The Development and Validation of the Healthcare Professional Humanization Scale (HUMAS) for Nursing

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
1.1. Definition
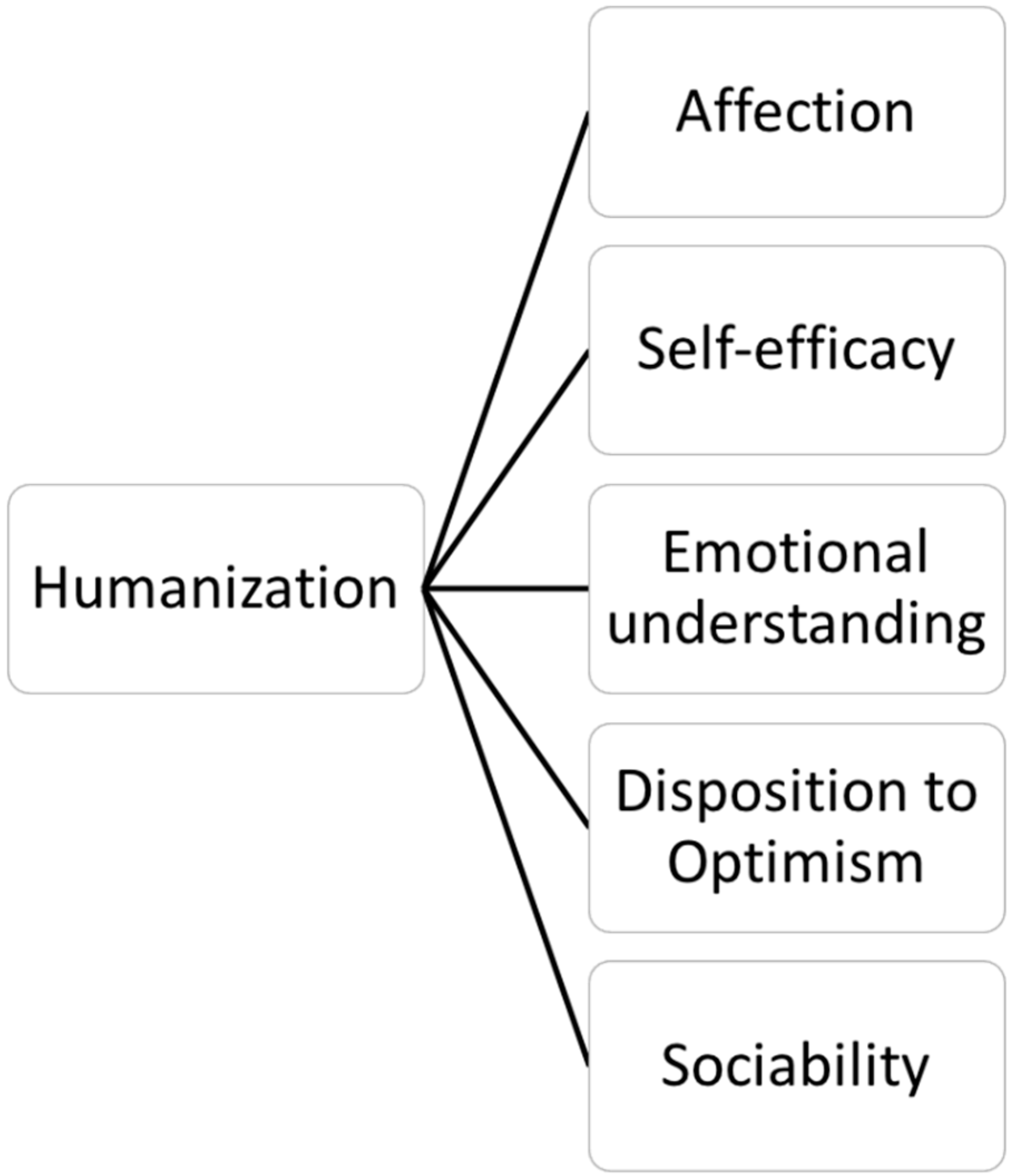
1.2. Dimensions
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Preliminary Analysis
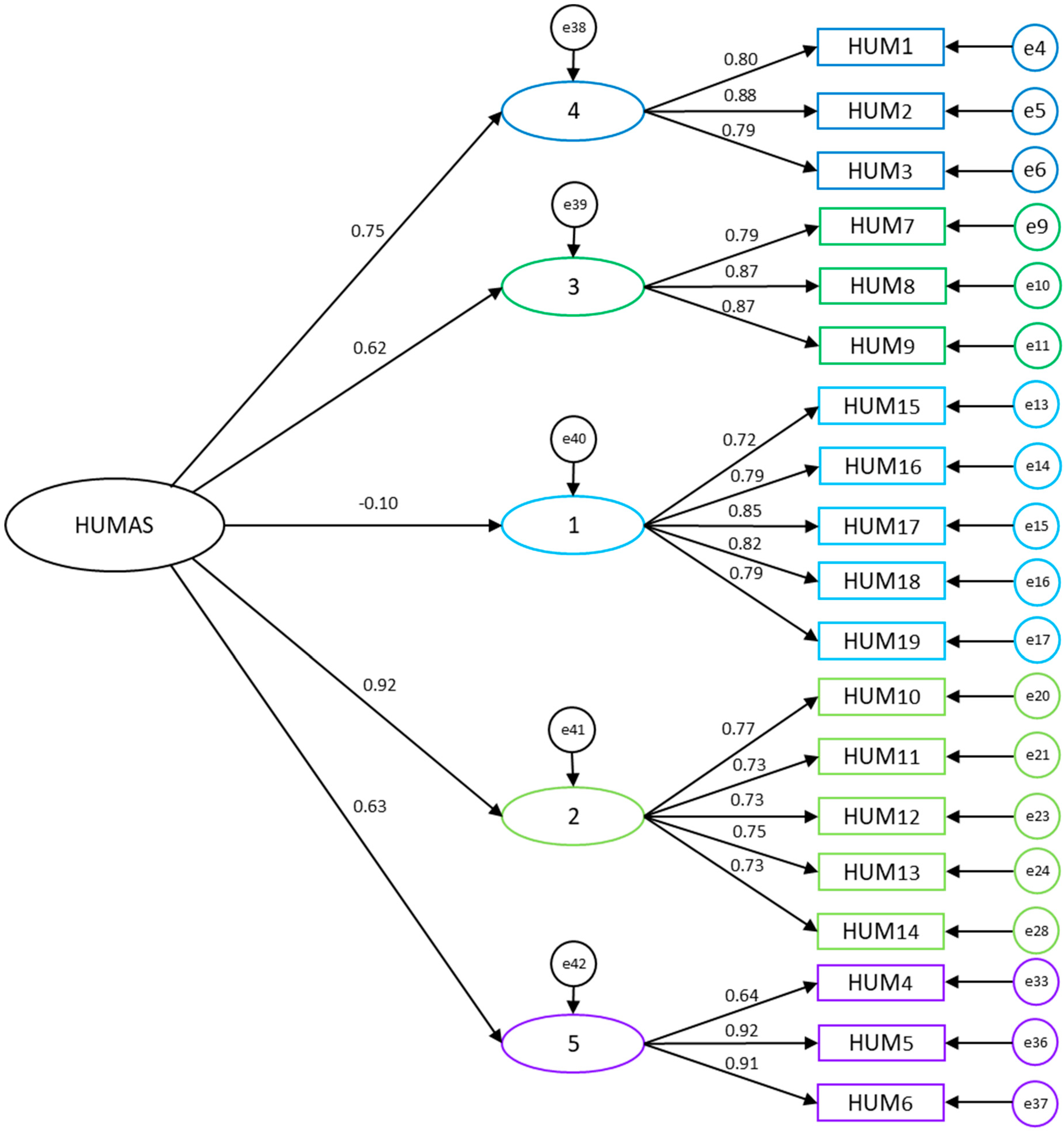
3.2. Confirmatory Factor Analysis of the HUMAS Model
3.3. Construct Validity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Behruzi, R.; Hatem, M.; Goulet, L.; Fraser, W.D. Perception of humanization of birth in a highly specialized hospital: Let’s think differently. Health Care Women Int. 2014, 35, 127–148. [Google Scholar] [CrossRef] [PubMed]
- Busch, I.M.; Moretti, F.; Travaini, G.; Wu, A.W.; Rimondini, M. Humanization of Care: Key Elements Identified by Patients, Caregivers, and Healthcare Providers. A Systematic Review. Patient 2019, 12, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Galvin, I.M.; Leitch, J.; Gill, R.; Poser, K.; McKeown, S. Humanization of critical care-psychological effects on healthcare professionals and relatives: A systematic review. Can. J. Anaesth. 2018, 65, 1348–1371. [Google Scholar] [CrossRef] [PubMed]
- Shin, S.; Kang, J. Development and Validation of a Person-Centered Perioperative Nursing Scale. Asian Nurs. Res. 2019, 13, 221–227. [Google Scholar] [CrossRef] [Green Version]
- March, J.C. Humanizing health to improve healthcare quality. Rev. Calid. Asist. 2017, 32, 245–247. [Google Scholar] [CrossRef]
- Molero, M.M.; Pérez-Fuentes, M.C.; Gázquez, J.J.; Barragán, A.B. Burnout in health professionals according to their self-esteem, social support and empathy profile. Front. Psychol. 2018, 9, 424. [Google Scholar] [CrossRef]
- Murji, A.; Gomez, M.; Knighton, J.; Fish, J.S. Emotional implications of working in a burn unit. J. Burn Care Res. 2006, 27, 8–13. [Google Scholar] [CrossRef]
- Parola, V.; Coelho, A.; Cardoso, D.; Sandgren, A.; Apóstolo, J. Prevalence of burnout in health professionals working in palliative care: A systematic review. JBI Database Syst. Rev. Implement Rep. 2017, 15, 1905–1933. [Google Scholar] [CrossRef]
- Michelan, V.C.A.; Spiri, W.C. Perception of nursing workers humanization under intensive therapy. Rev. Bras. Enferm. 2018, 71, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Greene, S.M.; Tuzzio, L.; Cherkin, D. A framework for making patient-centered care front and center. Perm. J. 2012, 16, 49–53. [Google Scholar] [CrossRef]
- Medeiros, A.C.D.; Siqueira, H.C.H.D.; Zamberlan, C.; Cecagno, D.; Nunes, S.D.S.; Thurow, M.R.B. Comprehensiveness and humanization of nursing care management in the Intensive Care Unit. Rev. Esc. Enferm. USP 2016, 50, 816–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tripodi, M.; Siano, M.A.; Mandato, C.; De Anseris, A.G.E.; Quitadamo, P.; Nuzio, S.G.; Siani, P.; Vajro, P. Humanization interventions in general pediatric wards: A systematic review. Eur. J. Pediatr. 2019, 178, 607–622. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, L.R.; Artmann, E. Pronouncements on humanization: Professionals and users in a complex health institution. Cienc. Saude Colet. 2018, 23, 1437–1450. [Google Scholar] [CrossRef] [PubMed]
- Sousa, K.H.J.F.; Damasceno, C.K.C.S.; Almeida, C.A.P.L.; Magalhães, J.M.; Ferreira, M.D.A. Humanization in urgent and emergency services: Contributions to nursing care. Rev. Gauch. Enferm. 2019, 40, e20180263. [Google Scholar] [CrossRef] [PubMed]
- Freitas, F.D.S.; Ferreira, M.A. Humanization knowledge of undergraduate nursing students. Rev. Bras. Enferm. 2016, 69, 261–268. [Google Scholar]
- Reeve, J.; Lynch, T.; Lloyd-Williams, M.; Payne, S. From personal challenge to technical fix: The risks of depersonalised care. Health Soc. Care Commun. 2012, 20, 145–154. [Google Scholar] [CrossRef]
- Heras, G.; Oviés, Á.A.; Gómez, V. A plan for improving the humanisation of intensive care units. Intensive Care Med. 2017, 43, 547–549. [Google Scholar] [CrossRef]
- Hosey, M.M.; Jaskulski, J.; Wegener, S.T.; Chlan, L.L.; Needham, D.M. Animal-assisted intervention in the ICU: A tool for humanization. Crit. Care 2018, 22, 1. [Google Scholar] [CrossRef]
- Luiz, F.F.; Caregnato, R.C.A.; Costa, M.R.D. Humanization in the Intensive Care: Perception of family and healthcare professionals. Rev. Bras. Enferm. 2017, 70, 1040–1047. [Google Scholar] [CrossRef]
- Lovato, E.; Minniti, D.; Giacometti, M.; Sacco, R.; Piolatto, A.; Barberis, B.; Papalia, R.; Bert, F.; Siliquini, R. Humanisation in the emergency department of an Italian hospital: New features and patient satisfaction. Emerg. Med. J. 2013, 30, 487–491. [Google Scholar] [CrossRef]
- Basit, A.A. Trust in supervisor and job engagement: Mediating effects of psychological safety and felt obligation. J. Psychol. 2017, 151, 701–721. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Oropesa, N.F. The Role of Emotional Intelligence in Engagement in Nurses. Int. J. Environ. Res. Public Health 2018, 15, 1915. [Google Scholar]
- Orgambídez, A.; Borrego, Y.; Vázquez-Aguado, O. Self-efficacy and organizational commitment among Spanish nurses: The role of work engagement. Int. Nurs. Rev. 2019, 66, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Fuentes, M.D.C.; Gázquez, J.J.; Ruiz, M.D.; Molero, M.M. Inventory of Overburden in Alzheimer’s Patient Family Caregivers with no Specialized Training. Int. J. Clin. Health Psychol. 2017, 17, 56–64. [Google Scholar] [CrossRef]
- Bandura, A. Self-Efficacy: The Exercise of Control; Freeman: New York, NY, USA, 1997. [Google Scholar]
- Williams, S.L. Self-efficacy, anxiety, and phobic disorders. In Self-Efficacy, Adaptation, and Adjustment: Theory, Research and Application; Maddux, J.E., Ed.; Plenum: New York, NY, USA, 1995; pp. 69–107. [Google Scholar]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J. Explanatory Value of General Self-Efficacy, Empathy and Emotional Intelligence in Overall Self-Esteem of Healthcare Professionals. Soc. Work Public Health 2019, 34, 318–329. [Google Scholar] [CrossRef]
- Lown, B.A.; McIntosh, S.; Gaines, M.E.; McGuinn, K.; Hatem, D.S. Integrating compassionate, collaborative care (the “Triple C”) into health professional education to advance the triple aim of health care. Acad. Med. 2016, 91, 310–316. [Google Scholar] [CrossRef]
- Orgambídez, A.; de Almeida, H. Work engagement, social support, and job satisfaction in Portuguese nursing staff: A winning combination. Appl. Nurs. Res. 2017, 36, 37–41. [Google Scholar] [CrossRef]
- Bar-On, R. The Bar-On model of emotional-social intelligence (ESI). Psicothema 2006, 18, 13–25. [Google Scholar]
- Gardner, H. Multiple Intelligences; Basic Books: Nueva York, NY, USA, 1983. [Google Scholar]
- Goleman, D. Emotional intelligence. Why it can matter more than IQ. Learning 1996, 24, 49–50. [Google Scholar]
- Hay, D.F.; Caplan, M.; Nash, A. The beginnings of peer relations. Handbook of peer interactions, relationships, and groups. In Handbook of Peer Interations, Relationthisps, and Groups; Rubin, K.H., Bukowski, W.M., Laursen, B., Eds.; Guilford Press: New York, NY, USA, 2009; pp. 121–142. [Google Scholar]
- Miao, C.; Humphrey, R.H.; Qian, S. A meta-analysis of emotional intelligence and work attitudes. J. Occup. Organ. Psychol. 2017, 90, 177–202. [Google Scholar] [CrossRef]
- Extremera, N.; Mérida-López, S.; Sánchez-Álvarez, N.; Quintana-Orts, C. How Does Emotional Intelligence Make One Feel Better at Work? The Mediational Role of Work Engagement. Int. J. Environ. Res. Public Health 2018, 15, 1909. [Google Scholar] [CrossRef] [PubMed]
- Baron-Cohen, S.; Wheelwright, S. The empathy quotient: An investigation of adults with Asperger syndrome or high functioning autism, and normal sex differences. J. Autism Dev. Disord. 2004, 34, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Dvash, J.; Shamay-Tsoory, S.G. Theory of mind and empathy as multidimensional constructs: Neurological foundations. Top Lang Dis. 2014, 34, 282–295. [Google Scholar] [CrossRef]
- Grove, R.; Baillie, A.; Allison, C.; Baron-Cohen, S.; Hoekstra, R.A. The latent structure of cognitive and emotional empathy in individuals with autism, first-degree relatives and typical individuals. Mol. Autism. 2014, 5, 42. [Google Scholar] [CrossRef]
- Decety, J.; Fotopoulou, A. Why empathy has a beneficial impact on others in medicine: Unifying theories. Front. Beahv. Neurosci. 2015, 8, 457. [Google Scholar] [CrossRef]
- Howick, J.; Steinkopf, L.; Ulyte, A.; Roberts, N.; Meissner, K. How empathic is your healthcare practitioner? A systematic review and meta-analysis of patient surveys. BMC Med. Educ. 2017, 17, 136. [Google Scholar] [CrossRef]
- Fernández-Berrocal, P.; Pacheco, N.E. La inteligencia emocional como una habilidad esencial en la escuela. RIE 2002, 29, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J. Mind-reading, emotion understanding, and relationships. Int. J. Behav. Dev. 2000, 24, 142–144. [Google Scholar] [CrossRef]
- Fonagy, P.; Bateman, A.W. Mentalizing and borderline personality disorder. J. Ment. Health 2007, 16, 83–101. [Google Scholar] [CrossRef]
- Piaget, J. El Lenguaje y el Pensamiento en el Niño; Guadalupe: Buenos Aires, Argentina, 1972. [Google Scholar]
- Selman, R.L. Social-cognitive understanding. A guide to educational and clinical practice. In Moral Development and Behavior: Theory, Research and Social Issues; Lickona, T., Ed.; Holt, Rinehart & Winston: New York, NY, USA, 1976; pp. 299–316. [Google Scholar]
- Segerstrom, S.C.; Carver, C.S.; Scheier, M.F. Optimism. In The Happy Mind: Cognitive Contributions to Well-Being; Robinson, M.D., Eid, M., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 195–212. [Google Scholar]
- Carver, C.S.; Scheier, M.F. Dispositional optimism. Trends Cogn. Sci. 2014, 18, 293–299. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E.; Schulman, P.; Tryon, A.M. Group prevention of depression and anxiety symptoms. Behav. Res. Ther. 2007, 45, 1111–1126. [Google Scholar] [CrossRef] [PubMed]
- Seligman, M.E. Learned Optimism: How to Change Your Mind and Your Life; Vintage Books: New York, NY, USA, 2006. [Google Scholar]
- Gerteis, M.; Edgman-Levitan, S.; Daley, J.; Delbanco, T.L. Understanding and Promoting Patient-Centered Care; Jossey-Bass: San Francisco, CA, USA, 1993. [Google Scholar]
- Gerteis, M.; Edgman-Levitan, S.; Walker, J.D.; Stoke, D.M.; Cleary, P.D.; Delbanco, T.L. What patients really want. Health Manag. Q. 1993, 15, 2–6. [Google Scholar]
- Merino-Soto, C.M.; Grimaldo-Muchotrigo, M.P.G. Validación estructural de la escala básica de empatía (Basic Empathy Scale) modificada en adolescentes: Un estudio preliminar. Revista Colombiana de Psicología 2015, 24, 261–270. [Google Scholar] [CrossRef]
- Oliva, A.; Antolín, L.; Pertegal, M.; Ríos, M.; Parra, A.; Hernando, A.; Reina, M. Instrumentos Para la Evaluación de la Salud Mental y el Desarrollo Positivo Adolescente y los Activos Que lo Promueven; Consejería de Salud: Sevilla, Spain, 2011. [Google Scholar]
- Jolliffe, D.; Farrington, D.P. Development and validation of the Basic Empathy Scale. J. Adolesc. 2006, 29, 589–611. [Google Scholar] [CrossRef] [PubMed]
- Caprara, G.V.; Alessandri, G.; Eisenberg, N.; Kupfer, A.; Steca, P.; Caprara, M.G.; Yamaguchi, S.; Fukuzawa, A.; Abela, J. The positivity scale. Psychol. Assess. 2012, 24, 701–712. [Google Scholar] [CrossRef]
- Rodríguez, L.M.; Mesurado, M.B.; Oñate, M.E.; Guerra, M.P.; Menghi, M.S. Adaptación de la Escala de Prosocialidad de Caprara en adolescentes argentinos. Revista Evaluar 2017, 17, 177–187. [Google Scholar] [CrossRef]
- Caprara, G.V.; Capanna, C.; Steca, P.; Paciello, M. Misura e determinanti personali della prosocialità. Un approccio sociale cognitivo. Giornale Italiano di Psicologia 2005, 32, 287–308. [Google Scholar]
- Álvarez-García, D.; Barreiro-Collazo, A.; Núñez, J.C.; Dobarro, A. Validity and reliability of the Cyber-aggression Questionnaire for Adolescents (CYBA). Eur. J. Psychol. Appl. Leg.Context 2017, 8, 69–77. [Google Scholar] [CrossRef]
- Bentler, P.M. EQS 6 Structural Equations Program Manual; Multiware Software, Inc.: Encino, LA, USA, 1986. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 7th ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2006. [Google Scholar]
- Akaike, H. A new look at the statistical model identification. IEEE Trans. Autom. Contr. 1974, 19, 716–723. [Google Scholar] [CrossRef]
- Byrne, B.M.; Stewart, S.M. The MACS approach to testing for multigroup invariance of a second-order structure: A walk through the process. Struct. Equ. Model. 2006, 13, 287–321. [Google Scholar] [CrossRef]
- Cheung, G.W.; Rensvold, R.B. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct. Equ. Model. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Finney, S.J.; di Stefano, C. Non-normal and categorical data in structural equation modeling. In Structural Equation Modeling: A Second Course; Hancock, G.R., Mueller, R.O., Eds.; Information Age: Greenwich, CT, USA, 2006; pp. 269–314. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| F1 | F2 | F3 | F4 | F5 | h2 | |
|---|---|---|---|---|---|---|
| Item1 | 0.830 | 0.782 | ||||
| Item2 | 0.820 | 0.818 | ||||
| Item3 | 0.753 | 0.728 | ||||
| Item4 | 0.702 | 0.627 | ||||
| Item5 | 0.878 | 0.871 | ||||
| Item6 | 0.858 | 0.859 | ||||
| Item7 | 0.819 | 0.770 | ||||
| Item8 | 0.858 | 0.833 | ||||
| Item9 | 0.856 | 0.826 | ||||
| Item10 | 0.772 | 0.694 | ||||
| Item11 | 0.645 | 0.602 | ||||
| Item12 | 0.713 | 0.642 | ||||
| Item13 | 0.761 | 0.683 | ||||
| Item14 | 0.752 | 0.662 | ||||
| Item15 | 0.791 | 0.637 | ||||
| Item16 | 0.836 | 0.717 | ||||
| Item17 | 0.870 | 0.763 | ||||
| Item18 | 0.849 | 0.739 | ||||
| Item19 | 0.835 | 0.710 | ||||
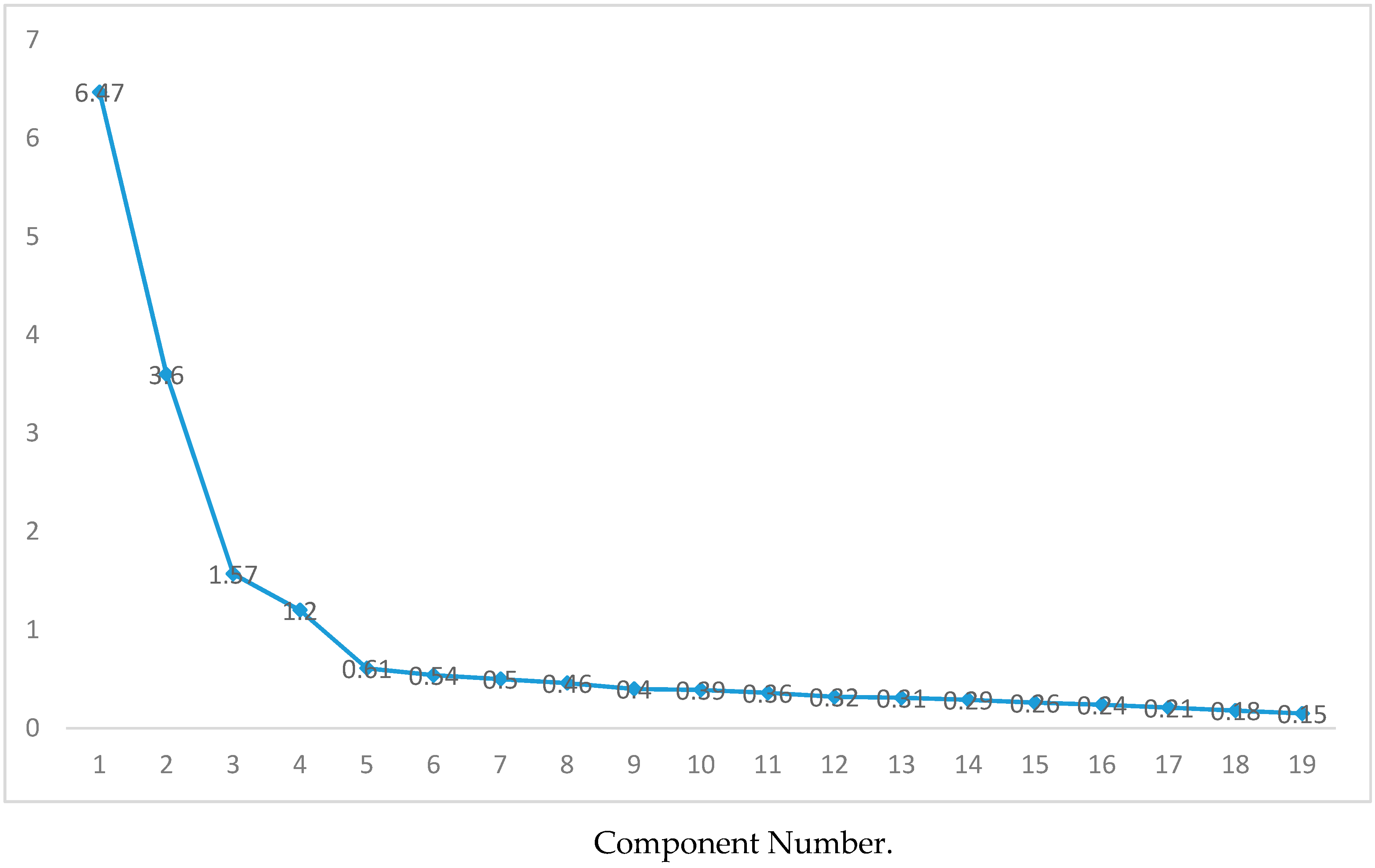
| Eigenvalue | 6.47 | 3.59 | 1.57 | 1.19 | 1.12 | |
| Percentage of explained variance | 34.07 | 18.93 | 8.27 | 6.30 | 5.90 | 73.47 |
| Kaiser-Meyer-Olkin | 0.88 | |||||
| Bartlett’s sphericity | χ2(171) = 3660.68, p < 0.000 | |||||
| Cronbach’s alpha | 0.89 | 0.86 | 0.88 | 0.86 | 0.85 | 0.86 |
| Model | χ2 (df) | χ2/df | CFI | TLI | IFI | RMSEA | ||
|---|---|---|---|---|---|---|---|---|
| Est. | CI90% | |||||||
| Low | High. | |||||||
| HUMAS Model without GF | 225.289 (142) | 1.586 | 0.977 | 0.972 | 0.977 | 0.042 | 0.031 | 0.052 |
| HUMAS Model with GF | 244.830 (147) | 1.665 | 0.973 | 0.968 | 0.973 | 0.045 | 0.035 | 0.055 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Affective Empathy | - | |||||||||
| 2. Cognitive Empathy | 0.420 ** | - | ||||||||
| 3. Prosocial Behavior | 0.283 ** | 0.557 ** | - | |||||||
| 4. Empathy and Emotional Support | 0.395 ** | 0.579 ** | 0.761 ** | - | ||||||
| 5. Positiveness | 0.042 | 0.397 ** | 0.510 ** | 0.408 ** | - | |||||
| 6. Optimistic disposition | 0.015 | 0.258 ** | 0.342 ** | 0.282 ** | 0.668 ** | - | ||||
| 7. Sociability | 0.242 ** | 0.398 ** | 0.557 ** | 0.472 ** | 0.421 ** | 0.493 ** | - | |||
| 8. Emotional understanding | 0.053 | 0.300 ** | 0.337 ** | 0.407 ** | 0.359 ** | 0.422 ** | 0.310 ** | - | ||
| 9. Self-efficacy | 0.107 | 0.434 ** | 0.630 ** | 0.577 ** | 0.609 ** | 0.577 ** | 0.533 ** | 0.522 ** | - | |
| 10. Affection | −0.131 * | 0.140 * | 0.218 ** | 0.053 | 0.311 ** | 0.114 * | 0.149 ** | −0.068 | 0.067 | - |
| HUMAS | 0.024 | 0.432 ** | 0.599 ** | 0.479 ** | 0.695 ** | 0.676 ** | 0.634 ** | 0.555 ** | 0.734 ** | 0.615 ** |
| Model | χ2 | df | χ2/df | Δχ2 | CFI | ΔCFI | IFI | RMSEA (IC 90%) |
|---|---|---|---|---|---|---|---|---|
| M0a (permanent) | 418.270 (p = 0.000) | 294 | 1.423 | 0.966 | 0.966 | 0.036 (0.028–0.044) | ||
| M0b (temporary) | 418.270 (p = 0.000) | 294 | 1.423 | 0.966 | 0.966 | 0.036 (0.028–0.044) | ||
| M1 (base model groups) | 418.270 (p = 0.000) | 294 | 1.423 | 0.966 | 0.966 | 0.036 (0.028–0.044) | ||
| M2 (SF) | 429.385 (p = 0.000) | 308 | 1.394 | 0.029 | 0.966 | - | 0.967 | 0.035 (0.026–0.042) |
| M3 (SF + Int) | 463.959 (p = 0.000) | 327 | 1.418 | 0.005 | 0.962 | 0.004 | 0.962 | 0.036 (0.028–0.043) |
| M4 (SF + Int + Err) | 546.904 (p = 0.000) | 356 | 1.536 | 0.113 | 0.947 | 0.019 | 0.947 | 0.040 (0.034–0.047) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Fuentes, M.d.C.; Herera-Peco, I.; Molero Jurado, M.d.M.; Oropesa Ruiz, N.F.; Ayuso-Murillo, D.; Gázquez Linares, J.J. The Development and Validation of the Healthcare Professional Humanization Scale (HUMAS) for Nursing. Int. J. Environ. Res. Public Health 2019, 16, 3999. https://doi.org/10.3390/ijerph16203999
Pérez-Fuentes MdC, Herera-Peco I, Molero Jurado MdM, Oropesa Ruiz NF, Ayuso-Murillo D, Gázquez Linares JJ. The Development and Validation of the Healthcare Professional Humanization Scale (HUMAS) for Nursing. International Journal of Environmental Research and Public Health. 2019; 16(20):3999. https://doi.org/10.3390/ijerph16203999
Chicago/Turabian StylePérez-Fuentes, María del Carmen, Iván Herera-Peco, María del Mar Molero Jurado, Nieves Fátima Oropesa Ruiz, Diego Ayuso-Murillo, and José Jesús Gázquez Linares. 2019. "The Development and Validation of the Healthcare Professional Humanization Scale (HUMAS) for Nursing" International Journal of Environmental Research and Public Health 16, no. 20: 3999. https://doi.org/10.3390/ijerph16203999
APA StylePérez-Fuentes, M. d. C., Herera-Peco, I., Molero Jurado, M. d. M., Oropesa Ruiz, N. F., Ayuso-Murillo, D., & Gázquez Linares, J. J. (2019). The Development and Validation of the Healthcare Professional Humanization Scale (HUMAS) for Nursing. International Journal of Environmental Research and Public Health, 16(20), 3999. https://doi.org/10.3390/ijerph16203999