Impact of Active Video Games on Body Mass Index in Children and Adolescents: Systematic Review and Meta-Analysis Evaluating the Quality of Primary Studies


 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Studies, Participants, and Interventions
2.2. Outcome Measures
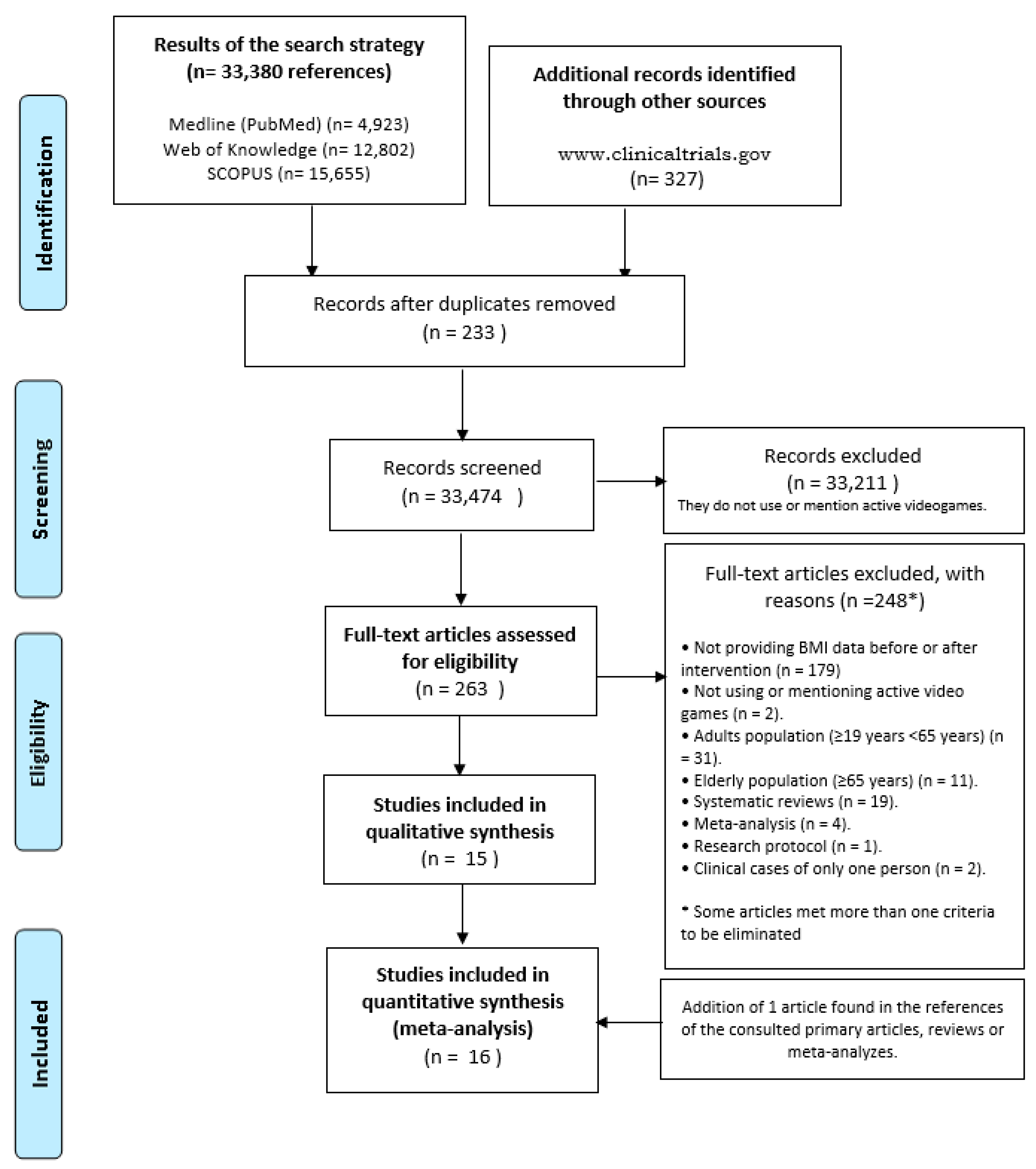
2.3. Search Strategy for Identification of Studies, Study Selection, and Data Abstraction
2.4. Assessment of Methodological Quality
- (1)
- Selection bias;
- (2)
- Design;
- (3)
- Confounders;
- (4)
- Blinding;
- (5)
- Data collection methods;
- (6)
- Withdrawals and dropouts;
- (7)
- Intervention integrity; and
- (8)
- Analysis.
2.5. Data Analyses
3. Results
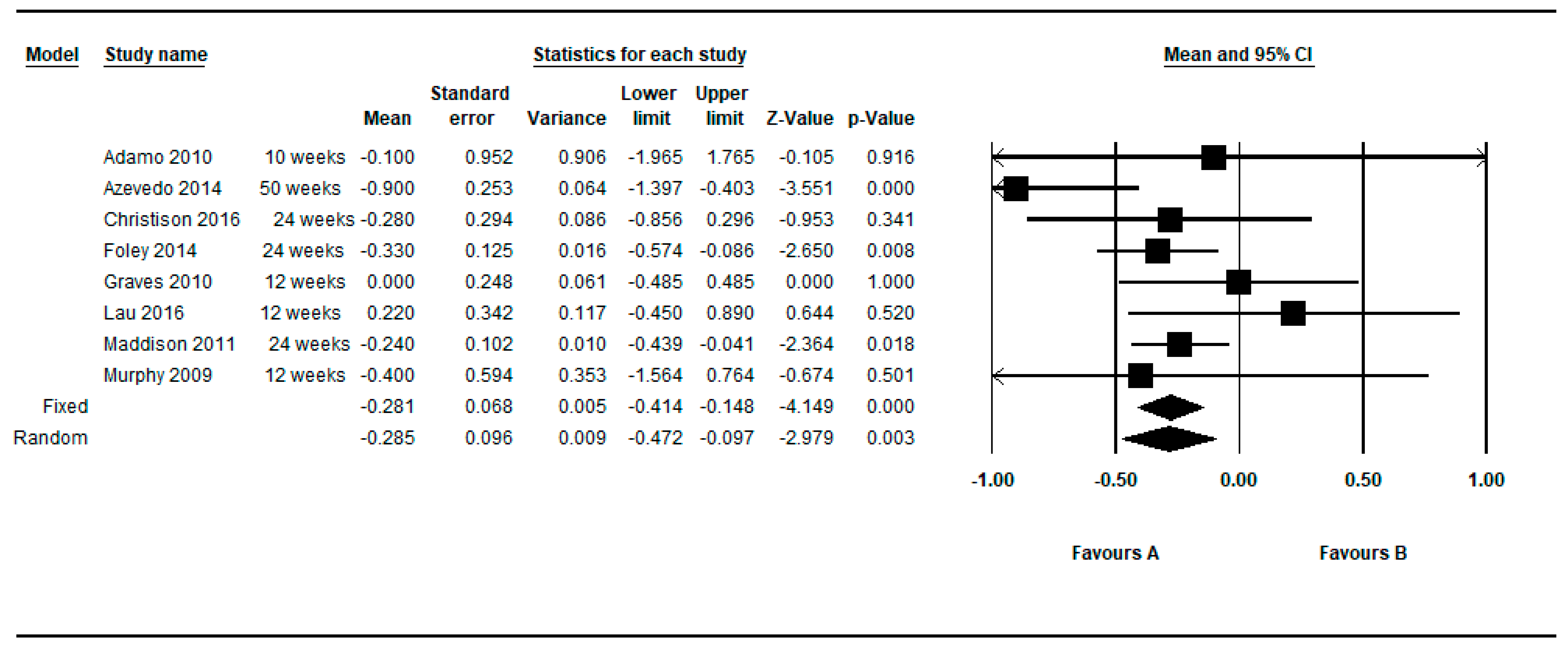
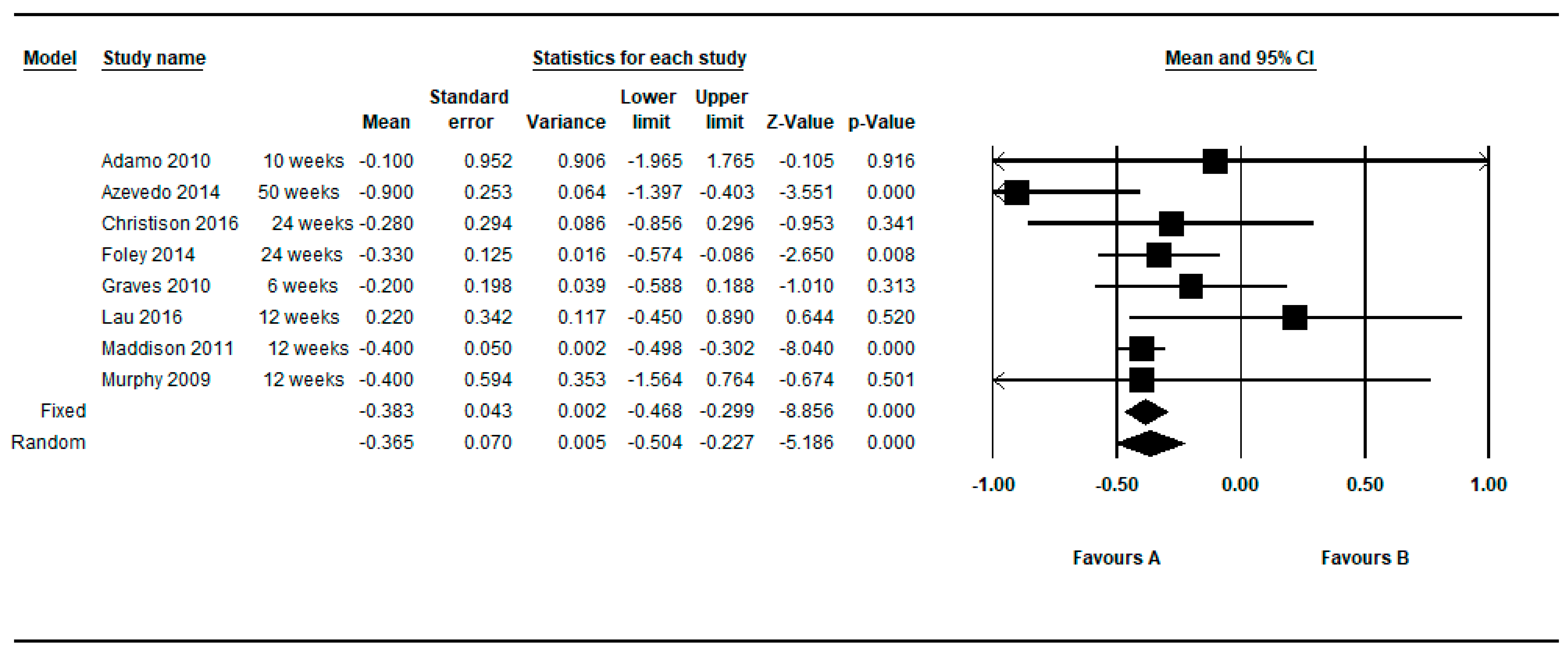
3.1. Intra-Group Pre-Post Difference in the BMI in the Intervention Group
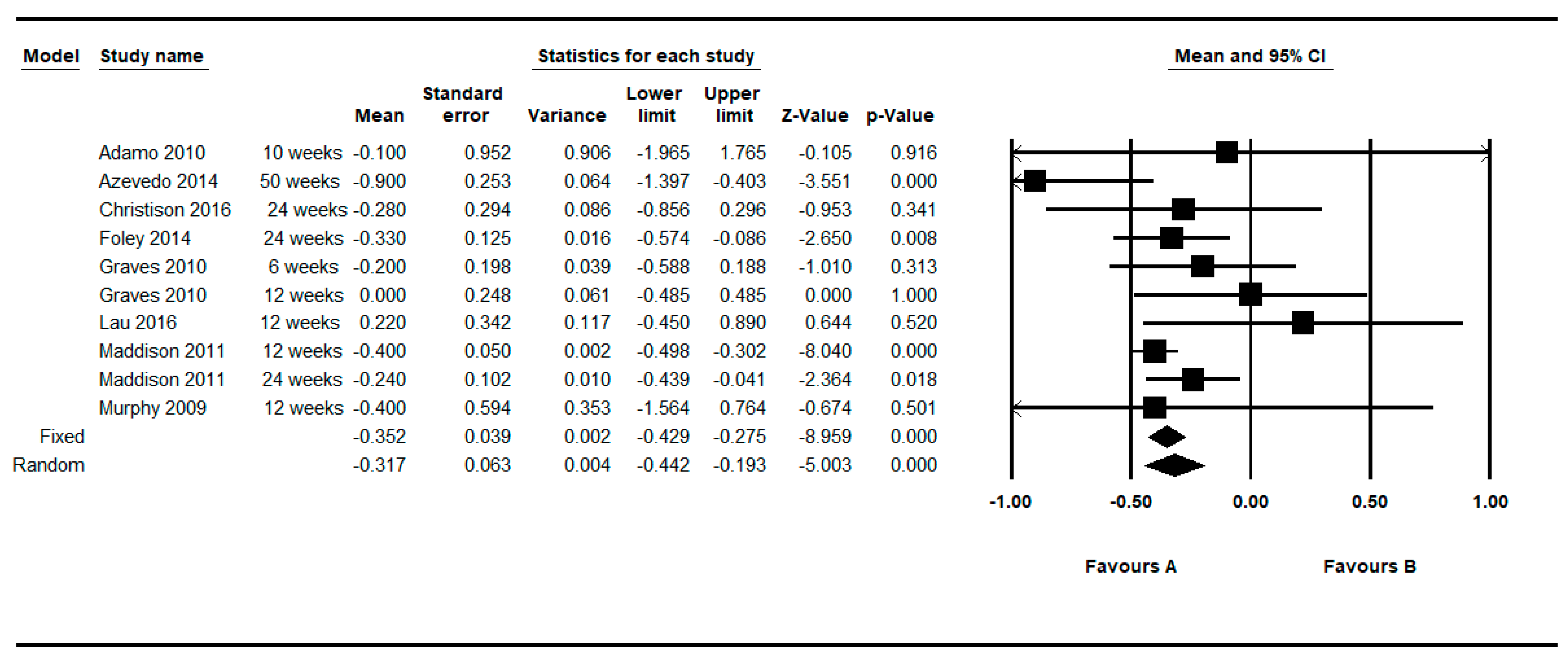
3.2. Intra-Group Pre-Post Difference in the BMI in the Control Group
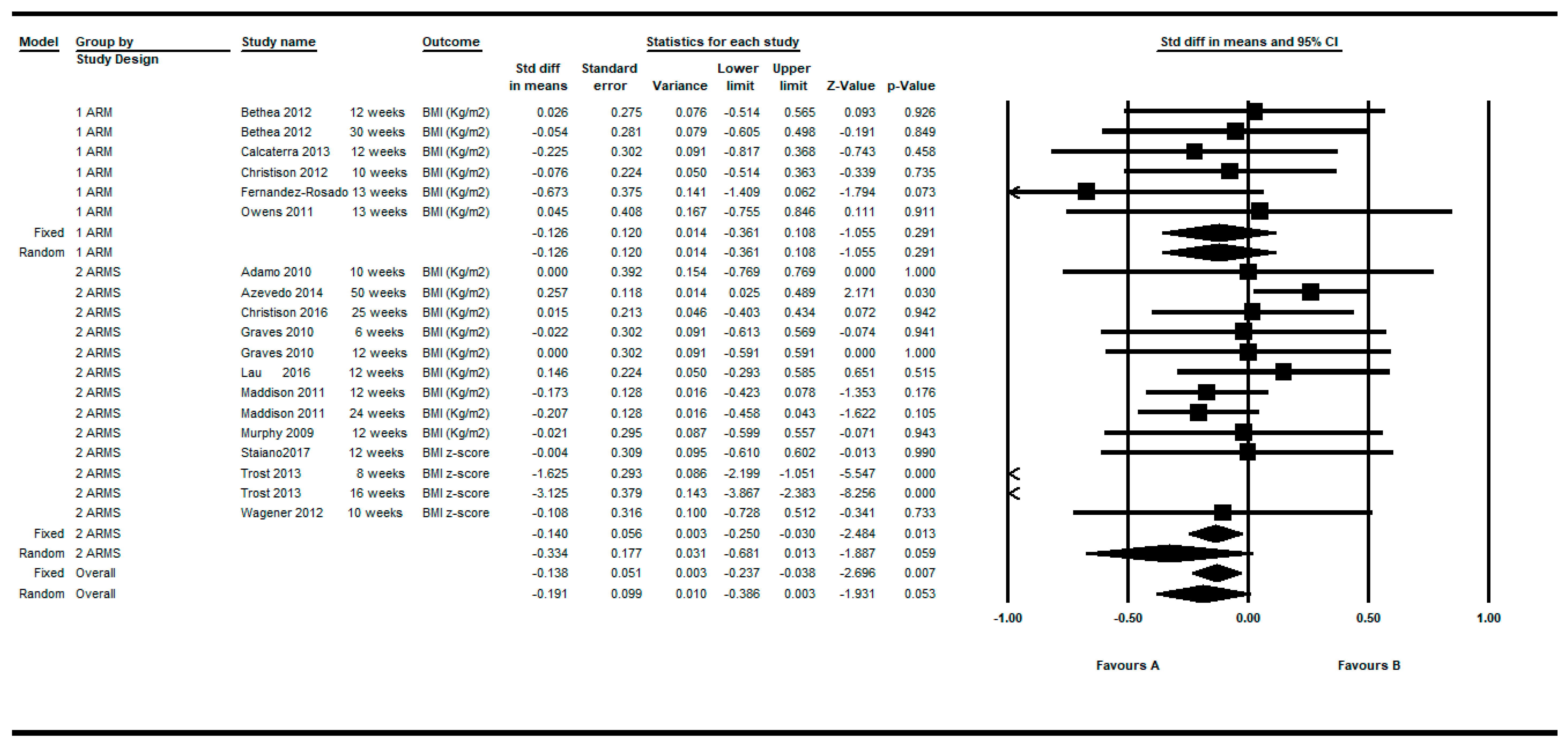
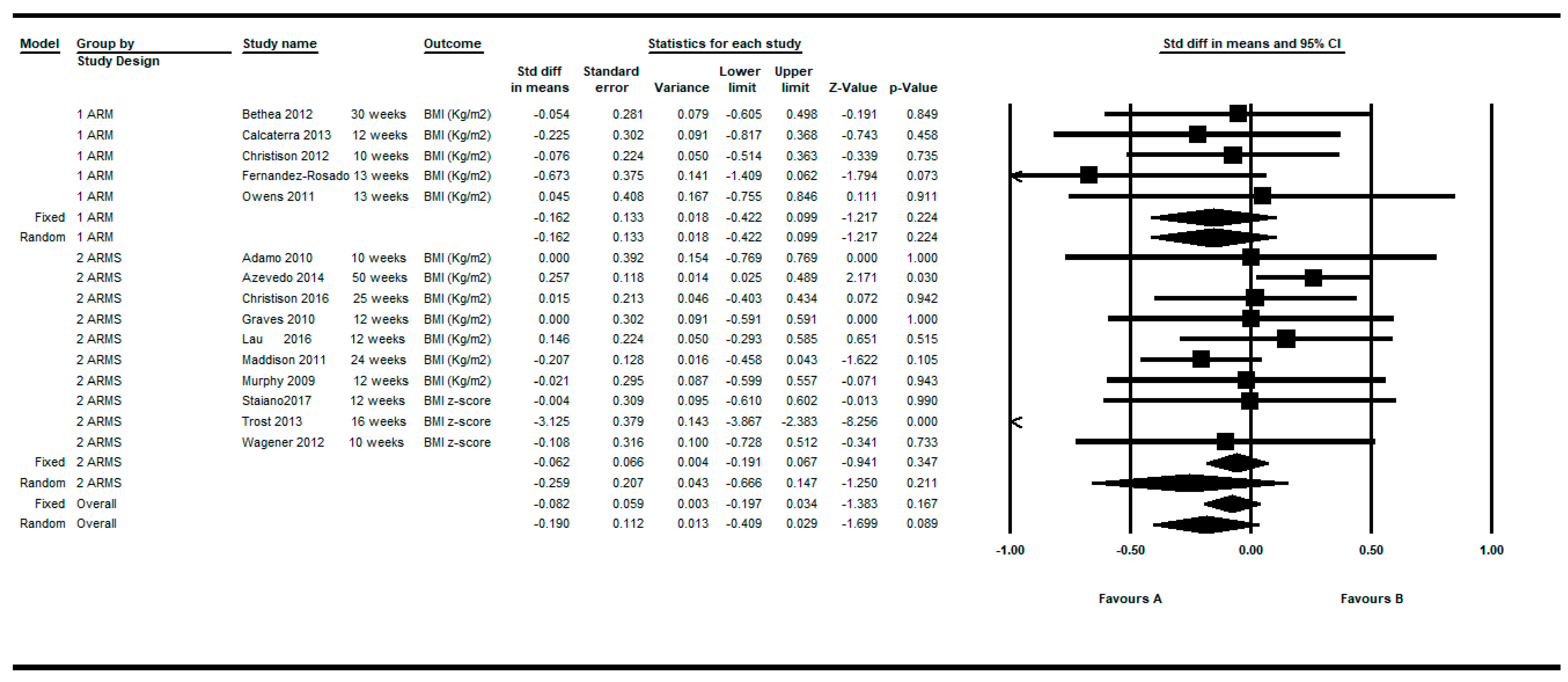
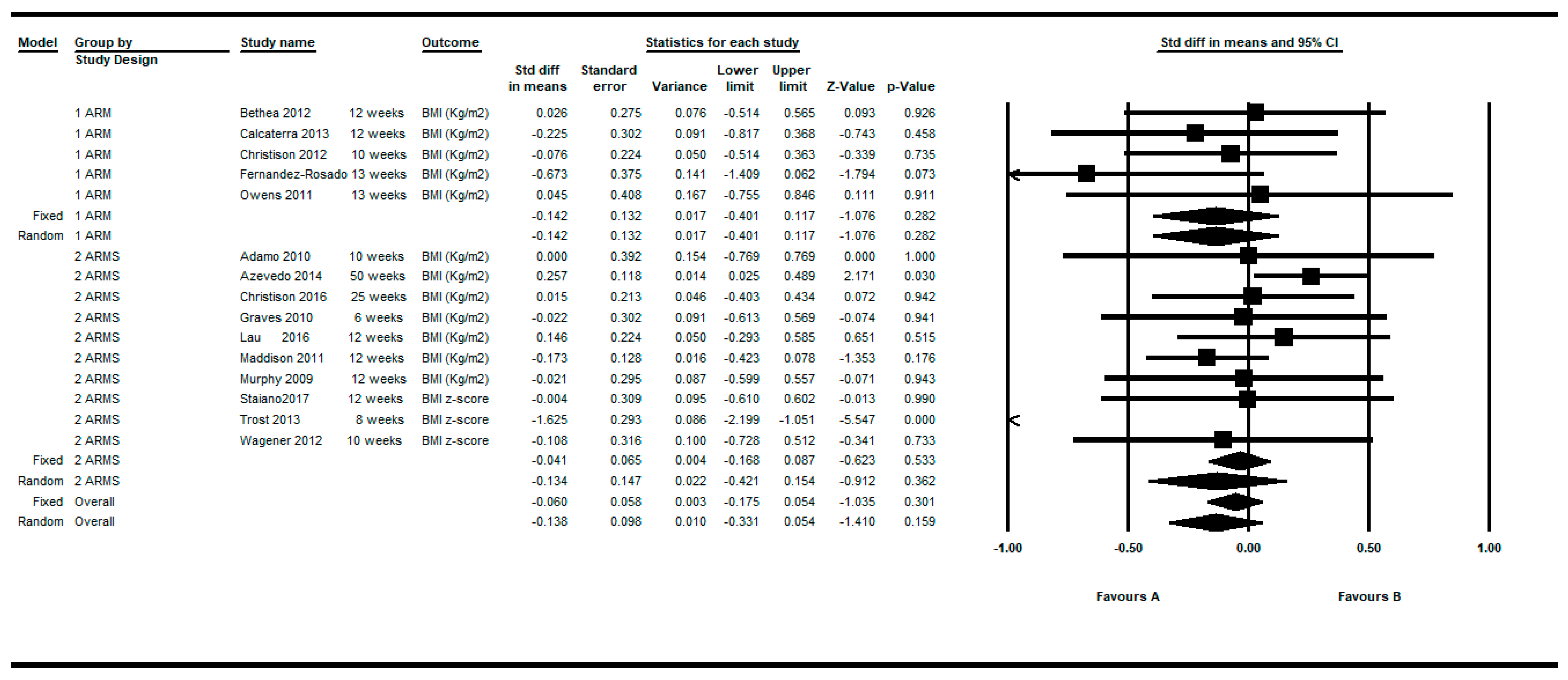
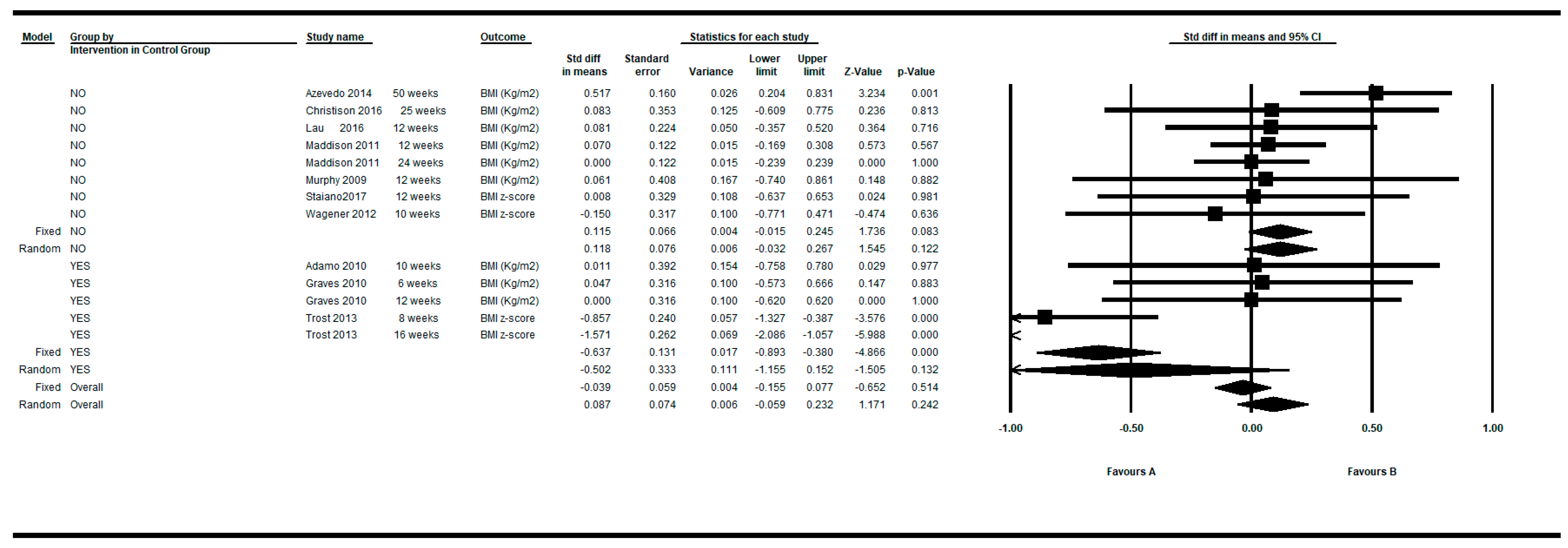
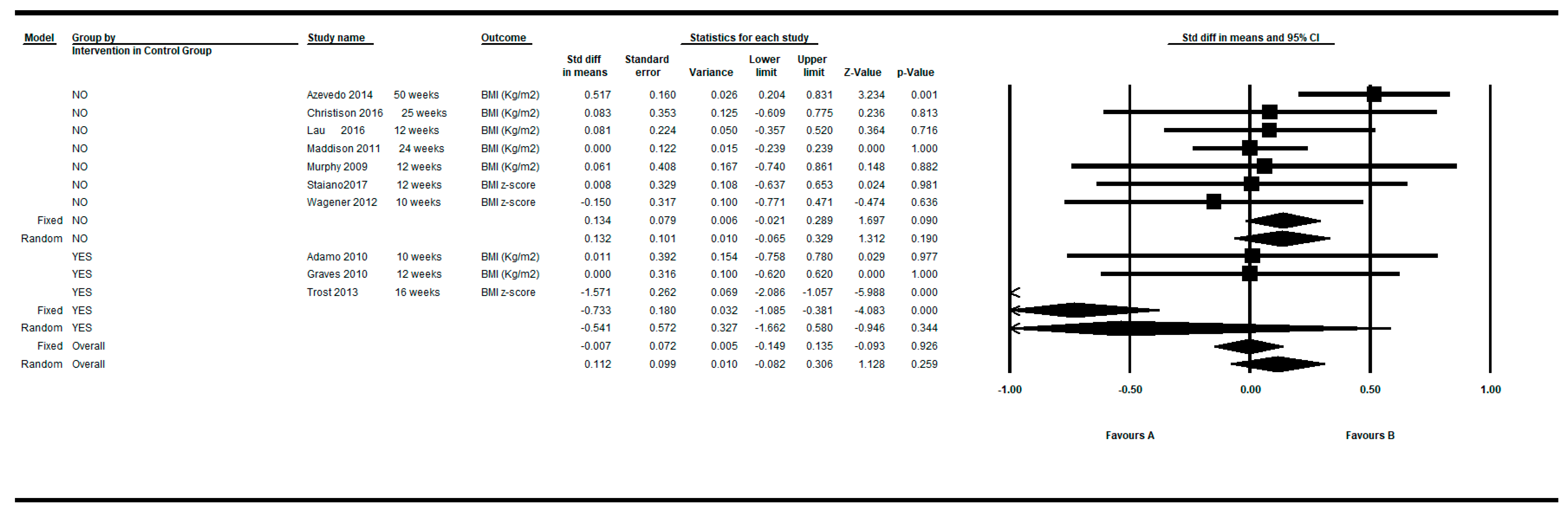
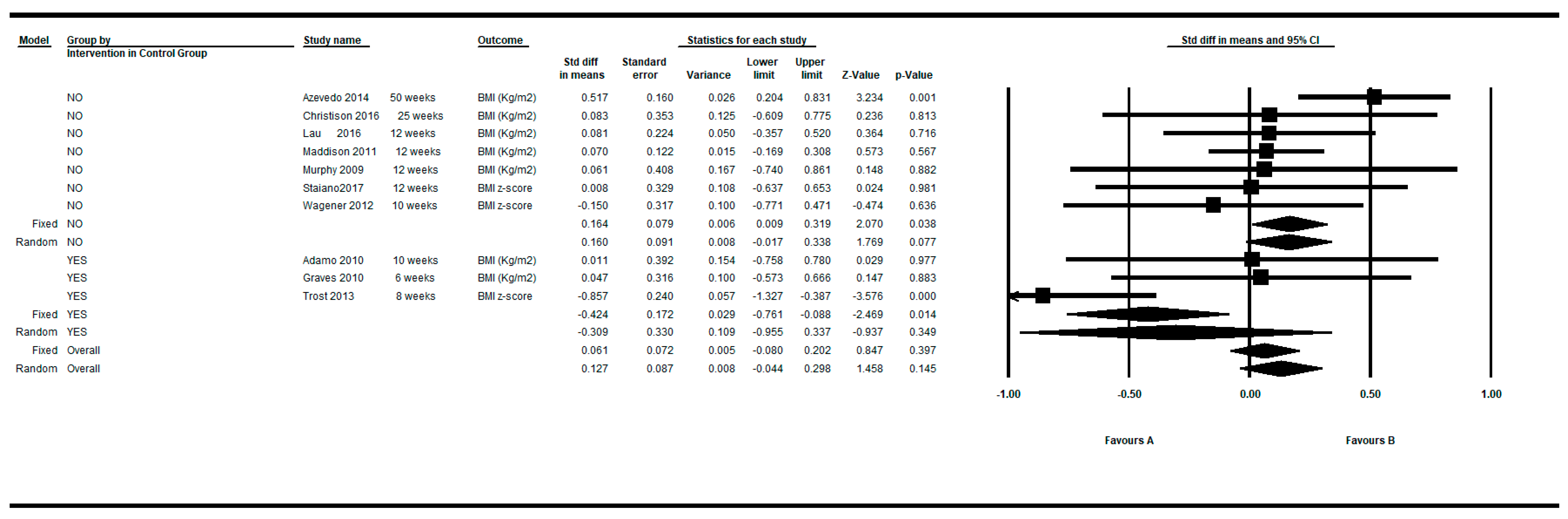
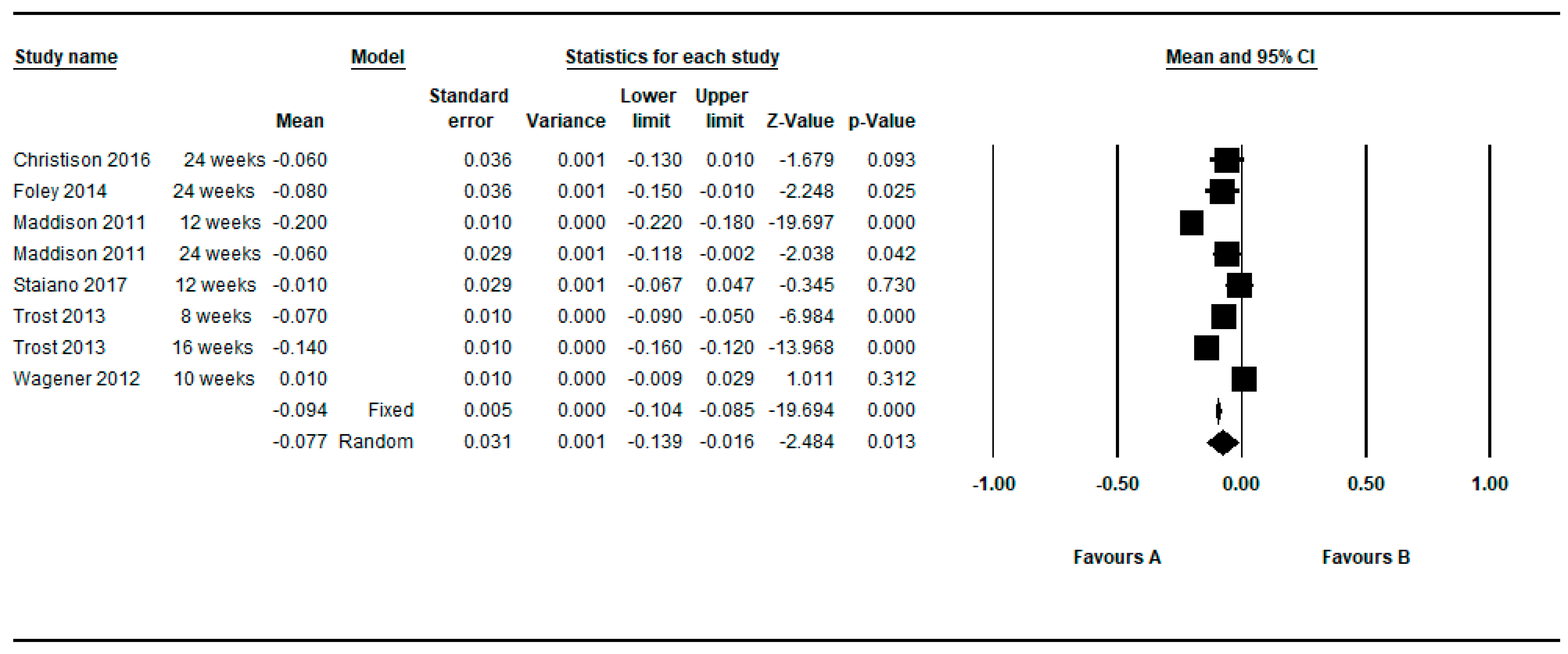
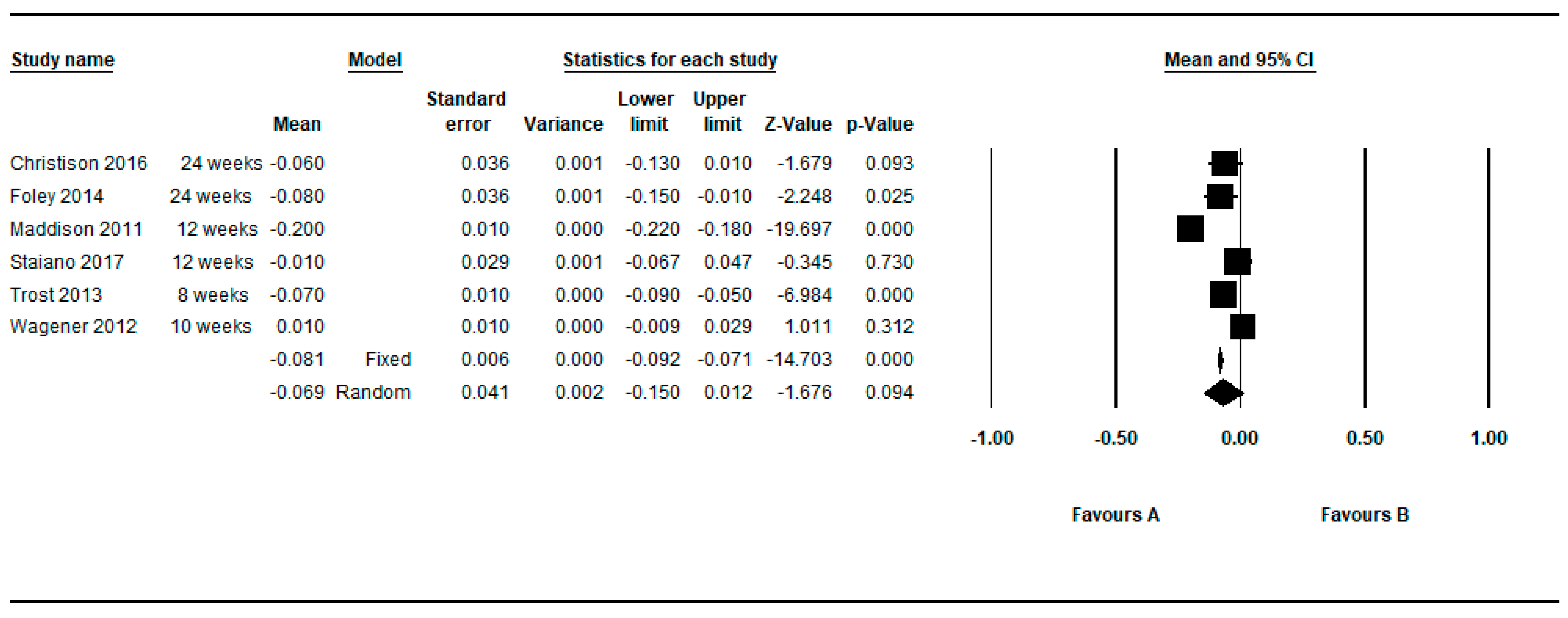
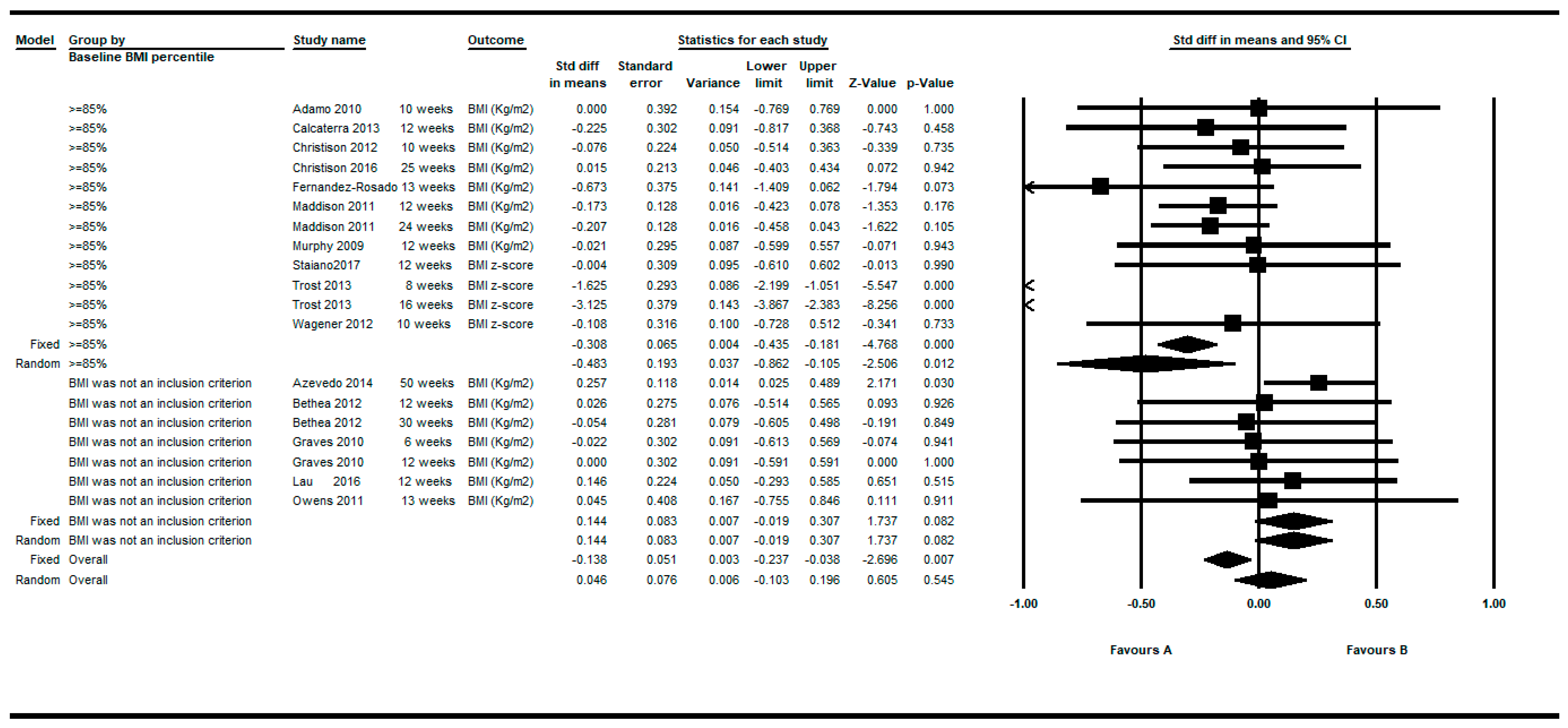
3.3. Between-Groups Differences in the BMI.
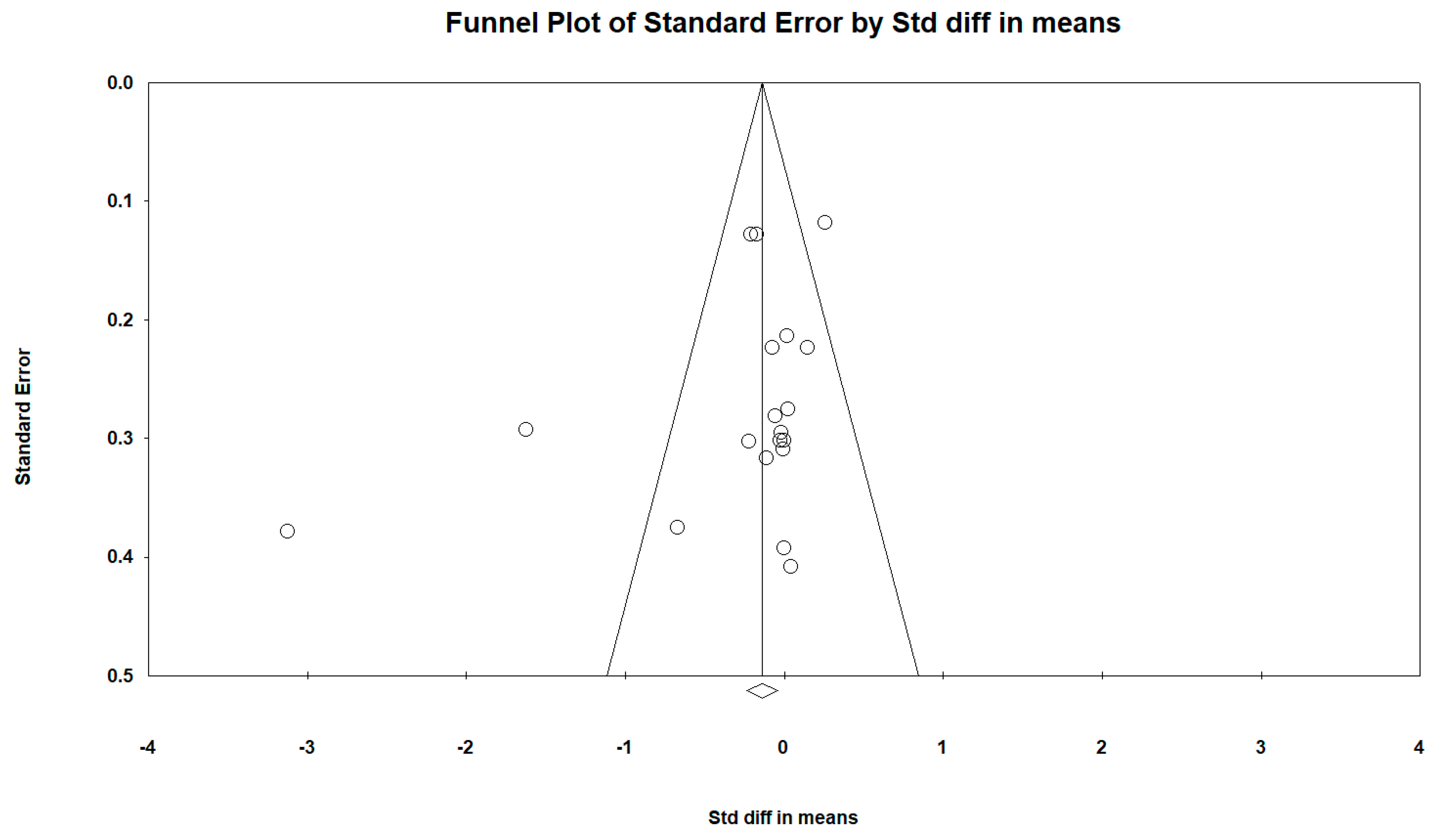
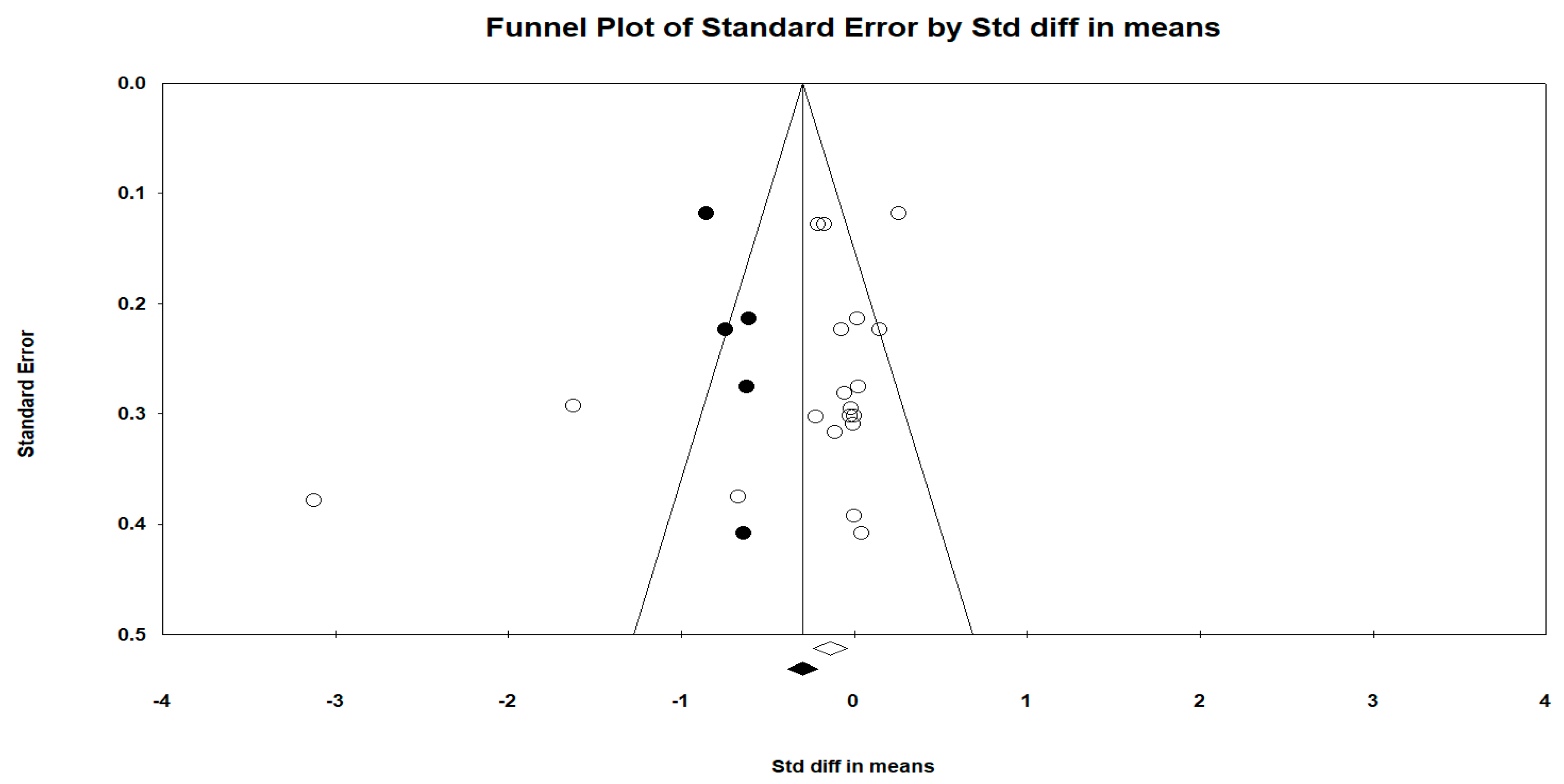
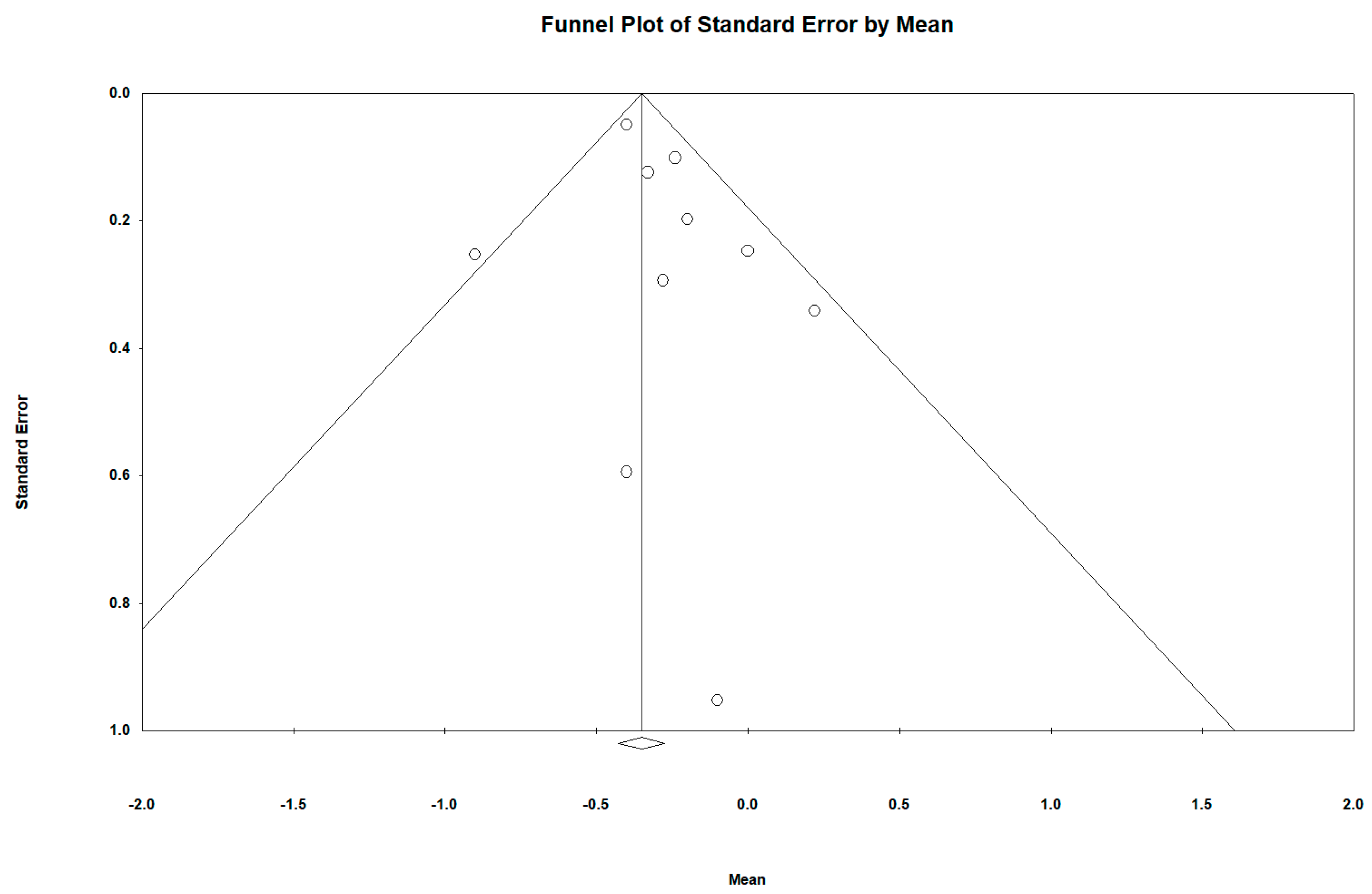
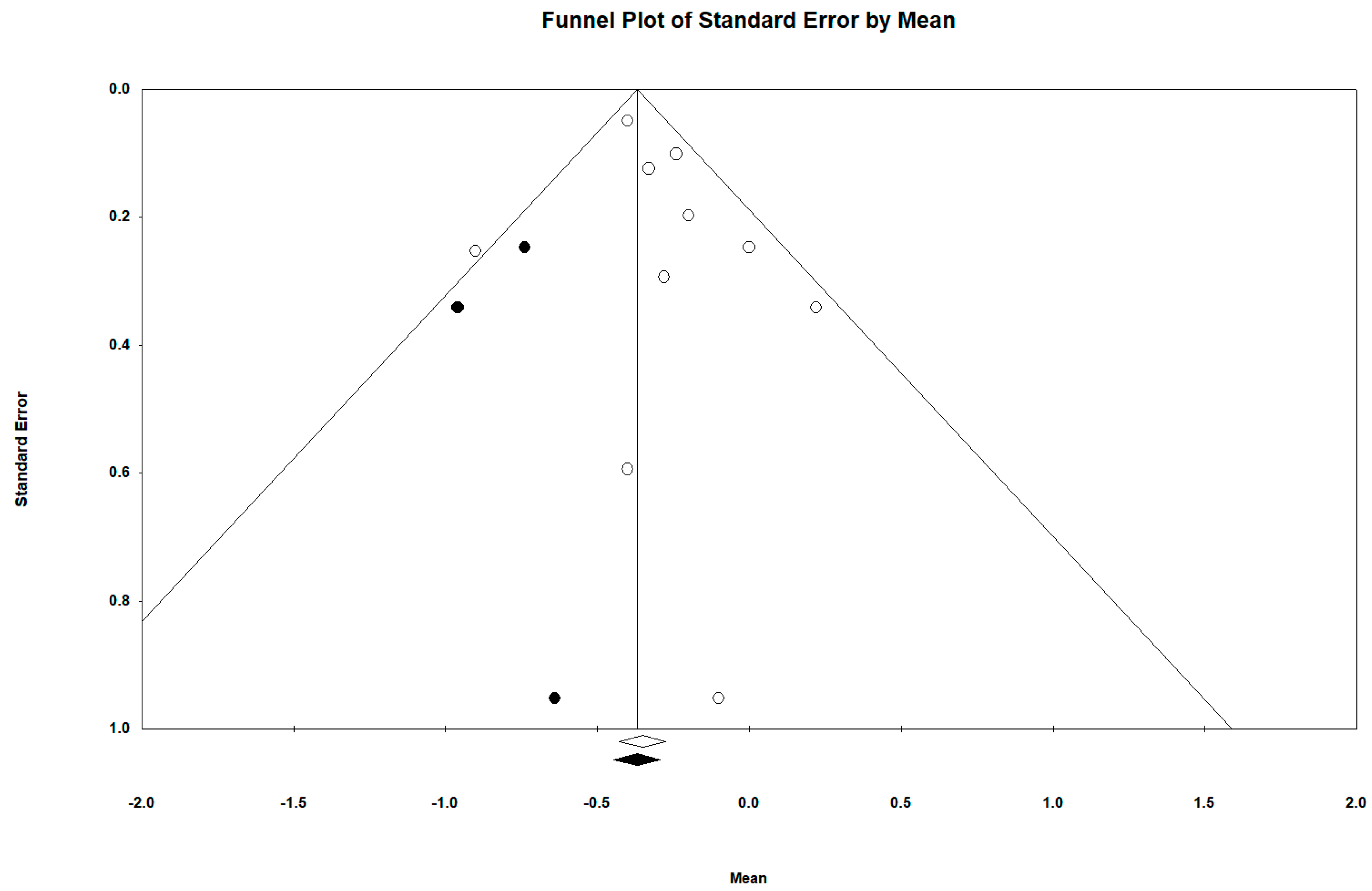
3.4. Publication Bias
3.5. Subgroup Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Fact Sheets. 2011. Available online: http://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight. (accessed on 3 January 2018).
- Mitchell, E.A.; Stewart, A.W.; Braithwaite, I.; Murphy, R.; Hancox, R.J.; Wall, C.; Beasley, R.; ISAAC Phase Three Study Group. Factors associated with body mass index in children and adolescents: An international cross-sectional study. PLoS ONE 2018, 13, e0196221. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; Visby, T.; Nyby, S.; Klingenberg, L.; Gregersen, N.T.; Tremblay, A.; Astrup, A.; Sjödin, A. Video game playing increases food intake in adolescents: A randomized crossover study. Am. J. Clin. Nutr. 2011, 93, 1196–1203. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.L.; Wilkosz, M.E. Efficacy of technology-based interventions for obesity prevention in adolescents: A systematic review. Adolesc. Health Med. Ther. 2014, 5, 159–170. [Google Scholar] [CrossRef] [PubMed]
- Lamboglia, C.M.G.F.; Silva, V.T.B.L.D.; Vasconcelos Filho, J.E.D.; Pinheiro, M.H.N.P.; Munguba, M.C.D.S.; Silva, F.V.I., Jr.; Paula, F.A.R.D.; Silva, C.A.B.D. Exergaming as a strategic tool in the fight against childhood obesity: A systematic review. J. Obes. 2013, 2013, 438364. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.G.; Chaput, J.P.; McFarlane, A.; Colley, R.C.; Thivel, D.; Biddle, S.J.; Maddison, R.; Leatherdale, S.T.; Tremblay, M.S. Active video games and health indicators in children and youth: A systematic review. PLoS ONE 2013, 8, e65351. [Google Scholar] [CrossRef] [PubMed]
- Ning, W.; Gao, Z.; Hart, M.A.; Zhang, Y.; Burley, H. A meta-analysis of physiological and psychological benefits of exergaming. Res. Quart. Exerc. Sport 2013, 84, A69. [Google Scholar]
- Peng, W.; Crouse, J.C.; Lin, J.H. Using active video games for physical activity promotion: A systematic review of the current state of research. Health Educ. Behav. 2013, 40, 171–192. [Google Scholar] [CrossRef] [PubMed]
- White, K.; Schofield, G.; Kilding, A.E. Energy expended by boys playing active video games. J Sci. Med. Sport 2011, 14, 130–134. [Google Scholar] [CrossRef]
- Bailey, B.W.; McInnis, K. Energy cost of exergaming: A comparison of the energy cost of 6 forms of exergaming. Arch. Pediatr. Adolesc. Med. 2011, 165, 597–602. [Google Scholar] [CrossRef]
- Jordan, M.; Donne, B.; Fletcher, D. Only lower limb controlled interactive computer gaming enables an effective increase in energy expenditure. Eur. J. Appl. Physiol. 2011, 111, 1465–1472. [Google Scholar] [CrossRef]
- Worley, J.R.; Rogers, S.N.; Kraemer, R.R. Metabolic responses to Wii Fit video games at different game levels. J. Strength Cond. Res. 2011, 25, 689–693. [Google Scholar] [CrossRef]
- Hurkmans, H.L.; Ribbers, G.M.; Streur-Kranenburg, M.F.; Stam, H.J.; Van den Berg-Emons, R.J. Energy expenditure in chronic stroke patients playing Wii Sports: A pilot study. J. Neuroeng. Rehabil. 2011, 8, 38. [Google Scholar] [CrossRef] [PubMed]
- Graves, L.E.; Ridgers, N.D.; Williams, K.; Stratton, G.; Atkinson, G.; Cable, N.T. The physiological cost and enjoyment of Wii Fit in adolescents, young adults, and older adults. J. Phys. Act. Health 2010, 7, 393–401. [Google Scholar] [CrossRef]
- Penko, A.L.; Barkley, J.E. Motivation and physiologic responses of playing a physically interactive video game relative to a sedentary alternative in children. Ann. Behav. Med. 2010, 39, 162–169. [Google Scholar] [CrossRef] [PubMed]
- Stroud, L.C.; Amonette, W.E.; Dupler, T.L. Metabolic responses of upper-body accelerometer-controlled video games in adults. Appl. Physiol. Nutr. Metab. 2010, 35, 643–649. [Google Scholar] [CrossRef] [PubMed]
- Leatherdale, S.T.; Woodruff, S.J.; Manske, S.R. Energy expenditure while playing active and inactive video games. Am. J. Health Behav. 2010, 34, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Graf, D.L.; Pratt, L.V.; Hester, C.N.; Short, K.R. Playing active video games increases energy expenditure in children. Pediatrics 2009, 124, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Lanningham-Foster, L.; Foster, R.C.; McCrady, S.K.; Jensen, T.B.; Mitre, N.; Levine, J.A. Activity-promoting video games and increased energy expenditure. J. Pediatr. 2009, 154, 819–823. [Google Scholar] [CrossRef] [PubMed]
- Graves, L.; Stratton, G.; Ridgers, N.D.; Cable, N.T. Energy expenditure in adolescents playing new generation computer games. Br. J. Sports Med. 2008, 42, 592–594. [Google Scholar]
- Adamo, K.B.; Rutherford, J.A.; Goldfield, G.S. Effects of interactive video game cycling on overweight and obese adolescent health. Appl. Physiol. Nutr. Metab. 2010, 35, 805–815. [Google Scholar] [CrossRef]
- Sween, J.; Wallington, S.F.; Sheppard, V.; Taylor, T.; Llanos, A.A.; Adams-Campbell, L.L. The role of exergaming in improving physical activity: A review. J. Phys. Act. Health 2014, 11, 864–870. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.; Cerin, E.; Baranowski, T. Active video games for youth: A systematic review. J. Phys. Act. Health 2011, 8, 724–737. [Google Scholar] [CrossRef] [PubMed]
- Biddiss, E.; Irwin, J. Active video games to promote physical activity in children and youth: A systematic review. Arch. Pediatr. Adolesc. Med. 2010, 164, 664–672. [Google Scholar] [CrossRef] [PubMed]
- Daley, A.J. Can exergaming contribute to improving physical activity levels and health outcomes in children? Pediatrics 2009, 124, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Lin, J.H.; Crouse, J. Is playing exergames really exercising? A meta-analysis of energy expenditure in active video games. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 681–688. [Google Scholar] [CrossRef] [PubMed]
- Guderian, B.; Borreson, L.A.; Sletten, L.E.; Cable, K.; Stecker, T.P.; Probst, M.A.; Dalleck, L.C. The cardiovascular and metabolic responses to Wii Fit video game playing in middle-aged and older adults. J. Sports Med. Phys. Fit. 2010, 50, 436–442. [Google Scholar]
- Bonetti, A.J.; Drury, D.G.; Danoff, J.V.; Miller, T.A. Comparison of acute exercise responses between conventional video gaming and isometric resistance exergaming. J. Strength Cond. Res. 2010, 24, 1799–1803. [Google Scholar] [CrossRef]
- Unnithan, V.B.; Houser, W.; Fernhall, B. Evaluation of the energy cost of playing a dance simulation video game in overweight and non-overweight children and adolescents. Int. J. Sports Med. 2006, 27, 804–809. [Google Scholar] [CrossRef]
- Kraft, J.A.; Russell, W.D.; Bowman, T.A.; Selsor, C.W., III; Foster, G.D. Heart rate and perceived exertion during self-selected intensities for exergaming compared to traditional exercise in college-age participants. J. Strength Cond. Res. 2011, 25, 1736–1742. [Google Scholar] [CrossRef]
- Graves, L.E.; Ridgers, N.D.; Atkinson, G.; Stratton, G. The effect of active video gaming on children’s physical activity, behavior preferences and body composition. Pediatr. Exerc. Sci. 2010, 22, 535–546. [Google Scholar] [CrossRef]
- Mellecker, R.R.; McManus, A.M. Energy expenditure and cardiovascular responses to seated and active gaming in children. Arch. Pediatr. Adolesc. Med. 2008, 162, 886–891. [Google Scholar] [CrossRef] [PubMed]
- Maddison, R.; Foley, L.; Mhurchu, C.N.; Jull, A.; Jiang, Y.; Prapavessis, H.; Rodgers, A.; Vander Hoorn, S.; Hohepa, M.; Schaaf, D. Feasibility, design and conduct of a pragmatic randomized controlled trial to reduce overweight and obesity in children: The electronic games to aid motivation to exercise (eGAME) study. BMC Public Health 2009, 9, 146. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, K.; Zhu, L.; Dawes, M.; Franco, J.; Huggins, A.; Igari, C.; Ranta, B.; Umez-Eronini, A. Wii health: A preliminary study of the health and wellness benefits of Wii Fit on university students. Br. J. Occup. Ther. 2011, 74, 262–268. [Google Scholar] [CrossRef]
- Madsen, K.A.; Yen, S.; Wlasiuk, L.; Newman, T.B.; Lustig, R. Feasibility of a dance videogame to promote weight loss among overweight children and adolescents. Arch. Pediatr. Adolesc. Med. 2007, 161, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Christison, A.; Khan, H.A. Exergaming for health: A community-based pediatric weight management program using active video gaming. Clin. Pediatr. 2012, 51, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Maddison, R.; Foley, L.; Ni Mhurchu, C.; Jiang, Y.; Jull, A.; Prapavessis, H.; Hohepa, M.; Rodgers, A. Effects of active video games on body composition: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 94, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.C.; Carson, L.; Neal, W.; Baylis, C.; Donley, D.; Yeater, R. Effects of an exercise intervention using Dance Dance Revolution on endothelial function and other risk factors in overweight children. Int. J. Pediatr. Obes. 2009, 4, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Owens, S.G.; Garner, J.C.; 3rd Loftin, J.M.; van Blerk, N.; Ermin, K. Changes in physical activity and fitness after 3 months of home Wii Fit use. J. Strength Cond. Res. 2011, 25, 3191–3197. [Google Scholar] [CrossRef] [PubMed]
- Wagener, T.L.; Fedele, D.A.; Mignogna, M.R.; Hester, C.N.; Gillaspy, S.R. Psychological effects of dance-based group exergaming in obese adolescents. Pediatr. Obes. 2012, 7, e68–e74. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S.; Horita, L.T.; Zbogar, D.; Scott, J.M.; Esch, B.T.; Rhodes, R.E. The health benefits of interactive video game exercise. Appl. Physiol. Nutr. Metab. 2007, 32, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Bethea, T.C.; Berry, D.; Maloney, A.E.; Sikich, L. Pilot study of an active screen time game correlates with improved physical fitness in minority elementary school youth. Games Health J. 2012, 1, 29–36. [Google Scholar] [CrossRef] [PubMed]
- National Collaborating Centre for Methods and Tools. Quality Assessment Tool for Quantitative Studies. 2016. Available online: http://www.ephpp.ca/PDF/Quality%20Assessment%20Tool_2010_2.pdf (accessed on 10 October 2018).
- National Collaborating Centre for Methods and Tools. Quality Assessment Tool for Quantitative Studies Dictionary. 2016. Available online: http://www.ephpp.ca/PDF/QADictionary_dec2009.pdf (accessed on 1 October 2018).
- Chalmers, T.C. Problems induced by meta-analyses. Stat. Med. 1991, 10, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Santibanez, M.; Bolumar, F.; Garcia, A.M. Occupational risk factors in Alzheimer’s disease: A review assessing the quality of published epidemiological studies. Occup. Environ. Med. 2007, 64, 723–732. [Google Scholar] [CrossRef]
- Peirson, L.; Fitzpatrick-Lewis, D.; Morrison, K.; Warren, R.; Usman Ali, M.; Raina, P. Treatment of overweight and obesity in children and youth: A systematic review and meta-analysis. CMAJ Open 2015, 3, E35–E46. [Google Scholar] [CrossRef] [PubMed]
- Waters, E.; De Silva-Sanigorski, A.; Burford, B.J.; Brown, T.; Campbell, K.J.; Gao, Y.; Armstrong, R.; Prosser, L.; Summerbell, C.D. Interventions for Preventing Obesity in Children; The Cochrane Library: Hoboken, NJ, USA, 2011. [Google Scholar]
- Whitlock, E.P.; O’Connor, E.A.; Williams, S.B.; Beil, T.L.; Lutz, K.W. Effectiveness of weight management interventions in children: A targeted systematic review for the USPSTF. Pediatrics 2010, 125, e396–e418. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DerSimonian, R.; Kacker, R. Random-effects model for meta-analysis of clinical trials: An update. Contemp. Clin. Trials 2007, 28, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Routledge: New York, NY, USA, 1977; Volume 7. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Introduction to Meta-Analysis; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.; Rothstein, H.R. Comprehensive Meta-Analysis Version 2; Biostat: Englewood, NJ, USA, 2005. [Google Scholar]
- Christison, A.L.; Evans, T.A.; Bleess, B.B.; Wang, H.; Aldag, J.C.; Binns, H.J. Exergaming for health: A randomized study of community-based exergaming curriculum in pediatric weight management. Games Health J. 2016, 5, 413–421. [Google Scholar] [CrossRef]
- Foley, L.; Jiang, Y.; Mhurchu, C.N.; Jull, A.; Prapavessis, H.; Rodgers, A.; Maddison, R. The effect of active video games by ethnicity, sex and fitness: Subgroup analysis from a randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 46. [Google Scholar] [CrossRef] [PubMed]
- Lau, P.W.; Wang, J.J.; Maddison, R. A randomized-controlled trial of school-based active videogame intervention on Chinese children’s aerobic fitness, physical activity level, and psychological correlates. Games Health J. 2016, 5, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Marker, A.M.; Beyl, R.A.; Hsia, D.S.; Katzmarzyk, P.T.; Newton, R.L. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr. Obes. 2017, 12, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Trost, S.G.; Sundal, D.; Foster, G.D.; Lent, M.R.; Vojta, D. Effects of a pediatric weight management program with and without active video games a randomized trial. JAMA Pediatr. 2014, 168, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, L.B.; Burges Watson, D.; Haighton, C.; Adams, J. The effect of dance mat exergaming systems on physical activity and health-related outcomes in secondary schools: Results from a natural experiment. BMC Public Health 2014, 14, 951. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Larizza, D.; Codrons, E.; De Silvestri, A.; Brambilla, P.; Abela, S.; Arpesella, M.; Vandoni, M. Improved metabolic and cardiorespiratory fitness during a recreational training program in obese children. J. Pediatr. Endocrinol. Metab. 2013, 26, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Rosado, F.F. Project to fight childhood overweight with video games. in child with social disadvantage. active assistance technology for health related behavior change. Ann. Nutr. Metab. 2013, 63, 1133. [Google Scholar]
- Paw, M.J.C.A.; Jacobs, W.M.; Vaessen, E.P.; Titze, S.; Van Mechelen, W. The motivation of children to play an active video game. J. Sci. Med. Sport 2008, 11, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, D.; Trakarnratanakul, N.; Smyth, B.; Caulfield, B. Effects of a wobble board-based therapeutic exergaming system for balance training on dynamic postural stability and intrinsic motivation levels. J. Orthop. Sports Phys. Ther. 2010, 40, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Bonis, J. Acute wiiitis. NEJM 2007, 356, 2431–2432. [Google Scholar] [CrossRef]
- Peek, A.C.; Ibrahim, T.; Abunasra, H.; Waller, D.; Natarajan, R. White-out from a wii: Traumatic haemothorax sustained playing Nintendo™ Wii. Ann. R. Coll. Surg. Engl. 2008, 90, W9–W10. [Google Scholar] [CrossRef] [PubMed]
- Fischer, P.; Greitemeyer, T.; Kastenmuller, A.; Vogrincic, C.; Sauer, A. The effects of risk-glorifying media exposure on risk-positive cognitions, emotions, and behaviors: A meta-analytic review. Psychol. Bull. 2011, 137, 367–390. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Egger, M.; Moher, D. Addressing Reporting Biases; Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series; John Wiley & Sons: Hoboken, NJ, USA, 2008; pp. 297–333. [Google Scholar]



















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria |
| • Children and adolescents (≤18 years old). Design: clinical trials both controlled (randomized or quasi-randomized) and non-controlled. • Intervention based on active video games. • Language: written in English or Spanish. • Information on at least one determination of the BMI (Kg/m2, Z score, or percentile) both pre and post intervention, or differences between groups in the BMI in case of controlled studies. |
| Exclusion Criteria |
| • Adults (≥19 years <65 years) or elderly (≥65 years). • Non-epidemiological studies: clinical cases of only one person. |
| First Author. Publication Year. | Country | Study Design | Study Population | Duration (Weeks) | Procedure | Main Results | Other Results |
|---|---|---|---|---|---|---|---|
| Adamo et al., 2010 [21] | Canada | Randomized controlled trial. | 26 participants. 12–17 years. Inclusion criterion: BMI ≥ 85th percentile with at least 1 metabolic complication; or BMI ≥ 95th percentile. | 10 weeks | Intervention group (n = 13): They used active videogame (GameBike). Control group (n = 13): They used stationary cycling while listening to music. Both: Sessions 60 minutes 2 times per week during 10 weeks. | BMI (kg/m2): Intervention group: Pre: 35.5 ± 9.3 Post: 35.5 ± 9.7 Control group: Pre: 39.9 ± 8.9 Post: 39.4 ± 8.9 BMI percentile: Intervention group: Pre: 97.8 ± 1.4 Post: 97.5 ± 1.8 Control group: Pre: 97.8 ± 2.7 Post: 97.8 ± 2.3 | Heart rate. Intervention group: Pre: 177.1 ± 21.4 Post: 169.1 ± 19.2 Control group: Pre: 172.2 ± 16 Post: 163.2 ± 23.1 |
| Azevedo et al., 2014 [63] | UK | Non-randomized controlled trial. | 189 participants. 11–13 years. BMI was not an inclusion criterion: Average baseline BMI intervention group = 20.4; DE [4.2]. Average baseline BMI control group = 19.5; DE [3.3]. | 50 weeks | Intervention group (n = 117). They used dancing active videogame (dance mat). Control group (n = 72). Non-intervention. | BMI (kg/m2): Intervention group: Pre: 20.4 ± 4.2 Post: 21.5 ± 4.4 Control group: Pre: 19.5 ± 3.3 Post: 21.3 ± 3.7 | |
| Bethea et al., 2012 [42] | USA | Non-controlled randomized trial. | 28 participants. 9–11 years. Only men. BMI was not an inclusion criterion: Average baseline BMI group = 19.8; DE [3.9]. Average baseline BMI percentile = 68.4; DE [28.7]. | 12–30 weeks | Intervention group (n = 28): They used dancing active videogame DDR (Dance Dance Revolution) 3 days per week about 30 min. | BMI (kg/m2): Intervention group: Pre: 19.8 ± 3.9 Post (12 weeks): 19.9 ± 3.9 Post (30 weeks): 19.6 ± 3.5 BMI z-score: Intervention group: Pre: 0.71 ± 1.05 Post (12 weeks): 0.66 ± 1.1 Post (30 weeks): 0,55 ± 1 BMI percentile: Intervention group: Pre: 68.4 ± 28.7 Post (12 weeks): 67.1 ± 30.6 Post (30 weeks): 64.5 ± 28.8 | Heart rate. Intervention group: Pre: 86 ± 11 Post: 86 ± 15 |
| Calcaterra et al., 2013 [64] | Italy | Non-controlled randomized trial | 22 participants. 9–16 years. Inclusion criterion: BMI ≥ 95th percentile. | 12 weeks | Intervention group (n = 22): Training program for sedentary obese children, including active video games. | BMI (kg/m2): Intervention group: Pre: 32.9 ± 4.3 Post: 31.9 ± 4.6 BMI z-score: Intervention group: Pre: 2.52 ± 0.55 Post: 2.37 ± 0.67 | VO2 max (maximal oxygen consumption) Intervention group: Pre: 47.5 ± 6.5 Post: 51.3 ± 6.3 |
| Christison et al., 2012 [36] | USA | Non- controlled randomized trial | 40 participants. 8–16 years. Inclusion criterion: BMI ≥ 85th percentile. | 10 weeks | Intervention group: The Exergaming for Health program was designed to be multidisciplinary and of moderate intensity. The curriculum had 3 main components: facilitated activity with exergaming, nutrition education, and behavioral management discussions. Subjects participated in 10 weekly 1hour facilitated activity sessions. There were five one-hour exergaming sessions in the first half of the program and five one-hour combined exergaming/traditional exercise sessions during the latter portion of the program. | BMI (kg/m2): Intervention group: Pre: 31.07 ± 6.41 Post: 30.59 ± 6.25 BMI z-score: Intervention group: Pre: 2.24 ± 0.41 Post: 2.17 ± 0.49 | |
| Christison et al., 2016 [58] | USA | Randomized controlled trial. | 48 participants 8–12 years. Inclusion criterion: Overweight or obese | 25 weeks | Intervention group (n = 35): Two main components: facilitated group activity with active videogaming and family-centered didactics focused on improved nutrition education and behavioral aspects of lifestyle change. Control group (n = 13): Non-intervention | BMI (kg/m2): Intervention group: Pre: 28.8 ± 6.4 Post (25 weeks): 28.9 ± 6.6 Control group: Pre: 29.5 ± 4.8 Post (25 weeks): 29.9 ± 4.8 BMI z-score: Intervention group: Pre: 2.13 ± 0.4 Post (25 weeks): 2.07 ± 0.5 Control group: Pre: 2.25 ± 0.3 Post (25 weeks): 2.25 ± 0.3 | Heart rate. Intervention group: Pre: 87 ± 12 Post: 77 ± 10 Control group: Pre: 87.2 ± 8.7 Post: 81.2 ± 9.9 |
| Fernández Rosado. 2013 [65] | Spain | Non-controlled randomized trial | 15 participants 7–13 years. Inclusion criterion: Obese | 13 weeks | Intervention group (n = 15): They provided 60 minutes PlayStation Eye Toy USB camera maximum day. | BMI (kg/m2): Intervention group: Pre: 27.91 ± 2.55 Post: 25.84 ± 3.52 | |
| Foley et al., 2014 [59] | New Zealand | Randomized controlled trial. | 322 participants. 10–14 years. Inclusion criterion: Overweight or obese. | 24 weeks | Intervention group (n = 160): They used active videogame (PlayStation Eye Toy USB). Control group (n = 162): Non-intervention | BMI (kg/m2): Intervention group: Pre: 25.64 ± 4.08 Control group: Pre: 25.75 ± 4.25 BMI z-score: Intervention group: Pre: 1.26 ± 1.11 Control group: Pre: 1.25 ± 1.1 | |
| Graves et al., 2010a [31] | UK | Randomized controlled trial. | 42 participants 8–10 years. BMI was not an inclusion criterion: Average baseline BMI intervention group = 18.9; DE [4.5]. Average baseline BMI control group= 19.7; DE [4.3]. | 6–12 weeks | Intervention group (n = 22): They used active videogame. Control group (n = 20): They used traditional sedentary videogame. | BMI (kg/m2): Intervention group: Pre: 18.9 ± 4.5 Post (6 weeks): 18.8 ± 4.5 Post (12 weeks): 18.9 ± 4.6 Control group: Pre: 19.7 ± 4.3 Post (6 weeks): 19.9 ± 4.3 Post (12 weeks): 19.7 ± 4.2 | |
| Lau et al., 2016 [60] | China | Randomized controlled trial. | 80 participants 8–11 years. | 12 weeks | Intervention group (n = 40): They played an active videogame, Xbox 360, twice per week during after-school hours, each for 60 min over 12 weeks in duration. Control group (n= 40): Non-intervention | BMI (kg/m2): Intervention group: Pre: 19.41 ± 3.63 Post (12 weeks): 19.95 ± 3.78 Control group: Pre: 19.75 ± 3.61 Post (12 weeks): 20.04 ± 3.51 | VO2 max (maximal oxygen consumption) Intervention group: Pre: 42.93 ± 1.47 Post: 45.21 ± 2.15 Control group: Pre: 42.62 ± 1.75 Post:43.38 ± 2.36 |
| Maddison et al., 2011 [37] | New Zealand | Randomized controlled trial. | 258 participants 10–14 years. Inclusion criterion: Overweight. | 12–24 weeks | Intervention group (n = 123): They used active videogame. (PlayStation Eye Toy USB). Control group (n = 135): Non-intervention | BMI (kg/m2): Intervention group: Pre: 25.6 ± 4.1 Post (12 weeks): 24.9 ± 4 Post (24 weeks): 24.8 ± 3.6 Control group: Pre: 25.8 ± 4.3 Post (12 weeks): 25.5 ± 4.3 Post (24 weeks): 25.8 ± 4.2 BMI z-score: Intervention group: Pre: 1.3 ± 1.1 Post (12 weeks): 1.1 ± 1.2 Post (24 weeks): 1.1 ± 1.1 Control group: Pre: 1.3 ± 1.1 Post (12 weeks): 1.3 ± 1.1 Post (24 weeks): 1.3 ± 1 | |
| Murphy et al., 2009 [38] | USA | Randomized controlled trial. | 35 participants 7–12 years. Inclusion criterion: BMI ≥ 85th percentile. | 12 weeks | Intervention group (n = 23): They used active videogame. DDR (Dance Dance Revolution), 1 session per week. Control group (n = 12): Non-intervention | BMI (kg/m2): Intervention group: Pre: 27.9 ± 4.8 Post: 27.8 ± 4.7 Control group: Pre: 31.8 ± 5 Post: 32.1 ± 4.9 | VO2 max (maximal oxygen consumption) Intervention group: Pre: 27.1 ± 5.4 Post: 29.5 ± 4.5 Control group: Pre: 25.6 ± 5.4 Post: 24.3 ± 4.8 |
| Owens et al., 2011 [39] | USA | Non-controlled randomized trial | 20 participants 12 children (8–13 years.) BMI was not an inclusion criterion: Average baseline BMI group = 19.4; DE [4.4]. | 13 weeks | Intervention group: They used active videogame Wii FitTM during 13 weeks daily. | BMI (kg/m2): Intervention group: Pre: 19.4 ± 4.4 Post: 19.6 ± 4.4 | VO2 max (maximal oxygen consumption) Intervention group: Pre: 34.3 ± 9.6 Post: 38.4 ± 8.6 |
| Staiano et al., 2017 [61] | USA | Randomized controlled trial. | 38 participants Girls. 14–18 years. Inclusion criterion: Overweight or obese. | 12 weeks | Intervention group (n = 20): They practiced three sessions of 1 h dance active video per week for 12 weeks. Control group (n = 18): Non-intervention | BMI z-score: Intervention group: Pre: 2.1 ± 0.5 Post: 2.098 ± 0.5 Control group: Pre: 2.1 ± 0.5 Post: 2.104 ± 0.501 | |
| Trost et al., 2013 [62] | USA | Randomized controlled trial. | 69 participants 8–12 years. Inclusion criterion: BMI ≥ 85th percentile. | 8–16 weeks | Intervention group (n = 31): They used two types of active video games during 16 weeks. Control group (n = 38): They performed a program of exercise without active video game. | BMI z-score: Intervention group: Pre: 2.14 ± 0.08 Post (8 weeks): 2.01 ± 0.08 Post (16 weeks): 1.89 ± 0.08 Control group: Pre: 2.16 ± 0.07 Post (8 weeks): 2.1 ± 0.07 Post (16 weeks): 2.05 ± 0.07 | |
| Wagener et al., 2012 [40] | USA | Randomized controlled trial. | 40 participants. 12–18 years. Inclusion criterion: BMI ≥ 95th percentile. | 10 weeks | Intervention group (n = 20): They used dancing active videogame. (dance pads) 3 times per week 40 min the first session, and 75 min for following sessions. Control group (n = 20): Non-intervention | BMI z-score: Intervention group: Pre: 3.15 ± 0.19 Post: 3.13 ± 0.18 Control group: Pre: 3.15 ± 0.2 Post: 3.12 ± 0.2 |
| Selection Bias (0–2 Points) | Study Design (0–2 Points) | Confounders (0–2 Points) | Blinding (0–2 Points) | Data Collection Methods (0–2 Points) | Withdrawals and Dropouts (0–2 Points) | Final Decision Based on the Dictionary | Final Mark (RCT and CCT 0–12 Points) (Pre + Post 0–10 Points) | |
|---|---|---|---|---|---|---|---|---|
| Adamo 2010 | W (0) | S (2) | W (0) | W (0) | S (2) | S (2) | W | 6 |
| Azevedo 2014 | W (0) | S (2) | S (2) | W (0) | S (2) | W (0) | W | 6 |
| Bethea 2012 | W (0) | M (1) | NA | W (0) | S (2) | S (2) | W | 5 |
| Calcaterra 2012 | W (0) | M (1) | NA | W (0) | S (2) | W (0) | W | 3 |
| Christison 2012 | M (1) | M (1) | NA | W (0) | W (0) | S (2) | W | 4 |
| Christison 2016 | S (2) | S (2) | M (1) | M (1) | S (2) | M/W (0.5) * | S/M * | 8.5 |
| Fernández-Rosado 2013 | W (0) | M (1) | NA | W (0) | W (0) | W (0) | W | 1 |
| Foley 2014 | M (1) | S (2) | S (2) | W (0) | W (0) | W (0) | W | 5 |
| Graves 2010 | W (0) | S (2) | S (2) | W (0) | S (2) | M (1) | W | 7 |
| Lau 2016 | M (1) | S (2) | W (0) | W (0) | S (2) | S (2) | W | 7 |
| Maddison 2011 | M (1) | S (2) | S (2) | W (0) | S (2) | S/M (1.5) * | M | 8.5 |
| Murphy, 2009 | M (1) | S (2) | S (2) | W (0) | W (0) | W (0) | W | 5 |
| Owens 2011 | W (0) | M (1) | NA | W (0) | S (2) | S (2) | W | 5 |
| Staiano 2017 | M (1) | S (2) | S (2) | M (1) | S (2) | S (2) | S | 10 |
| Trost 2013 | W (0) | S (2) | S (2) * | W (0) | S (2) | S (2) | W | 8 |
| Wagener 2012 | W (0) | S (2) | S (2) | M (1) | M (1) | S (2) | M | 8 |
| Intervention Group | N of Determinations | Heterogeneity | |||||
|---|---|---|---|---|---|---|---|
| Q | df | p (χ2) | I2 (%) | τ2 | τ | ||
| All determinations (15 studies, 4 with two determinations) | 19 | 105.33 | 18.00 | 0.00 | 82.91 | 0.25 | 0.50 |
| 1 arm | 6 | 2.83 | 5.00 | 0.72 | 0.00 | 0.00 | 0.00 |
| 2 arms | 13 | 102.49 | 12.00 | 0.00 | 88.29 | 0.33 | 0.58 |
| Control Group | N of Determinations | Heterogeneity | |||||
|---|---|---|---|---|---|---|---|
| Q | df | p (χ 2) | I2 (%) | τ2 | τ | ||
| All determinations (10 studies, three with two determinations) | |||||||
| All studies | 13 | 59.45 | 12.00 | 0.00 | 79.81 | 0.19 | 0.44 |
| No intervention in the control group | 8 | 8.20 | 7.00 | 0.31 | 14.71 | 0.007 | 0.08 |
| Any intervention not based on active video games | 5 | 24.98 | 4.00 | 0.00 | 83.98 | 0.46 | 0.67 |
| Difference between Groups. BMI (Kgr/m2). | N of Determinations | Heterogeneity | |||||
|---|---|---|---|---|---|---|---|
| Q | df | p (χ2) | I2 (%) | τ2 | τ | ||
| All determinations (eight studies, two with two determinations) | 10 | 12.40 | 9.00 | 0.19 | 27.44 | 0.01 | 0.10 |
| Difference between Groups. IMC z-Score. | N of Studies | Heterogeneity | |||||
|---|---|---|---|---|---|---|---|
| Q | df | p (χ2) | I2 (%) | τ2 | τ | ||
| All determinations (6 studies, 2 with two determinations) | 8 | 257.18 | 7.00 | 0.00 | 97.28 | 0.01 | 0.09 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hernández-Jiménez, C.; Sarabia, R.; Paz-Zulueta, M.; Paras-Bravo, P.; Pellico, A.; Ruiz Azcona, L.; Blanco, C.; Madrazo, M.; Agudo, M.J.; Sarabia, C.; et al. Impact of Active Video Games on Body Mass Index in Children and Adolescents: Systematic Review and Meta-Analysis Evaluating the Quality of Primary Studies. Int. J. Environ. Res. Public Health 2019, 16, 2424. https://doi.org/10.3390/ijerph16132424
Hernández-Jiménez C, Sarabia R, Paz-Zulueta M, Paras-Bravo P, Pellico A, Ruiz Azcona L, Blanco C, Madrazo M, Agudo MJ, Sarabia C, et al. Impact of Active Video Games on Body Mass Index in Children and Adolescents: Systematic Review and Meta-Analysis Evaluating the Quality of Primary Studies. International Journal of Environmental Research and Public Health. 2019; 16(13):2424. https://doi.org/10.3390/ijerph16132424
Chicago/Turabian StyleHernández-Jiménez, Carlos, Raquel Sarabia, María Paz-Zulueta, Paula Paras-Bravo, Amada Pellico, Laura Ruiz Azcona, Cristina Blanco, María Madrazo, María Jesus Agudo, Carmen Sarabia, and et al. 2019. "Impact of Active Video Games on Body Mass Index in Children and Adolescents: Systematic Review and Meta-Analysis Evaluating the Quality of Primary Studies" International Journal of Environmental Research and Public Health 16, no. 13: 2424. https://doi.org/10.3390/ijerph16132424
APA StyleHernández-Jiménez, C., Sarabia, R., Paz-Zulueta, M., Paras-Bravo, P., Pellico, A., Ruiz Azcona, L., Blanco, C., Madrazo, M., Agudo, M. J., Sarabia, C., & Santibáñez, M. (2019). Impact of Active Video Games on Body Mass Index in Children and Adolescents: Systematic Review and Meta-Analysis Evaluating the Quality of Primary Studies. International Journal of Environmental Research and Public Health, 16(13), 2424. https://doi.org/10.3390/ijerph16132424