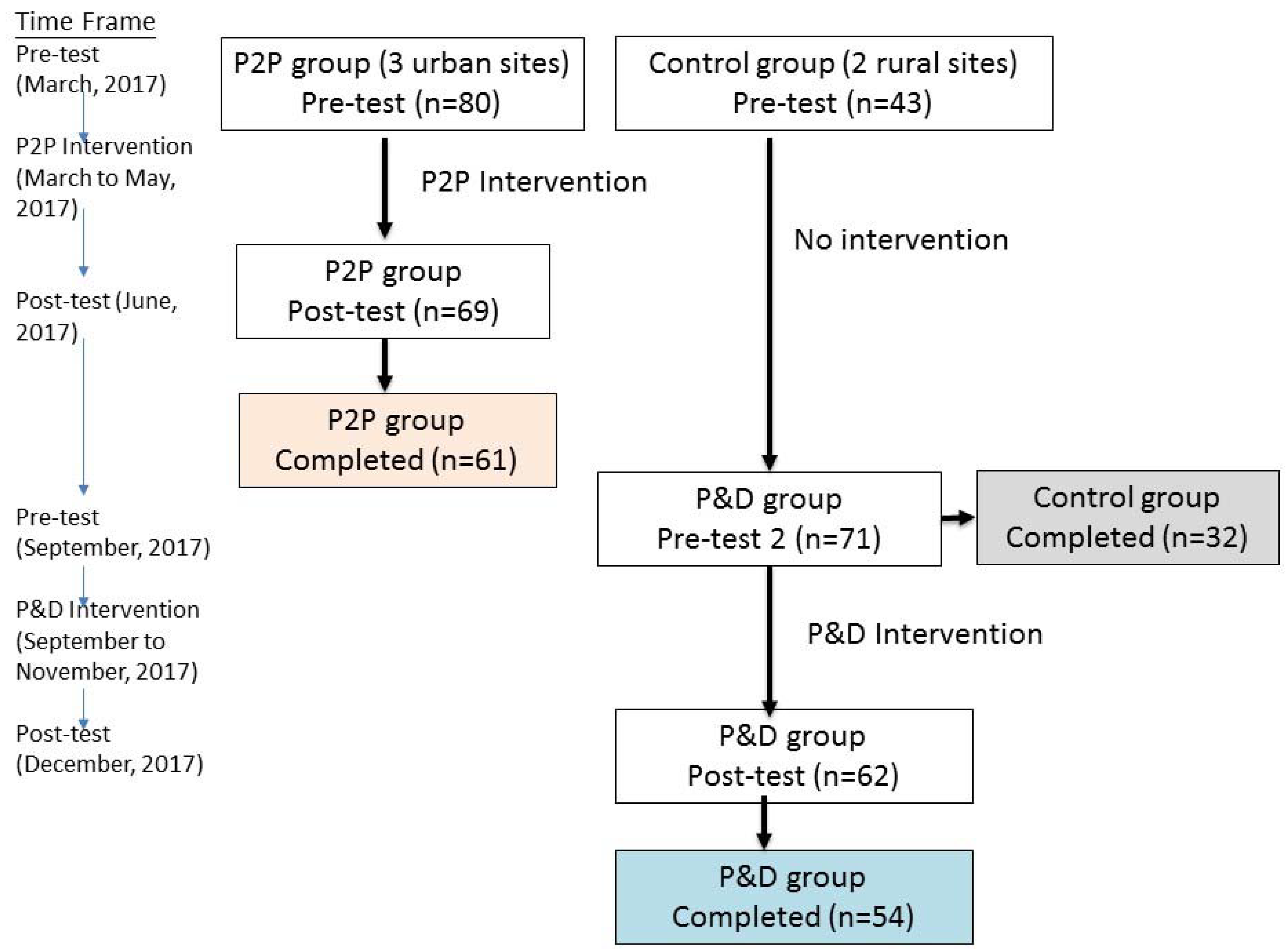
2.1. Setting and Participants
2.2. Intervention Program
- (1)
- Concept and preparation for successful aging: The lecture introduced the idea of successful aging, risk and protective factors to successful aging, strategies for successful aging, the importance of preparing for old age in life, and the framework of the whole program. The course was given by an expert in gerontology.
- (2)
- Physical activity: The unit introduced content about common physical activities and a fitness examination and then provided a demonstration of easy physical activity exercises that can be performed at home. An elastic band was provided for each participant to use in the physical activity exercise. The unit was given by a physical therapist, and trained graduate students helped to demonstrate and assist the participants with the exercise.
- (3)
- Nutrition and diet for older people: The educational content included reference material about daily diet, six categories of food and nutrition, portion size and calories, appropriate nutrition suggestions for older adults, the DASH diet (dietary approaches to stop hypertension, a diet which is rich in fruits, vegetables, whole grains, and low-fat dairy foods; includes meat, fish, poultry, nuts, and beans; and is limited in sugar-sweetened foods and beverages, red meat, and added fats; it is used for control hypertension and promote a well-balanced diet), etc. The lecture was given by an attending physician.
- (4)
- Chronic disease prevention and management: This unit included the management of common chronic diseases for older adults (hypertension, high blood cholesterol, heart disease, diabetes, arthritis, osteoporosis, insomnia, etc.), prevention strategies, and medication usage knowledge. The lecture was given by an attending physician.
- (5)
- Emotional health and coping with stress: The unit designed with the background of cognitive behavior therapy introduced self-awareness of emotions and distress, as well as practice of coping skills for a more balanced psychological well-being. The lecture was given by an expert and practitioner in the field of mental health.
- (6)
- Cognitive function training: Cognitive function training was provided, including activities to draw attention and concentration, retain short-term memory, execute daily activities of daily living, and perform executive functioning tasks. A device-assisted response training was given for the P2P group, and an online cognitive game was implemented as the exercise for the P&D group. The necessary training devices and tablets were provided in the training weeks.
- (7)
- Family relationship: The content focused on emotional awareness, forgiveness and conflict resolution in family relationships, and expressing appreciation and affection. The unit included a lecture and exercise, and a tablet game was also provided as the demonstration. The unit was led by two experts in family relationships.
- (8)
- Financial security: The lecture focused on the basic ideas of self-protection concepts in finance, knowledge of law related to inheritance, legal representation for those who are disabled, and property trust. The lecture was given by a lawyer with expertise in social protection for older adults.
- (9)
- Internet use: The lecture and practice focused on how to use a tablet to go online and introduced several useful applications for older adults, such as bus schedules, clinic registrations, and searching for information about songs on YouTube or health information on a recommended website. The tablets were provided for all the participants for the duration of the intervention. For the P&D group, the Internet use course was allowed additional weeks for practice. The lecture was given by a graduate student, and 4–10 students (according to the number of participants and the course content) and CCC volunteers assisted the older participants in learning to use the tablets every week.
2.3. Ethical Consideration
2.4. Data Collection and Measurements of Effective Evaluation
- (1)
- Demographics and background: Age, sex, education, marital status, living arrangement (living alone or with others), household income, and rated relative income.
- (2)
- Physical health: Self-rated health was measured as poor to excellent (score 1–5). Chronic disease numbers (accumulative numbers of the following chronic diseases: strokes (ever), hypertension, heart disease, diabetes, arthritis, spinal spurs, kidney or urinary tract diseases, stomach ulcers, liver- or gall bladder-related diseases, pulmonary or respiratory system diseases, cancer, cataracts or glaucoma, and reproductive system diseases). Nutritional risk was screened by the Mini Nutrition Assessment (MNA) [62] and coded as normal (score ≥ 12) or at risk of malnutrition (score ≤ 11). Physical function, measured by instrumental activities of daily living (IADLs) and the Nagi scale and scored 0–27 [63], was collected only at baseline to serve as a control. Fitness items for older people were also examined as an outcome but were not included in this article because some participants could not perform the fitness tests, and the sample size was small.
- (3)
- Mental health: Depressive symptoms were measured by the CES-D 10-item scale [64], scored 0–30. Cognitive function was measured by MoCA (Montreal Cognitive Assessment) [65], a more sensitive cognitive assessment tool; the total score ranged from 0 to 30 by the adjustment of education. A score of 25 or lower indicated the risk of mild cognitive impairment. Adaptation strategies to old age were conceptualized from the Baltes and Baltes’ successful aging model [66] and revised by Donnellan et al. (2012) [67]. The six items included the strategies of selection, optimization, and compensation. Each item was scored from 1 to 3 as disagree, no opinion, or agree; each type of strategy was scored from 2–6. Stress coping strategies were measured with a brief COPE scale [68]. The original scale included 18 items and was then reduced to 11 items in later tests. The stress coping strategies were analyzed by factor analysis, and three types of coping strategies were then extracted. Finally, the original item scores were summed as the strategy type score: action and positive thinking (score 4–16), emotion-focused coping (score 4–16), and negative coping (score 2–8).
- (4)
- Lifestyle and health literacy: Lifestyle included regular exercise (exercise three times or more per week), sedentary lifestyle hours per day, etc. In addition, 14 items for measuring diet behaviors and healthy literacy were asked [13], such as questions about choices for a balanced diet; intake of vegetables, fruit, milk and related products, drinks containing sugar, and foods high in cholesterol; noticing expiration dates; reminders from family and friends about diet nutrition, etc. Each item was scored from 1 to 3, and the total score ranged from 14 to 42; a higher score indicated a better diet style.
- (5)
- Social support: (a) Social support included questions about emotional support and instrumental support from family and friends, respectively; each item was scored from 4 to 12; (b) conflicts with family members (including spouse, children, or other family members) (coded as yes/no).
- (6)
- Financial security knowledge and preparation: The participants were asked if they had made financial preparations for life in old age (yes/no). They were also asked whether they knew about the laws regarding inheritance, guardian, and property trust (yes/no).
- (7)
- Internet use: The participants were asked whether they use the Internet and at what frequency (at least once every week) as well as whether they were able to search for health information online (yes/no). In the post-test, participants were also queried about reasons to use or not use the internet.
- (8)
- Life satisfaction: Life satisfaction was scored from 1 to 5, indicating very unsatisfactory to very satisfactory
2.5. Analysis
3. Results
3.1. Sample Description
3.2. Comparison within Groups
3.3. GEE Analysis
4. Discussion
4.1. Summary
4.2. Outcome Evaluation
4.2.1. Physical Health and Health Behaviors
4.2.2. Mental Health
4.2.3. Social Outcome
4.3. Process Evaluation and Intervention Approach
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Rowe, J.W.; Kahn, R.L. The structure of successful aging. In Successful Aging; Rowe, J.W., Kahn, R.L., Eds.; Dell Publishing: New York, NY, USA, 1997; pp. 36–52. ISBN 978-0440508632. [Google Scholar]
- Adams, G.A.; Rau, B.L. Putting off tomorrow to do what you want today: Planning for retirement. Am. Psychol. 2011, 66, 180–192. [Google Scholar] [CrossRef] [PubMed]
- Depp, C.A.; Jeste, D.V. Definitions and predictors of successful aging: A comprehensive review of larger quantitative studies. Am. J. Geriatr. Psychiatr. 2006, 14, 6–20. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, E.A.; Hinterlong, J.E. Changes in social participation and volunteer activity among recently widowed older adults. Gerontologist 2010, 50, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Elwood, P.; Galante, J.; Pickering, J.; Palmer, S.; Bayer, A.; Ben-Shlomo, Y.; Longley, M.; Gallacher, J. Healthy lifestyles reduce the incidence of chronic diseases and dementia: Evidence from the Caerphilly cohort study. PLoS ONE 2013, 8, e81877. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.K.; Lawrence, S.B. Retirement savings of the hip generation: A study of retirement preparation among individuals in their fifties. Southwest. Econ. Rev. 2007, 34, 115–130. [Google Scholar]
- Hsu, H.C.; Chang, W.C. Reducing the risks of morbidity, disability, and mortality using successful aging strategies. J. Am. Geriatr. Soc. 2015, 63, 2426–2428. [Google Scholar] [CrossRef] [PubMed]
- Lennartsson, C.; Silverstein, M. Does engagement with life enhance survival of elderly people in Sweden? The role of social and leisure activities. J. Gerontol. B Psychol. Sci. Soc. Sci. 2001, 56, S335–S342. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, D.; Vagenas, D.; Pachana, N.A.; Begum, N.; Dobson, A. Gender differences in social network size and satisfaction in adults in their 70s. J. Health Psychol. 2010, 15, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.; Kennedy, P. A longitudinal analysis of emotional impact, coping strategies and post-traumatic psychological growth following spinal cord injury: A 10-year review. Br. J. Health. Psychol. 2007, 12, 347–362. [Google Scholar] [CrossRef] [PubMed]
- Pruchno, R.A.; Wilson-Genderson, M.; Rose, M.; Carwright, F. Successful aging: Early influences and contemporary characteristics. Gerontologist 2010, 50, 821–833. [Google Scholar] [CrossRef] [PubMed]
- Estebasari, F.; Taghdisi, M.H.; Foroushani, A.R.; Ardebili, H.E.; Shojaeizadeh, D. An educational proram based on the successful aging approach on helaht-promoting behaviors in the elderly: A clinical trial study. Iran. Red. Crescent Med. J. 2014, 16, e16314. [Google Scholar] [CrossRef]
- Hsu, H.C.; Chuang, S.H.; Hsu, S.W.; Tung, H.J.; Chang, S.C.; Lee, M.M.; Wang, J.Y.; Kuo, L.T.; Tseng, F.Y.; Po, A.T. Evaluation of a successful aging promotion intervention program for middle-aged adults in Taiwan. Glob. Health Promot. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 year multimodmain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): A randomized controlled trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef]
- Rowe, J.W.; Kahn, R.L. Successful aging 2.0: Conceptual expansions for the 21st century. J. Gerontol. B Psychol. Sci. Soc. Sci. 2015, 70, 593–596. [Google Scholar] [CrossRef] [PubMed]
- Wilson, M.L.; Strayer, T.E., III; Davis, R.; Harden, S.M. Use of an integrated research-practice partnership to improve outcomes of a community-based strength-training program for older adults: Reach and effect of Lifelong Improvements through Fitness Together (LIFT). Int. J. Environ. Res. Public Health 2018, 15, 237. [Google Scholar] [CrossRef] [PubMed]
- Koniak-Griffin, D.; Brecht, M.-L.; Takayanagi, S.; Villegas, J.; Melendrez, M.; Balcázar, H. A community health worker-led lifestyle behavior intervention for Latian (Hispanic) women: Feasibility and outcomes of a randomized controlled trial. Int. J. Nurs. Stud. 2015, 52, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Ockene, I.S.; Tellez, T.L.; Rosal, M.C.; Reed, G.W.; Mordes, J.; Merriam, P.A.; Olendzki, B.C.; Handelman, G.; Nicolosi, R.; Ma, Y. Outcome of a Latino community-based intervention for the prevention of diabetes: The Lawrence Latino Diabetes Prevention Project. Am. J. Public Health 2011, 102, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Connelly, J.; Kirk, A.; Masthoff, J.; MacRury, S. The use of technology to promote physical activity in type 2 diabetes management: A systematic review. Diabet. Med. 2013, 30, 1420–1432. [Google Scholar] [CrossRef] [PubMed]
- Bock, C.; Jarczok, M.N.; Litaker, D. Community-based efforts to promote physical activity: A systematic review of interventions considering mode of delivery, study quality and population subgroups. J. Sci. Med. Sport 2014, 17, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Foy, C.G.; Vitolins, M.Z.; Case, L.D.; Harris, S.J.; Massa-Fanlae, C.; Hopley, R.J.; Gardner, L.; Rudiger, N.; Yamamoto, K.; Swain, B.; et al. Incorporating prosocial behavioral to promote physical activity in older adults: Rationale and design of the Program for Active Aging and Community Engagement (PACE). Contemp. Clin. Trials 2013, 36, 284–297. [Google Scholar] [CrossRef] [PubMed]
- Hefler, M.; Freeman, B.; Chapman, S. Tobacco control advocacy in the age of social media: Using Facebook, Twitter and Change. Tob. Control 2013, 22, 210–214. [Google Scholar] [CrossRef] [PubMed]
- Burton, E.; Lewin, G.; Clemson, L.; Boldy, D. Effectiveness of a lifestyle exercise program for older people receiving a restorative home care services: A pragmatic randomized controlled trial. Clin. Interv. Aging. 2013, 8, 1591–1601. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.M.; Tsui, C.M. A randomized trial comparing Tai Chi with and without cognitive-behavioral intervention (CBI) to reduce fear of falling in community-dwelling elderly people. Arch. Geriatr. 2014, 59, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Foroushani, A.R.; Estebsari, F.; Mostafaei, D.; Ardebili, H.E.; Shojaeizadeh, D.; Dastoorpour, M.; Jamshidi, E.; Taghdisi, M.H. The effect of health promoting intervention on healthy lifestyle and social support in elders: A clinical trial study. Iran. Red. Crescent Med. J. 2014, 16, e18399. [Google Scholar] [CrossRef] [PubMed]
- Ferry, M.; Coley, N.; Andrieu, S.; Bonhomme, C.; Caubere, J.P.; Cesari, M.; Gautry, J.; Garcia Sanchez, I.; Hugonot, L.; Mansuy, L.; et al. How to design nutritional intervention trials to slow cognitive decline in apparently healthy population and apply for efficacy claims: A statement from the International Academy on Nutrition and Aging Task Force. J. Nutr. Health Aging 2014, 17, 619–624. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Kuraoka, M.; Yasunaga, M.; Nonaka, K.; Sakurai, R.; Takeuchi, R.; Murayama, Y.; Ohba, H.; Fujiwara, Y. Cognitive intervention through a training program for picture book reading in community-dwelling older adults: A randomized controlled trail. BMC Geriatr. 2014, 14, 122. [Google Scholar] [CrossRef] [PubMed]
- Hötting, K.; Holzschneider, K.; Stenzel, A.; Wolbers, T.; Röder, B. Effects of a cognitive training on spatial learning and associated functional brain activations. BMC Neurosci. 2013, 14, 73. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, S.; Parrot, A.P.; Baruth, M.; Laken, M.; Condrasky, M.; Saunders, R.; Dowda, M.; Evans, R.; Addy, C.; Warren, T.Y.; et al. The faith, activity, and nutrition program. Am. J. Prev. Med. 2013, 44, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.K.; Ross, L.A.; Roth, D.L.; Edwards, J.D. Speed of processing training in the ACTIVE Study: How much is needed and who benefits? J. Aging Health 2013, 25, 65S. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; Berch, D.B.; Helmers, K.F.; Jobe, J.B.; Leveck, M.D.; Marsiskie, M.; Morris, J.N.; The ACTIVE Study Group. Effects of cognitive training interventions with older adults: A randomized controlled trial. J. Am. Med. Assoc. 2002, 288, 2271–2281. [Google Scholar] [CrossRef]
- Kueider, A.M.; Parisi, M.; Gross, A.L.; Rebok, G.W. Computerized cognitive training with older adults: A systematic review. PLoS ONE 2012, 7, e40588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angevaren, M.; Aufdemkampe, G.; Verhaar, H.J.; Aleman, A.; Vanhees, L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst. Rev. 2008, 16, CD005381. [Google Scholar] [CrossRef]
- Sink, K.M.; Espeland, M.A.; Castro, C.M.; Church, T.; Cohen, R.; Dodson, J.A.; Guralnik, J.; Hendrie, H.C.; Jennings, J.; Katula, J.; et al. LIFE Study Investigators. Effect of a 24-month physical activity intervention vs health education on cognitive outcomes in sedentary older adults: The LIFE randomized trial. JAMA 2015, 314, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Fledderus, M.; Bohlmeijer, E.T.; Smit, F.; Westerhof, G.J. Mental health promotion as a new goal in public mental care: A randomized controlled trial of an intervention enhancing psychological flexibility. Am. J. Public Health. 2011, 100, 2372–2378. [Google Scholar] [CrossRef] [PubMed]
- Li, K.Y.; Hsu, W.C.; Lin, L.J. Effect of the recreational life review program on patients with dementia in an outpatient clinic: A preliminary study. Percept. Mot. Skills 2014, 119, 949–960. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, L.N.; Szanton, S.L.; Huang, J.; Roth, D.L. Factors mediating the effects of a depression intervention on functional disability in older African Americans. J. Am. Geriatr. Soc. 2014, 62, 2280–2287. [Google Scholar] [CrossRef] [PubMed]
- Crisp, D.; Griffiths, K.; Mackinnon, A.; Bennett, K.; Christensen, H. An online intervention for reducing depressive symptoms: Secondary benefits for self-esteem, empowerment and quality of life. Psychiatr. Res. 2014, 216, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Sundsli, K.; Söderhamn, U.; Espnes, G.A.; Söderhamn, O. Self-care telephone talks as a health-promotion intervention in urban home-living persons 75+ years of age: A randomized controlled study. Clin. Interv. Aging 2014, 9, 95–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramirezl, E.; Ortega, A.R.; Chamorro, A.; Colmenero, J.M. A program of positive intervention in the elderly: Memories, gratitude and forgiveness. Aging Ment. Health 2014, 18, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Adams, K.B.; Leibbrandt, S.; Moon, H. A critical review of the literature on social and leisure activity and wellbeing in later life. Ageing Soc. 2011, 31, 683–712. [Google Scholar] [CrossRef]
- Huxhold, O.; Fiori, K.L.; Windsor, T.D. The dynamic interplay of social network characteristics, subjective well-being, and health: The costs and benefits of socio-emotional selectivity. Psychol. Aging 2013, 28, 3–16. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.L.; Hsu, H.C.; Chang-Lee, S.N.; Yang, H.Y.; Sung, Y.H. Successful aging awareness and retirement preparation in a sample of medical center employees. Chung Shan Med. J. 2014, 25, 11–20. [Google Scholar]
- Lin, J.P. Life Satisfaction among older adults in Taiwan: The effects of marital relations. In Successful Aging: Asian Perspectives; Cheng, S.T., Chi, I., Fung, H.H., Li, L.W., Woo, J., Eds.; Springer: New York, NY, USA, 2015; pp. 179–198. ISBN 978-94-017-9331-5. [Google Scholar]
- Proulx, C.M.; Snyder, L.A. Families and Health: An Empirical Resource Guide for Researchers and Practitioners. Fam. Relat. 2009, 58, 489–504. [Google Scholar] [CrossRef]
- Hopkinson, J.B.; Richardson, A. A mixed-methods qualitative research study to develop a complex intervention for weight loss and anorexia in advanced cancer: The family approach to weight and eating. Palliat. Med. 2015, 29, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Boltz, M.; Resnick, B.; Chippendale, T.; Galvin, J. Testing a family-centered intervention to promote functional and cognitive recovery in hospitalized older adults. J. Am. Geriatr. Soc. 2014, 62, 2398–2407. [Google Scholar] [CrossRef] [PubMed]
- Reid, R.D.; McDonnell, L.A.; Riley, D.L.; Mark, A.E.; Mosca, L.; Beaton, L.; Papadakis, S.; Blanchard, C.M.; Mochari-Greenberger, H.; O’Farrell, P.; et al. Effect of an intervention to improve the cardiovascular health of family members of patients with coronary artery disease: A randomized trial. CMAJ 2014, 186, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kwon, J.; Anderson, E.A. Factors related to retirement confidence: Retirement preparation and workplace financial education. J. Financ. Counsel. Plan. Educ. 2005, 16, 77–89. [Google Scholar]
- Hsu, H.C. Exploring elderly people’s perspective on successful aging in Taiwan. Ageing Soc. 2007, 27, 87–102. [Google Scholar] [CrossRef]
- UNECE Active Aging Group. Project ‘Active Ageing Index (AAI)’ 2012. Concept, Methodology and Final Results; UNECE Grant No: ECE/GC/2012/003; UNECE: Vienna, Austria, 2013. [Google Scholar]
- Alexander, G.L.; McClure, J.B.; Clavi, J.H.; Divine, G.W.; Stopponi, M.A.; Rolnick, S.J.; Heimendinger, J.; Tolsma, D.D.; Resnicow, K.; Campbell, M.K.; et al. MENU Choices Team. A randomized clinical trial evaluating online interventions to improve fruit and vegetable consumption. Am. J. Public Health 2010, 100, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Boekhout, J.M.; Berendsen, B.A.J.; Peels, D.A.; Bolman, C.A.W.; Lechner, L. Evaluation of a computer-tailored healthy ageing intervention to promote physical activity among single older adults with a chronic disease. International. J. Environ. Res. Public Health 2018, 15, 346. [Google Scholar] [CrossRef] [PubMed]
- Anderson-Bill, E.S.; Winett, R.A.; Wojcik, J.R. Social cognitive determinants of nutrition and physical activity among web-health users enrolling in an online intervention: The influence of social support, self-efficacy, outcome expectations, and self-regulation. J. Med. Internet Res. 2011, 13, e8. [Google Scholar] [CrossRef] [PubMed]
- Balastouskas, P.; Kennedy, C.M.; Buchan, I.; Powell, J.; Ainsworth, J. The role of social network technologies in online health promotion: A narrative review of theoretical and empirical factors influencing intervention effectiveness. J. Med. Internet Res. 2015, 17, e141. [Google Scholar] [CrossRef] [PubMed]
- Bewick, B.M.; Rumball, K.; Birtwistle, J.C.; Shaw, J.R.; Johnson, O.; Raistrick, D.; Tober, G. Developing a web-based intervention to increase motivation to change and encourage uptake of specialist face-to-face treatment by hospital inpatients: Change Drinking. Drug Alcohol Rev. 2014, 33, 674–677. [Google Scholar] [CrossRef] [PubMed]
- Stratton, E.; Lampit, A.; Choi, I.; Calvo, R.A.; Harvey, S.B.; Glozier, N. Effectiveness of eHealth interventions for reducing mental health conditions in employees: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0189904. [Google Scholar] [CrossRef] [PubMed]
- Eaton, L.H.; Doorenbos, A.Z.; Schmitz, K.L.; Carpenter, K.M.; McGergor, B.A. Establishing treatment fidelity in a web-based behavioral intervention study. Nurs. Res. 2011, 60, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.; Ferguson, M.; Vandelanotte, C.; Plotnikoff, R.; de Boudeaudhuij, I.; Thomas, S.; Nelson-Field, K.; Olds, T. A web-based, social networking physical activity intervention for insufficiently active adults delivered via Facebook App: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e174. [Google Scholar] [CrossRef] [PubMed]
- Morrell, R.W.; Mayhorn, C.B.; Echt, K.V. Why older adults use or dot not use the Internet. In Gerotechnology: Research and Practice in Technology and Aging: A Textbook and Reference for Multiple Disciplines; Burdick, D.C., Kwon, S., Eds.; Springer: New York, NY, USA, 2004; pp. 71–85. ISBN 0826125166. [Google Scholar]
- Pak, R.; McLaughlin, A. Designing Displays for Older Adults; CRC Press, Taylor & Francis Group: Boca Raton, FL, USA, 2011; ISBN 978-1439801390. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-Mental State: A practical method for grading the state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nagi, S.Z. An epidemiology of disability among adults in the United States. Milbank Mem. Fund Q. Health Soc. 1976, 54, 439–467. [Google Scholar] [CrossRef] [PubMed]
- Radloff, L.S. The CES-D scale: A self-reported depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment (MoCA): A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Baltes, P.B.; Baltes, M.M. Psychological perspectives on successful aging: The model of selective optimization with compensation. In Successful Aging: Perspectives from the Behavioral Sciences; Baltes, P.B., Baltes, M.M., Eds.; Cambridge University Press: Cambridge, UK, 1990; pp. 1–34. ISBN 978-0521435826. [Google Scholar]
- Donnellan, C.; Hevey, D.; Hickey, A.; O’Neill, D. Adaptation to stroke using a model of successful aging. Neuropsychol. Dev. Cogn. B Aging. Neuropsychol. Cogn. 2012, 19, 530–547. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the Brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef] [PubMed]
- Liang, K.Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Linnan, L.; Steckler, A. Process evaluation for public health interventions and research: An overview. In Process Evaluation for Public Health Interventions and Research; Steckler, A., Linan, L., Eds.; Jossey-Bass, John Wiley & Sons: San Francisco, CA, USA, 2002; pp. 1–24. ISBN 978-078795976069. [Google Scholar]


{kind=link}
| Variables | P2P (n = 61) | P&D (n = 54) | Control (n = 32) | Significance |
|---|---|---|---|---|
| Age | 77.25 (8.27) | 76.57 (7.01) | 78.16 (7.07) | |
| Sex | ||||
| Male | 16.7% | 25.9% | 28.1% | |
| Female | 83.3% | 74.1% | 71.9% | |
| Education | ||||
| Illiterate | 10.0% | 20.4% | 18.8% | * |
| Elementary school | 30.0% | 42.6% | 40.6% | |
| Primary high school | 23.3% | 18.5% | 28.1% | |
| Senior high school | 21.7% | 16.7% | 12.5% | |
| College/University + | 15.0% | 0.0% | 0.0% | |
| Marital status | ||||
| No spouse | 63.3% | 59.3% | 53.1% | |
| Having spouse | 36.7% | 40.7% | 46.9% | |
| Ethnic groups | ||||
| Mingnan | 63.3% | 88.9% | 90.3% | ** |
| Hakka | 5.0% | 1.9% | 6.5% | |
| Mainland provinces | 30.0% | 9.3% | 3.2% | |
| Aboriginal and others | 1.7% | 0.0% | 0.0% | |
| Religion belief | ||||
| None | 15.0% | 7.4% | 6.3% | *** |
| Buddhism, Dao, folk belief | 41.7% | 85.2% | 87.5% | |
| Christian, Catholics | 43.3% | 7.4% | 6.3% | |
| Don’t know/Refused to answer | 19.0% | 46.9% | 33.3% | |
| Relative income to others | ||||
| Higher | 5.2% | 0.0% | 5.6% | |
| About the same | 69.0% | 61.3% | 75.9% | |
| Lower | 25.9% | 38.7% | 18.5% | |
| Living arrangement | ||||
| Alone | 18.3% | 25.0% | 20.4% | |
| With others | 81.7% | 75.0% | 79.6% | |
| Family not living together | ||||
| No | 17.2% | 6.3% | 9.3% | |
| Yes | 82.8% | 93.8% | 90.7% |
| Evaluation | P2P Group | P&D Group | Control Group | |||
|---|---|---|---|---|---|---|
| Variables | Pre-test | Post-test | Pre-test | Post-test | Pre-test | Post-test |
| Self-rated health | 3.10 (0.75) | 3.38 (0.78) * | 3.31 (1.01) | 3.33 (0.91) | 2.84 (0.99) | 3.31 (1.18) * |
| Regular exercise (%) | 77.90% | 88.10% | 72.20% | 77.80% | 76.60% | 80.00% |
| Sedentary activity hours | 4.69 (3.08) | 5.03 (3.76) | 5.58 (4.58) | 4.25 (2.40) | 4.97 (2.50) | 5.73 (4.30) |
| Diet behavior and diet literacy | 30.87 (4.76) | 31.75 (4.34) | 31.95 (4.47) | 33.42 (5.16) * | 30.52 (3.75) | 32.32 (4.29) * |
| No nutrition risk (%) | 82.5% | 96.5% ** | 88.9% | 87.0% | 90.0% | 86.7% |
| Cognitive function | 22.91 (5.01) | 23.37 (5.51) | 17.94 (6.09) | 18.86 (6.08) | 17.89 (6.58) | 18.39 (5.94) |
| Depressive symptoms | 5.92 (5.06) | 5.53 (4.67) | 4.87 (5.05) | 5.04 (5.26) | 5.17 (5.91) | 5.13 (6.46) |
| Adaptation: selection | 5.05 (1.13) | 5.13 (1.13) | 4.25 (1.95) | 4.90 (1.09) ** | 4.87 (1.31) | 4.13 (1.07) ** |
| Adaptation: optimization | 5.65 (0.66) | 5.42 (0.87) | 5.33 (0.86) | 5.44 (0.98) | 5.63 (0.62) | 5.40 (0.81) |
| Adaptation: compensation | 5.22 (1.15) | 4.98 (1.24) | 5.21 (1.29) | 5.27 (1.17) | 5.23 (1.17) | 5.37 (1.16) |
| Action and positive thinking coping | 3.18 (0.64) | 3.10 (0.78) | 2.73 (0.90) | 3.00 (0.73) | 2.51 (0.96) | 2.88 (0.93) |
| Negative coping | 2.74 (0.60) | 2.37 (0.72) ** | 2.25 (0.71) | 2.51 (0.72) | 2.34 (0.75) | 2.28 (0.71) |
| Emotion-focused coping | 1.90 (0.69) | 1.77 (0.75) | 1.63 (0.70) | 1.66 (0.76) | 1.62 (0.80) | 1.53 (0.65) |
| Family social support | 9.92 (1.99) | 9.68 (1.96) | 9.85 (1.88) | 10.13 (1.93) | 9.15 (2.34) | 9.92 (1.76) |
| Friend social support | 7.69 (1.44) | 7.45 (1.50) | 8.57 (1.63) | 8.80 (1.60) | 7.68 (1.82) | 8.32 (1.49) |
| Conflict with family members | 14.3% | 4.8% | 13.0% | 4.3% | 8.3% | 8.3% |
| Use of Internet | 23.7% | 30.5% | 15.7% | 17.6% | 10.3% | 6.9% |
| Search for health information | 20.3% | 22.0% | 40.0% | 66.7% | 6.9% | 6.9% |
| Financial preparation | 61.0% | 62.7% | 58.8% | 58.8% | 31.0% | 62.1% * |
| Financial security knowledge | 27.1% | 45.8% * | 25.5% | 29.4% | 24.1% | 20.7% |
| Life satisfaction | 3.88 (0.67) | 4.02 (0.66) | 3.90 (1.05) | 4.31 (0.84) ** | 3.34 (0.23) | 3.72 (0.22) |
| Physical Health and Health Behaviors | Self-Rated Health | Regular Exercise | Sedentary Activity Hours per Day | Diet Behaviors and Diet Literacy | No Nutrition Risk | |||
| Intercept | 3.362 (0.694) *** | 2.839 (2.061) | 7.119 (2.578) ** | 26.841 (3.644) *** | 4.983 (2.369) * | |||
| P2P Group | 0.165 (0.189) | 0.121 (0.549) | −0.254 (0.653) | −0.727 (0.904) | −0.552 (0.706) | |||
| P&D Group | 0.448 (0.214) * | −0.214 (0.528) | 0.341 (0.782) | 1.335 (0.870) | −0.116 (0.728) | |||
| Time (months) | 0.081 (0.032) * | 0.016 (0.086) | 0.092 (0.141) | 0.294 (0.125) * | 0.014 (0.125) | |||
| P2P * Time | 0.008 (0.048) | 0.189 (0.153) | −0.010 (0.237) | 1.490 × 10−16 (0.235) | 0.573 (0.251) | |||
| P&D * Time | −0.074 (0.049) | 0.084 (0.131) | −0.502 (0.264) | 0.219 (0.248) | −0.073 (0.200) * | |||
| Age | −0.006 (0.008) | −0.021 (0.025) | −0.022 9).029) | 0.004 (0.042) | −0.033 (0.029) | |||
| Sex (Female) | −0.390 (0.184) * | −0.112 (0.428) | 0.534 (0.544) | 2.448 (0.863) ** | −0.348 (0.609) | |||
| Education | 0.163 (0.054) ** | −0.004 (0.172) | −0.420 (0.209) * | 1.196 (0.297) *** | −0.002 (0.207) | |||
| QIC # | 236.676 | 315.408 | 3409.545 | 5281.812 | 207.184 | |||
| Mental Health | Cognitive Function | Depressive Symptoms | Adaptation: Selection | Adaptation: Optimization | Adaptation: Compensation | Coping: Action and Positive Thinking | Coping: Negative | Coping: Emotion-Focused |
| Intercept | 29.936 (5.246) *** | 3.371 (4.107) | 4.341 (0.767) *** | 5.232 (0.595) *** | 6.984 (0.922) *** | 2.863 (0.577) *** | 2.699 (0.477) *** | 2.192 (0.489) *** |
| P2P Group | 2.840 (1.331) * | 0.958 (1.240) | 0.165 (0.280) | −0.058 (0.131) | 0.013 (0.255) | 0.543 (0.188) ** | 0.227 (0.168) | 0.406 (0.156) ** |
| P&D Group | −0.049 (1.268) | −0.385 (1.243) | −0.554 (0.294) | −0.327 (0.156) * | −0.059 (0.271) | 0.169 (0.204) | −0.082 (0.173) | −0.076 (0.162) |
| Time (months) | 0.112 (0.132) ** | −0.028 (0.191) | −0.122 (0.042) ** | −0.039 (0.025) | 0.006 (0.046) | 0.064 (0.037) | −0.013 (0.034) | −0.008 (0.029) |
| P2P * Time | 0.055 (0.227) | −0.100 (0.285) | 0.150 (0.076) * | −0.039 (0.048) | −0.083 (0.075) | −0.085 (0.053) | −0.029 (0.049) | −0.114 (0.044) ** |
| P&D * Time | 0.132 (0.231) | 0.154 (0.247) | 0.323 (0.078) *** | 0.061 (0.058) | 0.004 (0.076) | 0.023 (0.059) | 0.018 (0.058) | 0.081 (0.054) |
| Age | −0.205 (0.060) ** | 0.032 (0.049) | 0.002 (0.008) | 0.001 (0.007) | −0.021 (0.010) * | −0.009 (0.007) | −0.013 (0.006) * | 0.000 (0.056) |
| Sex (Female) | 0.677 (1.049) | 0.131 (1.038) | 0.234 (0.216) | 0.458 (0.145) ** | 0.014 (0.207) | 0.402 (0.140) ** | 0.122 (0.090) | 0.230 (0.108) * |
| Education | 2.507 (0.376) *** | −0.471 (0.379) | 0.089 (0.067) | 0.023 (0.043) | −0.079 (0.076) | 0.079 (0.046) | −0.051 (0.038) | −0.019 (0.041) |
| QIC # | 6540.177 | 7782.505 | 398.338 | 199.566 | 423.882 | 186.490 | 158.808 | 151.390 |
| Social Outcome | Family Social Support | Friend Social Support | Conflict with Any Family Members # | Use of Internet | Search for Health Information | Financial Preparation | Financial Security Law Knowledge | Life Satisfaction |
| Intercept | 8.963 (1.588) *** | 7.829 (1.295) *** | 5.900 (4.806) | 7.556 (2.456) ** | 7.157 (2.583) ** | 1.781 (1.617) | 1.423 (1.726) | 4.213 (0.671) *** |
| P2P Group | 0.492 (0.459) | −0.075 (0.398) | 0.806 (0.976) | 0.536 (0.791) | 0.852 (0.833) | 0.935 (0.512) | −0.302 (0.516) | 0.441 (0.218) * |
| P&D Group | 0.514 (0.457) | 0.796 (0.395) * | 0.119 (0.980) | 0.383 (0.825) | 0.776 (0.867) | 1.038 (0.527) * | −0.007 (0.518) | 0.464 (0.247) |
| Time (months) | 0.127 (0.063) * | 0.065 (0.055) | −0.080 (0.100) | −0.101 (0.163) | −0.004 (0163) | 0.180 (0.083) * | −0.045 (0.073) | 0.048 (0.036) |
| P2P * Time | −0.206 (0.096) * | −0.159 (0.099) | −0.531 (0.356) | 0.278 (0.199) | 0.068 (0.198) | −0.139 (0.132) | 0.344 (0.142) * | −0.003 (0.047) |
| P&D * Time | −0.050 (0.123) | −0.006 (0.099) | −0.213 (0.368) | 0.160 (0.208) | 0.884 (0.305) ** | −0.222 (0.159) | 0.108 (0.158) | 0.073 (0.061) |
| Age | 0.003 (0.019) | 0.003 (0.015) | −0.094 (0.058) | −0.152 (0.031) *** | −0.159 (0.031) *** | −0.034 (0.019) | −0.049 (0.021) * | −0.008 (0.008) |
| Sex (Female) | −0.137 (0.301) | −0.610 (0.261) * | −0.622 (0.733) | 0.149 (0.543) | −0.168 (0.657) | −0.193 (0.360) | 0.221 (0.421) | −0.315 (0.171) |
| Education | 0.166 (0.140) | 0.122 (0.099) | −0.336 (0.417) | 0.873 (0.210) *** | 1.105 (0.257) *** | 0.226 (0.125) | 0.678 (0.172) *** | 0.050 (0.056) |
| QIC # | 1036.473 | 637.722 | 103.719 | 207.208 | 159.629 | 388.300 | 316.777 | 239.243 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, H.-C.; Kuo, T.; Lin, J.-P.; Hsu, W.-C.; Yu, C.-W.; Chen, Y.-C.; Xie, W.-Z.; Hsu, W.-C.; Hsu, Y.-L.; Yu, M.-T. A Cross-Disciplinary Successful Aging Intervention and Evaluation: Comparison of Person-to-Person and Digital-Assisted Approaches. Int. J. Environ. Res. Public Health 2018, 15, 913. https://doi.org/10.3390/ijerph15050913
Hsu H-C, Kuo T, Lin J-P, Hsu W-C, Yu C-W, Chen Y-C, Xie W-Z, Hsu W-C, Hsu Y-L, Yu M-T. A Cross-Disciplinary Successful Aging Intervention and Evaluation: Comparison of Person-to-Person and Digital-Assisted Approaches. International Journal of Environmental Research and Public Health. 2018; 15(5):913. https://doi.org/10.3390/ijerph15050913
Chicago/Turabian StyleHsu, Hui-Chuan, Tsuann Kuo, Ju-Ping Lin, Wei-Chung Hsu, Chia-Wen Yu, Yen-Cheng Chen, Wan-Zhen Xie, Wei-Chiang Hsu, Ya-Lan Hsu, and Mu-Ting Yu. 2018. "A Cross-Disciplinary Successful Aging Intervention and Evaluation: Comparison of Person-to-Person and Digital-Assisted Approaches" International Journal of Environmental Research and Public Health 15, no. 5: 913. https://doi.org/10.3390/ijerph15050913
APA StyleHsu, H. -C., Kuo, T., Lin, J. -P., Hsu, W. -C., Yu, C. -W., Chen, Y. -C., Xie, W. -Z., Hsu, W. -C., Hsu, Y. -L., & Yu, M. -T. (2018). A Cross-Disciplinary Successful Aging Intervention and Evaluation: Comparison of Person-to-Person and Digital-Assisted Approaches. International Journal of Environmental Research and Public Health, 15(5), 913. https://doi.org/10.3390/ijerph15050913