Food Reference Budgets as a Potential Policy Tool to Address Food Insecurity: Lessons Learned from a Pilot Study in 26 European Countries



{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
- (1)
- a single man [35–45-years-old]
- (2)
- a single woman [35–45-years-old]
- (3)
- a couple [man, woman; 35–45-years-old]
- (4)
- a single woman [35–45-years-old] + 2 children [primary school boy, 10-years-old + secondary school girl, 14-years-old].
- (5)
- a couple [35–45-years-old] + 2 children [primary school boy, 10-years-old + secondary school girl, 14-years-old].
- -
- The household types are assumed to live in the capital city of each participant country. This point is particularly relevant in terms of the pricing of the items and the frequency in which people rely on the production of food for own consumption.
- -
- All meals are prepared and eaten at home. All food is acquired, prepared and consumed in the most economical way possible. This means families are well-informed about prices and are able to shop in the most economic retailers that are accessible with public transport. However, we do not assume that people can always buy all their ingredients in the cheapest available supermarket. Hence, we allowed for a certain freedom of choice to shop within a range of cheap retailers.
- -
- All household members are in good health and do not have specific dietary requirements. The reason for this assumption is not so much that this is the most common health condition, but rather that the cost of a diet varies depending on the kind and severity of health problems, each having different implications for the needs of the person affected.
- -
- The ingredients should give families access to healthy, tasty and well varied meals. The food basket should be acceptable for citizens with different background characteristics provided that the healthy aspect is not compromised.
- -
- Finally, we assume that the budget for food is allocated to each household member in accordance with her/his needs.
- (1)
- For the first milestone, the national experts provided a clear description of the scientific basis (DRVs) of the national FBDG, the results of the last food consumption survey and the model of health education in their country.
- (2)
- In the following step, in cooperation with a nutritionist, country teams translated the FBDG into a concrete list of food items, including the necessary amounts for each hypothetical household.
- (3)
- For the third milestone, three different focus groups were organized in the capital city. Several focus group trainings were organized and instructions were developed by the coordinating team to make sure that the focus groups were conducted and analysed in a standardized way (cf. Annex 1 in [26]). The national partners recruited for each focus group 5–11 participants of active age (30–50), through a questionnaire for recruitment ensuring a mix of different family situations, and a variety of socio-economic backgrounds. Involving people with different backgrounds increases the variation of opinions, the quality of discussions (in terms of argumentation) and validity of the outcome [27,28,29]. The recruitment of different socio-economic backgrounds was measured based on three variables: activity status, level of education and burden of housing costs as a proxy for income. Because of the limited number of focus groups, it was difficult to make sure ethnic minorities were equally involved. Therefore, this pilot project aimed in the first place at capturing the dominant cultural patterns through FG discussions, acknowledging that more research is necessary to reveal the cultural variety within cities.Each focus group followed a predefined topic list, with an estimated time of three hours. The first half of the discussion was devoted to evaluating the broader theoretical framework (the assessment of needs and essential social roles) and the underlying assumptions we made (characteristics of the reference family), and the second half was used to discuss the acceptability, feasibility and completeness of the food basket, the kitchen equipment and the other non-physical functions of food—as well as the related purchasing patterns. For the purpose of this article, we only make use of the second part of the focus group discussions, which had an average duration of approximately 90 min. To facilitate the discussion, an illustrative weekly menu was developed by the nutritionist, in accordance with the proposed food basket.The results were analysed by the country teams in accordance with a common template of analysis. Each focus group was recorded, and, during the discussion, an assistant wrote down the various arguments in a structured template. For each topic a final column was completed with the overall conclusions and general remarks on interaction processes, proxemics and paralinguistic information. In literature they call this a micro-interlocutor analysis [30], which allows to focus on the group as well as on the individual data while taking into account group dynamics. The purpose of the focus groups was not to decide on specific quantities but rather to assess the nature, the origin and the construction of the arguments regarding why items are needed or not and what is acceptable and feasible within a given socio-cultural context.
- (4)
- Next, the food baskets had to be adapted in function of feasibility and acceptability, based on the arguments put forward during focus group discussions. This was done in accordance with a common decision procedure that country teams had to follow to ensure that the healthy character of the diet was respected and to facilitate the consistency and robustness of the results across countries (cf. Annex 2 in [26]).
- (5)
- The last milestone consisted of estimating the minimum feasible cost of the food basket. Again, several common assumptions were made. First of all, the food budget should represent the minimum resources that people need to get access to all essential food items. Further, people should have a minimum acceptable degree of freedom in the choice of shops and products. Thirdly, market prices are used, unless other purchasing patterns are common practice, but no sales prices are used. Another important guideline was that economies of scale in buying and preparing food should be taken into account. For the choice of shops to buy food, the national teams had to choose a few retailors or markets which were suggested by the participants in the focus groups. The retailers had to meet the following criteria: (1) they offer a wide variety of food items of acceptable quality at low prices, (2) the shops are well spread over the city, (3) the shops are well accessible by public transport. Being well spread over the country was another criterion that could be considered, as this could facilitate the future pricing of reference budgets developed for other regions.All countries priced the food baskets between March and April 2015 (exceptions are the food baskets for Luxembourg, Denmark and Slovakia which were priced in December 2014, July 2015 and October 2015, respectively). Prices were collected on the basis of a small-scale survey, carried out by researchers from each country team, making use of a standardised excel sheet (with the exception of Luxembourg, where the country team had access to the official price survey). To price pre-packaged food, the lowest price of suitable products had to be chosen. With regard to fresh food and food categories which contain a large variety of products, country teams had to follow a specific predefined pricing procedure, such that a weighted price could be estimated which takes into account the available range of relevant products. The food categories for which a weighted price procedure had to be used are the following: fresh fruit, canned fruit, fruit puree, frozen fruit, dried fruit, fresh vegetables, frozen prepared & unprepared vegetables, canned vegetables, fresh fish, frozen fish, canned fish, lean meat, fat meat, charcuterie and cheese.For instance, the cost of fresh fruit is based on a weighted average of all fresh fruit available in the shop, taking from each type of fruit the cheapest alternative of sufficient quality (e.g., the cheapest apple, the cheapest pear, etc.). The cheapest products are weighted 5/7, whereas the average weight of the more expensive items is given a weight of 2/7, while discarding the 10% most expensive fruits. This procedure aims to meet the dual objective of identifying the minimum cost to prepare healthy menus that still offer sufficient variation (see Annex 3 in [26] for the detailed instructions for assessing the cost of the food basket).
3. Results
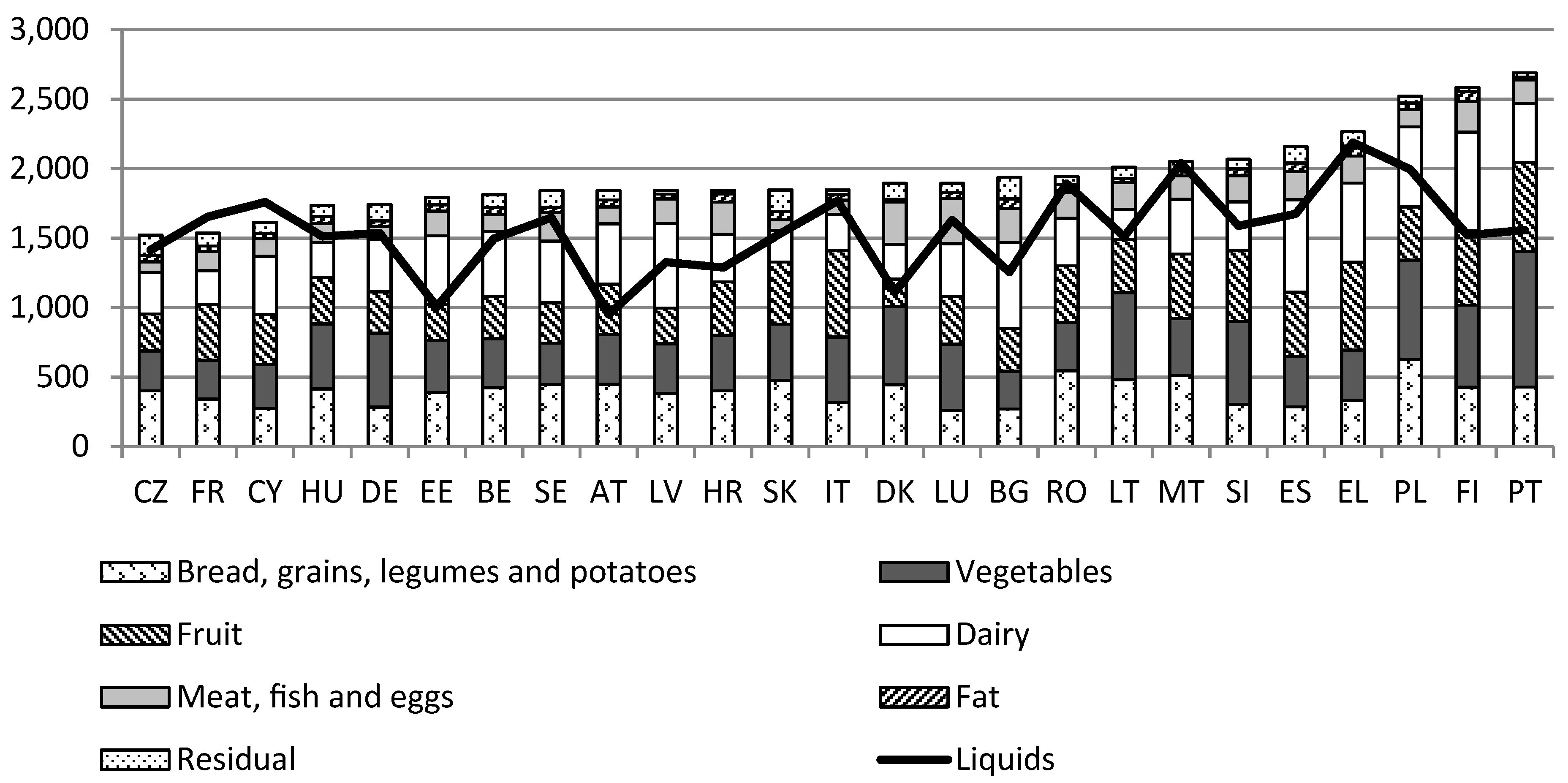
3.1. The Contents of the Food Basket
What Constitutes a Healthy Diet?
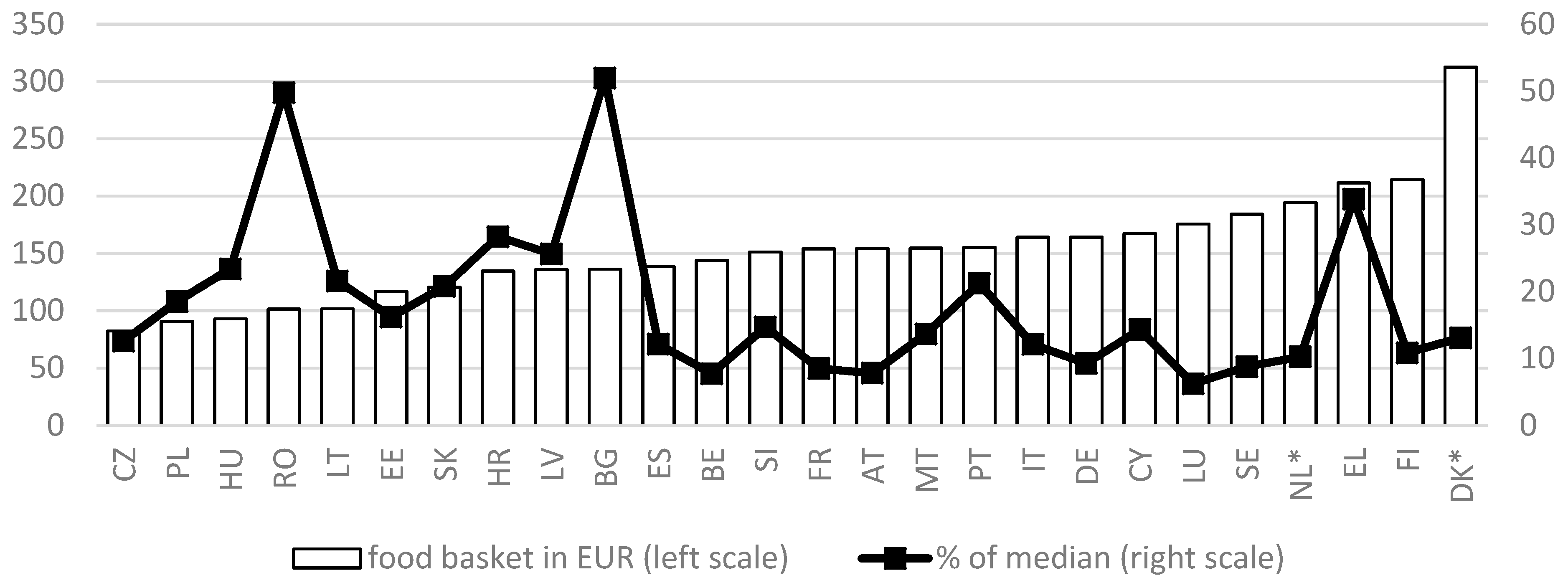
3.2. The Cost of the Food Baskets
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the global burden of disease study 2016. Lanct 2017. [Google Scholar] [CrossRef]
- Thomson, K.; Hillier-Brown, F.; Todd, A.; McNamara, C.; Huijts, T.; Bambra, C. The effects of public health policies on health inequalities in high-income countries: An umbrella review. BMC Public Health 2018, 18, 869. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2017. Monitoring Health for the SDGs; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- OECD. It Together: Why Less Inequality Benefits All; OECD Publishing: Paris, France, 2015. [Google Scholar]
- Brian, N. Inequality and Inclusive Growth in Rich Countries: Shared Challenges and Contrasting Fortunes; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Milanovic, B. Global Inequality. A New Approach for the Age of Globalization; Harvard University Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.-K.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. Lancet 2015, 385, 2400–2409. [Google Scholar] [CrossRef]
- Carrillo-Álvarez, E.; Riera-Romaní, J. Childhood obesity prevention: Does policy meet research? Evidence-based reflections upon the Spanish case. MOJ Public Heal. 2017, 6, 1–14. [Google Scholar] [CrossRef]
- Kumanyika, S.; Libman, K.; Garcia, A. Strategic Action to Combat the Obesity Epidemic. Available online: http://www.wish.org.qa/wp-content/uploads/2018/02/27425_WISH_Obesity_Report_web14.pdf (accessed on 14 December 2018).
- EFSA Panel on Dietetic Products, Nutrition, and Allergies (NDA). Scientific opinion on establishing food-based dietary guidelines. EFSA J. 2010, 8, 1–42. [Google Scholar] [CrossRef]
- FAO/WHO. Preparation and Use of Food-Based Dietary Guidelines; WHO: Nicosia, Cyprus, 1996. [Google Scholar]
- Stockley, L. Toward public health nutrition strategies in the European Union to implement food based dietary guidelines and to enhance healthier lifestyles. Public Health Nutr. 2001, 4, 307–324. [Google Scholar] [CrossRef] [PubMed]
- Roth, N.; Knai, C. Food Based Dietary Guidelines in the Who European Region; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- WHO. Global Status Report on Noncommunicable Diseases 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Pomerleau, J.; McKee, M.; Lobstein, T.; Knai, C. The burden of disease attributable to nutrition in Europe. Public Health Nutr. 2003, 6, 453–461. [Google Scholar] [CrossRef]
- Naska, A.; Fouskakis, D.; Oikonomou, E.; Almeida, M.; Berg, M.; Gedrich, K.; Moreiras, O.; Nelson, M.; Trygg, K.; Turrini, A.; et al. Dietary patterns and their socio-demographic determinants in 10 European countries: Data from the DAFNE databank. Eur. J. Clin. Nutr. 2006, 60, 181–190. [Google Scholar] [CrossRef]
- Gibney, M.; Sandstrom, B. A framework for food-based dietary guidelines in the European Union. Public Health Nutr. 2000, 4, 293–305. [Google Scholar] [CrossRef]
- European Food Information Council Food Based Dietary Guidelines in Europe. Available online: www.eufic.org/en/healthy-living/article/food-based-dietary-guidelines-in-europe (accessed on 14 December 2018).
- Montagnese, C.; Santarpia, L.; Buonifacio, M.; Nardelli, A.; Caldara, A.R.; Silvestri, E.; Contaldo, F.; Pasanisi, F. European food-based dietary guidelines: A comparison and update. Nutrition 2015, 31, 908–915. [Google Scholar] [CrossRef]
- Brown, K.A.; Timotijevic, L.; Barnett, J.; Shepherd, R.; Lähteenmäki, L.; Raats, M.M. A review of consumer awareness, understanding and use of food-based dietary guidelines. Br. J. Nutr. 2011, 106, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drewnowski, A.; Eichelsdoerfer, P. Can low-income Americans afford a healthy diet? Nutr. Today 2010, 44, 246–249. [Google Scholar] [CrossRef] [PubMed]
- Schönfeldt, H.C.; Hall, N.; Bester, M. Relevance of food-based dietary guidelines to food and nutrition security: A South African perspective. Nutr. Bull. 2013, 38, 226–235. [Google Scholar] [CrossRef]
- Poulain, J.-P. The Sociology of Food: Eating and the Place of Food in Society; Bloomsbury: New York, NY, USA; ISBN 9781472586209.
- Chrysostomou, S.; Andreou, S.N.; Polycarpou, A. Developing a food basket for fulfilling physical and non-physical needs in Cyprus. Is it affordable? Eur. J. Public Health 2017, 27, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Carrillo Álvarez, E.; Cussó-Parcerisas, I.; Riera-Romaní, J. Development of the Spanish Healthy Food Reference Budget for an adequate social participation at the minimum. Public Health Nutr. 2016, 19. [Google Scholar] [CrossRef] [PubMed]
- Goedemé, T.; Storms, B.; Penne, T.; Van den Bosch, K. Pilot Project for the Development of a Common Methodology on Reference Budgets in Europe. Final Report; European Commission: Antwerp, Belgium, 2015; ISBN 9789279540912. [Google Scholar]
- Deeming, C. The historical development of family budget standards in britafrom the 17th century to the present. Soc. Policy Adm. 2010. [Google Scholar] [CrossRef]
- Vranken, J. Using Reference Budgets for Drawing up the Requirements of a Minimum Income Scheme and Assessing Adequacy. Available online: https://ec.europa.eu/social/main.jsp?catId=1024&langId=en&newsId=1392&moreDocuments=yes&tableName=news (accessed on 14 December 2018).
- Devuyst, K.; Storms, B.; Penne, T. Methodologische Keuzes Bij De Ontwikkeling Van Referentiebudgetten: Welke Rol Voor Focusgroepen? Aromede: Antwerp, Belgium, 2014. [Google Scholar]
- Onwuegbuzie, A.J.; Dickinson, W.B.; Leech, N.L.; Zoran, A.G. A Qualitative Framework for Collecting and Analyzing Data in Focus Group Research. Int. J. Qual. Methods 2009. [Google Scholar] [CrossRef]
- Gezondheidsraad, H. Maten en Gewichten: Handleiding Voor Een Gestandaardiseerde Kwantificering Van Voedingsmiddelen [Measures and Weights: Manual for Standardized Quantification of Foods]; Belgische Hoge Gezondheidsraad: Brussels, Belgium, 2005. [Google Scholar]
- Atkinson, T.; Guio, A.C.; Marlier, E. Monitoring Social Inclusion in Europe. Available online: https://ec.europa.eu/eurostat/web/income-and-living-conditions/publications/-/asset_publisher/zdEOYZhr9af3/content/KS-05-14-075/3217494?inheritRedirect=false (accessed on 14 December 2018).
- Storms, B.; Goedemé, T.; Van den Bosch, K.; Penne, T.; Schuerman, N.; Stockman, S. Pilot Project for a Development of a Common Methodology on Reference Budgets in Europe. Review of Current State of Play on Reference Budget Practices at National, Regional and Local Level. Available online: http://www.referencebudgets.eu/ (accessed on 25 July 2014).
- Sobal, J.; Bisogni, C.A. Constructing food choice decisions. Ann. Behav. Med. 2009, 38, 37–46. [Google Scholar] [CrossRef]
- Leng, G.; Adan, R.A.H.; Belot, M.; Brunstrom, J.M.; de Graaf, K.; Dickson, S.L.; Hare, T.; Maier, S.; Menzies, J.; Preissl, H.; et al. The determinants of food choice. Proc. Nutr. Soc. 2017, 76, 316–327. [Google Scholar] [CrossRef]
- Antentas, J.M.; Vivas, E. Impacto de la crisis en el derecho a una alimentación sana y saludable. Informe SESPAS 2014. Gac. Sanit. 2014, 28, 58–61. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, A.; Aggarwal, A.; Tang, W.; Drewnowski, A. Cooking at home: A strategy to comply with U.S. Dietary guidelines at no extra cost. Am. J. Prev. Med. 2017, 52, 616–624. [Google Scholar] [CrossRef] [PubMed]
- Cornellis, I.; Vandervoort, B. Een Hele Dag Lekker en Gezond Eten Voor 5 Euros; Borgerhoff & Lamberigst: Ghent, Belgium, 2013. [Google Scholar]
- Muro, P.; Carrillo-Álvarez, E.; Marzo, T. Empoderar en hábitos saludables a familias vulnerables. In REPS 2018: Políticas sociales ante horizones de incertidumbre y desigualdad; Red Española de Política Social: Zaragoza, Spain, 2018. [Google Scholar]
- Carrillo-Álvarez, E.; Boeckx, H.; Penne, T.; Palma, I.; Goedemé, T.; Storms, B. Promoting healthy eating in Europe: A comparison of European countries FBDG. 2019. In press. [Google Scholar]
- Sainz García, P.; Carmen Ferrer Svoboda, M.; Sánchez Ruiz, E.; Pedro Sainz García, C. Competencias culinarias y consumo de alimentos procesados o preparados en estudiantes universitarios de barcelona. Rev. Esp. Salud. Pública 2016, 90, 1–13. [Google Scholar]
- Eurostat Eurostat Online Database. Available online: https://ec.europa.eu/eurostat/data/database (accessed on 14 December 2018).


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carrillo-Álvarez, E.; Penne, T.; Boeckx, H.; Storms, B.; Goedemé, T. Food Reference Budgets as a Potential Policy Tool to Address Food Insecurity: Lessons Learned from a Pilot Study in 26 European Countries. Int. J. Environ. Res. Public Health 2019, 16, 32. https://doi.org/10.3390/ijerph16010032
Carrillo-Álvarez E, Penne T, Boeckx H, Storms B, Goedemé T. Food Reference Budgets as a Potential Policy Tool to Address Food Insecurity: Lessons Learned from a Pilot Study in 26 European Countries. International Journal of Environmental Research and Public Health. 2019; 16(1):32. https://doi.org/10.3390/ijerph16010032
Chicago/Turabian StyleCarrillo-Álvarez, Elena, Tess Penne, Hilde Boeckx, Bérénice Storms, and Tim Goedemé. 2019. "Food Reference Budgets as a Potential Policy Tool to Address Food Insecurity: Lessons Learned from a Pilot Study in 26 European Countries" International Journal of Environmental Research and Public Health 16, no. 1: 32. https://doi.org/10.3390/ijerph16010032
APA StyleCarrillo-Álvarez, E., Penne, T., Boeckx, H., Storms, B., & Goedemé, T. (2019). Food Reference Budgets as a Potential Policy Tool to Address Food Insecurity: Lessons Learned from a Pilot Study in 26 European Countries. International Journal of Environmental Research and Public Health, 16(1), 32. https://doi.org/10.3390/ijerph16010032