The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Quality Evaluation
2.5. Information Extraction
- fasting plasma glucose (FPG) (mmol/L)
- glycated haemoglobin (HbA1c) (%)
- serum insulin concentration (µIU/mL)
2.6. Data Synthesis and Statistical Analyses
3. Results
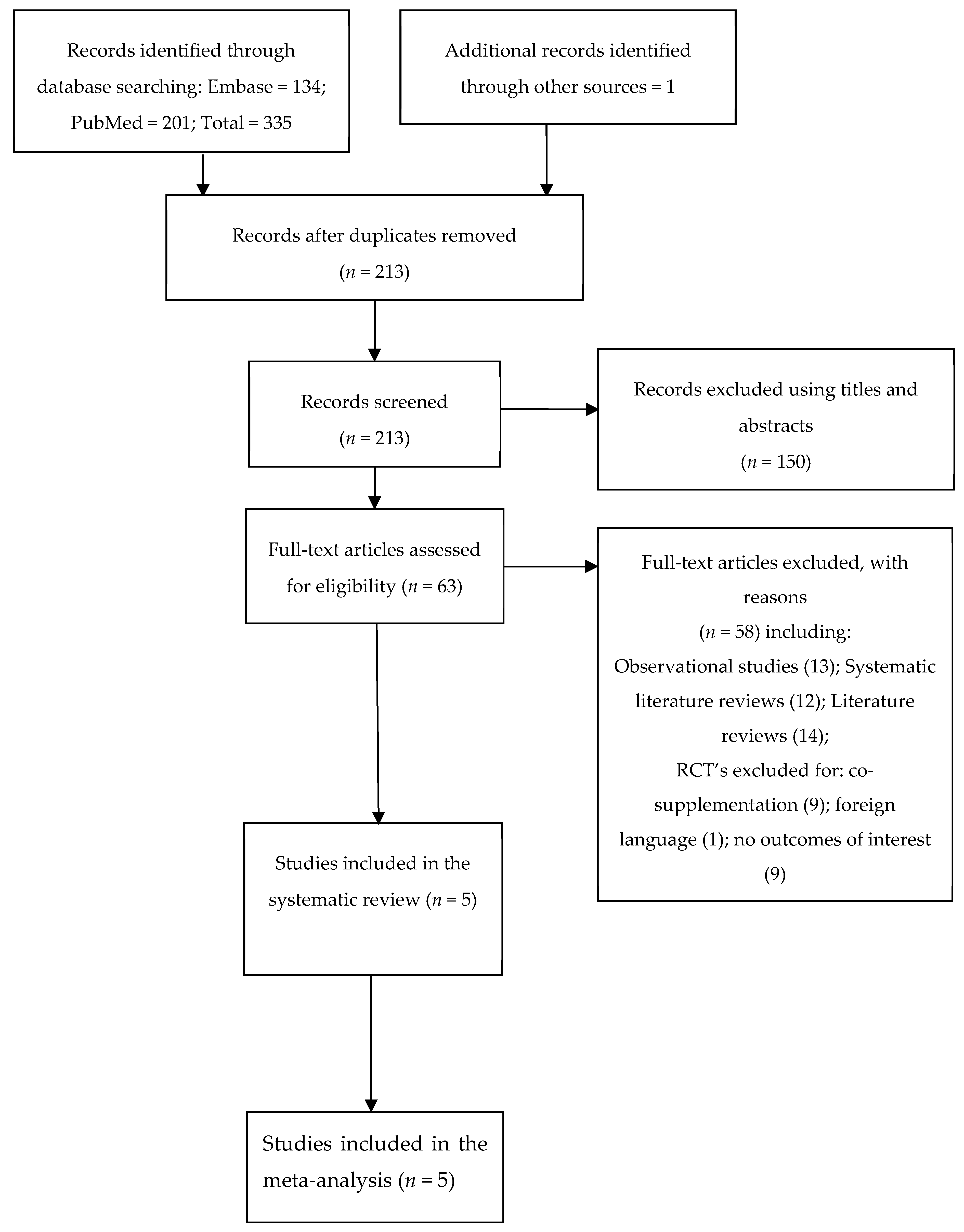
3.1. Study Selection
3.2. Data Inclusion Decisions and Discrepancies
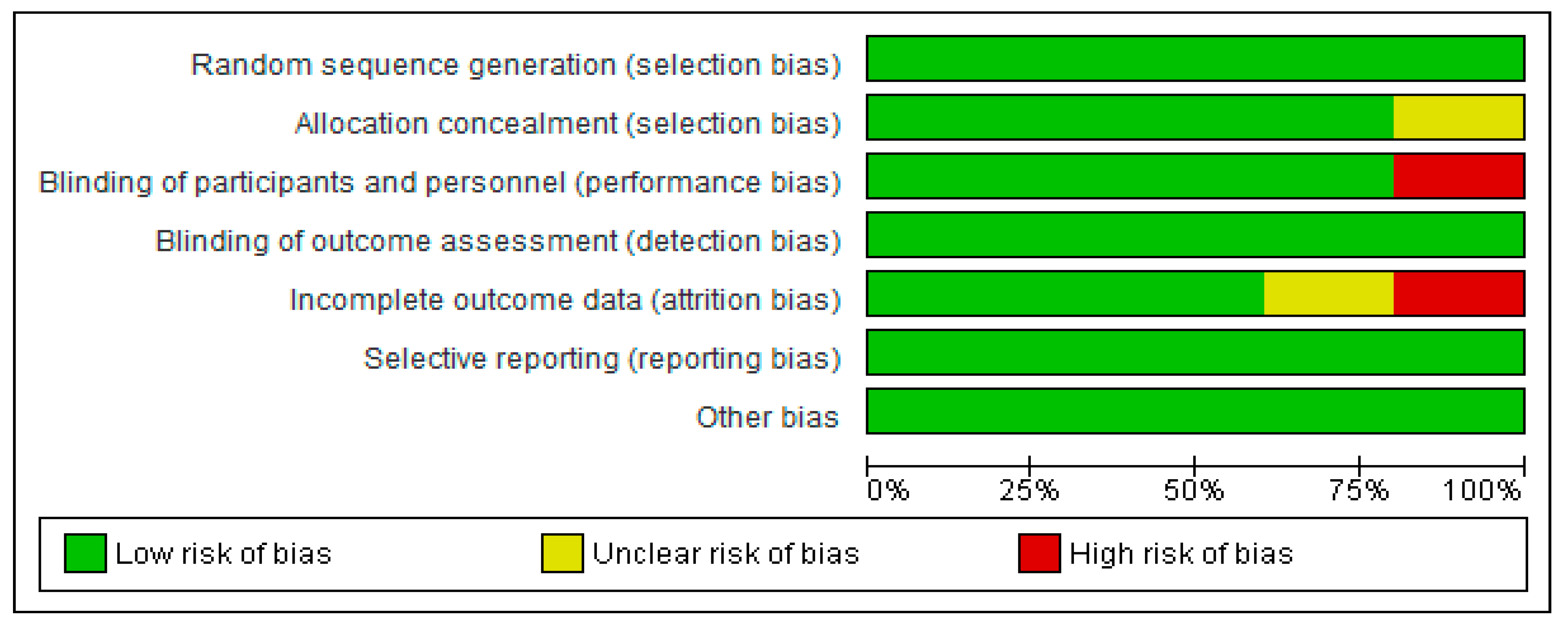
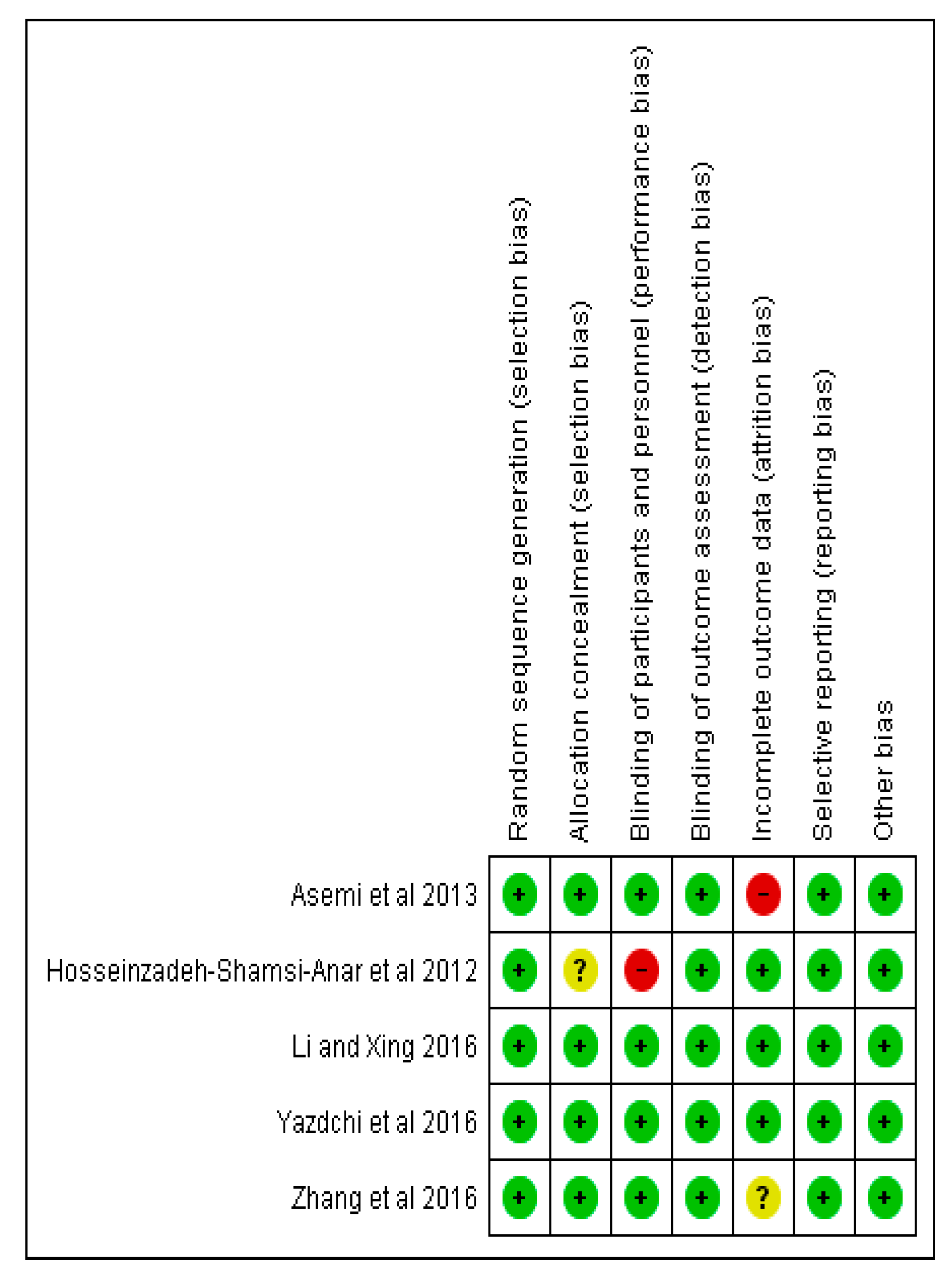
3.3. Assessment of The Risk of Bias
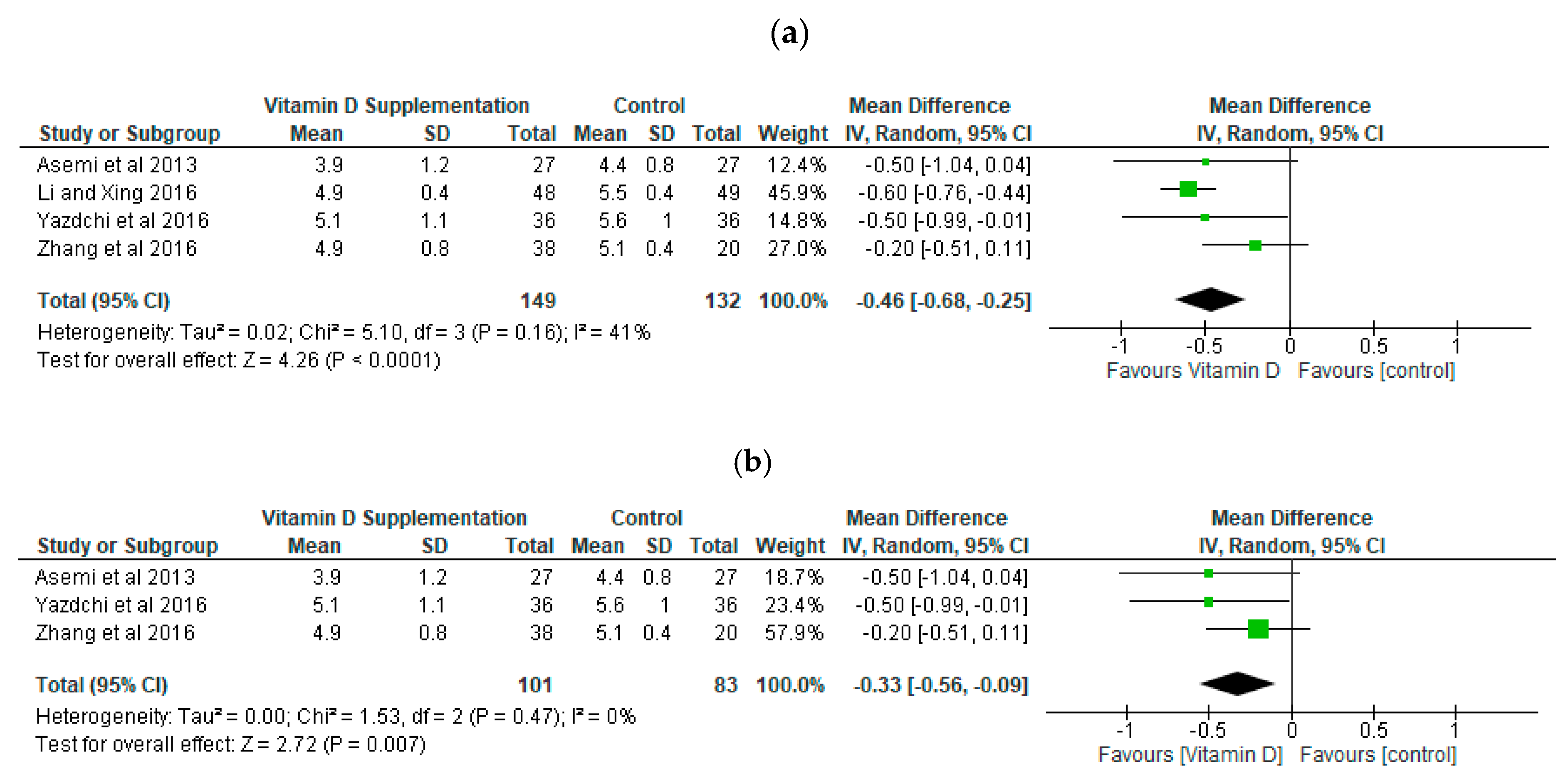
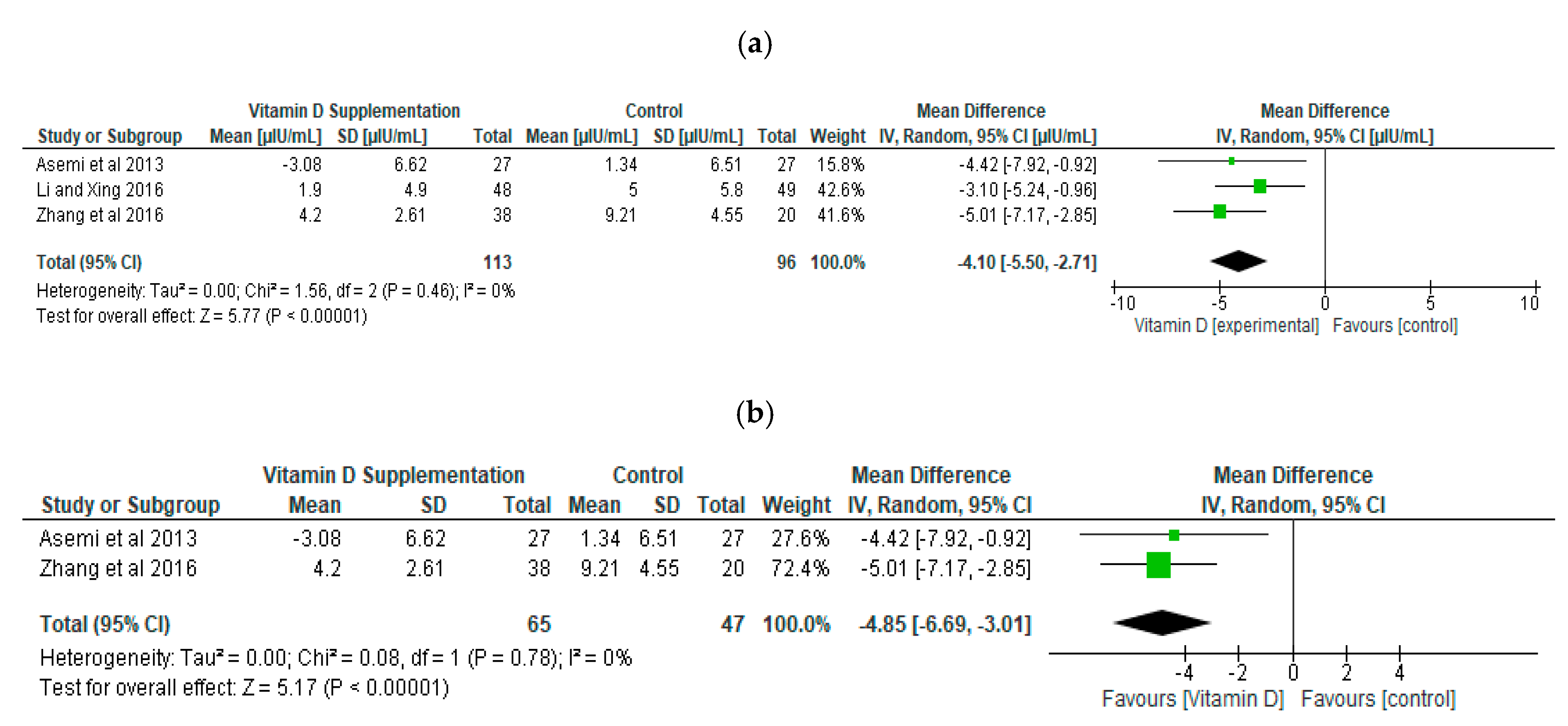
3.4. Effect of Vitamin D Supplementation During Pregnancy on Metabolic Parameters
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Search Terms
Embase
- exp pregnancy diabetes mellitus/or Gestational diabetes.mp. or GDM.mp. or gestational diabetes mellitus.mp. or diabetes mellitus, gestational.mp. or diabetes in pregnancy.mp (33032).
- exp vitamin D/or Vitamin D.mp. or 25- hydroxyvitamin D.mp. or 25OHD.mp. or calciferol.mp. or ergocalciferol.mp. or cholecalciferol.mp (144930).
- exp randomized controlled trial/or Randomised controlled trial.mp. or Controlled clinical trial.mp. or Randomized.mp. or Placebo.mp (1357496).
- 1 and 2 and 3 (138).
- limit 4 to human (134).
Pubmed
- #1
- Gestational diabetes OR GDM OR gestational diabetes mellitus OR diabetes mellitus, gestational OR diabetes in pregnancy OR Diabetes, gestational [MeSH] OR pregnancy in diabetics [MeSH] (37699).
- #2
- Vitamin D OR 25-hydroxyvitamin D OR 25OHD OR calciferol OR ergocalciferol OR cholecalciferol OR Vitamin D [MeSH] (79485).
- #3
- Randomised controlled trial OR Controlled clinical trial OR Randomized OR Placebo OR Drug therapy OR randomly OR trial OR groups OR “Randomized Controlled Trials as Topic” [MeSH] (5428822).
- #4
- Animals [MeSH] NOT Humans [MeSH] (4517123).
- #5
- #1 AND #2 AND #3 (208).
- #6
- #5 NOT #4 (201).
References
- Dunning, T. Care of People with Diabetes a Manual of Nursing Practice, 4th ed.; Wiley Blackwell: Chichester, UK, 2014. [Google Scholar]
- Hodson, K.; Robson, S.; Taylor, R. Gestational diabetes: Emerging concepts in pathophysiology. Obstet. Med. 2010, 3, 128–132. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation (WHO). Definition Diagnosis and Classification of Diabetes Mellitus and Its Complications Part 1. 1999. Available online: https://www.staff.ncl.ac.uk/philip.home/who_dmg.pdf (accessed on 16 July 2018).
- International Diabetes Federation. Gestational Diabetes. 2017. Available online: https://www.idf.org/our-activities/care-prevention/gdm (accessed on 10 December 2018).
- WHO. Diagnostic Criteria and Classification of Hyperglycaemia First Detected in Pregnancy. 2013. Available online: http://apps.who.int/iris/bitstream/handle/10665/85975/who_nmh_mnd_13.2_eng.pdf?sequence=1 (accessed on 10 December 2018).
- Zhang, M.-X.; Pan, G.-T.; Guo, J.-F.; Li, B.-Y.; Qin, L.-Q.; Zhang, Z.-L. Vitamin D Deficiency Increases the Risk of Gestational Diabetes Mellitus: A Meta-Analysis of Observational Studies. Nutrients 2015, 7, 8366–8375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosseinzadeh-Shamsi-Anar, M.; Mozaffari-Khosravi, H.; Salami, M.-A.; Hadinedoushan, H.; Mozayan, M.R. The Efficacy and Safety of a High Dose of Vitamin D in Mothers with Gestational Diabetes Mellitus: A Randomized Controlled Clinical Trial. Iran. J. Med. Sci. 2012, 37, 159–165. [Google Scholar]
- Christesen, H.T.; Falkenberg, T.; Lamont, R.F.; Jørgensen, J.S. The impact of vitamin D on pregnancy: A systematic review. Acta Obstet. Gynecol. Scand. 2012, 91, 1357–1367. [Google Scholar] [CrossRef]
- Burris, H.H.; Camargo, C.J. Vitamin D and gestational diabetes mellitus. Curr. Diabetes Rep. 2014, 14, 451. [Google Scholar] [CrossRef]
- Palacios, C.; Gonzalez, L. Is vitamin D deficiency a major global public health problem? J. Steroid Biochem. Mol. Biol. 2014, 144, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De-Regil, L.M.; Palacios, C.; Lombardo, L.K.; Peña-Rosas, J.P. Vitamin D supplementation for women during pregnancy. Sao Paulo Med. J. 2016, 134, 274–275. [Google Scholar] [CrossRef] [Green Version]
- Valdes-Ramos, R.; Laura, G.-L.A.; Elina, M.-C.B.; Donají, B.-A.A.; Laura, G.-L.; Elina, M.-C.; Donaji, B.-A. Vitamins and Type 2 Diabetes Mellitus. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 54–63. [Google Scholar] [CrossRef]
- Mir, S.A.; Masoodi, S.R.; Shafi, S.; Hameed, I.; Dar, M.A.; Bashir, M.I.; Wani, A.I.; Shah, Z.A.; Parveen, S.; Zargar, A.H.; et al. Efficacy and safety of Vitamin D supplementation during pregnancy: A randomized trial of two different levels of dosing on maternal and neonatal Vitamin D outcome. Indian J. Endocrinol. Metab. 2016, 20, 337–342. [Google Scholar]
- Poel, Y.; Hummel, P.; Lips, P.; Stam, F.; Van Der Ploeg, T.; Simsek, S. Vitamin D and gestational diabetes: A systematic review and meta-analysis. Eur. J. Intern. Med. 2012, 23, 465–469. [Google Scholar] [CrossRef]
- Theodoratou, E.; Tzoulaki, I.; Zgaga, L.; Ioannidis, J.P.A. Vitamin D and multiple health outcomes: Umbrella review of systematic reviews and meta-analyses of observational studies and randomised trials. BMJ 2014, 348, g2035. [Google Scholar] [CrossRef]
- Zhang, Y.; Gong, Y.; Xue, H.; Xiong, J.; Cheng, G. Vitamin D and gestational diabetes mellitus: A systematic review based on data free of Hawthorne effect. BJOG Int. J. Obstet. Gynaecol. 2018, 125, 784–793. [Google Scholar] [CrossRef]
- Kamudoni, P.; Poole, C.; Davies, S.J. An estimate of the economic burden of vitamin D deficiency in pregnant women in the United Kingdom. Gynecol. Endocrinol. 2016, 32, 592–597. [Google Scholar] [CrossRef]
- Pérez-López, F.R.; Pasupuleti, V.; Mezones-Holguín, E.; Benites-Zapata, V.A.; Thota, P.; Deshpande, A.; Hernandez, A.V. Effect of vitamin D supplementation during pregnancy on maternal and neonatal outcomes: A systematic review and meta-analysis of randomized controlled trials. Fertil. Steril. 2015, 103, 1278–1288.e4. [Google Scholar] [CrossRef]
- Agarwal, S.; Kovilam, O.; Devendra, K. Vitamin D and its impact on maternal-fetal outcomes in pregnancy: A critical review. Crit. Rev. Food Sci. Nutr. 2018, 58, 755–769. [Google Scholar] [CrossRef]
- Wei, S.Q. Vitamin D and pregnancy outcomes. Curr. Opin. Obstet. Gynecol. 2014, 26, 438–447. [Google Scholar] [CrossRef]
- Dornhorst, A.; Frost, G. The principles of dietary management of gestational diabetes: Reflection on current evidence. J. Hum. Nutr. Diet. 2002, 15, 145–156. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.; Moosazadeh, M.; Tabrizi, R.; Samimi, M.; Karamali, M.; Jamilian, M.; Kolahdooz, F.; Lankarani, K.B.; Asemi, Z. The Effects of Vitamin D Supplementation on Glucose Metabolism and Lipid Profiles in Patients with Gestational Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Horm. Metab. Res. 2017, 49, 647–653. [Google Scholar] [PubMed]
- Roth, D.E.; Leung, M.; Mesfin, E.; Qamar, H.; Watterworth, J.; Papp, E. Vitamin D supplementation during pregnancy: State of the evidence from a systematic review of randomised trials. BMJ 2017, 359, j5237. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme (CASP). Randomised Controlled Trial Checklist. 2017. Available online: http://docs.wixstatic.com/ugd/dded87_4239299b39f647ca9961f30510f52920.pdf (accessed on 10 December 2018).
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- Metzger, B.E.; Lowe, L.P.; Dyer, A.R.; Trimble, E.R.; Chaovarindr, U.; Coustan, D.R.; Hadden, D.R.; McCance, D.R.; Hod, M.; McIntyre, H.D.; et al. Hyperglycemia and Adverse Pregnancy Outcomes. N. Engl. J. Med. 2008, 358, 1991–2002. [Google Scholar] [Green Version]
- The Nordic Cochrane Centre. Review Manager (RevMan) [Computer Program] Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014. [Google Scholar]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Asemi, Z.; Hashemi, T.; Karamali, M.; Samimi, M.; Esmaillzadeh, A. Effects of vitamin D supplementation on glucose metabolism, lipid concentrations, inflammation, and oxidative stress in gestational diabetes: A double-blind randomized controlled clinical trial. Am. J. Clin. Nutr. 2013, 98, 1425–1432. [Google Scholar] [CrossRef] [PubMed]
- Xing, B.; Li, Q. Vitamin D3-Supplemented Yogurt Drink Improves Insulin Resistance and Lipid Profiles in Women with Gestational Diabetes Mellitus: A Randomized Double Blinded Clinical Trial. Ann. Nutr. Metab. 2016, 68, 285–290. [Google Scholar]
- Zhang, Q.; Cheng, Y.; He, M.; Li, T.; Ma, Z.; Cheng, H. Effect of various doses of vitamin D supplementation on pregnant women with gestational diabetes mellitus: A randomized controlled trial. Exp. Ther. Med. 2016, 12, 1889–1895. [Google Scholar] [CrossRef] [Green Version]
- Yazdchi, R.; Gargari, B.P.; Asghari-Jafarabadi, M.; Sahhaf, F. Effects of vitamin D supplementation on metabolic indices and hs-CRP levels in gestational diabetes mellitus patients: A randomized, double-blinded, placebo-controlled clinical trial. Nutr. Res. Pract. 2016, 10, 328–335. [Google Scholar] [CrossRef]
- Reeves, B.C. Principles of research: Limitations of non-randomized studies. Surgery 2008, 26, 120–124. [Google Scholar] [CrossRef]
- Asemi, Z.; Karamali, M.; Esmaillzadeh, A. Effects of calcium–vitamin D co-supplementation on glycaemic control, inflammation and oxidative stress in gestational diabetes: A randomised placebo-controlled trial. Diabetologia 2014, 57, 1798–1806. [Google Scholar] [CrossRef]
- Mozaffari-Khosravi, H.; Hosseinzadeh-Shamsi-Anar, M.; Salami, M.-A.; Hadinedoushan, H.; Mozayan, M.R. Effects of a single post-partum injection of a high dose of vitamin D on glucose tolerance and insulin resistance in mothers with first-time gestational diabetes mellitus. Diabet. Med. 2012, 29, 36–42. [Google Scholar] [CrossRef]
- Valizadeh, M.; Piri, Z.; Mohammadian, F.; Kamali, K.; Moghadami, H.R.A. The Impact of Vitamin D Supplementation on Post-Partum Glucose Tolerance and Insulin Resistance in Gestational Diabetes: A Randomized Controlled Trial. Int. J. Endocrinol. Metab. 2016, 14, 34312. [Google Scholar] [CrossRef]
- Zhu, J.; Chen, Y.; Li, C.; Tao, M.; Teng, Y. The diagnostic value of glycated albumin in gestational diabetes mellitus. J. Endocrinol. Investig. 2018, 41, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Rudnicki, P.M.; Mølsted-Pedersen, L. Effect of 1,25-dihydroxycholecalciferol on glucose metabolism in gestational diabetes mellitus. Diabetologia 1997, 40, 40–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asemi, Z.; Samimi, M.; Tabassi, Z.; Shakeri, H.; Esmaillzadeh, A. Vitamin D Supplementation Affects Serum High-Sensitivity C-Reactive Protein, Insulin Resistance, and Biomarkers of Oxidative Stress in Pregnant Women. J. Nutr. 2013, 143, 1432–1438. [Google Scholar] [CrossRef] [Green Version]
- El Lithy, A.; Abdella, R.M.; El-Faissal, Y.M.; Sayed, A.M.; Samie, R.M. The relationship between low maternal serum vitamin D levels and glycemic control in gestational diabetes assessed by HbA1c levels: An observational cross-sectional study. BMC Pregnancy Childbirth 2014, 14, 362. [Google Scholar] [CrossRef]
- Soheilykhah, S.; Mojibian, M.; Moghadam, M.J.; Shojaoddiny-Ardekani, A. The effect of different doses of vitamin D supplementation on insulin resistance during pregnancy. Gynecol. Endocrinol. 2013, 29, 396–399. [Google Scholar] [CrossRef]
- Shaat, N.; Ignell, C.; Katsarou, A.; Berntorp, K. Glucose homeostasis, beta cell function, and insulin resistance in relation to vitamin D status after gestational diabetes mellitus. Acta Obstet. Gynecol. Scand. 2017, 96, 821–827. [Google Scholar] [CrossRef]
- Boucher, D.B.J.; Mannan, N.; Noonan, K.; Hales, C.N.; Evans, S.J.W. Glucose intolerance and impairment of insulin secretion in relation to vitamin D deficiency in East London Asians. Diabetologia 1995, 38, 1239–1245. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE, 2014) vitamin D: Supplement Use in Specific Population Groups. Available online: https://www.nice.org.uk/guidance/ph56/resources/vitamin-d-supplement-use-in-specific-population-groups-pdf-1996421765317 (accessed on 16 July 2018).
- Boucher, B.J. Early Pregnancy Maternal Vitamin D Concentrations and Risk of Gestational Diabetes Mellitus. Paediatr. Perinat. Epidemiol. 2015, 29, 196–199. [Google Scholar] [CrossRef] [PubMed]
- Royal College of Obstetricians and Gynaecologists (RCOG, 2014) Vitamin D in Pregnancy Scientific Impact Paper No. 43. Available online: https://www.rcog.org.uk/globalassets/documents/guidelines/scientific-impact-papers/vitamin_d_sip43_june14.pdf (accessed on 16 July 2018).
- World Health Organisation. Vitamin D Supplementation in Pregnant Women. 2012. Available online: http://apps.who.int/iris/bitstream/handle/10665/85313/9789241504935_eng.pdf;jsessionid=C077E6F9BA149099945FBBDE03992525?sequence=1 (accessed on 10 December 2018).
- National Institute for Health and Care Excellence (NICE) Diabetes in Pregnancy: Management from Preconception to the Postnatal Period. 2015. Available online: https://www.nice.org.uk/guidance/ng3/resources/diabetes-in-pregnancy-management-from-preconception-to-the-postnatal-period-51038446021 (accessed on 10 December 2018).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Citation | Country | Type of Study | Study Dates | Length of Study | Sample Size (Intervention, Control-Placebo) | Mean Age of Mother | Time of Vitamin D Intervention | Intervention | Outcome Measures of Interest | Risk of Biases | Study Results |
|---|---|---|---|---|---|---|---|---|---|---|---|
| #Asemi et al. (2013a) [31] | Iran | Randomized, double-blinded, placebo controlled clinical trial | Jan 2013–April 2013 | 6 weeks | 54 (27,27) | 31.5 ± 6.1 years | At 24–28 weeks of gestation | 50,000 IU Vitamin D3 supplements at baseline and at day 21 | FPG, SI concentration | 6/7 low risk 1 high risk for attrition bias | Change from baseline: Vitamin D group versus the control FBG −17.12 ± 14.84 compared with −0.96 ± 16.64 mg/dL; p < 0.001- SI Concentration −3.08 ± 6.62 compared with 1.34 ± 6.51 µIU/mL; p = 0.01 ANOVA |
| #Li and Xing, (2016) [32] | China | Randomized Study Design | Between early November and late February each year from 2010 to 2014 | 16 weeks | 97 (48,49) | 24–32 years old | At 13 weeks of gestation | 2 servings (200g) of supplemented yogurt per day (500 IU vitamin D3 per serving) | FPG, SI concentration | 7/7 low risk | Change from baseline: Vitamin D group versus the control FBG −9.9 ± 7.2 compared with 2.9 ± 7.6 mg/dL; p = 0.04 SI Concentration −1.9 ± 4.9 compared with 5.0 ± 5.8 µIU/mL; p = 0.03 t-test |
| ##Zhang et al. (2016) [33] | China | Randomized, double-blind placebo-controlled clinical trial | Sept 2009–Nov 2014 | 4 weeks | 133 (38,20) ** | 29.8 ± 4.7 years | At 24–28 weeks of gestation | Low dosage: 200 IU Vitamin D supplement daily Medium dosage: 2000 IU daily for 25 days High dosage: 4000 daily for 12.5 days | FPG, SI concentration | 6/7 low risk 1 unclear risk for attrition bias | FBG Low: 96.12; Medium: 88.59; High: 84.73 vitamin D supplementation compared with control: 92.49 mg/dL; p > 0.05 SI Concentration Medium: 5.01; High: 4.2 vitamin D supplementation compared with control: 9.21 IU/mL; p < 0.01 Non-parametric tests |
| ###Yazdchi et al., (2016) [34] | Iran | Randomized, double-blinded, placebo-controlled clinical trial | July 2013–Sept 2014 | 8 weeks | 72 (36,36) | 31.88 ± 4.0 years | At 24–28 weeks of gestation | 4 oral treatments of 50,000 IU of Vitamin D3 (one capsule every 2 weeks) | FPG, SI concentration HbA1c | 7/7 low risk | Change from baseline: Vitamin D group versus the control FBG −4.72 ± 13.99 compared with 5.27 ± 9.93 mg/dL; p = 0.01 SI Concentration 1.80 (−1.67–3.77) compared with −0.45 (−1.07–1.35) µIU/mL; p = 0.23 HbA1c −0.18% ± 0.48% compared with 0.17% ± 0.39%; p = 0.02 ANCOVA |
| ####Hosseinzadeh-Shamsi-Anar et al. (2012) [7] | Iran | Randomized clinical trial | Study dates not provided | 12 weeks | 45 (24,21) | 30.7 ± 6.2 years | At 24–28 week gestation | Intramuscular 300,000 IU of vitamin D | HbA1c | 5/7 low risk 1 unclear risk for selection bias 1 high risk for performance bias | Vitamin D group versus control HbA1c 5.58% ± 12 compared with 5.21±0.52% p = 0.2 t-test |
| Citation | Interventions | Estimated Average Intake of Vitamin D Per Day IU/day | Pre-Intervention Vitamin D Level in Blood/Serum |
|---|---|---|---|
| Asemi et al. (2013a) [31] | Vitamin D | 4762 | 20.44 ± 14.31 * |
| Control | Placebo | 20.41 ± 13.43 * | |
| Li and Xing, (2016) [32] | Vitamin D supplemented Yoghurt | 1000 | 16.8 ± 4.6 * |
| Plain Yoghurt | Plain Yoghurt | 16.2 ± 3.4 * | |
| Zhang et al. (2016) [33] | Vitamin D | 2000 | Actual values not stated. Vit. D deficiency (<20 ng/mL) |
| Control | Placebo | Actual values not stated. Vit. D deficiency (<20 ng/mL) | |
| Yazdchi et al., (2016) [34] | Vitamin D | 3333 | 9.54 (Median) (6.12–15.94) (25th and 75th percentile) |
| Control | Placebo | 9.02 (Median) (7.29–14.70) (25th and 75th percentile) | |
| Hosseinzadeh-Shamsi-Anar et al. (2012) [7] | Vitamin D | 3333 | 24.25 nmol/L (Median) (13.3–202.4) (Min–Max) |
| Control | No Vitamin D | 25.30 nmol/L (Median) (12.8–137.2) (Min–Max) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Weldon, S.M.; Thompson, T.; Vargo, E.J. The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Int. J. Environ. Res. Public Health 2019, 16, 1716. https://doi.org/10.3390/ijerph16101716
Ojo O, Weldon SM, Thompson T, Vargo EJ. The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. International Journal of Environmental Research and Public Health. 2019; 16(10):1716. https://doi.org/10.3390/ijerph16101716
Chicago/Turabian StyleOjo, Omorogieva, Sharon M. Weldon, Trevor Thompson, and Elisabeth J. Vargo. 2019. "The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials" International Journal of Environmental Research and Public Health 16, no. 10: 1716. https://doi.org/10.3390/ijerph16101716
APA StyleOjo, O., Weldon, S. M., Thompson, T., & Vargo, E. J. (2019). The Effect of Vitamin D Supplementation on Glycaemic Control in Women with Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. International Journal of Environmental Research and Public Health, 16(10), 1716. https://doi.org/10.3390/ijerph16101716