From Complex Interventions to Complex Systems: Using Social Network Analysis to Understand School Engagement with Health and Wellbeing


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Ethical Approval
2.3. Case Study Sampling
2.4. Case Study Schools’ Engagement with the School Health Research Network
2.5. The Embeddedness of Health Improvement within Case Study Schools
2.6. Social Network Analysis with Wellbeing Leads
2.7. Qualitative Interviews with Wellbeing Leads and Other School Staff
2.8. Qualitative Interview Analysis
3. Results
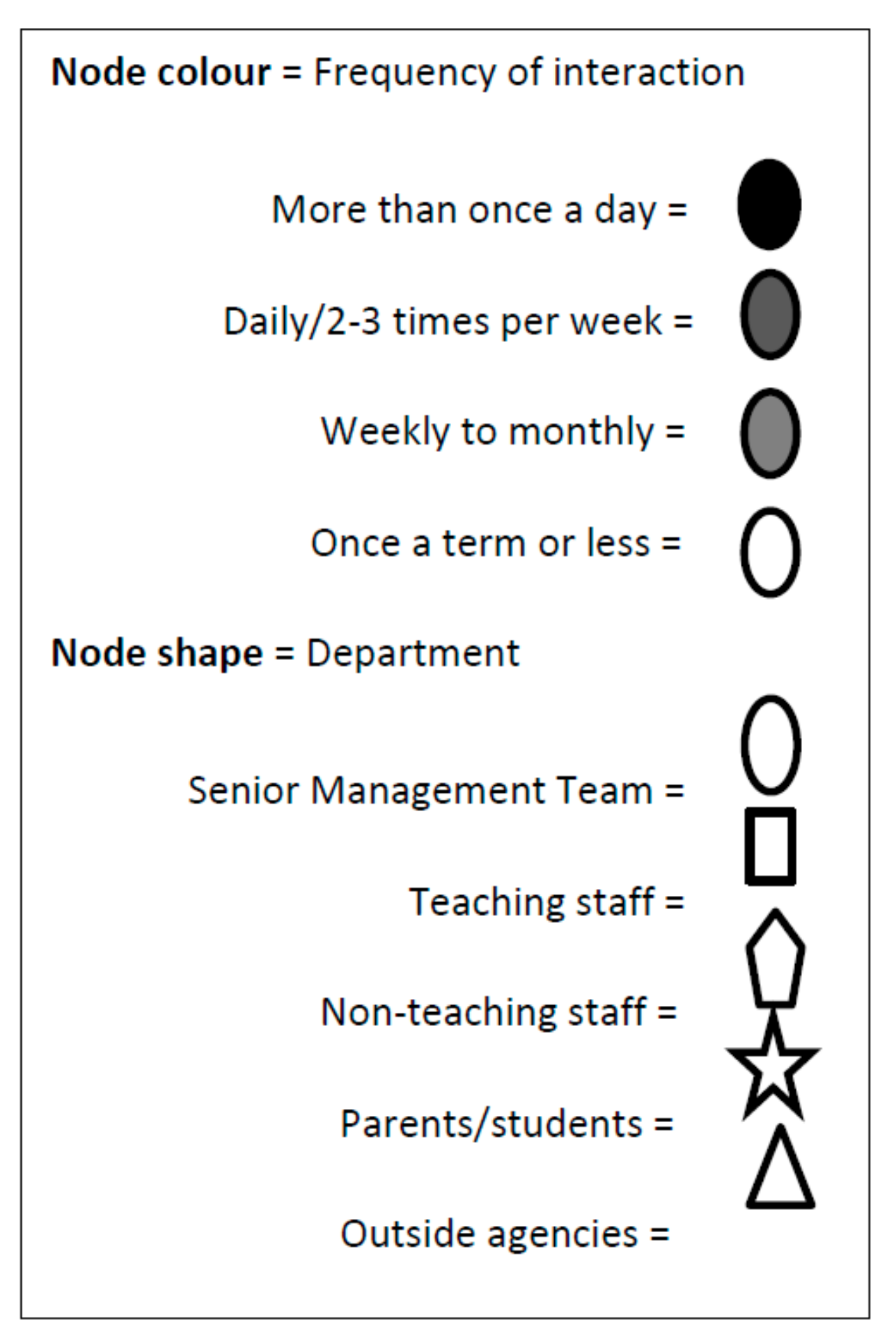
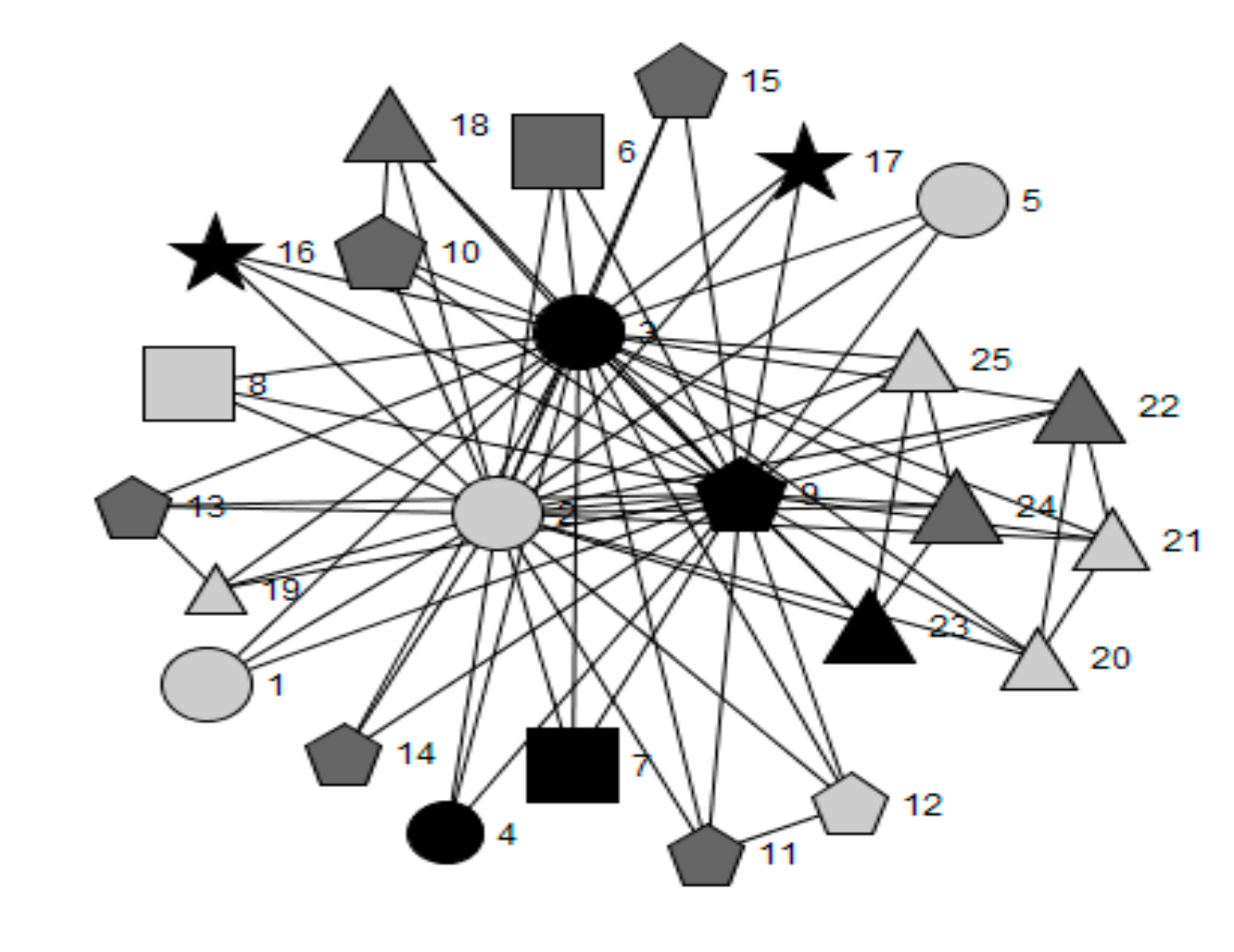
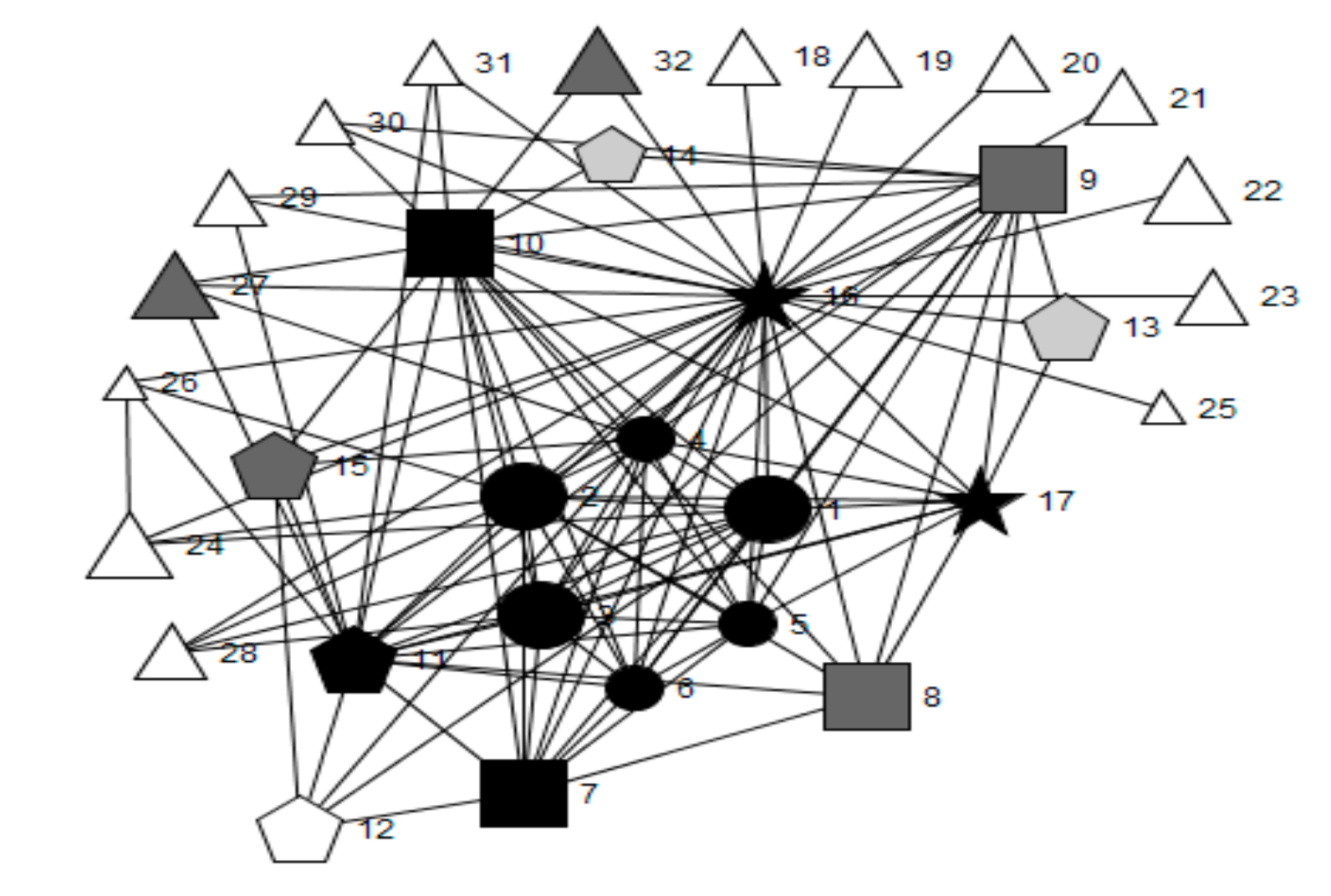
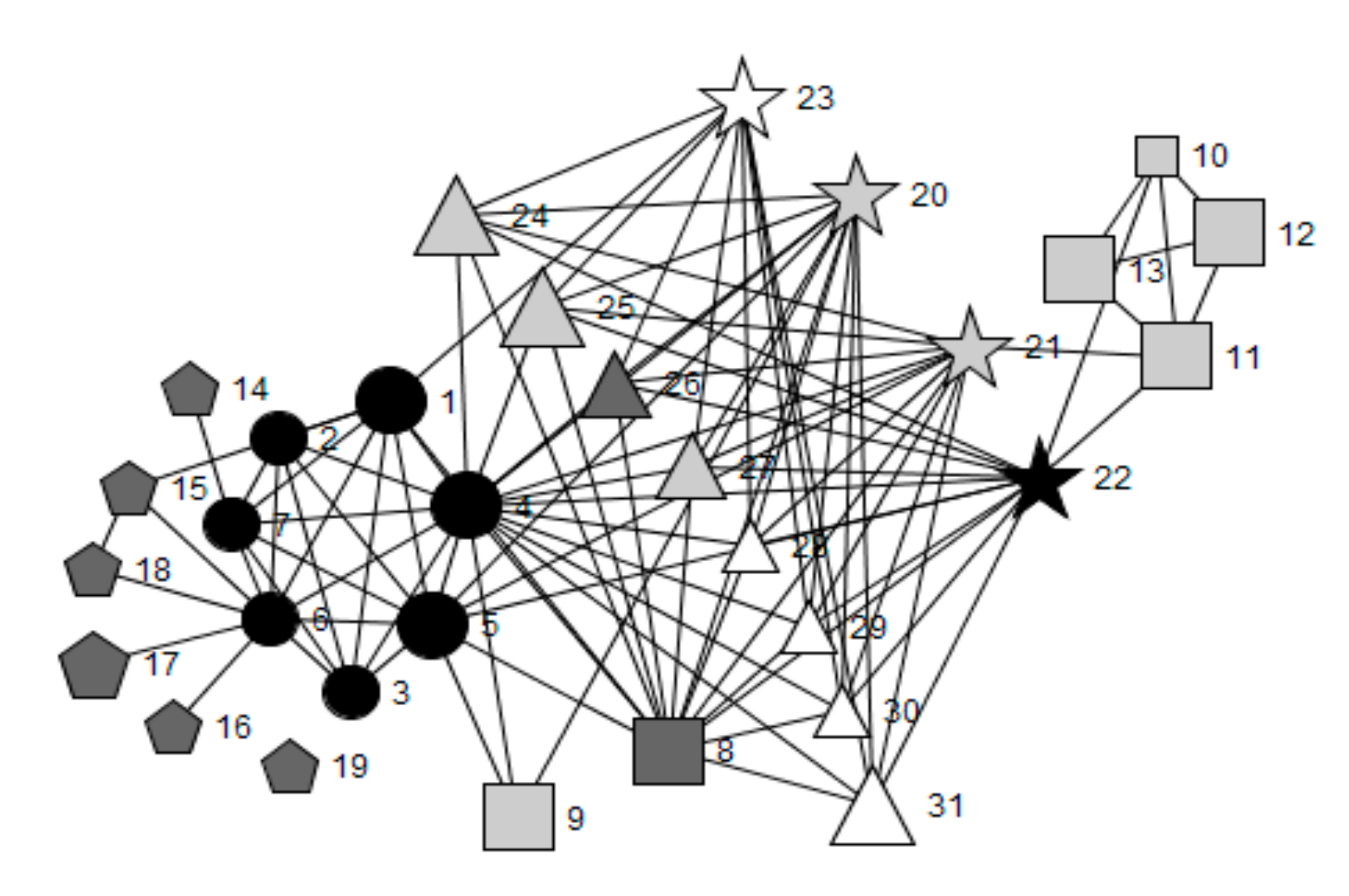
3.1. Social Networks of Wellbeing Leads in Case Study Schools
3.1.1. Influential Champions for Health: Characteristics and Position within Social Networks
3.1.2. Frequency of Health and Wellbeing-Related Interactions and Their Importance Ratings
3.2. Qualitative Perceptions of the Broader Context Surrounding Health and Wellbeing in Case Study Schools
3.2.1. Perceptions of the Allocation of Responsibility for Leading Health and Wellbeing
“I think having [name] who is the deputy head and our Inclusion and Wellbeing Officer, the fact that that’s from that level at the senior management level. She drives this wellbeing ethos in our school (…)”Oakwood School, school nurse
“The wellbeing lead has to be part of the Senior Management Team because the wellbeing lead could never ever just be a middle manager because huge decisions have to be made and it’s got to be pushed right from the top down (…)”Oakwood School, wellbeing lead
“(…) generally if someone is saying ‘this is a good thing to do’ then it’s more likely to have an impact if it’s someone in the Senior Management Team, than it is if it’s someone who is just an ordinary teacher, generally.”Greenfield, Healthy Schools Coordinator
“(…) even for myself as a head of department it’s easy for me to make sure things are in place in my department, but if I go out of my department to say ‘Oh can you do this, can you do that’, it’s very, it’s difficult (…)”Woodlands School, head of science and student voice
“ (…) it would be beneficial to have one person without all these other jobs to see to, to be you know solely dedicated, that would obviously (…) be a positive, you know?”Highbridge school, teaching assistant
“(…) So I think it’s actually a real positive of where it’s sat at the moment (…) in line with heads of departments as well because and because it becomes that person’s primary driver and therefore it probably has more effects than it being part of wider job brief higher up I think.”Greenfield School, assistant head for PSE
3.2.2. Wider Leadership Models
“Absolutely, I couldn’t do my job if it wasn’t for the fact that I had a member of senior team who, sometimes she will say, ‘I don’t necessarily understand, but go for it’, or she hasn’t necessarily got the time because of her other, the other demands of her job. But I know I have her support, and I know that she trusts me and she will back me up.”Oakwood School, PSE teacher
“Obviously the head teacher is a very busy man. I do speak to him if there’s something like when we had our Healthy Schools Assessment, obviously I spoke to him and if there’s something I usually I wouldn’t necessarily (…). It would be good to have a specific, like allocated time for that maybe but, I don’t think that’s going to happen, but it would be good (…)”Greenfield School, wellbeing lead
“we’ve got some heavy demands on pastoral care within the school so we’ve got a dedicated team for each year group which includes a pastoral support assistant who’ll look out for the health and wellbeing of each child in their year group.”Highbridge School, wellbeing lead
“certainly a network within school primarily because I feel overwhelmed. I do feel overwhelmed. I’ve got great colleagues but everybody’s so busy and everybody’s got their own job descriptions, their own priorities and even within my own role it falls into a pocket sometimes and it’s not, it hasn’t got the priority on a day to day basis (…)”Woodlands school, wellbeing lead
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bonell, C.; Farah, J.; Harden, A.; Wells, H.; Parry, W.; Fletcher, A.; Petticrew, M.; Thomas, J.; Whitehead, M.; Campbell, R.; et al. Systematic Review of the Effects of Schools and School Environment Interventions on Health: Evidence Mapping and Synthesis. Publlic Health Res. 2013, 1, 1–320. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ottawa Charter for Health Promotion: An International Conference on Health Promotion—The Move Towards A New Public Health, Nov. 17–21, Ottawa; World Health Organization: Geneva, Switzerland, 1986. [Google Scholar]
- Dierker, L.; Hedeker, D.; Rose, J.; Selya, A.; Mermelstein, R. Early Emerging Nicotine Dependence Symptoms in Adolescence Predict Daily Smoking in Young Adulthood. Drug Alcohol Depend. 2015, 151, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Kvaavik, E.; Tell, G.S.; Klepp, K.-I. Predictors and Tracking of Body Mass Index from Adolescence into Adulthood: Follow-Up of 18 to 20 Years in the Oslo Youth Study. Arch. Pediatr. Adolesc. Med. 2003, 157, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Littlecott, H.; Moore, G.; Murphy, S. Student Health and Well-Being in Secondary Schools: The Role of School Support Staff Alongside Teaching Staff. Pastor. Care Educ. 2018, 36, 297–312. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.P.; Jones, H.E.; Pouliou, T.; Murphy, S.M.; Waters, E. The WHO Health Promoting School Framework for Improving the Health and Well-Being of Students and Their Academic Achievement. Cochrane Database Syst. Rev. 2014, 16, CD008958. [Google Scholar] [CrossRef] [PubMed]
- Langford, R.; Bonell, C.; Jones, H.; Campbell, R. Obesity Prevention and the Health Promoting Schools Framework: Essential Components and Barriers to Success. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P. Lessons from Complex Interventions to Improve Health. Annu. Rev. Public Health 2015, 36, 307. [Google Scholar] [CrossRef] [PubMed]
- Thompson, B.; Coronado, G.; Snipes, S.A.; Puschel, K. Methodologic Advances and Ongoing Challenges in Designing Community-Based Health Promotion Programs. Annu. Rev. Public Health 2003, 24, 315–340. [Google Scholar] [CrossRef] [PubMed]
- Hawe, P.; Shiell, A.; Riley, T. Theorising Interventions as Events in Systems. Am. J. Community Psychol. 2009, 43, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Keshavarz, N.; Nutbeam, D.; Rowling, L.; Khavarpour, F. Schools as Social Complex Adaptive Systems: A New Way to Understand the Challenges of Introducing the Health Promoting Schools Concept. Soc. Sci. Med. 2010, 70, 1467–1474. [Google Scholar] [CrossRef]
- Burt, R.S. Structural Holes and Good Ideas. Am. J. Sociol. 2004, 110, 349–399. [Google Scholar] [CrossRef]
- Hawe, P.; Bond, L.; Ghali, L.M.; Perry, R.; Davison, C.M.; Casey, D.M.; Butler, H.; Webster, C.M.; Scholz, B. Replication of a Whole School Ethos-Changing Intervention: Different Context, Similar Effects, Additional Insights. BMC Public Health 2015, 15, 265. [Google Scholar] [CrossRef]
- Moore, G.; Evans, R.E.; Hawkins, J.; Littlecott, H.J.; Melendez-Torres, G.J.; Bonell, C.; Murphy, S. From Complex Social Interventions to Interventions in Complex Social Systems: Future Directions and Unresolved Questions for Intervention Development and Evaluation. Evaluation 2019, 25, 23–45. [Google Scholar] [CrossRef]
- Murphy, S.; Littlecott, H.J.; Hewitt, G.; MacDonald, S.; Roberts, J.; Bishop, J.; Roberts, C.; Thurston, R.; Bishop, A.; Moore, L.; et al. A Transdisciplinary Complex Adaptive Systems (T-CAS) Approach to Developing a National School-Based Culture of Prevention for Health Improvement: The School Health Research Network (SHRN) in Wales. Prev. Sci. 2018, 25, 23–45. [Google Scholar] [CrossRef]
- Rutter, H.; Savona, N.; Glonti, K.; Bibby, J.; Cummins, S.; Finegood, D.T. The Need for a Complex Systems Model of Evidence for Public Health. Lancet 2017, 390, 2602–2604. [Google Scholar] [CrossRef]
- Badham, J.; Chattoe-Brown, E.; Gilbert, N.; Chalabi, Z.; Zee, F.; Hunter, R.F. Developing Agent-Based Models of Complex Behaviour. Health Place 2018, 54, 170–177. [Google Scholar] [CrossRef]
- Minary, L.; Alla, F.; Cambon, L.; Kivits, J.; Potvin, L. Addressing Complexity in Population Health Intervention Research: The Context/Intervention Interface. J. Epidemiol. Community Health 2018, 72, 319–323. [Google Scholar] [CrossRef]
- Roberts-Gray, C.; Gingiss, P.M.; Boerm, M. Evaluating School Capacity to Implement New Programs. Eval. Program Plan 2007, 30, 247–257. [Google Scholar] [CrossRef]
- Van Der Poel, M.G.M. Delineating Personal Support Networks. Soc. Netw. 1993, 15, 49–70. [Google Scholar] [CrossRef]
- Moolenaar, N.M. A Social Network Perspective on Teacher Collaboration in Schools: Theory, Methodology, and Applications. Am. J. Educ. 2012, 119, 7–39. [Google Scholar] [CrossRef]
- Hawe, P.; Ghali, L. Use of Social Network Analysis to Map the Social Relationships of Staff and Teachers at School. Health Educ. Res. 2008, 23, 62–69. [Google Scholar] [CrossRef]
- Marks, J.; Barnett, L.M.; Foulkes, C.; Hawe, P.; Allender, S. Using Social Network Analysis to Identify Key Child Care Center Staff for Obesity Prevention Interventions: A Pilot Study. J. Obes. 2013, 2013, 1–9. [Google Scholar] [CrossRef]
- Laumann, E.O.; Marsden, P.V.; Prensky, D. The Boundary Specification Problem in Network Analysis. Res. Methods Soc. Netw. Anal. 1989, 61, 87. [Google Scholar]
- Teutsch, F.; Gugglberger, L.; Dür, W. School Health Promotion Providers’ Roles in Practice and Theory: Results from a Case Study. Health Policy 2015, 119, 82–87. [Google Scholar] [CrossRef]
- Coburn, C.E.; Russell, J.L. District Policy and Teachers’ Social Networks. Educ. Eval. Policy Anal. 2008, 30, 203–235. [Google Scholar] [CrossRef]
- Carmichael, P.; Fox, A.; McCormick, R.; Procter, R.; Honour, L. Teachers’ Networks in and out of School. Res. Pap. Educ. 2006, 21, 217–234. [Google Scholar] [CrossRef]
- Storey, K.E.; Spitters, H.; Cunningham, C.; Schwartz, M.; Veugelers, P.J. Implementing Comprehensive School Health: Teachers’ Perceptions of the Alberta Project Promoting Active Living and Healthy Eating in Schools-APPLE Schools. Available online: http://ojs.acadiau.ca/index.php/phenex/article/view/1422 (accessed on 13 May 2019).
- Schwartz, M.; Karunamuni, N.D.; Veugelers, P.J. Tailoring and Implementing Comprehensive School Health: The Alberta Project Promoting Active Living and Healthy Eating in Schools. Available online: http://ojs.acadiau.ca/index.php/phenex/article/view/56 (accessed on 13 May 2019).
- Hogan, B.; Carrasco, J.A.; Wellman, B. Visualizing Personal Networks: Working with Participant-Aided Sociograms. Field Method 2007, 19, 116–144. [Google Scholar] [CrossRef]
- Hewitt, G.; Roberts, J.; Fletcher, A.; Moore, G.; Murphy, S. Improving Young People’s Health and Wellbeing Through a School Health Research Network: Reflections on School-Researcher Engagement at the National Level. Res. All 2018, 2, 16–33. [Google Scholar] [CrossRef]
- Welsh Government. Available online: https://gov.wales/welsh-index-multiple-deprivation-full-index-update-ranks-2014 (accessed on 2 May 2019).
- Public Health Network Cymru. Available online: https://www.publichealthnetwork.cymru/en/social-determinants/education/welsh-network-of-healthy-school-schemes-wnhss/ (accessed on 2 May 2019).
- Robins, G. Doing Social Network Research: Network-Based Research Design for Social Scientists; Sage Publications: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Borgatti, S.P. Centrality and Network Flow. Soc. Netw. 2005, 27, 55–71. [Google Scholar] [CrossRef]
- Nohria, N.; Eccles, R.G. The Social Stucture of Competition. Networks and Organizations: Structure, Form, and Action; Harvard Business School Press: Boston, MA, USA, 1992. [Google Scholar]
- Wasserman, S.; Faust, K. Social Network Analysis: Methods and Applications; Cambridge University Press: Cambridge, UK, 1994. [Google Scholar]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Newman, M.E.J.; Park, J. Why Social Networks are Different from Other Types of networks. Phys. Rev. 2003, 68, 036122. [Google Scholar] [CrossRef]
- Granovetter, M.S. The Strength of Weak Ties. Am. J. Sociol. 1973, 78, 1360–1380. [Google Scholar] [CrossRef]
- Provan, K.G.; Sebastian, J.G. Networks within Networks: Service Link Overlap, Organizational Cliques, and Network Effectiveness. Acad. Manag. J. 1998, 41, 453–463. [Google Scholar] [CrossRef]
- Harris, A. Distributed Leadership and School Improvement Leading or Misleading? Educ. Manag. Adm. Leadersh. 2004, 32, 11–24. [Google Scholar] [CrossRef]
- Hulpia, H.; Devos, G.; Rosseel, Y. The Relationship between the Perception of Distributed Leadership in Secondary Schools and Teachers’ and Teacher Leaders’ Job Satisfaction and Organizational Commitment. Sch. Eff. Sch. Improv. 2009, 20, 291–317. [Google Scholar] [CrossRef]
- Hite, J.M.; Reynolds, B.; Hite, S.J. Who Ya Gonna Call? Networks of Rural School Administrators. Rural Educ. 2010, 32, 11–28. [Google Scholar]
- Timperley, H.S. Distributed Leadership: Developing Theory from Practice. J. Curric. Stud. 2005, 37, 395–420. [Google Scholar] [CrossRef]
- Sharples, J. Developing an Evidence-Informed Support Service for Schools—Reflections on a UK Model. Evid. Policy 2015, 11, 577–587. [Google Scholar] [CrossRef]
- Inchley, J.; Muldoon, J.; Currie, C. Becoming a Health Promoting School: Evaluating the Process of Effective Implementation in Scotland. Health Promot. Int. 2007, 22, 65–71. [Google Scholar] [CrossRef]
- Moore, G.F.; Littlecott, H.J.; Fletcher, A.; Hewitt, G.; Murphy, S. Variations in Schools’ Commitment to Health and Implementation of Health Improvement Activities: A Cross-Sectional Study of Secondary Schools in Wales. BMC Public Health 2016, 16, 138. [Google Scholar] [CrossRef]
- Harper, D. Talking about Pictures: A Case for Photo Elicitation. Vis. Stud. 2002, 17, 13–26. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Data Source | Date | Participants | Uses |
| Data usage survey | September 2014–June 2015 | Wellbeing Leads within 4 case study schools. | To derive contextual measures of school engagement with pupil-level feedback from the School Health Research Network. |
| Ego Network Analysis | October 2014–April 2015 | Wellbeing leads within 4 case study schools. | To measure the characteristics of wellbeing leads’ health and wellbeing networks, and the position of key change agents within this. |
| Semi-structured qualitative interviews | October 2014–April 2015 | 4 case study schools (wellbeing leads, members of staff, members of staff and a healthy schools Coordinator at differing positions in the wellbeing leads’ ego-networks. | To explore stakeholder perceptions of wellbeing leads’ health and wellbeing networks, and the position of key change agents within this. |
| School Environment Questionnaire | March–May 2016 | A representative (Wellbeing Lead or a member of senior leadership) from each case study school. | To derive contextual measures of embeddedness of health improvement within case study schools aligned with three topics within the Health Promoting Schools Scheme [2]: Curriculum, environment (measured by a number of policies related to health) and parental involvement. |
| School | No. of Students | Welsh Index of Multiple Deprivation Score (Low Score = Highest Deprivation) * | Geographic Location ** | Stage of Health Promoting Schools Scheme *** | Characteristics of Wellbeing Lead | Engagement with the School Health Research Network (Ranking 1–4) **** | Embeddedness of Health Improvement in the School (Out of 3) ***** |
|---|---|---|---|---|---|---|---|
| Greenfield | <900 | Highest 10% (affluent) | Rural | National Quality Award (highest accolade) | Female PE Teacher, aged 26–35 years | 4 | 1.66 (rank 3) |
| Woodlands | >1200 | Around median | Welsh Valleys | Stage 1 | Female Assistant Head Teacher, aged 46–55 years | 3 | 1.83 (rank 2) |
| Highbridge | <700 | Lowest 10% (deprived) | Urban | National Quality Award | Female Deputy Head, aged 46–55 years | 1 | 2.43 (rank 1) |
| Oakwood | >1000 | Highest 10% (affluent) | Urban | Stage 3 | Female Deputy Head, aged 46–55 years | 2 | 1.34 (rank 4) |
| Greenfield School | Woodlands School | Highbridge School | Oakwood School | ||
|---|---|---|---|---|---|
| Wellbeing Lead | Role | PE Teacher | Assistant Head Teacher | Deputy Head Teacher | Deputy Head Teacher |
| Age group | 26–35 | 46–55 | 46–55 | 46–55 | |
| Gender | Female | Female | Female | Female | |
| Interviewee 2 | Role | Assistant Head for PSE | Food Technology Teacher | Wellbeing Manager | School Nurse |
| Age group | 36–45 | 26–35 | 36–45 | 46–55 | |
| Gender | Male | Female | Female | Female | |
| Interviewee 3 | Role | Healthy Schools Coordinator | PE Teacher | Behaviour Support Officer | Head of PSE |
| Age group | 26–35 | 26–35 | 36–45 | 36–45 | |
| Gender | Female | Female | Female | Female | |
| Interviewee 4 | Role | Food Technology Teacher | Head of Science and Student Voice | Teaching Assistant | Senior Learning Support Officer |
| Age group | 36–45 | 26–35 | 36–45 | 46–55 | |
| Gender | Female | Female | Female | Female | |
| Interviewee 5 | Role | Student Support Manager | |||
| Age group | 46–55 | ||||
| Gender | Female | ||||
| Betweenness Centrality | Highest Scores | |
|---|---|---|
| Greenfield School | 1 | Assistant Head (Wellbeing and Safeguarding) (98) |
| 2 | Assistant Head (PSE Line Manager) (71) | |
| 3 | Student Support Team (LSAs) (27) | |
| 4 | Learning and Wellbeing Department Manager (26) | |
| =5 | Head of PE, Parent-student Support and Head of Student Support (17) | |
| Woodlands School | 1 | Assistant Head 3 (126) |
| 2 | Deputy Head 1 (87) | |
| 3 | All year groups (74) | |
| 4 | Assistant Head 4 (45) | |
| 5 | Girls’ PE Teacher (36) | |
| Highbridge School | =1 | Head Teacher (74) |
| =1 | Safeguarding Officer (74) | |
| =1 | Wellbeing Manager (74) | |
| =2 | All other alters (0) | |
| Oakwood School | 1 | Heads of Year (23) |
| 2 | School Nurse (20) | |
| 3 | Additional Learning Needs Coordinator (15) | |
| 4 | Deputy Head (10) | |
| 5 | Head Teacher (7) | |
| Alter Attribute | Greenfield School | Woodlands School | Highbridge School | Oakwood School | |
|---|---|---|---|---|---|
| Frequency of interaction between alters and ego | More than once a day | 4/20 (20.0%) | 8/31 (25.8%) | 7/25 (28.0%) | 11/32 (34.4%) |
| Daily to 2–3 times a week | 4/20 (20.0%) | 8/31 (25.8%) | 9/25 (36.0%) | 5/32 (15.6%) | |
| Weekly-monthly | 8/20 (40.0%) | 10/31 (32.3%) | 9/25 (36.0%) | 2/32 (6.3%) | |
| Once a term or less | 3/20 (15.0%) | 5/31 (16.1%) | 0/25 (0.0%) | 3/32 (9.4%) | |
| Unknown | 1/20 (5.0%) | 0/31 (0.0%) | 0/25 (0.0%) | 1/32 (3.1%) | |
| Importance | Not important | 3/20 (15.0%) | 1/31 (3.2%) | 1/25 (4.0%) | 2/32 (6.3%) |
| Important | 5/20 (25.0%) | 12/31 (38.7%) | 1/25 (4.0%) | 5/32 (15.6%) | |
| Very important | 7/20 (35.0%) | 11/31 (35.5%) | 8/25 (32.0%) | 8/32 (25.0%) | |
| Extremely important | 5/20 (25.0%) | 7/31 (22.6%) | 15/25 (60.0%) | 17/32 (53.1%) | |
| Attribute | Senior Leadership Team | Teaching Staff | Non-Teaching Staff | Parents and Students | Outside Agencies | |
|---|---|---|---|---|---|---|
| Frequency of interaction >2–3 times per week | Greenfield School | 2/2 (100.0%) | 3/7 (42.9%) | 3/5 (60.0%) | 0/3 (0.0%) | 0/3 (0.0%) |
| Woodlands School | 7/7 (100.0%) | 1/5 (20.0%) | 7/7 (100.0%) | 1/4 (25.0%) | 1/8 (12.5%) | |
| Highbridge School | 2/5 (40.0%) | 2/3 (66.6%) | 6/7 (85.7%) | 2/2 (100.0%) | 4/8 (50.0%) | |
| Oakwood School | 6/6 (100.0%) | 4/4 (100.0%) | 2/5 (40.0%) | 2/2 (100.0%) | 2/15 (13.3%) | |
| Interactions rated as extremely important | Greenfield School | 2/2 (100.0%) | 1/7 (14.3%) | 1/5 (20.0%) | 0/3 (0.0%) | 1/3 (33.3%) |
| Woodlands School | 0/7 (0.0%) | 0/10 (0.0%) | 0/6 (0.0%) | 4/4 (100.0%) | 3/8 (37.5%) | |
| Highbridge School | 4/5 (80.0%) | 3/3 (100.0%) | 2/7 (28.6%) | 2/2 (100.0%) | 4/8 (50.0%) | |
| Oakwood School | 3/6 (50.0%) | 4/4 (100.0%) | 4/5 (80.0%) | 2/2 (100.0%) | 4/15 (26.7%) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Littlecott, H.J.; Moore, G.F.; Gallagher, H.C.; Murphy, S. From Complex Interventions to Complex Systems: Using Social Network Analysis to Understand School Engagement with Health and Wellbeing. Int. J. Environ. Res. Public Health 2019, 16, 1694. https://doi.org/10.3390/ijerph16101694
Littlecott HJ, Moore GF, Gallagher HC, Murphy S. From Complex Interventions to Complex Systems: Using Social Network Analysis to Understand School Engagement with Health and Wellbeing. International Journal of Environmental Research and Public Health. 2019; 16(10):1694. https://doi.org/10.3390/ijerph16101694
Chicago/Turabian StyleLittlecott, Hannah J., Graham F. Moore, Hugh Colin Gallagher, and Simon Murphy. 2019. "From Complex Interventions to Complex Systems: Using Social Network Analysis to Understand School Engagement with Health and Wellbeing" International Journal of Environmental Research and Public Health 16, no. 10: 1694. https://doi.org/10.3390/ijerph16101694
APA StyleLittlecott, H. J., Moore, G. F., Gallagher, H. C., & Murphy, S. (2019). From Complex Interventions to Complex Systems: Using Social Network Analysis to Understand School Engagement with Health and Wellbeing. International Journal of Environmental Research and Public Health, 16(10), 1694. https://doi.org/10.3390/ijerph16101694