Assessment of Occupational Safety and Hygiene Perception among Afro-Caribbean Hair Salon Operators in Manchester, United Kingdom



Abstract
:1. Introduction
2. Importance of the Study Rationale
3. Materials and Methods
3.1. Selection of Participants
3.2. Questionnaire Design
3.3. Environmental Monitoring of Selected Variables
3.4. Environmental Sampling Methods
4. Results
4.1. Questionnaire Analysis
4.2. Indoor Air Sampling
4.3. Impact of Work Environment on Pollutants Generation
5. Discussion
6. Conclusions
Recommendations
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van der Wal, J.F.; Hoogeveen, A.W.; Moons, A.M.; Wouda, P. Investigation on the exposure of hairdressers to chemical agents. Environ. Int. 1997, 23, 433–439. [Google Scholar] [CrossRef]
- Hollund, B.E.; Moen, B.E. Chemical exposure in hairdresser salons: Effect of local exhaust ventilation. Ann. Occup. Hyg. 1998, 42, 277–281. [Google Scholar] [CrossRef]
- Nemer, M.; Kristensen, P.; Nijem, K.; Bjertness, E.; Skare, Ø.; Skogstad, M. Lung function and respiratory symptoms among female hairdressers in Palestine: A 5-year prospective study. BMJ Open 2015, 5, e007857. [Google Scholar] [CrossRef]
- De Gennaro, G.; de Gennaro, L.; Mazzone, A.; Porcelli, F.; Tutino, M. Indoor air quality in hair salons: Screening of volatile organic compounds and indicators based on health risk assessment. Atmos. Environ. 2014, 83, 119–126. [Google Scholar] [CrossRef]
- European Commission. Commission decision 2006/257/EC of 9 February 2006 amending Decision 96/335/EC Establishing an Inventory and a Common Nomenclature of Ingredients Employed in Cosmetic Products. Official Journal of the European Union. 2006. Available online: https://publications.europa.eu/en/publication-detail/-/publication/db30de80-11f8-4358-b1d6-e38d6cf96625 (accessed on 8 August 2019).
- Mandiracioglu, A.; Kose, S.; Gozaydin, A.; Turken, M.; Kuzucu, L. Occupational health risks of barbers and coiffeurs in Izmir. Indian J. Occup. Environ. Med. 2009, 13, 92–96. [Google Scholar] [CrossRef]
- Liu, N.; Xu, L.; Cai, Y. Methyl siloxanes in barbershops and residence indoor dust and the implication for human exposures. Sci. Total Environ. 2018, 618, 1324–1330. [Google Scholar] [CrossRef]
- Lysdal, S.H.; Søsted, H.; Andersen, K.E.; Johansen, J.D. Hand eczema in hairdressers: A Danish register-based study of the prevalence of hand eczema and its career consequences. Contact Dermatitis. 2011, 65, 151–158. [Google Scholar] [CrossRef]
- Bradshaw, L.; Harris-Roberts, J.; Bowen, J.; Rahman, S.; Fishwick, D. Self-reported work-related symptoms in hairdressers. Occup. Med. 2011, 61, 328–334. [Google Scholar] [CrossRef] [Green Version]
- Scranton, A. Beauty and Its beast: Unmasking the Impacts of Toxic Chemicals on Salon Workers. Womens Voices for the Earth. 2008. Available online: https://www.womensvoices.org/wp-content/uploads/2014/11/Beauty-and-Its-Beast.pdf (accessed on 20 May 2018).
- Monakhova, Y.B.; Kuballa, T.; Mildau, G.; Kratz, E.; Keck-Wilhelm, A.; Tschiersch, C.; Lachenmeier, D.W. Formaldehyde in hair straightening products: Rapid 1H NMR determination and risk assessment. Int. J. Cosmet. Sci. 2013, 35, 201–220. [Google Scholar] [CrossRef]
- Lind, M.L.; Albin, M.; Brisman, J.; Diab, K.K.; Lillienberg, L.; Mikoczy, Z.; Nielsen, J.; Rylander, L.; Torén, K.; Meding, B. Incidence of hand eczema in female Swedish hairdressers. Occup. Environ. Med. 2007, 64, 191–195. [Google Scholar] [CrossRef]
- Ibler, K.S.; Jemec, G.B.; Diepgen, T.L.; Gluud, C.; Hansen, J.L.; Winkel, P.; Thomsen, S.F.; Agner, T. Skin care education and individual counselling versus treatment as usual in healthcare workers with hand eczema: Randomised clinical trial. BMJ 2012, 345, e7822. [Google Scholar] [CrossRef]
- Wiszniewska, M.; Walusiak-Skorupa, J. Recent trends in occupational contact dermatitis. Curr. Allergy Asthma Rep. 2015, 15, 43. [Google Scholar] [CrossRef]
- Chang, C.J.; Cheng, S.F.; Chang, P.T.; Tsai, S.W. Indoor air quality in hairdressing salons in Taipei. Indoor Air 2018, 28, 173–180. [Google Scholar] [CrossRef]
- Steengaard, S.S.; Bregnhøj, A.; Johansen, J.D. Hand eczema among hairdressing apprentices in Denmark following a nationwide prospective intervention programme: 6-year follow-up. Contact Dermatitis 2016, 75, 32–40. [Google Scholar] [CrossRef]
- Hairdressers of the World Unite against Hidden Dangers of the Salon. Available online: https://www.theguardian.com/lifeandstyle/2017/mar/04/hidden-dangers-hairdressing-salon-block-eu-safety-rules (accessed on 5 May 2018).
- Veiersted, K.B.; Gould, K.S.; Østerås, N.; Hansson, G.Å. Effect of an intervention addressing working technique on the biomechanical load of the neck and shoulders among hairdressers. Appl. Ergon. 2008, 39, 183–190. [Google Scholar] [CrossRef]
- Chen, H.C.; Chang, C.M.; Liu, Y.P.; Chen, C.Y. Ergonomic risk factors for the wrists of hairdressers. Appl. Ergon. 2010, 41, 98–105. [Google Scholar] [CrossRef]
- English, C.J.; Maclaren, W.M.; Court-Brown, C.; Hughes, S.P.F.; Porter, R.W.; Wallace, W.A.; Graves, R.J.; Pethick, A.J.; Soutar, C.A. Relations between upper limb soft tissue disorders and repetitive movements at work. Am. J. Ind. Med. 1995, 27, 75–90. [Google Scholar] [CrossRef]
- Mancini, L.; Figliomeni, M.; Puccinelli, C. A descriptive survey on microbiological risk in beauty salons. Microchem. J. 2018, 136, 223–226. [Google Scholar] [CrossRef]
- Gallicchio, L.; Miller, S.; Greene, T.; Zacur, H.; Flaws, J.A. Premature ovarian failure among hairdressers. Hum. Reprod. 2009, 24, 2636–2641. [Google Scholar] [CrossRef]
- Halliday-Bell, J.A.; Gissler, M.; Jaakkola, J.J. Work as a hairdresser, cosmetologist, and adverse pregnancy outcomes. Occup. Med. 2009, 59, 180–184. [Google Scholar] [CrossRef]
- EU-OSHA, European Agency for Safety and Health at Work. Occupational Health and Safety in the Hairdressing Sector. 2014. Available online: https://osha.europa.eu/en/publications/literature_reviews/occupational-health-and-safety-in-the-hairdressing-sector (accessed on 8 August 2019).
- Ronda, E.; Hollund, B.E.; Moen, B.E. Airborne exposure to chemical substances in hairdresser salons. Environ. Monit. Assess. 2009, 153, 83–93. [Google Scholar] [CrossRef]
- Visser, M.J.; Verberk, M.M.; van Dijk, F.J.; Bakker, J.G.; Bos, J.D.; Kezic, S. Wet work and hand eczema in apprentice nurses; part I of a prospective cohort study. Contact Dermatitis 2014, 70, 44–55. [Google Scholar] [CrossRef]
- Arezes, P.M.; Baptista, J.S.; Barroso, M.P.; Carneiro, P.; Costa, N.; Melo, R.B.; Miguel, A.S.; Perestrelo, G. Prevalence of Skeletal Muscle injuries in hairdressers in the district of Setubal. In Occupational Safety and Hygiene III, 1st ed.; CRC Press: London, UK, 2015; pp. 355–357. ISBN 978-1-138-02765-7. [Google Scholar]
- HSE 1992. Workplace (Health, Safety and Welfare) Regulations 1992 L24. Available online: http://www.hse.gov.uk/pUbns/priced/l24.pdf (accessed on 10 July 2018).
- Indoor Air Quality and Ventilation—CIBSE Knowledge Series: KS17. Available online: https://app.knovel.com/hotlink/toc/id:kpIAQVCIB3/indoor-air-quality-ventilation/indoor-air-quality-ventilation (accessed on 10 July 2018).
- HSG20: General Ventilation in the Work Place. Guidance for Employers, 2000. Available online: http://www.ucu.org.uk/media/1358/General-ventilation---guidance-for-employers-HSG202/pdf/HSG202_-_Ventilation.pdf (accessed on 8 August 2019).
- Goldin, L.J.; Ansher, L.; Berlin, A.; Cheng, J.; Kanopkin, D.; Khazan, A.; Kisivuli, M.; Lortie, M.; Peterson, E.B.; Pohl, L.; Porter, S. Indoor air quality survey of nail salons in Boston. J. Immigr. Minor. Health 2014, 16, 508–514. [Google Scholar] [CrossRef]
- Mølhave, L.; Clausen, G.; Berglund, B.; De Ceaurriz, J.; Kettrup, A.; Lindvall, T.; Maroni, M.; Pickering, A.C.; Risse, U.; Rothweiler, H.; Seifert, B. Total volatile organic compounds (TVOC) in indoor air quality investigations. Indoor Air 1997, 7, 225–240. [Google Scholar] [CrossRef]
- Behroozy, A.; Keegel, T.G. Wet-work exposure: A main risk factor for occupational hand dermatitis. Saf. Health Work 2014, 5, 175–180. [Google Scholar] [CrossRef]
- English, J.S.C. Current concepts of irritant contact dermatitis. Occup. Environ. Med. 2004, 61, 722–726. [Google Scholar] [CrossRef] [Green Version]
- Work-related Skin Disease in Great Britain, 2018. Available online: http://www.hse.gov.uk/statistics/causdis/dermatitis/skin.pdf (accessed on 2 May 2018).
- Oikawa, D.; Takeuchi, W.; Murata, S.; Takahashi, K.; Sekine, Y. Measurement of concentrations of thioglycolic acid, dithiodiglycolic acid and ammonia in indoor air of a beauty salon. J. Occup. Health 2012, 54, 370–375. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | n (%) | Mean | Median | Standard Deviation |
|---|---|---|---|---|
| Gender | ||||
| Male | 35 (22.9) | 1.81 | 2 | 0.483 |
| Female | 112 (73.2) | |||
| Prefer not to say | 6 (3.9) | |||
| Age in years | ||||
| 18–20 | 12 (7.8) | |||
| 21–25 | 19 (12.4) | 4.43 | 4 | 1.691 |
| 26–30 | 27 (17.6) | |||
| 31–35 | 30 (19.6) | |||
| 36–40 | 25 (16.3) | |||
| 41–45 | 17 (11.1) | |||
| 46–50 | 14 (9.2) | |||
| 5–above | 6 (3.9) | |||
| Prefer not to say | 3 (2.0) | |||
| Years working in the hair salon industry | ||||
| 1–5 | 67 (43.8) | |||
| 6–10 | 49 (32) | 2 | 2 | 1.187 |
| 11–15 | 17 (11.1) | |||
| 16–20 | 10 (6.5) | |||
| 21–above | 10 (6.5) |
| Occupational Disease/Injury | n (%) | Frequency of Occurrence (n) | ||
|---|---|---|---|---|
| Always | Sometimes | Most Time | ||
| Respiratory allergy | 38 (24.8) | 3 | 20 | 15 |
| Contact dermatitis, | 47 (30.7) | 4 | 18 | 25 |
| Itchy eyes and nose | 68 (44.4) | 5 | 36 | 27 |
| Shoulder, neck and back pain | 60 (39.2) | 2 | 35 | 23 |
| Joint aches | 30 (19.6) | 2 | 12 | 16 |
| Headache, dizziness and nausea | 57 (37.3) | 4 | 27 | 26 |
| Swollen joints: wrist, ankles and legs | 42 (27.5) | 5 | 19 | 18 |
| Age | Reported Occupation Aliments Reported (%) | ||||||
|---|---|---|---|---|---|---|---|
| Allergies | Itchy Eyes and Nose | Contact Dermatitis | Swollen Ankle and Leg | Joint Ache | Shoulder, Neck and Back Pain | Headache, Dizziness and Nausea | |
| 21–25 | 3 (7.9) | 9 (13.2) | 3 (6.4) | 5 (11.9) | 2 (6.7) | 9 (15) | 5 (8.8) |
| 26–30 | 8 (21.1) | 16 (24) | 11 (23.4) | 4 (9.5) | 5 (16.7) | 10 (16.7) | 14 (24.6) |
| 31–35 | 9 (24) | 13 (19.1) | 7 (14.9) | 8 (19.1) | 8 (26.7) | 13 21.7) | 12 (21.1) |
| 36–40 | 8 (21.1) | 12 (17.6) | 11 (23.4) | 12 (28.6) | 10 (33.3) | 13 (21.7) | 12 (21.1) |
| 41–45 | 7 (18.4) | 9 (13.2) | 7 (14.9) | 8 (19.1) | 3 (10) | 9 (15) | 5 (8.8) |
| 46–50 | 3 (7.9) | 3 (4.4) | 4 (8.5) | 2 (4.8) | 1 (3.3) | 4 (6.7) | 5 (8.8) |
| 51+ | - | 6 (8.8) | 4 (8.5) | 3 (7.1) | 1 (3.3) | 2 (3.3) | 4 (7) |
| Total | 38 | 68 | 47 | 42 | 30 | 60 | 57 |
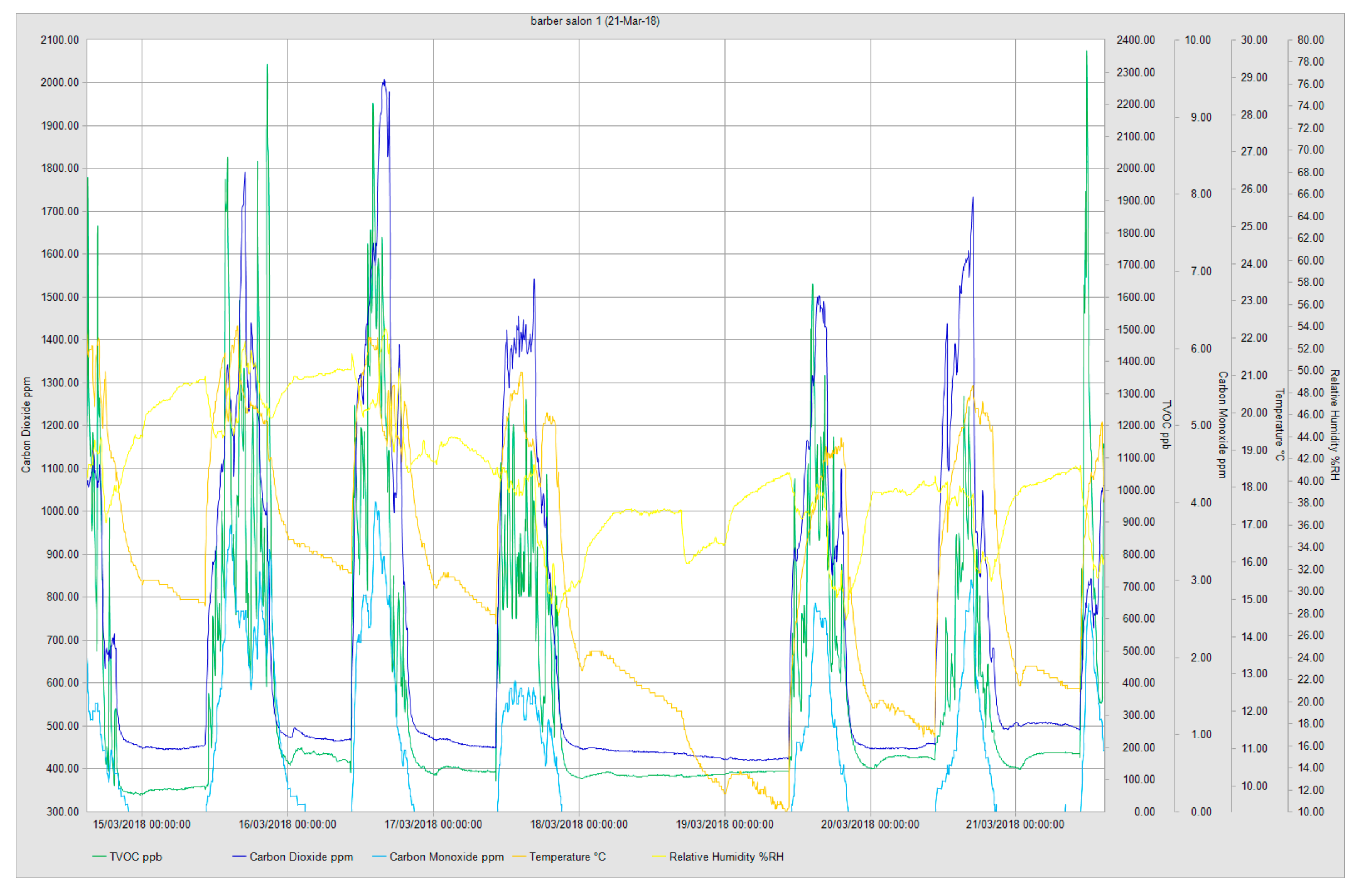
| Measured Compounds | Salon 1 | Salon 2 | Salon 3 | Salon 4 | Salon 5 |
|---|---|---|---|---|---|
| TVOC (ppb) | |||||
| Min | 52 | 2501 | 304 | 1182 | 168 |
| Max | 2351 | 15752 | 5909 | 8809 | 2428 |
| Average | 365.6 | 8215.9 | 1521.2 | 3330.9 | 2463.8 |
| STEL (15 min) | 1096 | 5316 | 2119 | 5851 | 291 |
| TWA (8 h) | 550 | 6955 | 907 | 2248 | 232 |
| CO2 (ppm) | |||||
| Min | 420 | 554 | 457 | 491 | 517 |
| Max | 2009 | 2124 | 2668 | 3006 | 7257 |
| Average | 695.1 | 1117.5 | 794.2 | 1117.1 | 2463.8 |
| STEL (15 min) *** | 1055 | 586 | 1783 | 1614 | 2239 |
| TWA (8 h) *** | 654 | 670 | 809 | 638 | 1214 |
| CO (ppm) | |||||
| Min | 0.0 | 0.3 | 0.0 | 0.7 | 0.2 |
| Max | 4.0 | 1.7 | 5.8 | 14.6 | 23.4 |
| Average | 0.57 | 0.94 | 1.08 | 4.42 | 6.8 |
| STEL (15 min) ** | 0.8 | 0.3 | 1.6 | 5.4 | 7.5 |
| TWA (8 h) ** | 0.8 | 0.6 | 0.4 | 2.0 | 3.4 |
| Temperature (°C) | |||||
| Min | 9.3 | 14.2 | 13.4 | 16.6 | 16.7 |
| Max | 22.3 | 19.4 | 28.2 | 24.6 | 24.8 |
| Average | 15.61 | 17.92 | 18.92 | 20.25 | 21.1 |
| STEL (15 min) | 17.8 | 17.2 | 24.3 | 21.8 | 22.8 |
| TWA (8 h) | 15.2 | 17.5 | 18.0 | 18.6 | 21.4 |
| Relative Humidity (%RH) | |||||
| Min | 27.4 | 39.8 | 25.3 | 29.1 | 43.0 |
| Max | 53.9 | 59.2 | 49.7 | 48.4 | 51.6 |
| Average | 40.42 | 41.58 | 34.11 | 36.54 | 45.57 |
| STEL (15 min) | 32.9 | 40.5 | 38.8 | 47.7 | 46.7 |
| TWA (8 h) | 37.8 | 40.9 | 39.5 | 42.9 | 46.7 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moda, H.M.; King, D. Assessment of Occupational Safety and Hygiene Perception among Afro-Caribbean Hair Salon Operators in Manchester, United Kingdom. Int. J. Environ. Res. Public Health 2019, 16, 3284. https://doi.org/10.3390/ijerph16183284
Moda HM, King D. Assessment of Occupational Safety and Hygiene Perception among Afro-Caribbean Hair Salon Operators in Manchester, United Kingdom. International Journal of Environmental Research and Public Health. 2019; 16(18):3284. https://doi.org/10.3390/ijerph16183284
Chicago/Turabian StyleModa, Haruna Musa, and Debrah King. 2019. "Assessment of Occupational Safety and Hygiene Perception among Afro-Caribbean Hair Salon Operators in Manchester, United Kingdom" International Journal of Environmental Research and Public Health 16, no. 18: 3284. https://doi.org/10.3390/ijerph16183284
APA StyleModa, H. M., & King, D. (2019). Assessment of Occupational Safety and Hygiene Perception among Afro-Caribbean Hair Salon Operators in Manchester, United Kingdom. International Journal of Environmental Research and Public Health, 16(18), 3284. https://doi.org/10.3390/ijerph16183284