Effect of a Positive Photo Appreciation Program on Depressive Mood in Older Adults: A Pilot Randomized Controlled Trial

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
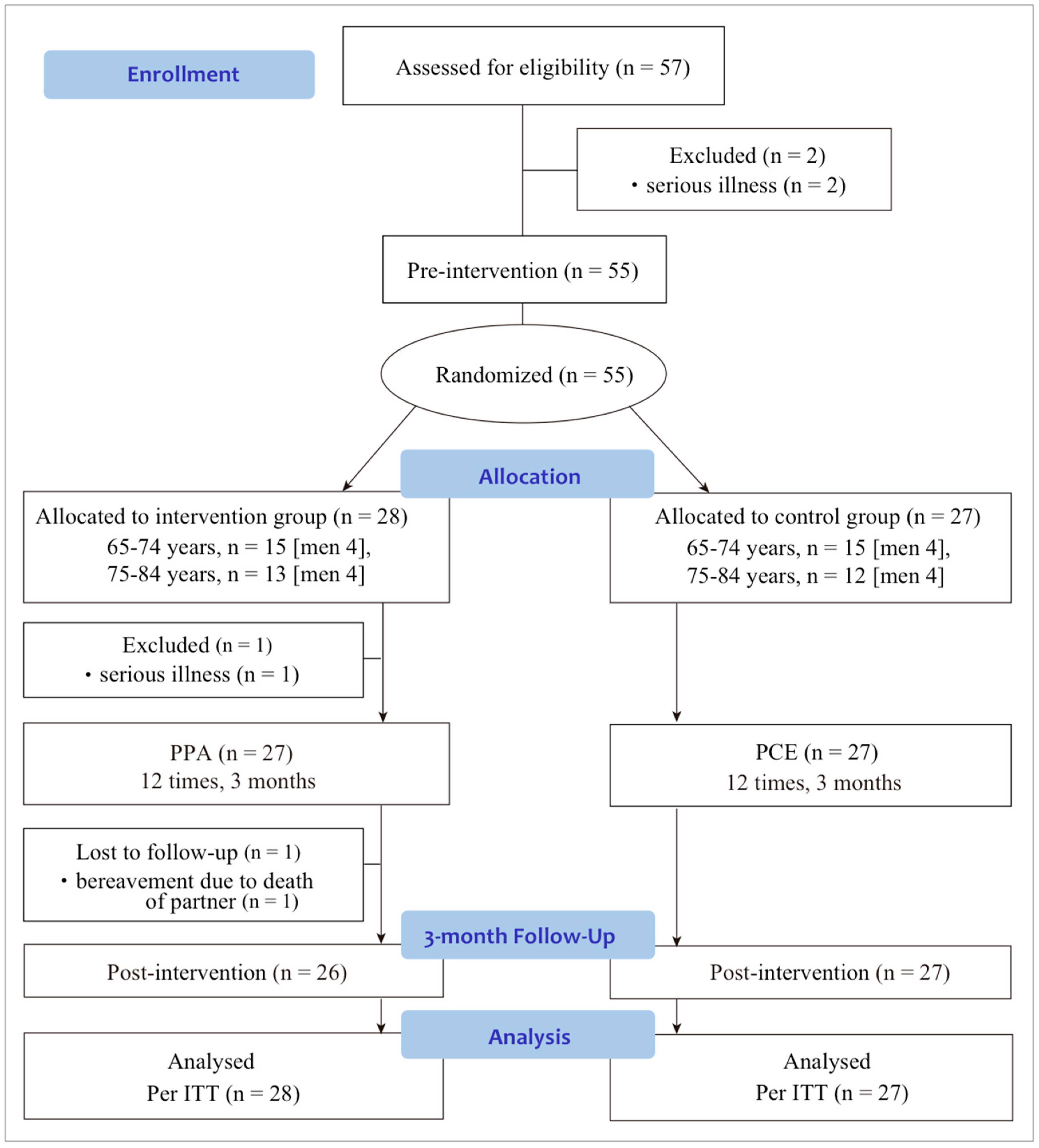
2.2. Participants
2.3. Study Settings
2.4. Randomization
2.5. Interventions
2.5.1. PPA Program (Intervention Group)
2.5.2. Photo Correspondence Education (Control Group)
2.6. Outcome Measures
2.6.1. Primary Outcome Measures
2.6.2. Secondary Outcome Measures
2.7. Statistics
3. Results
3.1. Baseline Characteristics of Study Participants
3.2. Feasibility of the PPA Program
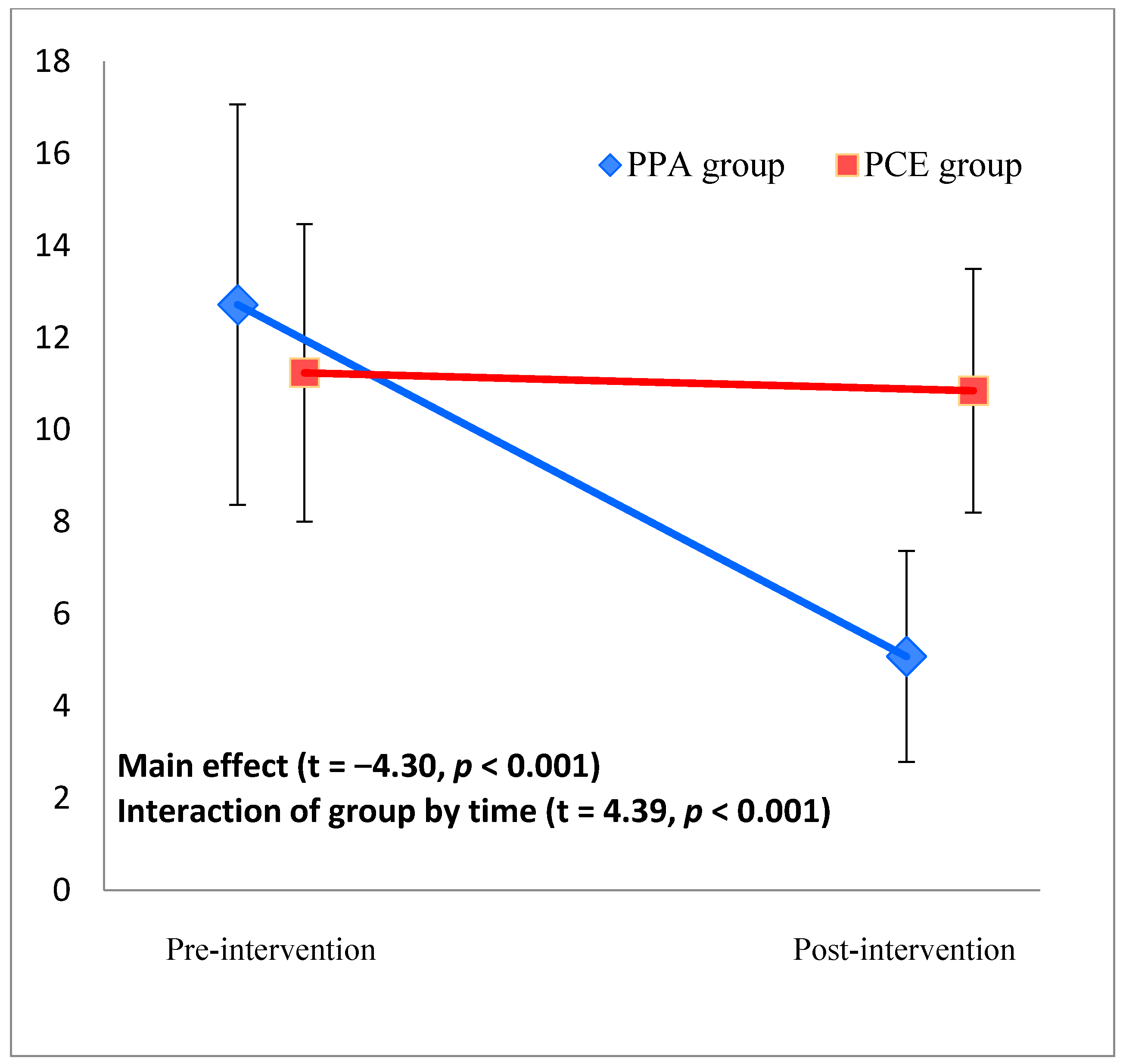
3.3. Primary Outcome: CES-D Score
3.4. Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Measurement | Group | Pre-Intervention | Post-Intervention | Measurement (Group) | Interaction Effect (Group by Time) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | n | Mean ± SD | n | t | p | t | p | ||
| Male | PPA | 11.43 ± 3.40 | 7 | 3.13 ± 3.23 | 8 | −2.66 | 0.019 | 4.56 | 0.001 |
| PCE | 7.13 ± 4.91 | 8 | 9.00 ± 5.35 | 8 | |||||
| Female | PPA | 13.10 ± 9.70 | 20 | 5.94 ± 4.89 | 17 | −3.49 | 0.001 | 2.70 | 0.011 |
| PCE | 13.17 ± 2.01 | 18 | 11.63 ± 5.22 | 19 | |||||
| Younger | PPA | 14.07 ± 9.72 | 15 | 5.87 ± 4.93 | 15 | −2.71 | 0.011 | 3.23 | 0.003 |
| PCE | 10.06 ± 6.22 | 16 | 10.29 ± 4.22 | 17 | |||||
| Older | PPA | 10.92 ± 6.63 | 12 | 4.00 ± 3.92 | 11 | −3.40 | 0.003 | 3.55 | 0.002 |
| PCE | 13.33 ± 6.71 | 9 | 11.80 ± 6.91 | 10 | |||||
| Non Depression b | PPA | 8.95 ± 4.21 | 20 | 3.67 ± 2.61 | 19 | −4.78 | <0.001 | 4.61 | <0.001 |
| PCE | 8.28 ± 4.85 | 18 | 9.22 ± 4.70 | 18 | |||||
| Depression b | PPA | 23.29 ± 8.85 | 7 | 9.67 ± 6.25 | 6 | −2.06 | 0.064 | 2.39 | 0.035 |
| PCE | 18.86 ± 2.54 | 7 | 15.71 ± 4.42 | 7 | |||||
References
- Nations, U. World Population Prospects: The 2017 Revision; United Nations Publications: New York, NY, USA, 2017. [Google Scholar]
- Office, C. The Aging Society: Current Situation and Implementation Measures fy 2015; The Cabinet Office: Tokyo, Japan, 2016. [Google Scholar]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Ministry of Health, Law. Depression Prevention/Support Manual: Prevention Care Manual; Health, Labour and Welfare Statistics Association: Tokyo, Japan, 2012. [Google Scholar]
- Smoliner, C.; Norman, K.; Wagner, K.-H.; Hartig, W.; Lochs, H.; Pirlich, M. Malnutrition and depression in the institutionalised elderly. Br. J. Nutr. 2009, 102, 1663–1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sultzer, D.L.; Levin, H.S.; Mahler, M.E.; High, W.M.; Cummings, J.L. A comparison of psychiatric symptoms in vascular dementia and alzheimer’s disease. Am. J. Psychiatry 1993, 150, 1806. [Google Scholar] [PubMed]
- Pietrzak, R.H.; Lim, Y.Y.; Neumeister, A.; Ames, D.; Ellis, K.A.; Harrington, K.; Lautenschlager, N.T.; Restrepo, C.; Martins, R.N.; Masters, C.L. Amyloid-β, anxiety, and cognitive decline in preclinical alzheimer disease: A multicenter, prospective cohort study. JAMA Psychiatry 2015, 72, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Seligman, M.E.; Rashid, T.; Parks, A.C. Positive psychotherapy. Am. Psychol. 2006, 61, 774. [Google Scholar] [CrossRef] [PubMed]
- Rashid, T. Positive psychotherapy: A strength-based approach. J. Posit. Psychol. 2015, 10, 25–40. [Google Scholar] [CrossRef]
- Meyer, P.S.; Johnson, D.P.; Parks, A.; Iwanski, C.; Penn, D.L. Positive living: A pilot study of group positive psychotherapy for people with schizophrenia. J. Posit. Psychol. 2012, 7, 239–248. [Google Scholar] [CrossRef]
- Reinsch, C.C. Adding Science to the Mix of Business and Pleasure: An Exploratory Study of Positive Psychology Interventions with Teachers Accessing Employee Assistance Counselling; University of Manitoba: Winnipeg, MN, Canada, 2013. [Google Scholar]
- Uliaszek, A.A.; Rashid, T.; Williams, G.E.; Gulamani, T. Group therapy for university students: A randomized control trial of dialectical behavior therapy and positive psychotherapy. Behav. Res. Ther. 2016, 77, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.F.; Zhang, X.; Plummer, V.; Lam, L.; Cross, W.; Zhang, J.P. Positive psychotherapy for depression and self-efficacy in undergraduate nursing students: A randomized, controlled trial. Int. J. Ment. Health Nurs. 2017, 26, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.; Cassidy, M.; Priebe, S. The application of positive psychotherapy in mental health care: A systematic review. J. Clin. Psychol. 2017, 73, 638–651. [Google Scholar] [CrossRef] [PubMed]
- Schotanus-Dijkstra, M.; Pieterse, M.E.; Drossaert, C.H.; Walburg, J.A.; Bohlmeijer, E.T. Possible mechanisms in a multicomponent email guided positive psychology intervention to improve mental well-being, anxiety and depression: A multiple mediation model. J. Posit. Psychol. 2017, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Carstensen, L.L. Evidence for a life-span theory of socioemotional selectivity. Curr. Dir. Psychol. Sci. 1995, 4, 151–156. [Google Scholar] [CrossRef]
- Seligman, M.E.; Steen, T.A.; Park, N.; Peterson, C. Positive psychology progress: Empirical validation of interventions. Am. Psychol. 2005, 60, 410. [Google Scholar] [CrossRef] [PubMed]
- Bolier, L.; Haverman, M.; Kramer, J.; Westerhof, G.J.; Riper, H.; Walburg, J.A.; Boon, B.; Bohlmeijer, E. An internet-based intervention to promote mental fitness for mildly depressed adults: Randomized controlled trial. J. Med. Internet Res. 2013, 15. [Google Scholar] [CrossRef] [PubMed]
- Parks, A.C.; Szanto, R.K. Assessing the efficacy and effectiveness of a positive psychologybased self-help book. Terapia Psicol. 2013, 1, 141–148. [Google Scholar] [CrossRef]
- Schotanus-Dijkstra, M.; Drossaert, C.H.; Pieterse, M.E.; Walburg, J.A.; Bohlmeijer, E.T. Efficacy of a multicomponent positive psychology self-help intervention: Study protocol of a randomized controlled trial. JMIR Res. Protoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Schotanus-Dijkstra, M.; Drossaert, C.H.; Pieterse, M.E.; Boon, B.; Walburg, J.A.; Bohlmeijer, E.T. An early intervention to promote well-being and flourishing and reduce anxiety and depression: A randomized controlled trial. Internet Int. 2017, 9, 15–24. [Google Scholar] [CrossRef]
- Sloane-Seale, A.; Kops, B. Older adults’ participation in education and successful aging: Implications for university continuing education in Canada. Can. J. Univ. Contin. Educ. 2010, 36. [Google Scholar] [CrossRef]
- Matsumoto, Y. Faces of Aging: The Lived Experiences of the Elderly in Japan; Stanford University Press: Redwood City, CA, USA, 2011. [Google Scholar]
- Tam, M.; Chui, E. Ageing and learning: What do they mean to elders themselves? Stud. Contin. Educ. 2016, 38, 195–212. [Google Scholar] [CrossRef]
- Lambert, N.M.; Fincham, F.D.; Stillman, T.F. Gratitude and depressive symptoms: The role of positive reframing and positive emotion. Cognit. Emot. 2012, 26, 615–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, C. On Becoming a Person Boston; Houghton Mifflin: Boston, MA, USA, 1961. [Google Scholar]
- Rogers, C. On Becoming a Person: A Therapist's View of Psychotherapy; Houghton Mifflin Harcourt: Boston, MA, USA, 2012. [Google Scholar]
- Kitwood, T. Dementia Reconsidered: The Person Comes First; Oxford University Press: Buckingham, UK, 1997. [Google Scholar]
- Rogers, N. The Creative Connection: Expressive Arts as Healing; Science and Behavior Books: Palo Alto, CA, USA, 1993. [Google Scholar]
- Keltner, D.; Haidt, J. Social functions of emotions at four levels of analysis. Cognit. Emot. 1999, 13, 505–521. [Google Scholar] [CrossRef]
- Öhman, A. Automaticity and the amygdala: Nonconscious responses to emotional faces. Curr. Dir. Psychol. Sci. 2002, 11, 62–66. [Google Scholar] [CrossRef]
- Dimberg, U.; Thunberg, M.; Elmehed, K. Unconscious facial reactions to emotional facial expressions. Psychol. Sci. 2000, 11, 86–89. [Google Scholar] [CrossRef] [PubMed]
- Shima, S.; Shikano, T.; Kitamura, T.; Asai, M. On the new depression self-rating scale. Clin. Psychiatry 1985, 27, 717–723. [Google Scholar]
- Radloff, L.S. The ces-d scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Furukawa, T.A.; Kessler, R.C.; Slade, T.; Andrews, G. The performance of the k6 and k10 screening scales for psychological distress in the australian national survey of mental health and well-being. Psychol. Med. 2003, 33, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H. The performance of the japanese version of the k6 and k10 in the world mental health survey japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.; Demler, O.; Jin, R.; Koretz, D.; Merikangas, K.R.; Rush, A.J.; Walters, E.E.; Wang, P.S. The epidemiology of major depressive disorder: Results from the national comorbidity survey replication (NCS-R). JAMA 2003, 289, 3095–3105. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okada, K.; Kobayashi, S.; Aoki, K.; Suyama, N.; Yamaguchi, S. Assesment of motivational loss in poststroke patients using the japanese version of starkstein's apathy scale. Jpn. J. Stroke 1998, 20, 318–323. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Mayberg, H.S.; Preziosi, T.; Andrezejewski, P.; Leiguarda, R.; Robinson, R. Reliability, validity, and clinical correlates of apathy in parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 1992, 4, 134–139. [Google Scholar] [PubMed]
- Oishi, S. Culture and well-being: Conceptual and methodological issues. In International Differences in Well-Being; Diener, E., Kahneman, D., Helliwell, J.F., Eds.; Oxford University Press, Inc.: Oxford, UK, 2010; pp. 34–69. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Kawahito, J.; Otsuka, Y.; Kaida, K.; Nakata, A. Reliability and validity of the japanese version of 20-item positive and negative affect schedule. Hiroshima Psychol. Res. 2011, 11, 225–240. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The panas scales. J. Pers. Soc. Psychol. 1988, 54, 1063. [Google Scholar] [CrossRef] [PubMed]
- Watson, D.; Tellegen, A. Toward a consensual structure of mood. Psychol. Bull. 1985, 98, 219. [Google Scholar] [CrossRef] [PubMed]
- Shimada, H.; Makizako, H.; Park, H.; Lee, S. Validity of the national center for geriatrics and gerontology-functional assessment tool and mini-mental state examination for detecting the incidence of dementia in older japanese adults. Geriatr. Gerontol. Int. 2017, 17, 2383–2388. [Google Scholar] [CrossRef] [PubMed]
- Makizako, H.; Shimada, H.; Park, H.; Yoshida, D.; Uemura, K.; Tsutsumimoto, K.; Suzuki, T. Evaluation of multidimensional neurocognitive function using a tablet personal computer: Test-retest reliability and validity in community-dwelling older adults. Geriatr. Gerontol. Int. 2013, 13, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Taylor & Francis Inc.: Oxfordshire, UK, 1988. [Google Scholar]
- Cuadra-Peralta, A.; Veloso-Besio, C.; Ibergaray Perez, M.; Rocha Zuniga, M. Positive psychotherapy results in patients with depression. Terapia Psicol. 2010, 28, 127–134. [Google Scholar]
- Odou, N.; Vella-Brodrick, D.A. The efficacy of positive psychology interventions to increase well-being and the role of mental imagery ability. Soc. Indic. Res. 2013, 110, 111–129. [Google Scholar] [CrossRef]
- Chaves, C.; Lopez-Gomez, I.; Hervas, G.; Vazquez, C. A comparative study on the efficacy of a positive psychology intervention and a cognitive behavioral therapy for clinical depression. Cognit. Ther. Res. 2017, 41, 417–433. [Google Scholar] [CrossRef]
- O’Connor, M.; Piet, J.; Hougaard, E. The effects of mindfulness-based cognitive therapy on depressive symptoms in elderly bereaved people with loss-related distress: A controlled pilot study. Mindfulness 2014, 5, 400–409. [Google Scholar] [CrossRef]
- Ernst, S.; Welke, J.; Heintze, C.; Zöllner, A.; Kiehne, S.; Schwantes, U.; Esch, T. Effects of mindfulness-based stress reduction on quality of life in nursing home residents: A feasibility study. Forsch. Komplement./Res. Complement. Med. 2008, 15, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Yuki, A.; Otsuka, R.; Tange, C.; Nishita, Y.; Tomida, M.; Ando, F.; Shimokata, H. Epidemiology of frailty in elderly japanese. J. Phys. Fitness Sports Med. 2016, 5, 301–307. [Google Scholar] [CrossRef]


| Measurement a | PPA b Group | n | PCF b Group | n | p-Value | |
|---|---|---|---|---|---|---|
| Sociodemographic characteristics | ||||||
| Age (in years) | Mean ± SD | 74.29 ± 5.87 | 28 | 73.04 ± 5.01 | 27 | 0.847 |
| Sex (female) | n (%) | 20 (71.4%) | 28 | 19 (70.4%) | 27 | 1.00 |
| Education (in years) | Mean ± SD | 12.00 ± 2.71 | 28 | 12.22 ± 2.41 | 27 | 0.749 |
| Psychological measurements | ||||||
| CES-D | Mean ± SD | 12.67 ± 8.48 | 27 | 11.24 ± 6.46 | 25 | 0.501 |
| K-6 | Mean ± SD | 3.00 ± 3.19 | 28 | 3.35 ± 3.44 | 26 | 0.703 |
| Apathy Scale | Mean ± SD | 11.13 ± 5.40 | 23 | 11.42 ± 5.61 | 24 | 0.860 |
| SWLS | Mean ± SD | 24.29 ± 5.87 | 28 | 23.63 ± 6.25 | 27 | 0.690 |
| PANAS | Mean ± SD | 34.40 ± 7.76 | 25 | 34.20 ± 6.46 | 25 | 0.922 |
| Cognitive measurements | ||||||
| DSC_90 | Mean ± SD | 46.57 ± 8.89 | 28 | 43.89 ± 10.08 | 27 | 0.299 |
| DSC_120 | Mean ± SD | 63.60 ± 12.08 | 28 | 59.63 ± 13.64 | 27 | 0.257 |
| FS | Mean ± SD | 5.89 ± 1.23 | 28 | 6.04 ± 1.26 | 27 | 0.688 |
| ADAS1 | Mean ± SD | 7.74 ± 0.96 | 28 | 7.98 ± 1.15 | 27 | 0.411 |
| ADAS2 | Mean ± SD | 4.00 ± 2.11 | 28 | 4.11 ± 2.69 | 27 | 0.865 |
| ADAS3 | Mean ± SD | 7.50 ± 1.20 | 28 | 7.52 ± 1.89 | 27 | 0.965 |
| TMT_A | Mean ± SD | 25.25 ± 19.73 | 28 | 24.89 ± 13.24 | 27 | 0.937 |
| TMT_B | Mean ± SD | 35.36 ± 12.86 | 28 | 44.88 ± 30.41 | 27 | 0.142 |
| SM1 | Mean ± SD | 6.64 ± 1.91 | 28 | 7.22 ± 2.01 | 27 | 0.277 |
| SM2 | Mean ± SD | 7.18 ± 1.79 | 28 | 7.52 ± 1.70 | 27 | 0.473 |
| Attendance | |
| Perfect attendance | 82.1% |
| Absent once | 7.1% |
| 7 times absent | 3.6% |
| Lost to follow up: owing to a serious illness | 3.6% |
| Lost to follow up: owing to the bereavement due to death of partner | 3.6% |
| Evaluation of Participants | |
| Very enjoyable | 82.1% |
| Enjoyable | 7.1% |
| Normal | 3.6% |
| Not enjoyable | 0% |
| Not very enjoyable | 0% |
| Lost to follow up: owing to a serious illness | 3.6% |
| Lost to follow up: owing to the bereavement due to death of partner | 3.6% |
| Measurement a | Group | Pre-Intervention | Post-Intervention | Main Effect (Group) | Interaction Effect (Group by Time) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | n | Mean ± SD | n | t | p | t | p | ||
| Psychological measurements | |||||||||
| K-6 | PPA | 3.00 ± 3.19 | 28 | 2.21 ± 2.77 | 24 | −1.50 | 0.141 | 1.10 | 0.276 |
| PCE | 3.35 ± 3.44 | 26 | 3.22 ± 2.89 | 27 | |||||
| Apathy | PPA | 11.13 ± 5.40 | 23 | 9.32 ± 4.71 | 25 | −1.64 | 0.107 | 0.92 | 0.362 |
| PCE | 11.42 ± 5.61 | 24 | 11.32 ± 4.81 | 25 | |||||
| SWLS | PPA | 24.29 ± 5.87 | 28 | 25.31 ± 6.66 | 26 | 0.49 | 0.624 | −0.11 | 0.917 |
| PCE | 23.63 ± 6.25 | 27 | 24.56 ± 5.15 | 27 | |||||
| PANAS | PPA | 34.40 ± 7.76 | 25 | 40.92 ± 7.33 | 24 | 1.79 | 0.080 | −2.33 | 0.024 |
| PCE | 38.12 ± 6.85 | 25 | 37.22 ± 7.37 | 27 | |||||
| Cognitive measurements | |||||||||
| DSC_90 | PPA | 46.57 ± 8.89 | 28 | 48.65 ± 10.62 | 26 | 1.26 | 0.212 | −0.65 | 0.520 |
| PCE | 43.89 ± 10.08 | 27 | 45.29 ± 10.33 | 27 | |||||
| DSC_120 | PPA | 63.60 ± 12.08 | 28 | 65.73 ± 13.77 | 26 | 1.25 | 0.217 | −0.38 | 0.703 |
| PCE | 59.63 ± 13.64 | 27 | 61.22 ± 13.91 | 27 | |||||
| FS | PPA | 5.89 ± 1.23 | 28 | 5.85 ± 0.97 | 26 | 0.43 | 0.668 | −0.64 | 0.523 |
| PCE | 6.04 ± 1.26 | 27 | 5.70 ± 1.35 | 27 | |||||
| ADAS1 | PPA | 7.74 ± 0.96 | 28 | 7.87 ± 10.62 | 26 | -0.67 | 0.509 | −0.11 | 0.914 |
| PCE | 7.98 ± 1.15 | 27 | 8.05 ± 1.11 | 27 | |||||
| ADAS2 | PPA | 4.00 ± 2.11 | 28 | 5.31 ± 1.69 | 26 | 0.82 | 0.411 | −1.08 | 0.287 |
| PCE | 4.11 ± 2.69 | 27 | 4.89 ± 2.17 | 27 | |||||
| ADAS3 | PPA | 7.50 ± 1.20 | 28 | 7.31 ± 1.67 | 26 | −0.53 | 0.602 | 0.51 | 0.611 |
| PCE | 7.52 ± 1.89 | 27 | 7.56 ± 2.06 | 27 | |||||
| TMT_A | PPA | 25.25 ± 19.73 | 26 | 19.69 ± 4.40 | 26 | − b | 0.942 b | − b | 0.727 b |
| PCE | 24.89 ± 13.24 | 27 | 20.56 ± 5.24 | 27 | |||||
| TMT_B | PPA | 35.36 ± 12.86 | 28 | 36.15 ± 14.78 | 26 | −1.31 | 0.194 | 0.06 | 0.956 |
| PCE | 44.88 ± 30.41 | 27 | 45.96 ± 35.96 | 27 | |||||
| SM1 | PPA | 6.64 ± 1.91 | 28 | 8.35 ± 0.98 | 26 | 0.39 | 0.695 | −1.84 | 0.072 |
| PCE | 7.22 ± 2.01 | 27 | 8.19 ± 1.78 | 27 | |||||
| SM2 | PPA | 7.18 ± 1.79 | 28 | 8.30 ± 1.35 | 26 | 0.29 | 0.776 | −1.38 | 0.173 |
| PCE | 7.51 ± 1.70 | 27 | 8.15 ± 1.77 | 27 | |||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ishihara, M.; Saito, T.; Sakurai, T.; Shimada, H.; Arai, H. Effect of a Positive Photo Appreciation Program on Depressive Mood in Older Adults: A Pilot Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2018, 15, 1472. https://doi.org/10.3390/ijerph15071472
Ishihara M, Saito T, Sakurai T, Shimada H, Arai H. Effect of a Positive Photo Appreciation Program on Depressive Mood in Older Adults: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2018; 15(7):1472. https://doi.org/10.3390/ijerph15071472
Chicago/Turabian StyleIshihara, Masumi, Tami Saito, Takashi Sakurai, Hiroyuki Shimada, and Hidenori Arai. 2018. "Effect of a Positive Photo Appreciation Program on Depressive Mood in Older Adults: A Pilot Randomized Controlled Trial" International Journal of Environmental Research and Public Health 15, no. 7: 1472. https://doi.org/10.3390/ijerph15071472
APA StyleIshihara, M., Saito, T., Sakurai, T., Shimada, H., & Arai, H. (2018). Effect of a Positive Photo Appreciation Program on Depressive Mood in Older Adults: A Pilot Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 15(7), 1472. https://doi.org/10.3390/ijerph15071472